
Abstract
Research from the United States has supported two hypotheses. First, educational gaps in health widen with age—the cumulative (dis)advantage hypothesis. Second, this relationship has intensified across cohorts—the rising importance hypothesis. In this article, we used 23 waves of panel data (Socio-Economic Panel Study, 1992–2014) to examine both hypotheses in the German context. We considered individual and contextual influences on the association between education and health, and we assessed gender differences in health trajectories over the life course (ages 23 to 84) and across cohorts (born between 1930 and 1969). For women, we found no support for either hypothesis, as educational gaps in self-rated health remained stable with age and across cohorts. Among men, we found support for both hypotheses, as educational gaps in self-rated health widened with age and increasingly in newer cohorts.
Keywords
Education is one of the most important predictors of health and mortality. Beneficial effects of education on health are transmitted via work environments, economic means, social support, and health behaviors as well as the abilities to self-regulate and to cope with stressors (Mirowsky and Ross 2003). Over the past decades, the relationship between education and health has been intensely studied and found to be pronounced in all advanced societies (Mackenbach 2012).
This picture becomes less clear when viewed from a life course perspective. Do the health benefits of education increase over the life course, do they remain stable, or do they decrease? Initial studies on this question yielded contradictory findings of divergence, persistence, or convergence over the life course (Clark and Maddox 1992; House et al. 1994; Ross and Wu 1996). The puzzle was later resolved in research that considered cohort patterns and their interactions with age and education as well as selective attrition and mortality (Lynch 2003). Studies that addressed these factors found that educational gaps in health increased over major stages of the adult life course—a result that analysts have interpreted as support for the cumulative (dis)advantage hypothesis (Willson, Shuey, and Elder 2007). Moreover, this life course divergence was found to intensify across cohorts, a result that has been termed “rising importance of education for health” (Goesling 2007; Mirowsky and Ross 2008).
The findings on cohort differences revealed how educational differences in health trajectories are shaped by social conditions. Yet, the importance of context is still not widely recognized. This neglect is reflected in the near absence of cross-national research on health inequality over the life course. Pertinent studies are almost exclusively based on U.S. data.
The present study examines the cumulative (dis)- advantage hypothesis and the “rising importance” hypothesis in the German context. We address individual and contextual influences on the association between education and health, viewing it (1) from a life course perspective considering individual age-related change, (2) from a cohort perspective considering sociohistorical change, and (3) through a gendered lens considering how structural forces may differentially shape men’s and women’s health across their life courses.
Health inequality in Germany is shaped by opposing forces. On the one hand, Germany’s educational system inhibits social mobility and strongly determines socioeconomic positions in later life (Allmendinger 1989). This setting appears to be conducive to the accumulation of initial advantages and disadvantages. On the other hand, the German welfare state aims to alleviate resulting inequalities, comprising various measures that might inhibit divergence in educational health trajectories. In light of these contrasts, the German setting can shed new light on both hypotheses.
Background
The Cumulative (Dis)advantage Hypothesis
According to the cumulative (dis)advantage perspective, initial advantages or disadvantages associated with structural positions accumulate over time. Advantages and disadvantages are usually defined in terms of access to resources and exposure to risks (Dannefer 2003; DiPrete and Eirich 2006; Ferraro, Shippee, and Schäfer 2009; O’Rand 1996). The concept of cumulative (dis)advantage has informed various analyses of changing inequality. An assumption that underlies these analyses is that by the mechanisms of accumulation and path dependency, inequality increases within a cohort that is followed over time (Dannefer 2003).
Life course research on education and health is rooted in this tradition. It emphasizes that educational differences in resources and risks translate into health consequences as people age. In young adulthood, higher- and lower-educated people are generally healthy, and disparities in health-relevant factors have not yet taken their toll (House et al. 1994; Ross and Wu 1996). With age, differences in physical activity, for example, gradually translate into differences in health measures, such as overweight, joint problems, and number of chronic conditions (Ross and Wu 1996). This applies similarly to various health-related factors. Because of their lack of resources, lower-educated individuals are not only more exposed to health risks but also more vulnerable to the adverse consequences of these risks. Higher-educated individuals, in contrast, are not only less exposed to health risks but also in a better position to compensate for their adverse effects on health. Life course studies of health inequality have argued that these differences translate into an intracohort increase in the health gaps between lower- and higher-educated people across the major life stages (Lynch 2003; Mirowsky and Ross 2008; Ross and Wu 1996; Willson et al. 2007).
In previous studies on health inequality, a widening gap between health trajectories with age is commonly interpreted as evidence for the cumulative (dis)advantage hypothesis (Brown et al. 2016; Herd 2006; Kim 2008; Lynch 2003; Mirowsky and Ross 2008; Ross and Wu 1996; Willson et al. 2007). In keeping with this literature, the current study also examines the cumulative (dis)advantage hypothesis on the basis of aggregate-level health trajectories. It is important to note, however, that an aggregate-level pattern of widening health gaps between educational groups does not necessarily emerge from processes of accumulation at the individual level (Dupre 2007). Conversely, an absence of this pattern does not necessarily indicate the absence of such processes at the individual level. In light of these complications, caution is warranted about conclusions regarding the mechanisms underlying aggregate-level health trajectories (Bask and Bask 2015).
Pioneering research on educational inequality in health trajectories produced mixed findings. Some studies were consistent with the cumulative (dis)-advantage hypothesis, reporting the expected age-related increase in health differences between educational groups (e.g., Ross and Wu 1996). Others found that educational health gaps remained stable or even narrowed with age (e.g., Clark and Maddox 1992; Herd 2006; House et al. 1994). These contradictory findings fueled an intense debate. An important conclusion to emerge from this debate was that cross-sectional or short-term longitudinal data are ill suited to examine health trajectories of educational groups. Only longitudinal data allow the analysts to account for two potential sources of bias: selection effects and cohort effects (Lynch 2003; Noymer, Beckett, and Elliot 2001).
Two types of selection effects—attrition due to health problems and premature mortality—may compress the estimated health differences between educational groups (Noymer et al. 2001). Whereas higher rates of attrition among the lower educated constitute a bias in the data, higher rates of mortality among the lower educated have been reconsidered as a substantive outcome of a process of cumulative (dis)advantage. Given that death in older age typically ends a trajectory of steep physical health decline (Hayward and Sheehan 2016), educational differences in mortality constitute a part of the phenomenon under study (Dupre 2007; Ferraro et al. 2009; Lynch 2003; Rohwer 2016; Willson et al. 2007). This means that divergence in educational health differences might be compressed or even replaced by convergence, although this aggregate-level pattern may still result from individual-level processes of accumulating (dis)advantages.
A second potential source of bias is cohort effects. Studies that ignore cohort effects implicitly assume that health trajectories remain unchanged across cohorts. This assumption appears unwarranted, given that health-relevant conditions surrounding individuals from different birth cohorts have changed considerably. In the United States, several studies have addressed this problem, using panel data to disentangle age and cohort patterns in the relationship between education and health. These studies consistently found that health gaps between educational groups widened with age (Kim 2008; Lynch 2003; Mirowsky and Ross 2008; Willson et al. 2007).
Recent research from the United States further pointed to gender differences in processes of cumulative (dis)advantage. The intersection between gender and social stratification creates different contexts for men’s and women’s health trajectories (Pudrovska 2014). According to the “reinforcement-of-advantage” hypothesis (also known as “resource multiplication” hypothesis), men translate education more effectively into economic advantages and disadvantages, along with their beneficial or adverse effects on health (Ross and Mirowsky 2006, 2010). Consequently, educational gaps in health are expected to grow faster among men.
