
Abstract
The inclusion of same-sex married couples can illuminate and challenge assumptions about gender that are routinely taken for granted in studies of physical illness. We analyze gender dynamics in gay, lesbian, and heterosexual marriages with in-depth interview data from 90 spouses (45 couples) to consider how spouses co-construct illness experiences in ways that shape relationship dynamics. Overall, findings indicate that men tend to downplay illness and thus provide minimal care work, whereas women tend to construct illness as immersive and involving intensive care work—in both same-sex and different-sex marriages. Yet same-sex spouses describe similar constructions of illness much more so than different-sex couples, and as such, same-sex spouses describe less illness-related disagreement and stress. These findings help inform policies to support the health of gay and lesbian, as well as heterosexual, patients and their spouses, an important goal given health disparities of gay and lesbian populations.
About half of all Americans have one or more serious health conditions at any given time (Ward, Schiller, and Goodman 2014). When significant illness or injury occurs, it is a shared experience for spouses with consequences for the patient, their spouse, and the marriage. Past research shows that within heterosexual marriage, men and women react to a spouse’s illness in gendered ways. For example, compared to men, women provide more emotional support and physical care for an ill spouse and experience more stress from providing this care (Pinquart and Sorensen 2006; Thomeer, Reczek, and Umberson 2015). Yet prior research is limited in that it focuses only on heterosexual couples and typically considers only one spouse’s perspective.
In the present study, we draw from a gender-as-relational perspective (Springer, Hankivsky, and Bates 2012) to argue that social constructions of illness and interactions around illness unfold differently for men and women in same-sex marriages than in different-sex marriages. Based on this framework, we analyze in-depth interview data from both spouses in gay, lesbian, and heterosexual marriages to consider how men and women in same-sex and different-sex marriages (90 spouses in 45 marriages) understand their own illness as well as their spouse’s illness. We pay particular attention to the ways that perceptions of illness shape care work (i.e., the emotional and physical work of caring for a partner), expectations for care, and illness-related stress. We bridge literatures on gendered social constructions of the illness experience, gendered experiences of illness within relationships, and gender dynamics within same-sex and different-sex relationships to form a foundation for this analysis.
Understanding how same-sex and different-sex spouses interact around illness is particularly important because of health disparities for sexual minority compared to heterosexual populations (Institute of Medicine 2011). Such disparities may be reduced by marriage with associated benefits for health (Wight, LeBlanc, and Badgett 2013), necessitating the inclusion of same-sex couples in studies of marital dynamics and illness. Comparing same-sex and different-sex married couples also reframes existing assumptions about gendered illness and marital dynamics currently based on different-sex marriages. We extend the existing literature by including same-sex couples and considering the perspectives of both the patient and their spouse.
Background
Sociologists have long theorized that illness experiences are socially constructed (Brown 1995; Conrad 1987; Conrad and Barker 2010; Strauss and Glaser 1975). Illness is not solely a biological reality; it is also shaped by cultural values, experienced in social contexts, and influenced by beliefs about health. When sick, individuals imbue illness with socially constructed meanings that in turn shape their reaction and adaptation to illness (Conrad and Barker 2010). Social constructions of illness are also gendered in ways that frame how men and women understand and react to illness (Barker 2005; Lorber and Moore 2002). Gender is a powerful structural system characterized by different opportunities, demands, and constraints for men and women that in turn shape social experiences, including illness (Bird and Rieker 2008; Ridgeway 2011; Umberson et al. 1996). For example, men are pressured to be physically strong, self-reliant, and inattentive to physical symptoms and pain, and thus some men reject the position of patient as illness implies weakness and femininity; as a result, men sometimes avoid seeking help for their health concerns (Courtenay 2000; García-Calvente et al. 2012; McVittie and Willock 2006). Based on past studies and in line with a masculinity narrative, men may downplay or minimize their own illness concerns and physical limitations. In comparison, the literature on women’s illness constructions shows that women are often constructed as the “weaker sex” with frailer bodies (Emslie and Hunt 2008; Nathanson 1975). Perhaps consequently, women are more aware of and responsive to their own physical symptoms (Lyons 2009; Young 1990). This literature suggests that—in contrast to men—women will be more aware of and responsive to their own illness and physical limitations.
Most research on the social construction of illness focuses on patients as individuals, considering how the patient constructs his or her own illness experience. Yet, as Brown (1995:36) argues, “the social construction of illness . . . has to do with a more interactionist perspective of experience at personal, dyadic, and group levels.” In this study, we consider the dyadic level, focusing on how illness is co-constructed by both spouses within the context of marital unions. We build on past understandings of illness as gendered and socially constructed to argue that within marriage, illness is constructed by both spouses in gendered ways. Within heterosexual relationships, women are more likely to be positioned as health experts and nurturers, perhaps giving women more authority in constructing their spouse’s illness experience. For example, women do more work to monitor and improve their spouse’s health habits than do men within heterosexual marriage (Reczek and Umberson 2012). In contrast, heterosexual men are more likely to ignore their own physical symptoms and resist formal healthcare (Courtenay 2000; García-Calvente et al. 2012), which may further extend to dismissing and minimizing their spouse’s illnesses, although this is less studied.
In marriage, illness co-constructions may be fairly concordant with both spouses in general agreement on illness constructions, or they may be more discordant with spouses in general disagreement about the meaning of illness and how illness should be dealt with (Klein Woolthuis et al. 2013). These co-constructions have implications for both spouses as well as the marital relationship. For example, heterosexual spouses who are more concordant in their assessment of the seriousness of an illness have higher quality of life and less distress than couples who are more discordant in these constructions (Merz et al. 2011; Twiddy, House, and Jones 2012). Yet, the studies that consider illness constructions have focused on heterosexual marriage and rarely direct explicit attention to gendered patterns. Gendered co-constructions of illness likely shape whether and how spouses support and care for each other during illness. Studies of spousal caregiving within heterosexual marriage show that women provide more intensive and routine care to a sick spouse than do men. Moreover, women’s caregiving is more emotionally and physically taxing, less appreciated, and more likely to be performed in isolation than is men’s caregiving (Freedman, Cornman, and Carr 2014; Pinquart and Sorenson 2006). Consequently, research on heterosexual relationships shows that caring for a sick spouse is perceived as more stressful for women caregivers than men and is decidedly more detrimental to women’s physical and mental health and marital satisfaction (Penning and Wu 2015; Pinquart and Sorenson 2006).