A competing perspective posits that educational health gaps accumulate more rapidly among women. According to the “resource substitution” hypothesis, education may improve women’s health more than men’s health because women can draw on fewer alternative socioeconomic resources (Ross and Mirowsky 2010). An additional argument highlights differential socialization. In their roles as future mothers, women are socialized to be more attentive to health matters (Reczek and Umberson 2012). In this process, education determines their capacity to understand health-relevant information, implement it into daily life, and thus, maintain good health (Pudrovska 2014).
Evidence from the United States has supported the latter perspective, indicating a stronger increase in educational differences among women in physical impairment (Ross and Mirowsky 2010) and mortality (Pudrovska 2014). Moreover, educational gaps in self-rated health (SRH) have been found to widen more rapidly among women over the past decades (Liu and Hummer 2008).
The Rising Importance Hypothesis
Demographic research has shown that educational disparities in health and mortality increase over time (Lauderdale 2001). These results reverberated through the U.S. literature in medical sociology, leading to the formulation of the rising importance hypothesis, which states that the rate at which health trajectories diverge across educational groups has increased in newer cohorts (Mirowsky and Ross 2008). U.S. studies have supported this hypothesis (Lynch 2003; Mirowsky and Ross 2008).
The rising importance hypothesis is based on two arguments. Each of these arguments highlights changes that are specific to the U.S. context. The first focuses on change in the distribution of health-related resources, such as material means and health behaviors. In the United States, the relationship between education and income has intensified (Hout 2012). In the absence of welfare state intervention, quality of living, exposure to stressors, and access to health care are highly dependent on financial means (Lynch 2006). Through this pathway, growing educational differences in income may have increased health gaps in more recent cohorts (Goesling 2007).
The relationship between education and health-related behaviors has also intensified. Following the epidemiologic transition from infectious to chronic diseases from the 1960s onward, the stock of information about health and preventive behaviors has expanded greatly. Higher-educated individuals in the United States have not only disproportionally improved their health behaviors by optimizing their diet, exercising more, and smoking less but have also taken more advantage of new health services and medical technology (Lleras-Muney and Lichtenberg 2002).
The second argument emphasizes compositional change and selection. With educational expansion and upward social mobility, the group of lower-educated individuals is shrinking. As a result, lower-educated groups might represent an increasingly negative selection of individuals on characteristics such as early health condition, cognitive ability, and sense of control (Haas 2006).
The German Context
Knowledge about how educational differences in health trajectories change with age and across cohorts remains almost exclusively limited to the U.S. context. From a cross-national perspective, it is important to consider whether the social forces that have shaped health trajectories within the U.S. context apply to a lesser, similar, or greater extent in other countries. For the West German context of the present investigation, extant research suggests marked differences compared with the United States. These differences concern all key arguments on which the hypotheses of cumulative (dis)advantage and rising importance are based.
Cumulative (dis)advantage of education for health in Germany
The educational system strongly connects social origin to social destination both in the United States and in Germany, but the role of education as a “sorting machine” is particularly salient in the German context. Germany is a textbook example for a selective and rigid school system, which translates educational degrees into occupational positions. These conditions favor the reproduction of initial advantages and disadvantages related to social origin and stratify economic outcomes over the life course along educational lines (Allmendinger 1989).
These properties are mainly attributed to early educational tracking and the strong vocational orientation of education. Based on their performance in the fourth grade, children are tracked into three hierarchically structured educational pathways: lower secondary (Hauptschule), intermediate secondary (Realschule), and higher secondary (Gymnasium). Because performance at this young age highly depends on learning environments in families, early tracking strongly reproduces initial advantages and disadvantages of family background and exacerbates initial differences in cognitive ability, self-regulation, and economic means, suggesting pronounced accumulation of health-relevant resources in early life.
These early disparities are intensified by the vocational orientation of the German educational system and its close connection to the labor market (Shavit and Müller 1998). In contrast to the United States, where employers focus more on performance on the job (Daly, Büchel, and Duncan 2000), vocational qualifications are crucial for attaining occupational positions in Germany (DiPrete et al. 2017). Moreover, occupational mobility over the life course is exceptionally low in Germany. Throughout their working lives, individuals remain exposed to favorable or unfavorable working conditions associated with higher or lower occupational positions (Mayer 2009).
Compared with the United States, these characteristics of the German educational and occupational systems create an even more fertile breeding ground for the accumulation of initial advantages and disadvantages in health-related resources. The reverse picture, however, emerges for the remaining arguments behind the cumulative (dis)advantage hypothesis, which fit more closely with the U.S. context. These arguments pertain to inequalities in the labor market, in protection against risks, in access to and quality of health care, and in health behaviors.
Regarding labor market factors, U.S. studies have highlighted material means as a driving force of increasing health inequality over the life course (Lynch 2006). Less attention has been devoted to the fact that the link between material means and health is tightened by institutional characteristics that are specific to this context. In the United States, the welfare state provides only basic social protection (Social Security program) and offers access to health care (Medicare) only after the age of 65. Given the low levels of social protection against risks across major stages of the adult life course, level of living, access to health care, and the degree of stress associated with negative life events strongly depend on individuals’ material means. Moreover, the distribution of these resources is highly unequal, rendering those who are most susceptible to adverse events unable to respond.
In Germany, income inequality between educational groups is considerably smaller (Freeman 1994), and income is less strongly linked to health (T. Klein and Unger 2001). The German welfare state ensures a comparatively high standard of living regardless of economic means. Furthermore, employment protection is strong, payments in case of unemployment or long-term sickness or disability are generous (DiPrete 2002), health insurance is mandatory, and access to health care is universal.
Finally, educational gaps in health behaviors and related competencies are also more pronounced in the United States than in Germany. Highly educated individuals in the United States lead much healthier lifestyles than their lower-educated counterparts. These differences in smoking, physical activity, and preventive health care are smaller in Germany (Cockerham et al. 1986; Pampel et al. 2015).
Consideration of these factors suggests that the life course pattern implied by the cumulative (dis)-advantage hypothesis—a steady increase of educational health disparities—may apply less to the German context. Unlike in the United States, where policy measures aimed at reducing health disparities are implemented only in older age, the German welfare state targets health inequality throughout adulthood.
Empirical evidence from Germany seemingly supports this view. No divergence was found in health trajectories between educational groups (Knesebeck 2005; Schöllgen, Huxhold, and Tesch-Römer 2010). These results, however, are based on cross-sectional data. As noted, if health gaps increase with age—a pattern implied by the cumulative (dis)advantage hypothesis—and if this divergence intensifies across cohorts—a pattern implied by the rising importance hypothesis—these processes may offset each other in an estimation that does not separate age and cohort effects.
Rising importance of education for health in Germany
U.S.-based formulations of the rising importance hypothesis emphasize two factors: increasing inequality in health-related resources and compositional change of educational groups. With regard to the first factor, the United States has witnessed a steep rise of inequality in economic returns to education. In Germany, this trend was less pronounced, albeit still present. Compared to people born before and during the war, postwar and baby boom cohorts have experienced declining returns to education in terms of income and job security (Boockmann and Steiner 2006). These changes were most pronounced among the lower educated, whereas the higher educated maintained comparatively high and stable educational returns.