Recent work further suggests that it may be more stressful for women when they themselves are sick; Thomeer and colleagues (2015) recently argued that because women are often viewed as natural nurturers who place a high priority on caring for others, they find ways to resist proffered care and reject the sick role in order to provide care to others even during their own illness. These findings may partly explain why heterosexual couples are more likely to divorce when a wife is seriously ill than when a husband is seriously ill (Karraker and Latham 2015).
Gender-as-relational Approach to Illness within Marriage
Despite a significant literature on both caregiving and illness experiences within marriage, our understanding of how gender shapes relationship dynamics during periods of illness is incomplete. Illness and caregiving research has largely been heteronormative, failing to consider the experiences of gay and lesbian couples. Including gay and lesbian couples alongside heterosexual couples allows for a “decentering” of heteronormativity (Oswald, Blume, and Marks 2005). A gender-as-relational perspective is ideally suited to an examination of men and women in the context of same-sex and different-sex marriages and allows us to reimagine and broaden our understandings of how gender matters for illness and caregiving dynamics within intimate relationships. A relational perspective on gender conceptualizes “gender as a pervasive system of stratification that structures relationships and interactions between and among men and women” (Springer et al. 2012:1661; also see Connell 2005; Connell and Messerschmidt 2005). Theoretical work in this area emphasizes that men and women are encouraged via social rewards and sanctions to adhere to cultural ideals of masculinity and femininity, but that gender is relational and acted out differently depending on the gender and sexuality of one’s self and one’s spouse (Umberson, Thomeer, and Lodge 2015b).
Previous research raises questions about whether the gendered experiences of illness and care work are expressed in different ways for spouses with a same-sex partner compared to those with a different-sex partner. For example, men and women in same-sex unions may “queer” marriage by interacting, either consciously or unconsciously, in ways that diverge from traditional heterosexual norms (Oswald et al. 2005). Indeed, a growing body of work suggests that gendered interactions within same-sex relationships differ from those of different-sex relationships (Reczek and Umberson 2012; Umberson et al. 2015a). Gender dynamics and scripts within gay and lesbian couples are theorized to be more fluid and include less emphasis on power differences between partners as compared to gender dynamics within different-sex couples (Moore 2008; Reczek and Umberson 2012). For example, same-sex relationships are characterized by greater egalitarianism regarding attempts to enhance each partner’s health behaviors (Reczek and Umberson 2012) as well as the division of household tasks and child care (Goldberg, Smith, and Perry-Jenkins 2012). Extrapolating from this literature, same-sex spouses may be more concordant than different-sex spouses in their approach to a spouse’s illness, and, by extension, same-sex spouses may experience more equality as well as less conflict and stress in relation to illness and care work—considerations that have not been explored in prior empirical research.
This approach does not preclude the possibility that dominant gender scripts are as strong an influence in same-sex marriages as in different-sex marriages. Moore (2008) argues that gender continues, “to profoundly influence the construction of family life,” (p. 352) even within same-sex couples. Recent studies working from a gender-as-relational perspective highlight important differences in the ways that gay men, compared to lesbian women, conceptualize gendered selves in their intimate relationships, demonstrating that gendered discourses in gay and lesbian relationships often align with discourses used in heterosexual relationships (Moore 2008; Peplau and Fingerhut 2007; Reczek and Umberson 2012; Umberson et al. 2015b), For example, lesbian women tend to engage in reciprocal emotional support due to an emphasis on feminine norms around caring for the emotional needs of others (Umberson et al. 2015a). In contrast, gay men are inclined to engage in more limited and targeted exchanges of emotional support that they partly explain in terms of a masculinity discourse of self-sufficiency and autonomy (Umberson et al. 2015a). Thus, gendered discourses and constructions around physical illness may follow a different pattern in marriages between two men than in marriages between two women.
The Present Study
Examining gendered experiences and relationship dynamics surrounding illness in same-sex and different-sex marriages necessitates dyadic analyses that consider both the sick spouse and the partner’s perspective in relation to each other (Carr and Springer 2010; Umberson et al. 2015a). We analyze dyadic data (i.e., data collected from both spouses in a marriage) that allow us to consider each spouse’s perspective on the experiences and strains of dealing with their own illness as well as their spouse’s illness. Dyadic-level data allow us to go further than individual-level data to examine whether illness experiences depend on the gender composition of a couple (i.e., same-sex or different-sex). Moreover, qualitative investigation is ideally suited to examining the subjective meanings and dynamic processes around illness (Strauss and Glaser 1975). Thus, we analyze qualitative dyadic data from in-depth interviews to ask: How do men and women in gay, lesbian, and heterosexual marriages construct the illness experience, and how do these co-constructions of illness shape their provision and/or receipt of care and illness-related stress when one of them is ill?