Unlike in the United States, however, these changes in the distribution of economic resources have not been accompanied by growing educational disparities in health-related behaviors (Pampel et al. 2015). Educational differences in smoking, drinking, physical exercise, and obesity have remained stable. A slight increase of educational differences in these behaviors was found only in the most recent cohorts (Kroll 2010).
The second factor motivating the rising importance hypothesis—compositional change of educational groups—fits more closely with the German context. Unlike in the United States, where size and composition of higher as well as lower educational groups have changed considerably across cohorts, this trend was largely one-sided in Germany. Higher education expanded only modestly, and mainly among postwar cohorts. After this initial increase, the share of tertiary degrees has settled down at approximately 20% (Solga 2002)—compared to about 40% in the United States (Goldin and Katz 2009). In contrast, the group of lower-educated individuals (i.e., up to lower secondary degrees with vocational training) shrank dramatically from over 70% in prewar cohorts to about 20% among those born in the 1970s (Solga 2002). Since the 1980s, intermediate and, increasingly, higher secondary degrees became a requirement for accessing most vocational tracks in Germany (M. Klein 2011). The group of those who fail to attain these degrees is increasingly composed of the most disadvantaged people in terms of family background, cognitive skills, and other health-relevant resources. The group of higher educated, in contrast, has changed little in these respects (Jürges, Reinhold, and Salm 2011).
These considerations suggest that although the basic expectation of “rising importance” applies in both societies, the social forces driving this change are different. In the United States, the rising importance of education for health has been primarily attributed to increasing advantages among the highly educated, such as growing economic returns and disproportionate improvements in health behaviors. Slower health declines in this group can be expected to drive the process of rising importance.
In Germany, cross-cohort trends suggest the reverse pattern: whereas the higher educated have not changed much in their educational returns, health behaviors, and compositional characteristics, the lower educated have experienced declines in returns to education and become more negatively selected on health-relevant characteristics. The rising importance of education for health should therefore result from steeper health declines among the lower educated rather than flatter health declines among the higher educated.
Gender differences in the German context
In U.S. studies, educational health gaps were found to grow faster among women (Pudrovska 2014; Ross and Mirowsky 2010). Compared with the United States, Germany offers two contrasts. First, the resource substitution hypothesis—which has been supported in the United States—is less applicable to the life courses of German women. Hypergamy has long been the norm, weakening the link between women’s level of education and their social position. Moreover, after motherhood, most women either left the labor force for good or returned only on a part-time basis. Both of these characteristics constitute pathways through which German women were able to compensate for a lack of education.
Second, the reinforcement-of-advantage hypothesis—which has not been supported in the United States—fits closely with the life courses of German men. This applies especially to two critical links between education and health: labor market outcomes and health behaviors (Boockmann and Steiner 2006). The German welfare state has long been organized around a male-breadwinner model that encourages gender specialization by combining tax incentives with low coverage of public childcare (DiPrete 2002). As a result, the labor market factors highlighted by the cumulative (dis)advantage hypothesis apply more strongly to men’s than to women’s life courses in Germany. The same is true for risky health behaviors. In this domain, educational differences are much larger among men. In smoking prevalence, the gap amounts to 26 percentage points among men (30% of high-educated and 56% of low-educated Germans smoke), compared to only 8 percentage points among women (20% vs. 28%; Pampel 2010).
Data and Methods
Sample
Our analysis was based on data from the German Socio-Economic Panel Study (SOEP), a large-sсale study of individuals and households (Wagner, Frick, and Schupp 2007). In 1984, the SOEP started in West Germany with a sample population of approximately 12,000 individuals living in 6,000 households. Since 1992, the SOEP has collected data about SRH at each annual wave (except for 1993). Our analysis drew on these data from an observation period between 1992 and 2014, yielding up to 21 measurements of SRH per individual.
In 1992, the anchor year of our study, the sample comprised 13,397 individuals. We restricted this sample to West Germans, excluding immigrants (n = 2,204) and persons who lived in the German Democratic Republic before unification in 1990 (n = 4,349). These sample restrictions ensured that individuals shared a common context with regard to educational degrees, returns to these degrees, and life conditions associated with cohort membership. We further excluded persons who were born before 1930 or after 1969 (n = 2,050). Most men born before 1930 were enlisted to fight in the war and might constitute a selective group of survivors. The upper bound of 1969 marked the end of the baby boom cohort. Finally, we removed respondents without information on education (n = 8). After all restrictions, our analytic sample consisted of 4,786 individuals ages 23 to 62 in the anchor year of 1992, comprising 72,169 person-years across the observation period between 1992 and 2014.
Our data combined a large range of cohorts with an extensive window of observation. A benefit of these data was that they allowed for two types of analyses. The approach first was a model in which linear change across cohorts was interacted with age and education. This approach has been used in previous analyses of the cumulative (dis)advantage hypothesis (Willson et al. 2007). The second approach were models in which educational health trajectories were analyzed for different groups of cohorts, which were separated on theoretical grounds.
Measures
Measures of cohort
Given the large age overlaps between cohorts in our sample, our data allowed us to examine linear as well as nonlinear patterns of change. For the linear cohort model, we centered birth year at the mean age of entry, equaling zero for those who were initially observed at the age of 41 in the year 1992 (i.e., born in 1951). Higher values of this cohort variable denote older cohorts.
For the analysis of cohort categories, we assigned respondents to four theoretically meaningful groups: (1) prewar cohort, born between 1930 and 1939; (2) war-and-postwar cohort, born between 1940 and 1949; (3) economic-wonder cohort, born between 1950 and 1959; and (4) baby boom cohort, born between 1960 and 1969.
Those in the prewar cohort spent their childhood before and during the war. At this time, Germany’s economy was relatively stable, schools were opened, and most children did not live in poverty. After the war, however, this cohort experienced severe food shortage, poor living conditions, and a lack of medical care. Although those in the prewar cohort were born too early to benefit from educational expansion, labor market conditions during their young adulthood were favorable, as the German economy recovered quickly. Members of this cohort spent most of their working lives during a time of exceptional economic growth between the late 1940s and the mid-1970s. The prewar cohort benefited from this “economic wonder” (a term coined by the Times in 1950), sharing a relatively high standard of living across all educational levels (Boockmann and Steiner 2006).
Those in the war-and-postwar cohort were affected by the turmoil of the war at younger ages. Many newborns and small children died or suffered severe sicknesses. From 1948 onward, however, survivors from this cohort were living under the favorable conditions of the economic wonder, entered a booming labor market, and experienced stable working lives. Many of the war-and-postwar babies remained lower educated, however, as educational expansion started only in the 1950s. Due to traditional gender roles in the West German context, the large majority of people born in prewar and war-and-postwar years adopted the male breadwinner–female homemaker model.
The economic-wonder cohort grew up under favorable conditions. Compared with preceding cohorts, these individuals were not only healthier during childhood but also more likely to grow up in stable, two-parent families. They were also the first to benefit from educational expansion on a larger scale. Yet, the booming economy surrounding the time of their birth had changed considerably when the economic-wonder cohort entered the labor market. The oil crisis of 1973 marked the beginning of unstable economic times in Germany. Compared to prewar and war-and-postwar cohorts, returns to education declined across all levels and particularly among the lower educated (Boockmann and Steiner 2006).