Data and Methods
Data
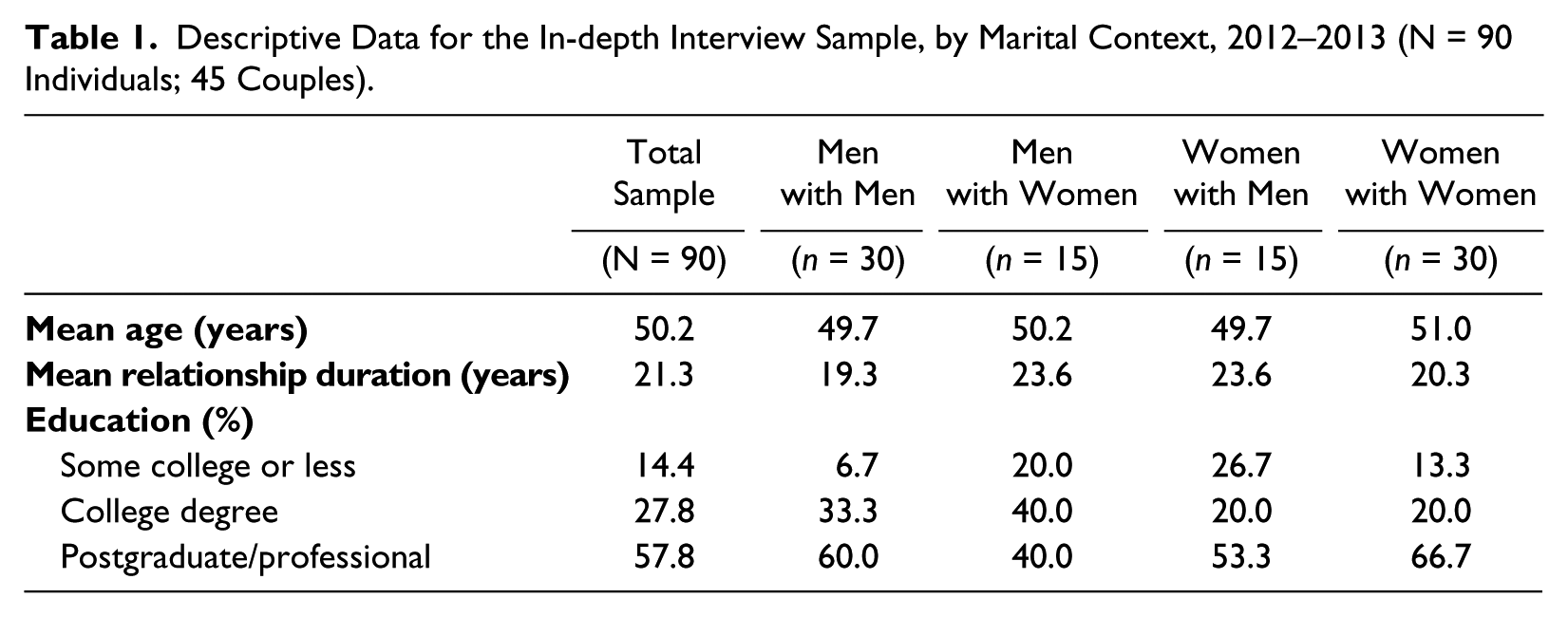
Our dyadic design relied on the participation of both spouses in each marriage. The in-depth interview sample included 90 individuals in 45 couples: 15 gay couples (30 men), 15 lesbian couples (30 women), and 15 heterosexual couples (15 men and 15 women). The overall study was designed to consider how same-sex and different-sex spouses influence each other’s health. We focused on midlife (given that chronic and serious conditions become more common by midlife) couples with marital durations that ensured a significant history between spouses (minimum seven years). Massachusetts was chosen as the study site because it was the first U.S. state to legalize same-sex marriage (in 2004) and thus had the largest population of same-sex couples in long-term marriages at the time of the study. Due to past legal restrictions on marriage for same-sex couples, we measured total relationship duration based on number of years cohabiting and married combined. For the in-depth interview sample, we recruited spouses aged 40 to 60, legally married for at least seven years at the time of the interviews (2012–2013), and residing in Massachusetts. The average age of the sample was 50, average relationship duration was 21 years, and 9% of all respondents described themselves as nonwhite. Descriptive data on demographic characteristics of the in-depth interview sample are provided in Table 1.
Descriptive Data for the In-depth Interview Sample, by Marital Context, 2012–2013 (N = 90 Individuals; 45 Couples).
Although not representative of the U.S. population, the sample was recruited through a systematic strategy designed to create comparability across gay, lesbian, and heterosexual couples, particularly in relationship duration and age. First, same-sex couples married between 2004 and 2006 were identified through the Massachusetts vital records office and invited to participate via letters/flyers mailed to the address obtained from those records. Second, spouses enrolled in the study were asked to refer same-sex and different-sex couples, especially siblings and friends, from their social networks, with an emphasis on recruiting couples of a similar age. This strategy was designed to maximize comparability across groups not only in terms of age but also in terms of race, socioeconomic status, and social background. The vast majority of same-sex couples in the in-depth interview sample were identified through Massachusetts vital records, and the majority of different-sex couples were identified through referrals from same-sex couples.
Methods
In-depth interviews were conducted separately (to ensure privacy and confidentiality) with each spouse and included open-ended questions about illness experiences within marriage; each individual received a $50 gift card for their participation in the research project. Interviewers used the same interview guide (with open-ended questions) for all respondents and asked follow-up questions when appropriate. We obtained basic information on current health status and prior serious illnesses/injuries from both spouses in each couple. Spouses were asked to identify and fully report on “the most serious physical illness or injury” that they and their spouse had experienced during their relationship. Physical conditions varied in severity and included cancer, autoimmune disorders, heart conditions, serious accidents, and chronic conditions (e.g., diabetes, arthritis). After we obtained basic information about illnesses, we asked more specific questions about how each spouse approached and experienced the illness, including questions about whether either spouse provided care work during this illness. For example, respondents were asked, “What did your spouse do for you when you were ill that was helpful to you during this time? What did your spouse do that was unhelpful during this time?”
All interviews were independently analyzed by the authors using a standardized method of inductive data analysis that emphasizes the dynamic construction of codes for the purpose of developing analytical and theoretical interpretations of data (Silverman 2006). NVivo qualitative software was used to organize the data; no NVivo programs were run to automatically code the data. The authors used inductive reasoning to guide the coding and analysis, identifying patterns and conceptual categories as they emerged from the transcripts. In line with a standard approach to qualitative data analysis, the authors read the transcripts multiple times to ensure understanding of the content of the interviews; thereafter, the authors followed a three-step coding process. First, the authors conducted line-by-line, data-driven categorization in order to summarize each piece of data as it related to the illness of one or both spouses. Next, the authors independently performed “focused” coding to develop categories regarding both the illness and perceptions of marital dynamics regarding the illness, connecting initial line-by-line codes together for conceptual purposes. In the final stage of analysis, the authors created categories and subcategories that related to one another on a theoretical level; the themes from this final stage are discussed below. A key component of our analysis was a dyadic comparison; we use the terms “patient” (the spouse who experienced illness) and “spouse” to distinguish between spouses within a marriage in the following results section. Spouses are also sometimes referred to as “care providers”. We considered “concordance” and/or “discordance” between spouses, indicating degree of alignment between spouses in regard to constructions of illness and provision and receipt of care.
Results
Overall, our analysis suggested that patients and spouses construct and approach illness in two dominant and distinctive ways. Spouses typically constructed illness in ways that either minimized the seriousness of illness or that emphasized immersion in the illness experience. Most spouses who minimized illness also generally downplayed the need for care work around the illness. In contrast, spouses who constructed the illness as immersive generally described illness as requiring intensive care and attention from both the patient and care provider. Findings suggested that among both patients and care providers within same-sex and different-sex marriages, men generally engaged in more minimizing of illness and consequently expected and provided less care work. In contrast, women generally engaged in more illness immersion and consequently more care work and a wider range of types of care work for their same- or different-sex spouse.
Reflecting the gendered co-construction of illness, spouses in same-sex relationships generally described illness experiences in similar ways, suggesting a fairly high level of concordance between spouses. In contrast, spouses in different-sex relationships tended to describe illness experiences in divergent ways, suggesting more discordance between spouses. When constructions of illness were concordant (e.g., both spouses minimized or immersed in the illness), as was typically the case with same-sex couples, spouses described very little interpersonal strain and conflict around care work. Yet, when constructions of illness were discordant (e.g., one spouse minimized the illness while the other was immersed in the illness), as was typically the case with different-sex couples, spouses often described misunderstandings and relationship strain around the provision and receipt of care.
Concordant Couples
We begin by illustrating concordant illness experiences, which were primarily described by same-sex couples. First, we discuss concordant minimization themes that were primarily found for men married to men. We then turn to concordant immersion themes typically found among women married to women.
Concordant Spouses and Illness Minimization
The vast majority of the gay men we interviewed talked about illness experiences in ways that minimized their own and their spouse’s illness concerns. Although a concordant minimization frame was most common among gay men, a few lesbian couples and one heterosexual couple also described this kind of concordance. When there was significant concordance in minimization, both spouses tended to downplay the seriousness of illness and generally agreed with each other about the ways and extent to which illness disrupted usual routines and relationship dynamics. This construction was also characterized by a tendency for patients and their spouse to downplay the need for care work. For example, Richard learned three weeks before our interview that he had advanced prostate cancer; William discussed Richard’s recent diagnosis and the impending launch of a significant treatment regimen saying, “Richard calls it ‘a little bit of a nuisance.’ . . . There’s something telling me that this is not going to be a big issue.” This minimizing approach was echoed in the way Richard talked about his own expectations for cancer treatment, “The major side effects are pretty minimal . . . I anticipate that the first couple months will just be kind of like, you won’t be in your typical kind of groove.” Richard’s low-key approach was particularly striking because he knew the stark reality of serious illness in that he provided six months of intensive caregiving for a previous long-term partner who died of brain cancer.
About four years prior to our interview, Andrew, married to Eric, was diagnosed with bladder cancer that required surgery and three years of treatment. When Eric discussed Andrew’s cancer, he also minimized the seriousness and difficulty of the situation; his efforts appear to have made the illness less threatening and stressful: Maybe it was ignorance is bliss . . . because it wasn’t anything like testicular cancer or melanoma or anything that had a big more widespread name. . . . That maybe kept me calm and made it sound a little bit more routine.
Andrew went through a painful treatment regimen that he describes as “hell,” even while downplaying the difficulty of his own experience. Despite spending days in bed during his treatment, he said he never needed hands-on assistance and was not worried, “This kind of cancer isn’t typically lethal or whatever; you’re not going to die from this, but it is something you’ve got to take care of and keep an eye on.”
For most gay couples in the sample, minimization concordance seemed to keep care work low-key, helping to also minimize stress for both spouses. Not only did the spouse use the minimization construction of illness to justify not providing care or providing low-key care, but the ill spouse typically did not expect a lot of care and emphasized self-sufficiency. When Andrew was asked how Eric helped him during his cancer treatment, he said, “I don’t think there’s anything he does differently, it’s just like knowing he’s there, knowing he’s like, you know, concerned.” Similarly, Michael felt supported by his spouse during treatment for melanoma but described this support as minimal, “It was mostly him, at key moments, taking time off to sort of help.” In another example, Martin explicitly tied gender and masculinity to self-sufficiency in dealing with advanced kidney disease, “Because we are two men and both type A personalities, we tend to, it’s not that we don’t care for one another but that we both kind of assume the other person is okay unless they ask for help.” For most of the gay respondents, both spouses generally shared the expectation that more intensive caregiving would be provided if needed. For example, Martin said, “Obviously if I ask him to he would but . . . it’s not that we don’t care but it’s that we, there’s a line, there’s a threshold where when one of us raises our hand and says, ‘Okay I need help.’”