Those in the baby boom cohort spent their childhood during a time of economic stability and benefited from further educational expansion, especially at intermediate vocational levels. Yet the downsides of belonging to an “oversized” cohort coupled with the economic crisis of the 1970s resulted in less favorable conditions on the labor market, as economic returns to lower education declined further (Boockmann and Steiner 2006). An important shift compared to preceding cohorts was that women’s labor force participation surged among the baby boomers, increasingly replacing the male-breadwinner model by dual-earner arrangements.
Measure of health
SRH is regarded as a particularly useful measure of health (Idler and Benyamini 1997) in life course studies, as it captures differences in health at any age. For this reason, it has been widely used in previous studies on educational differences in health trajectories (Lynch 2003; Mirowsky and Ross 2008; Willson et al. 2007). In the SOEP, data about SRH are based on the annual survey question, “How would you describe your current health?” Respondents answer on a scale from 1 (“very good”) to 5 (“bad”). We reverse-coded this variable so that lower values indicated worse health.
Measures of age
Age was measured in years, ranging from 23 to 62 in the anchor year of 1992 and increasing up to 84 across the observation window. In the linear cohort model, we centered the age variable at the grand median of 49 years. In the categorical cohort model, age ranged from 53 to 84 in the prewar cohort, from 43 to 74 in the war-and-postwar cohort, from 33 to 64 in the economic-wonder cohort, and from 23 to 54 in the baby boom cohort. For this model, we centered age at the minimum of each cohort. Table 1 presents descriptive statistics for the total sample and separately by the four cohort groups.
Descriptive Statistics: Total Sample and Separately by Cohort.
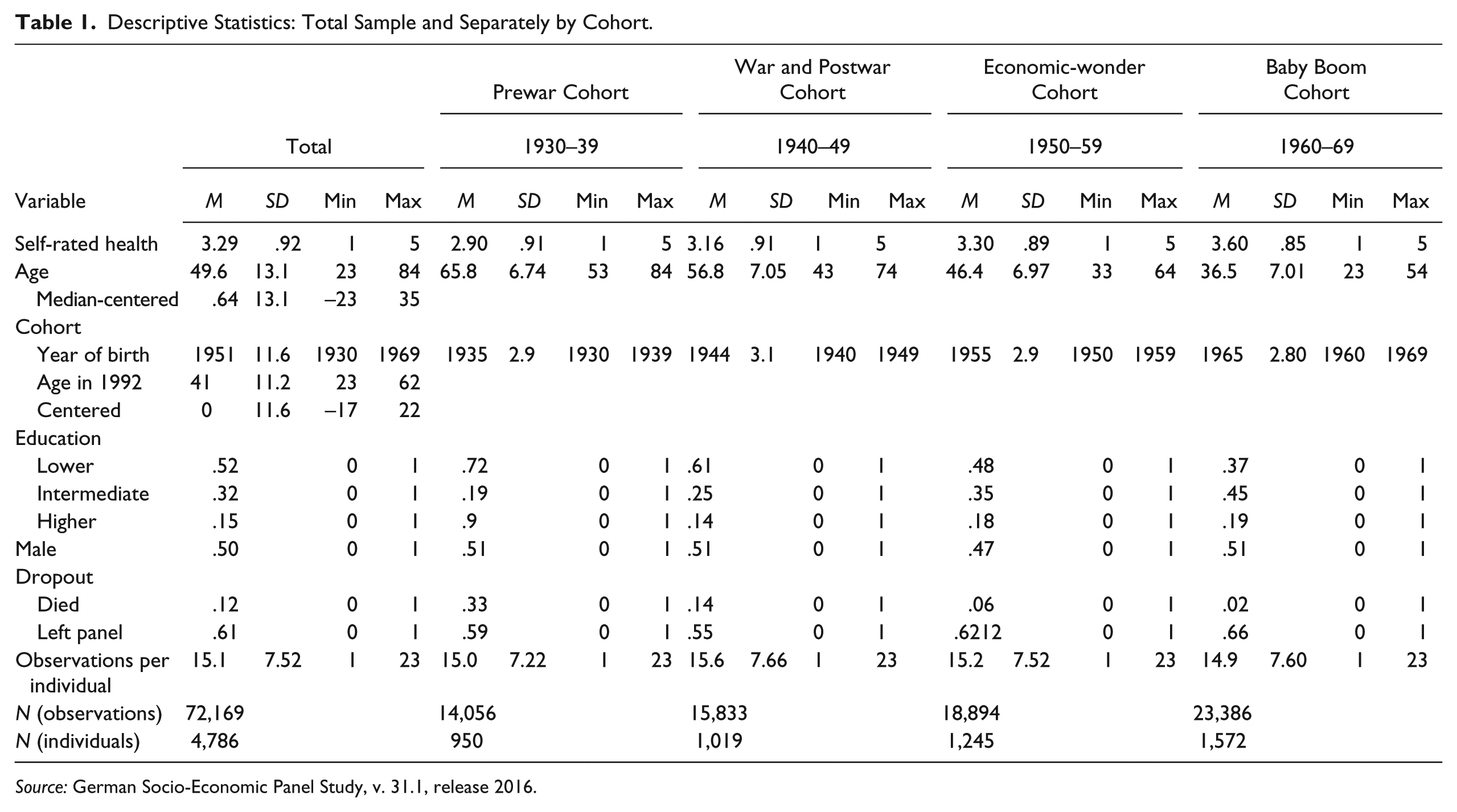
Source: German Socio-Economic Panel Study, v. 31.1, release 2016.
Measures of education
In the German context, institutional characteristics, such as entry requirements in the labor market, render educational degrees and especially vocational qualifications more important than years of schooling for economic outcomes in adult life (Boockmann and Steiner 2006).
We measured educational degrees by the Comparative Analysis of Social Mobility in Industrial Nations (CASMIN) classification. This variable indicates the highest educational degree reported by respondents within the observation period. Figure 1 shows the distribution of educational degrees in the four cohort groups separately by gender. We grouped the CASMIN categories as follows: the bottom category comprised individuals holding lower-secondary degrees with completed vocational qualification or less (CASMIN 1a–1c); intermediate education ranged from intermediate-secondary degrees to higher secondary-degrees with vocational qualification (CASMIN 2a–2c); the top category included respondents holding tertiary degrees (CASMIN 3a–3b).

Distribution of Educational Levels by Cohort.
Controls for dropout
To control for nonrandom dropout associated with poor health, we applied the method suggested by Chen, Yang, and Liu (2010), introducing direct controls for panel attrition. We created two time-constant indicator variables for whether respondents (1) had left the panel or (2) had died before the last wave (2014). Results were similar if the models were estimated without these controls.
Models
We estimated change in SRH using hierarchical linear models (HLM). Our data included up to 23 observations per person, measured at yearly intervals. The HLM estimation accounts for heterogeneity in health trajectories, allowing individual age trajectories to differ in their starting levels (random intercepts) and rates of change (random slopes). The estimation of HLM provided information about mean health trajectories (growth curves) as well as individual variation around the average curves.
An appropriate analytical strategy to estimate change in the relationship between education and health is to account simultaneously for change with age, change across cohorts, and their interactions (Lynch 2003; Mirowsky and Ross 2008; Willson et al. 2007). This approach translates into a model that includes age, cohort, and education as well as twofold and threefold interactions between these variables. Comparable U.S. studies (Lynch 2003; Willson et al. 2007) used linear functions to represent age effects on health. Given that our study was based on a larger window of panel observations, we examined whether higher-level polynomials provided a better representation of age effects on health. According to the Bayesian information criterion, inclusion of four age terms (linear, quadratic, cubic, and quartic) provided the best fit to our data. Regarding interaction effects, we found that model fit improved after including interactions with the linear age terms but declined substantially when we included interactions with age squared, age cubic, or age quartic.