Minimization concordance occurred in just a few lesbian couples. Pamela and Lori both reported chronic illnesses—Lori had a degenerative eye condition, and Pamela had kidney issues and arthritis. When asked about how illness changed their daily interactions in the home, Pamela said, “We don’t have any gender roles. It’s like, if stuff needs to be done, stuff needs to be done,” linking their low-key dynamic to a lack of gender power dynamics within their relationship. This approach extended to the independent way they dealt with their own illnesses. Both partners were content with the level of support they received from each other, which was minimal, in line with mutual construction of their conditions. Curtis and Annette were the only heterosexual couple in our sample to describe a shared minimization framework. Annette had a double mastectomy and chemotherapy after being diagnosed with breast cancer, but when asked about major illnesses during their relationship, Curtis did not initially remember her breast cancer, saying, “You sort of push it back a little bit,” and Annette minimized her own experience of breast cancer and said she needed to stay strong for her young daughters.
Concordant Spouses and Illness Immersion
The majority of lesbian women (but only a few gay and heterosexual couples) described concordance around an immersive approach to illness. The co-construction of illness as immersive was often associated with the provision of intensive care work. Intensive care work included making detailed arrangements for treatment and caring for, monitoring, and responding to the needs of the sick spouse. Lesbian spouses were typically highly concordant in this immersive approach to illness and tended to describe reciprocal care work in which both patient and spouse provided care for each during the illness. For example, Kathy talked about how she and her spouse would be there for each other no matter who gets sick, “I think we’re under the basic assumption that we’re going to take care of each other as much as we possibly can. So you know when it’s who takes care of who doesn’t really make a difference.” Maureen also described reciprocity in her relationship with Alice, “We both want to take care of each other. So I think if she’s sick I’m more attentive and vice versa.” Importantly, lesbian spouses, unlike gay spouses and heterosexual women (described in the following section), did not typically talk about having to ask for help because each partner monitored and responded to the other partner’s needs. In turn, the recipient of care generally recognized the demands and strains of care work and made some effort to limit demands on their spouse. Lesbian patients also frequently expressed appreciation for their spouse’s immersive caregiving efforts (more so than other couples), which both spouses typically described as beneficial to their relationship. Laura said: Not [beneficial] in terms of our commitment to each other, our love for each other or anything like that, but I have, like I have such a deep appreciation and admiration for her after watching how she’s come through [for me].
Most of the lesbian spouses we interviewed conveyed the sense that they generally knew what their sick spouse needed or wanted (i.e., empathy as a component of intensive care work), a dynamic also discussed by many heterosexual women but few gay and heterosexual men in our sample. Knowing what a spouse needed was framed as “natural” and something that women just do for each other within relationships. Katie, despite having chronic back pain, also talked about care work as an easy task that she naturally did for Sarah: It’s what I’m supposed to do. I love her so I got to take care of her. You know, there’s no jealousy or there’s no pain in the butt or getting tired of doing this. It’s just part of our relationship. I have mine and she has hers and we have to take care of each other.
Lesbian spouses often talked about reading and understanding each other’s needs. Cheryl said, regarding Anne’s cervical cancer diagnosis, “We were so connected that I could tell what her blood work was going to be . . . I mean, it was weird, but we were so tuned in. . . . It was almost like being one person.” Similarly, Katie talked about her spouse’s Crohn’s disease, “I feel everything with her . . . she’ll be in here and I’ll be like did you just take your shot? She goes, ‘Why?’ I’m like, ‘I feel it.’” Heidi talked about how she worked to understand what Sally needed after being diagnosed with breast cancer: I [tried] to figure out where she was and how she wanted to respond to it. So the way I responded was probably more trying to figure out what was going on for her, see what happens and where it goes and be positive about it. Just follow her lead.
Empathy and connection worked both ways, wherein patients recognized that the caregiving spouse sometimes kept her own emotions in check. For example, Sally said, “Heidi always rallies. She may be like flipping out inside but she stays calm and she was very supportive of me.”
Continuously providing intensive care work, even when appreciated by the patient and viewed as not particularly hard on the relationship, often created personal stress for the caregiving spouse. As a strategy to keep their personal stress from negatively affecting the relationship or the patient, care providers sometimes described how they made an effort to hide their own stress from the patient. This was described by lesbian and heterosexual women but not by any of the gay or heterosexual men we interviewed. For example, Anne was diagnosed with stage four cervical cancer about a year before our interview. She described the intensive care work Cheryl did for her during the cancer treatment: Oh, she went to every appointment, every infusion . . . every appointment that I had . . . every pap smear, every oncology meeting that I had. She advocated for me, she had the questions, she knew exactly what it was that she needed to ask, and she dealt with all the insurance people.
Cheryl also handled all the household tasks and worked full-time throughout Anne’s treatment. Cheryl never considered doing otherwise, but the intensive caregiving was difficult for her; she said, “It was just crushing. I’m self-employed, and I couldn’t really take a lot of time off. I would cry on the way to work and I would cry on the way home. I really pretty much did everything.” Notably, Cheryl said she never cried in the presence of her spouse because part of her intensive care work involved shielding Anne from additional stress, “It’s just like if someone’s that weak, you’re not going to share that.” Sharon also talked about hiding her own worries when her spouse was dealing with endometrial cancer: It was a hard time . . . At the time I am sure I was freaked out, calling my girlfriends saying, “Oh my God, I’m losing my girl. Am I losing my girl?” Not letting her see that—there was no way. I was all positive with her. Because I don’t think that’s good for her recovery.
A few gay and heterosexual couples also described concordance around an immersion construction of a spouse/patient’s illness. However, this was typically described only for circumstances in which the patient—specifically the wife in the case of heterosexual couples—needed extensive care. In all but one instance in which heterosexual men provided intensive care work for a spouse, the situation was dire and the wife was unable to care for herself. We also found this pattern in reports for gay men. For example, Roger gave it his all over a three-month period when Patrick was being treated for stage four throat cancer: I slept on the couch in the living room because he was so uncomfortable . . . I felt like I wanted to know if Patrick was out of bed because he was, he was coughing, which sometimes led to choking, which sometimes led to retching and I wanted to be there for him. And so, you know, I basically kind of slept between him and the bathroom . . . I never thought about anything but taking care of him.
Patrick also said in his interview, “Roger was there for me in, in amazing ways, physically, morally, you know, tangibly, and intangibly.” It is not that most gay men said they were unwilling to help each other unless the situation is dire but because both care provider and patient tended to view the patient as self-sufficient and not in need of assistance in most cases.
In contrast to women in same-sex and different-sex marriages, when gay and heterosexual men found themselves immersed in intensive care work, they often talked about the need to carve out occasional respite for themselves. For example, Eric talked about the limits on what he could do for Andrew during Andrew’s cancer treatment as well as the need to occasionally take time off: There was, obviously, a little care needed right when he was a few days outside of surgery. Pain was really, was really tough and certainly to get him up to walk and things like that. Because it was internal [there was] not really anything I could do . . . We’ve always been kind of there when you need [help] or if you don’t . . . If you need your own time, that’s fine, too.
Discordant Couples
Illness constructions were discordant between partners when one spouse approached illness from a minimization frame and the other spouse from an immersion frame. Discordant experiences were more common in different-sex than same-sex marriages and reflected strongly gendered patterns, with heterosexual men typically adopting a minimization frame and heterosexual women an immersion frame.
Discordant Couples and Illness Minimization
In general, heterosexual men talked about illness in ways that reflected a minimization frame. This illness framing was very similar to that of gay men—downplaying the seriousness of the illness and the need for intensive care work. For example, Roseanne had retinal degeneration and was slowly losing her eyesight, but her husband’s approach to her illness was to minimize it; Abe said, “I try to not really act like it affects her when I’m around people and doing things. So sometimes I’m a little bit unsympathetic.” Roseanne said Abe restricted how much he helped her, noting, “He doesn’t let me not do things because of it. He tries to encourage me by being facetious if I say, ‘I can’t do that’ he says, ‘Why not?’ and ‘Try it.’”
Bill also glossed over his spouse’s serious illness. When Bill was asked about Miranda’s history of health problems, he recalled her health problems as “nothing nagging” but then added later, “She did have breast cancer about ten years ago, and did chemo.” Bill went on to note that the cancer was difficult for his wife but concluded by minimizing the seriousness of her cancer: Well it was traumatic for her, you know, because cancer is a bad word. I mean she’s thinking she won’t get her, she won’t see her children grow up and all that . . . The worst case would be getting something late in life. It’s probably not as troubling as someone who got it at a younger age.
Miranda noted that Bill approached her cancer rationally but not emotionally, saying, “He was being very intellectual about it and I know about this and I know what it means and it’s like, ‘no you don’t.’” This may have been an effective coping strategy for Bill because when asked if he experienced stress during his wife’s cancer, he said, “No, nothing, nothing out of the ordinary.”
Like Bill and Curtis, Dean minimized how much help his wife needed and how little he could do to help when she had breast cancer: I was there as much as I could be to make her comfortable, but I still had to go to work. But do I care for her as much as she cares for me? Probably not as much. She’s more attentive, I try to be, I try my best to be attentive. I think it’s enough to satisfy her.
Dean was asked to give an example of what he might do to be more attentive. He said, “At the time when she was really down, you know, [I asked] ‘what do you need, what can I get you?’ I will buy flowers. I don’t usually buy flowers.” Dean viewed his spouse as strong and self-sufficient and not in much need of help and added, “She is tough.” During his wife’s interview, when asked who looked after her during her cancer, Cindy said, “It was me. That was it.” But rather than framing this as self-sufficiency, as Dean did, Cindy complained that Dean was working during much of her illness when she wanted him to take more days off. She said, “When it was going on, I think I was resentful that he couldn’t take the time off.” Dean and Cindy demonstrated, as did many heterosexual couples, how discordance around constructions of illness between spouses contributed to less care work from men and more relationship strain related to the illness.
Even when heterosexual men provided care to their ill wife, men often minimized how much work they did and how much effort it took, whereas their spouse sometimes described the men as providing a great deal of care work. Ben was one of the heterosexual men who was very immersed in providing intensive care for his wife, who was largely incapacitated by multiple sclerosis. Denise described the care Ben provided for her: He does everything. Now I can’t cook anymore. I used to cook voraciously. I have a suprapubic catheter, he has to flush that and change it, which was very hard for him but he does it. He’s supported me all along in every way, I mean everything that happened, he supports.
Even though he provided an incredible amount of care for Denise, Ben still minimized the extent of his care work: It’s not a lot of time. It’s just that, I get up in the morning . . . and I’ll help her get dressed and everything. . . . Help her into the wheelchair and get her over to the bathroom. . . . Clean the bag while she’s getting ready . . . then she needs help to transfer into a shower. . . . Then I help her get dressed. . . . I get her breakfast then take off for work. That’s no time.
Discordant Couples and Illness Immersion
Much like lesbian women, most heterosexual women described their own and their spouse’s illness in ways that suggested an immersive experience. However, in contrast to lesbian spouses, heterosexual women often described a very different illness approach than their spouse. For instance, Bruce, who suffered from migraines, noted that his wife Penny was skilled at recognizing serious health issues and providing helpful care, “And I think in a sense there’s a, I won’t say innate, but a learned reaction that kicks in whenever something’s a little more serious. She does pretty good at that.” Dean has diabetes, and his wife provided intensive care work for him, working to constantly monitor his health. Dean said, “She is very concerned about [my diabetes] but she can’t monitor me all the time.” Yet Dean did not share this same serious approach to his own illness, minimizing it instead: We’ve tried to lose weight together, because diabetes has a lot to do with weight. So we’ve done bicycling. She’s got me to Weight Watchers once, we went to a gym club, a health club once. Like everything else, it’s a fad. You fall off and you go back to your old habits. I go on paths of self-destruction sometimes if she is not around. I’m cheating.
Dean’s “cheating” led to conflict, and he noted that Cindy “gets disappointed with me.” He minimized the seriousness of his illness, saying, “I tell people I’m the healthiest sick guy around,” and his minimization is in direct contrast to Cindy’s more immersive approach.