In a second step, we relaxed the assumption of linear cohort effects, replacing the linear cohort variable by a categorical variable distinguishing between the four cohort groups. This approach allowed us to model age trajectories within each cohort and to account for nonlinear change across cohorts. As noted above, there are strong theoretical reasons to expect gender differences in the association between education and health. To gain insight into such differences, we complemented the analysis by separate models for health trajectories of men and women.
Results
In Table 2 we present the results of the linear cohort model for the total sample (Model 1) and separately for the subsamples of men (Model 2) and women (Model 3). For a test of the cumulative (dis)advantage hypothesis, the main interest is in educational differences in the slope of age (Table 2). Positive interaction terms between higher education and age would indicate that age slopes are flatter (i.e., health declines slower) in higher-educated people, as postulated by the cumulative (dis)advantage hypothesis.
Hierarchical Linear Models for Self-rated Health: Total Sample, Men, and Women.
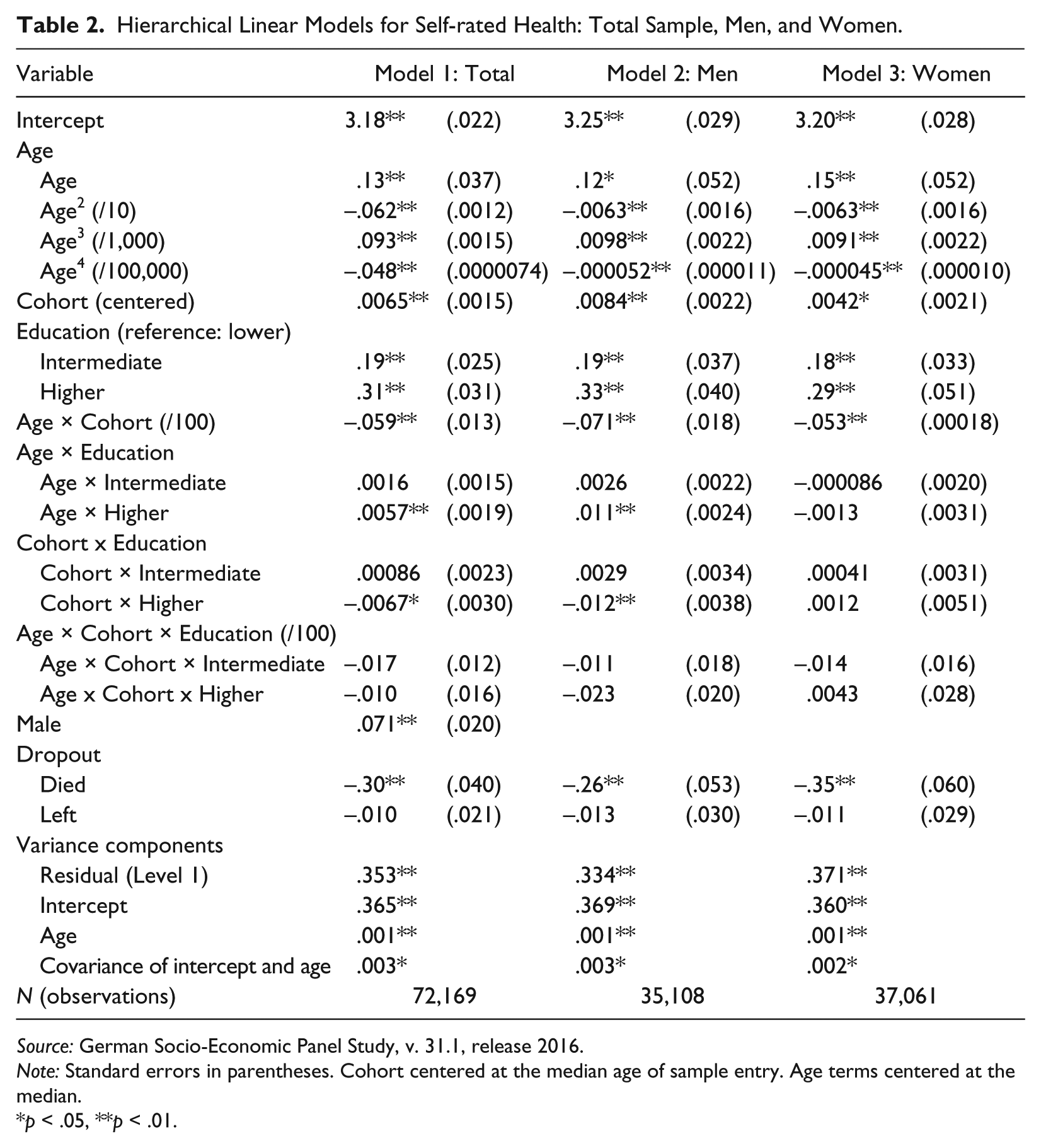
Source: German Socio-Economic Panel Study, v. 31.1, release 2016.
Note: Standard errors in parentheses. Cohort centered at the median age of sample entry. Age terms centered at the median.
p < .05, **p < .01.
For a test of the rising importance hypothesis, the focus is on cross-cohort change in the interactions between age and education. This change is indicated by a three-way interaction between age, education, and cohort. In the models shown in Table 2, the two-way interactions between age and education are defined for the centered cohort variable equaling zero (i.e., for the cohort of 1951). In our specification, higher values of the cohort variable indicate older cohorts. Consequently, a negative three-way interaction between education, age, and cohort would indicate that educational differences in health grow faster in younger cohorts. This is what the rising importance hypothesis predicts.
Results on the Cumulative (Dis)advantage Hypothesis
In Model 1, pertaining to the full sample, the interactions between age and education show that health declines were slower among higher-educated people. This is the aggregate-level pattern of health trajectories that is commonly associated with the cumulative (dis)advantage hypothesis. It contradicts the results of previous cross-sectional studies from Germany (Knesebeck 2005; Schöllgen et al. 2010). Next, we addressed gender differences in separate models for men (Model 2) and women (Model 3). Compared with the full sample, the interaction effect between age and higher education more than doubled in size among men and was absent among women.
Figure 2 illustrates the results for the full sample (left-hand panel), the subsample of men (middle panel), and the subsample of women (right-hand panel). Each graph shows predicted trajectories of SRH for higher- and lower-educated individuals. The curves pertain to the cohort of 1951, as we fixed all covariates at their means. A comparison between the three graphs shows that divergence with age emerged as the overall pattern only because this effect was so strong among men. In the subsample of women, educational gaps in health even narrowed with age, although this convergence was slight and statistically insignificant. Importantly, the absence of divergence in women was due to faster health declines among higher-educated women compared to those of higher-educated men.