These patterns illustrate that even though heterosexual women tended to immerse themselves in their own or their spouse’s illness, heterosexual men often minimized these same illnesses and thus did not recognize their wife’s intensive care, sometimes leading to relationship tension. Penny talked at length about her husband’s frequent debilitating migraines and the care she provided for him during these times, but her husband never discussed his migraines as a problem. Similarly, Sherrie discussed the stark difference in her and her husband’s surgeries: If I have surgery, he’ll maybe bring me to the hospital and then wait for me to get checked in and then go home. Whereas, I, if he has surgery, I’ll bring him to the hospital, check him in, I’ll stay in the waiting room. I’m not gonna leave until I know he’s done with the surgery and fine.
As part of intensive care work, heterosexual women often talked about feeling guilty when they took time off from their care worker role. In fact, it seemed to not even occur to many women that they could take time for themselves when there is care work to be done. Women, especially heterosexual women, in comparison to men, emphasized feeling guilty in the patient role—because they were burdening their spouse. In turn, sick heterosexual women often worked to reduce stress for their well spouse. For example, Denise worried about how her multiple sclerosis affected Ben, “I try not to make things too tough on him but sometimes I can’t help it. . . . I hate the fact that I’m the patient though. I’d much rather be the nurse.”
Although a majority of the same-sex couples were characterized by concordance, a few couples described discordance. For example, Debbie downplayed illness concerns and needs when talking about Karen’s migraines: She doesn’t want too much fussing. She doesn’t want me to tell her to go to the doctor. She doesn’t want me to tell her. . . . I will usually ask her if she’s taken aspirin or some kind of medication. Because sometimes she’ll get stubborn and she won’t take it and she’ll get mad. . . . So I’ll reason with her on it. . . . But she really, she doesn’t like to be told what to do, ever, and especially when she’s sick.
When Debbie was diagnosed with shingles and expected care from Karen, she said she did not receive any because of Karen’s preferred approach. Debbie reported how she understood that this reflected Karen’s approach to illness: “I don’t mean that she does not have many wonderful qualities but I think [caregiving] would be a challenge for her.”
Similarly, Kevin downplayed his diabetes and many diabetes-related complications, yet his spouse, Joe, expressed a lot of concern about Kevin’s illness. Joe said he tried to help Kevin eat healthy foods and manage his diabetes, but Kevin was resistant to these efforts partly because he did not see his condition as serious. Kevin talked about the conflict they have regarding his diabetes: I know that Joe has stress over my health and I know that he worries about it and worries about why I don’t do more to take of that. But over the years he’s also recognized that he can’t push me to do anything because I’m an immoveable force when it comes to these things. . . . I think [this is] probably one of the biggest stresses in our lives.
Discussion
Previous research on illness in marriage has focused almost exclusively on heterosexual spouses, showing that illness is a strongly gendered experience within marriage. Now that marital equality for same-sex couples is guaranteed under federal law, social scientists are in a position to advance scientific understanding of marital dynamics and health for same-sex as well as different-sex couples. Past studies also relied primarily on reports from only one spouse about the illness, but illness is clearly a shared experience within marriage. To elucidate the ways in which same-sex and different-sex spouses co-construct and experience illness, we blended theoretical work on gendered social constructions of illness with a gender-as-relational perspective. Using this theoretical frame, we analyzed qualitative data with attention to illness as a dyadic process. We extend previous research to show that the experience of illness varies not only by gender but also depends on whether men and women are married to a same-sex or different-sex spouse.
Constructed Illness Experiences and Care Work
The first major theme from our analysis is that patients and spouses tend to construct and approach illness in gendered ways. Our findings suggest that whether respondents were in a same-sex or different-sex relationship and whether narratives were reported from the perspective of patient or care provider, illness constructions are strongly gendered with women tending to immerse themselves in the illness experience and men tending to downplay illness-related concerns and needs. Prior studies highlight gender inequality within heterosexual marriage, indicating that women provide more care than men and are also more burdened by that care (Pinquart and Sorensen 2006). We suggest that the burden of care work is partly due to gender differences in constructions of a spouse’s illness, and this extends to spouses in same-sex marriages. Our findings support past theoretical and empirical work by demonstrating gender differences in illness constructions (Lorber and Moore 2002) but go beyond previous research to suggest that gender differences in illness constructions and experiences transcend heterosexual marital contexts. Past work suggests that in different-sex relationships, women provide more support and care to a sick spouse than do men (Thomeer et al. 2015). Our analysis suggests that caring for a sick spouse is more low-key, less time-intensive, and less emotionally intensive for men than women, and this may reduce the stress of illness and care work for men.
Gender theory and empirical evidence suggest that social forces push women, regardless of the gender of their partner, to be highly attuned to the needs of others, provide nurturance and care to family members, and be self-sacrificing even while caring for others (Bird and Rieker 2008; Freedman et al. 2014; Lyons 2009; Pinquart and Sorensen 2006; Ridgeway 2011; Thomeer et al. 2015; Umberson et al. 1996)—helping to explain why the women in our study were more likely than the men to provide intensive care work for spouses and immerse themselves in the illness experience, particularly when in the position of caring for a sick spouse. Intensive care work involves labor- and emotion-intensive work in which the patient’s needs are placed above the spouse’s needs. In contrast, social forces push men to ignore and be stoic in response to physical and perhaps especially emotional symptoms of both the self and others (Courtenay 2000; García-Calvente et al. 2012). This may be especially true for older men, as men in poor health may have a greater incentive to get and stay married because of the health benefits marriage affords them (Lillard and Panis 1996).