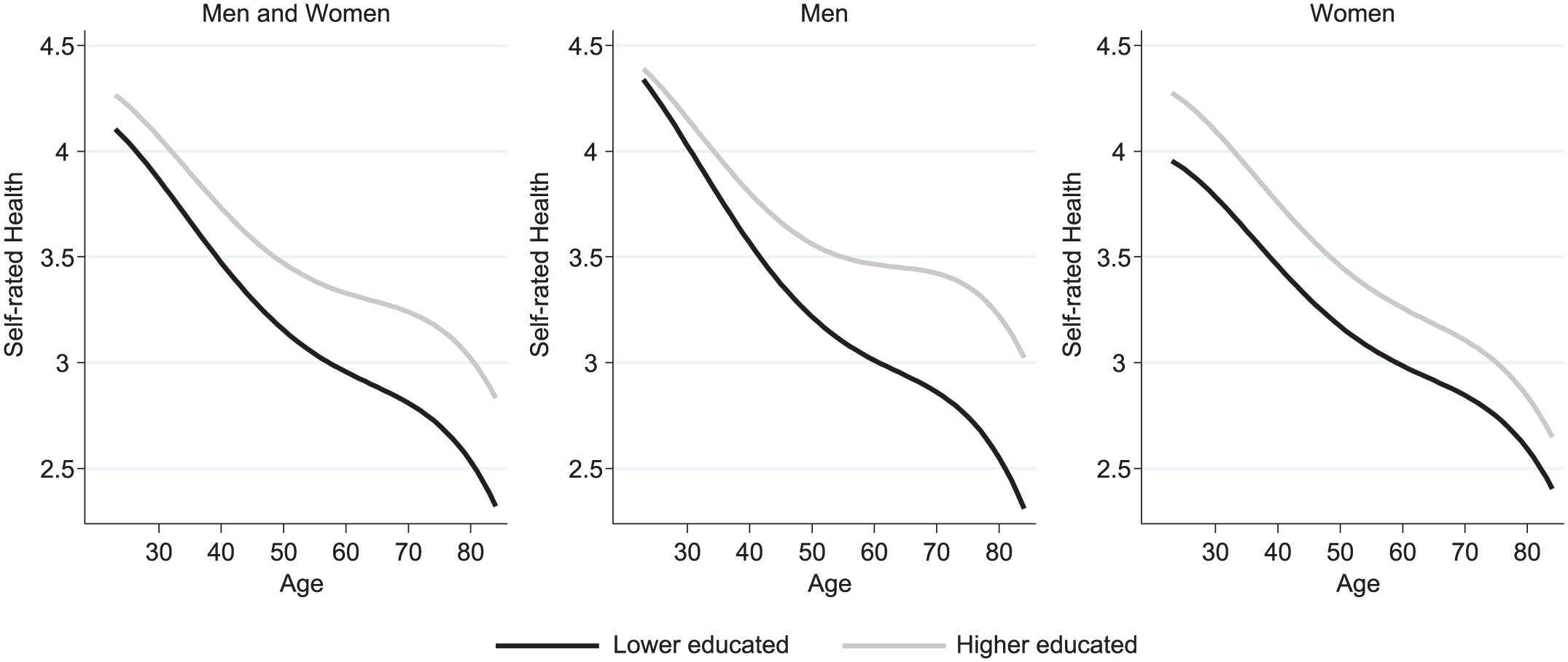
Predicted Trajectories of Self-rated Health: Full Sample, Men, and Women.
Within the subsample of men, the educational health gap widened at a rapid pace. To evaluate the size of this effect, we compared the ages at which educational groups are expected to cross the level of “acceptable” health (i.e., descending below the value of 3). Among lower-educated men, this occurred around the age of 60; among higher-educated men, in their mid-80s—approximately 25 years later in life.
Note that the results shown in Figure 2 are limited to a comparison between higher- and lower-educated people. Figure A1 located in the appendix presents a fuller picture, showing the curves for three educational groups of people holding higher, intermediate, and lower degrees.
Results on the Rising Importance Hypothesis
The second hypothesis guiding the present study postulated that divergence in the health trajectories of different educational groups will intensify across cohorts. Although Model 3 did not indicate divergence among women, these results do not necessarily contradict the rising importance hypothesis, as a linear cohort model might suppress a trend that emerges only among the most recently born. Therefore, we examined women’s health trajectories separately for the four cohort groups, but we found no divergence in any cohort group and generally no substantial cohort differences among women (results not shown). Overall, our results for women were inconsistent with the hypotheses of both cumulative (dis)advantage and rising importance.
For men, in contrast, both hypotheses were supported. In Model 2, the negative sign of the three-way interaction between age, high education, and cohort was consistent with the rising importance hypothesis, indicating that health gaps increased more slowly in older cohorts of men. In Figure 3, we examine the rising importance hypothesis in more detail, comparing health trajectories of the prewar cohort, war-and-postwar cohort, economic-wonder cohort, and baby boom cohort of German men. The model on which Figure 3 is based is shown in Table A1 in the appendix. The figure shows the large overlaps between age and cohort, which allowed us to disentangle their effects. On the basis of these predicted trajectories, we calculated health gaps at the lower and upper bounds of age overlaps between the four cohort groups. Table 3 shows health gaps between higher- and lower-educated men, measured in scale points of SRH, at each of these overlapping ages. The rows of Table 3 show the age-related increase of health gaps within each cohort; the columns show cross-cohort change in the size of these gaps measured at overlapping ages.

Predicted Trajectories of Self-rated Health in Three Cohorts of Men.
Health Gaps between Higher- and Lower-educated Men at Overlapping Ages.
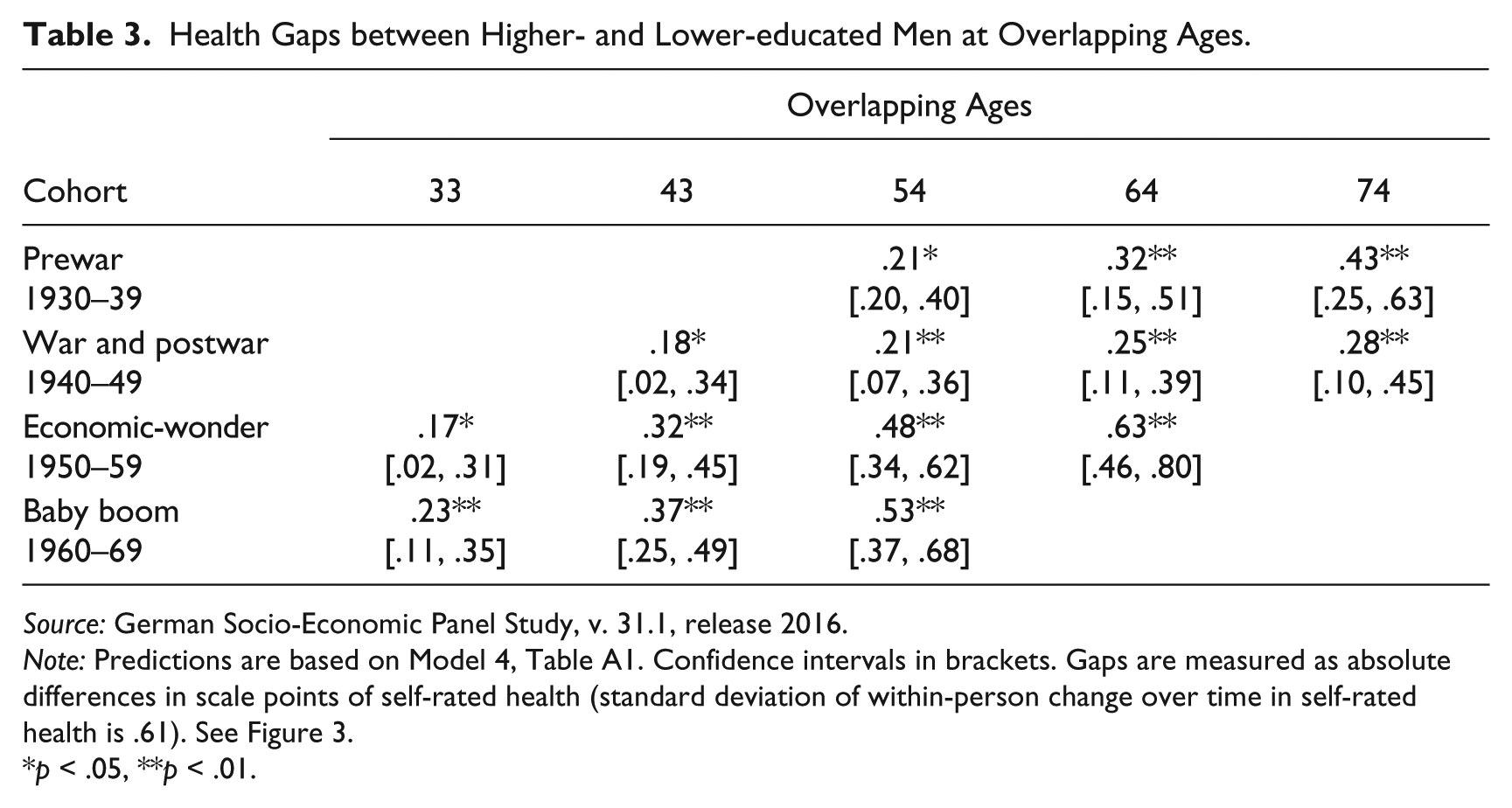
Source: German Socio-Economic Panel Study, v. 31.1, release 2016.
Note: Predictions are based on Model 4, Table A1. Confidence intervals in brackets. Gaps are measured as absolute differences in scale points of self-rated health (standard deviation of within-person change over time in self-rated health is .61). See Figure 3.
p < .05, **p < .01.
With regard to the rising importance hypothesis, Figure 3 and Table 3 show three notable patterns. First, health trajectories between lower- and higher-educated men diverged in every cohort. Second, in line with the rising importance hypothesis, the pattern of divergence was less pronounced in the two older cohort groups (prewar cohort, war-and-postwar cohort) and more pronounced in the two younger cohort groups (economic-wonder cohort, baby boom cohort). Gaps measured at the age of 54, for example, more than doubled from approximately 0.2 scale points in the older cohorts to approximately 0.5 scale points in the younger cohorts (Table 3). Third, this cross-cohort trend was primarily produced by steeper health declines among the lower educated. Lower-educated men who belonged to the economic-wonder cohort fell below the level of “acceptable” health by their mid-50s. In the preceding cohorts of lower-educated men, this occurred approximately 10 years later in life (Figure 3).
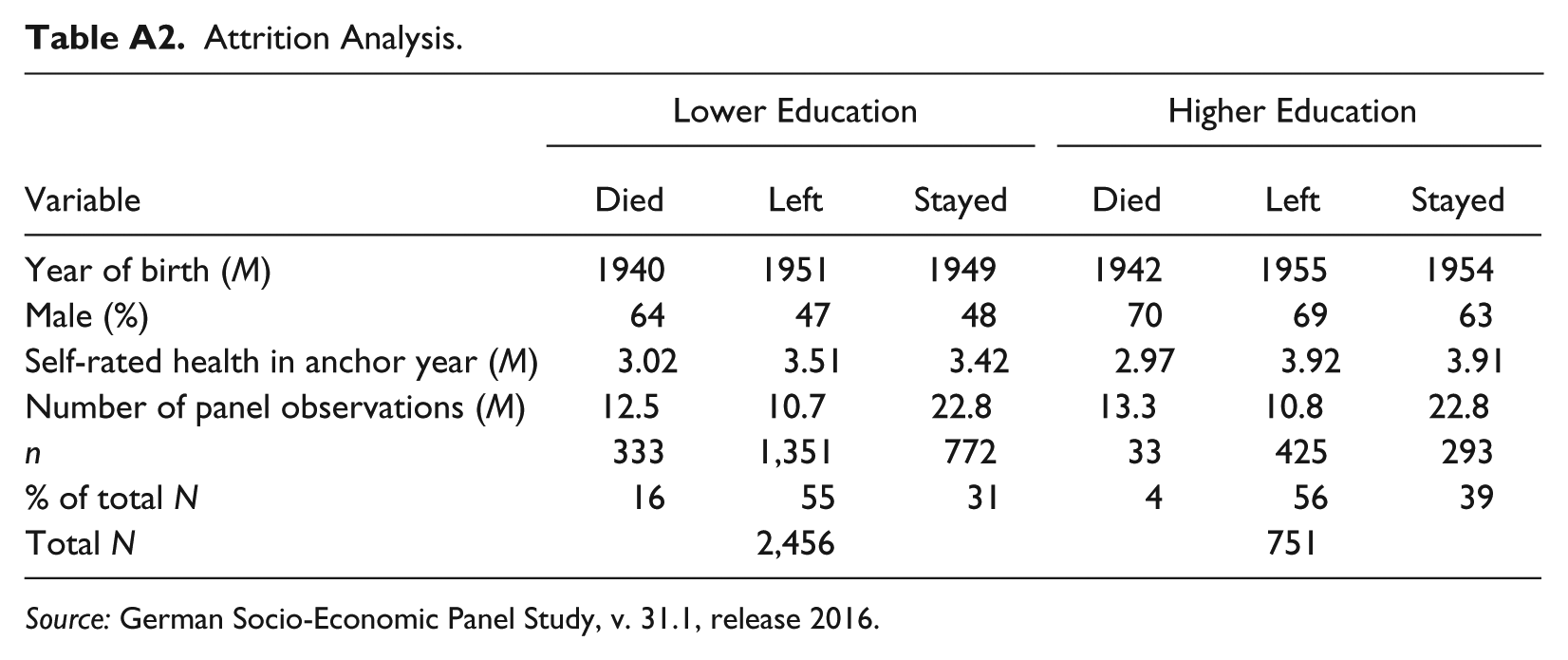
Attrition Analyses
In additional analyses, we examined the extent to which selective panel dropout and mortality might affect our results. Descriptive results based on these analyses are shown in Table A2 in the appendix. As expected, mortality was higher among lower-educated than among higher-educated men. Among lower-educated men, 17.4% died across the observation period; among higher-educated men, 4.6% died. Among women, 9.8% of the lower educated and 4% of the higher educated died. However, only very few deaths (n = 82 or 18% of all deaths) occurred before the age of 54—the highest age at which all four cohorts overlap. Second, the chance of dying before this age barely differed between educational groups. This indicates that our conclusions about cohort differences observed at overlaps up to this age are unlikely to be affected by selective mortality. Furthermore, we examined whether panel dropout for reasons other than death differed across levels of education. These analyses showed, first, that dropout rates were similar for lower- and higher-educated respondents and, second, that baseline levels of health (i.e., at initial observation in 1992) did not differ between those who later dropped out of the panel and those who stayed in the panel until the last observation in 2014. These findings suggest that panel dropout was unlikely to bias the health trajectories found for different educational groups.