Past research has paid attention to what cultural norms of masculinity mean for men’s personal healthcare practices (e.g., men are less likely to comply with medical advice or visit a doctor) and self-rated health within a heteronormative context (Courtenay 2000), but we argue that this masculinity approach to men’s own illness extends to men downplaying their spouse’s illnesses—in both different- and same-sex marital contexts. Men in both marital types rarely described intensive care work for a sick spouse unless the illness was particularly severe and their spouse was largely incapacitated, and even in these cases, men often emphasized their need and willingness to take some time for themselves in order to cope with the stress of care work. Future research should consider whether gender differences in intensive care work (and the potential costs and rewards of care work) extend to other family relationships, such as adult child–parent relationships and sibling relationships, as these relationships may also differ across gendered relational contexts (Reczek and Umberson 2016).
Gender-as-relational
Our second major theme is that gender is interactive, wherein the gender of the patient in relation to the gender of the spouse shapes dyadic illness constructions, care work, and subsequent relationship stress. Our findings suggest that gendered care work is borne out of dissimilar constructions of illness for men and women and is not unique to different-sex couples as women in same-sex relationships reported that they provided more support and care to a sick spouse than did men in same-sex relationships. This is a source of strength within lesbian couples as caregiving benefits may be greater within lesbian married couples than other couple types. Yet, our findings also suggest that future studies should consider the potential mental and physical health costs, alongside the economic costs, of the burden of intensive care work within lesbian couples. We also found that spousal concordance or discordance in the experience of illness depended on whether individuals were married to a same-sex or different-sex partner—with greater concordance found between same-sex spouses. Our dyadic results concerning concordance in illness constructions correspond to a gender-as-relational paradigm and suggest that spousal concordance/discordance in illness constructions and lived experiences of illness reflect the gender of the patient in relation to the gender of the spouse. Thus, a comprehensive understanding of how illness impacts marital dynamics in gendered ways must take into account the gender of both spouses concurrently.
We go beyond previous work to emphasize that illness is constructed in strongly gendered ways regardless of relational context. Thus, we argue that same-sex marriage does not fully “queer” gendered experiences of illness (Oswald et al. 2005); rather, gender discourses continue to influence constructions of illness, experiences of care work, and marital strain even within same-sex contexts. At the same time, our results suggest that same-sex marriages may be more egalitarian than different-sex marriages around the division of care work, echoing research finding a more equal division of child care, housework, paid work, and efforts to promote healthy behavior within same-sex unions compared to different-sex unions (Kurdek 2005; Prickett, Martin-Storey, and Crosnoe 2015; Reczek and Umberson 2012). Future research should further interrogate the extent of reciprocity and equality in care work across marital contexts.
Limitations
We extend previous research to include married same-sex as well as different-sex couples in our sample and to analyze qualitative dyadic data. However, our sample is limited in potentially important ways that should be addressed in future studies. First, findings are likely to differ for other birth cohorts; these midlife respondents came of age in an era of greater discrimination against sexual minorities and with little hope of ever being able to legally marry. Such constraints may have influenced how partners interacted and cared for each other—in ways that we are unable to discern. Second, men and women tend to describe experiences in ways that conform to gender norms and expectations (Schwalbe and Wolkomir 2001), which may not accurately reflect their actual behaviors. Our use of dyadic data begins to address this concern by including both partners’ reports of their behavior, but future research that also includes observational data (Umberson et al. 2015a) can better address this concern.
Third, this is a purposive sample with most of the same-sex couples recruited through vital records and most of the different-sex couples recruited through referrals from same-sex couples and other recruitment strategies. However, this approach of overlapping social networks for same-sex and heterosexual couples is a strength of our study design in that it promotes social, economic, and geographic comparability across union types, giving us greater confidence that our results are due to relational differences rather than background differences and likely results in understating differences in our key findings.
Fourth, our methods may be limited by retrospective bias; respondents may be describing past events as more negative or positive in retrospect than they would have if interviewed at the time of the illness. In addition, the illnesses that respondents report on vary in severity and duration. However, recent quantitative research suggests that similar gendered patterns of care work in relation to a spouse’s illness are robust when taking into account illness severity (Umberson 2015). Future studies should consider how illness constructions relate to biological reality (Timmermans and Haas 2008) as indicated by objective measures (e.g., biomarkers) of seriousness.
Conclusion
Overall, our findings suggest that same-sex couples may experience less stress around illness and care work and be more likely to receive the kind of care they desire, even as the nature of that care differs for men and women in same-sex marriages. Investigating how same-sex spouses care for each other during a spouse’s illness and how this compares to different-sex couples is key to developing health policies and clinical strategies to best support the health of gay, lesbian, and heterosexual patients and their spouses. This is especially important given health disparities characterizing gay and lesbian populations, including higher rates of breast cancer, AIDS, respiratory disease, and other chronic conditions (Cochran and Mays 2007; Fredriksen-Goldsen et al. 2013; Institute of Medicine 2011).
Given the clearly documented benefits of marriage for health in heterosexual populations (Carr and Springer 2010) and an expected rise in the number of same-sex marriages in the U.S. (Badgett and Mallory 2014), we must begin to consider marital and health processes in same-sex as well as different-sex marriages. Future research should consider the possibility that marriage benefits the health of same-sex spouses even more than marriage benefits different-sex spouses (especially heterosexual women), perhaps because same-sex relationship dynamics are more health-promoting or because those dynamics are especially important to populations exposed to sexual minority stress (Wight et al. 2013). In addition to addressing health disparities of sexual minority populations (Institute of Medicine 2011), the inclusion of same-sex married couples has the potential to shift our thinking about gendered marital and illness dynamics by revealing how gender of the patient in relation to gender of their spouse influences marital and illness experiences. Comparing same-sex and different-sex married couples can transform longstanding assumptions about gender and marital dynamics that have been based on decades of research on heterosexual couples.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported, in part, by an Investigator in Health Policy Research Award to Debra Umberson from the Robert Wood Johnson Foundation and by grant R21AG044585 from the National Institute on Aging (PI, Debra Umberson); grant R24 HD042849 awarded to the Population Research Center at The University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development; and grant 5 T32 HD007081, Training Program in Population Studies, awarded to the Population Research Center at The University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.