Discussion
This study investigated change with age and change across cohorts in the relationship between education and health in Germany. We examined two hypotheses about aggregate-level health trajectories of different educational groups. The cumulative (dis)-advantage hypothesis posits divergence with age, and the rising importance hypothesis posits that this divergence intensifies across cohorts. Our theoretical framework highlighted differences between Germany and the United States—the context most extensively studied in previous research—in terms of health-relevant factors on which these hypotheses are based. These include the role of the educational system in reproducing initial advantages and disadvantages related to social origin and stratifying economic outcomes in later life, the role of the welfare state in targeting the steady increase of educational disparities in health-related resources over the life course, change over time in the distribution of health-relevant resources and the composition of educational groups, and the gendered structure of the life course differentially distributing health-related resources between men and women.
Our analyses offer the first assessment of the cumulative (dis)advantage hypothesis and the rising importance hypothesis in the German context. Compared with previous findings from the United States, our results revealed two notable differences. First, the pattern of divergent health trajectories between educational groups was limited to men. Among women, the rates of health decline did not differ between the higher and the lower educated. These results contrast sharply with U.S. findings indicating that divergence not only pertains to both sexes but is more pronounced among women (Pudrovska 2014; Ross and Mirowsky 2010).
We argued that critical links between education and health—in particular, labor market factors and health behaviors—are tighter among men than among women in Germany. Moreover, women’s resources in our study cohorts were largely determined by their partners’ socioeconomic status, potentially weakening the relationship between women’s education and health. Due to hypergamy, however, this argument would suggest slower health declines among lower-educated women rather than faster health declines among higher-educated women. Our data showed the opposite pattern.
We can only speculate about why higher-educated women did not benefit from their education as much as men did. One possible reason is disadvantages on the labor market and the partner market. Higher-educated women of our study cohorts had lower chances of attaining higher occupational positions and incomes (Sørensen and Trappe 1995). Moreover, unlike their lower-educated counterparts, they were less likely to marry and to reap associated benefits, such as economies of scale and within-household compensation for individual labor market disadvantages (Blossfeld and Timm 2003).
Although our results for women contradict the common interpretation of the cumulative (dis)-advantage hypothesis, they do not imply that the mechanism of cumulative (dis)advantage was absent in women. For example, higher-educated women were already in better health than lower-educated women early in life and kept this advantage across the life course. This may indicate that higher-educated women accumulated health-related advantages early in life (i.e., before our starting age of 23). Alternatively, health selection into education may explain why gaps among women emerged so early. A further possibility concerns gender-specific responses to our outcome measure of SRH. Research has shown that men and women might evaluate their health differently (Benyamini et al. 2003). Moreover, research from the United States has shown educational differences in the reliability of SRH measurements (Zajacova and Dowd 2011). In light of these limitations of our outcome measure, a replication of our analysis on the basis of more objective health measures could shed more light on gender differences in health trajectories.
In research on health inequality, theoretical formulations and empirical tests of the cumulative (dis)advantage hypothesis have often ignored the possibility of gender differences (Kim 2008; Lynch 2003; Mirowsky and Ross 2008; Willson et al. 2007). Our findings show that attention to such differences is warranted, particularly in studies that examine whether evidence from the United States can be generalized to other societies. The opposing patterns found for the United States and Germany point to the role of structural forces that have differentially shaped health trajectories of men and women in these societies.
With regard to the rising importance hypothesis, our results also contrast with those obtained for the U.S. context. The cohort pattern of increasing divergence was limited to men and attributable to steeper health declines among lower-educated men from younger cohorts. We found no cross-cohort differences among higher-educated men. In the United States, in contrast, the rising importance of education for health emerged both for men and women as a combined outcome of slower health declines among the higher educated accompanied by faster health declines among the lower educated of younger cohorts as compared to older cohorts (Mirowsky and Ross 2008).
Again, these differences highlight the potential for comparative research, showing how health trajectories are differentially shaped by the context in which they unfold. In Germany, changes in returns to education and compositional change in health-relevant characteristics were negligible among higher-educated men. Lower-educated men, in contrast, represent a shrinking group in which disadvantage is increasingly concentrated. This group has faced substantial declines in educational returns (Solga 2002). In the United States, increasingly adverse conditions among the lower educated were accompanied by increasingly favorable conditions among the higher educated (Hout 2012). These cross-national differences are broadly consistent with our findings on the rising importance hypothesis. We note, however, that more precision is necessary in future comparative research to unravel whether, and to what extent, the proposed mechanisms have produced the observed patterns.
Considering the rising importance hypothesis, we further note that although we did not find divergent health trajectories in our study cohorts of women, this might change among the more recently born. Especially among women born in the ’70s and ’80s, education became more relevant to various outcomes. Examples are the narrowing gender gap in labor force participation, women’s increasing economic returns to education (Fitzenberger and Wunderlich 2003), and growing differences in risky health behaviors, such as smoking (Pampel et al. 2015). Moreover, the proportion of higher-educated women surged upward in these cohorts, whereas the group of lower-educated women shrank, suggesting increasingly negative selection on health-relevant characteristics. In view of these shifts, we consider it important to explore whether the relationship between education and health has intensified among more recent cohorts of German women.
Although we modeled our study after the designs used in previous studies from the United States, our results are not fully comparable. One limitation is our measure of SRH. Recent research has indicated substantial cross-national differences in how people evaluate their health. For example, the prevalence of chronic conditions is much higher in the United States than in Europe, but U.S. respondents score much higher than Europeans on measures of SRH (Avendano and Kawachi 2014). Moreover, Germans score lower on SRH than many other Europeans even after controlling for chronic conditions and functional limitations (Hardy, Acciai, and Reyes 2014). In light of these differences, caution is warranted about direct comparisons between SRH in Germany and that in the United States, in particular, regarding absolute levels of health, absolute health gaps, and unstandardized effects on health.
In regard to the life course literature on health inequality, the present study is only an initial step in the direction of comparative research on social disparities in health across lives, cohorts, and countries. Future research should extend the comparative scope to include more societies. Longitudinal data for further countries are available, for example, in the Survey of Health, Ageing and Retirement in Europe (SHARE) and in the English Longitudinal Study of Ageing (ELSA), allowing for a comparison of Scandinavian welfare states, central and southern European countries, and the United Kingdom. Adding these countries to the analysis will introduce more variation in the contextual factors shaping health inequality across lives and cohorts, such as educational systems, working conditions, income inequality, healthcare, and social policy.
Footnotes
Appendix
Attrition Analysis.
| Lower Education |
Higher Education |
|||||
|---|---|---|---|---|---|---|
| Variable | Died | Left | Stayed | Died | Left | Stayed |
| Year of birth (M) | 1940 | 1951 | 1949 | 1942 | 1955 | 1954 |
| Male (%) | 64 | 47 | 48 | 70 | 69 | 63 |
| Self-rated health in anchor year (M) | 3.02 | 3.51 | 3.42 | 2.97 | 3.92 | 3.91 |
| Number of panel observations (M) | 12.5 | 10.7 | 22.8 | 13.3 | 10.8 | 22.8 |
| n | 333 | 1,351 | 772 | 33 | 425 | 293 |
| % of total N | 16 | 55 | 31 | 4 | 56 | 39 |
| Total N | 2,456 | 751 | ||||
Source: German Socio-Economic Panel Study, v. 31.1, release 2016.
Acknowledgements
We thank Mel Bartley, Fabrizio Bernardi, David Blane, Hans-Peter Blossfeld, Henriette Engelhardt, Anette Fasang, Juho Härkönen, Rasmus Hoffmann, Tim Huijts, and Hannes Kröger for comments on earlier versions.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Liliya Leopold acknowledges financial support from the German Research Foundation (DFG), Grant No. EN 424/7-1.