
Abstract
Socioeconomic and health disadvantages can emerge early in the life course, making adolescence a key period to examine the association between socioeconomic status and health. Past research on obesity in adolescence has focused on family measures of socioeconomic status, overlooking the role of individual-level nascent indicators of socioeconomic disadvantage. Using measured height and weight from nationally representative data from Brazil, we estimate sibling fixed effects models to examine the independent effects of nascent socioeconomic characteristics—school enrollment and work status—on adolescent overweight and obesity, accounting for unobserved genetic and environmental factors shared by siblings. Results show that school enrollment is associated with lower odds of overweight and obesity. Working is not significantly associated with overweight/obesity risk. However, adolescents not enrolled but working face the highest risk of overweight/obesity. Findings suggest that adolescents face added layers of disadvantage from being out of school, with important implications for the accumulation of health disadvantages.
Brazilian children and adolescents are now among the heaviest in the world due to the recent and rapid growth in overweight and obesity prevalence (IBGE 2010). Projections suggest that Brazil, the fifth most populous country in the world, will surpass the United States in the proportion of overweight and obese children as early as 2022 (Harrod and Mitting 2012). Brazil is also one of the most unequal countries in the world (Besarria et al. 2018), and obesity increasingly affects those with lower socioeconomic status (SES) as the country continues to undergo the nutrition transition (Monteiro, Conde, and Popkin 2001)—a phenomenon present in most middle- and high-income countries, characterized by increases in the consumption of ultraprocessed foods high in saturated fat, sodium, and sugar.
A large body of research has established family SES, such as household income and parental education, as a predictor of adolescent overweight and obesity worldwide, but this research has paid relatively less attention to the role of adolescents’ own socioeconomic characteristics such as their schooling and work status. Although adolescents’ schooling and work experiences are typically tied to their family socioeconomic circumstances, they are not mere extensions of family SES. Instead, they represent nascent indicators of individual SES that provide the foundation for an individual’s eventual adult SES and that may affect adolescent weight status net of family socioeconomic characteristics. Moreover, adolescents’ individual socioeconomic characteristics go beyond the simple possession of or access to resources. Schooling and work experiences also reflect the process of adolescents acquiring resources and status on their own. For example, through the process of schooling, adolescents may gain a greater sense of personal control, which is associated with healthier lifestyles (Mirowsky and Ross 1998). School and work connect adolescents to people, institutions, and experiences and provide routine and a sense of purpose at a formative stage in the life course (Burd-Sharps and Lewis 2018). In contexts such as Brazil, where disparities in school enrollment and work experiences emerge early in the life course, it is important to consider how these two dimensions of adolescents’ individual SES are associated with overweight and obesity. Moreover, in countries like Brazil that are still undergoing the nutrition transition, the associations between various socioeconomic characteristics and overweight and obesity may be changing (Monteiro et al. 2007). Thus, the SES of parents (an older generation) may have different consequences for overweight and obesity than the emerging SES of adolescents (a younger generation). This study, therefore, examines whether and how adolescents’ school and work experiences are associated with overweight and obesity in Brazil.
Research on the association between SES and adolescent weight status typically applies a between-families approach, comparing adolescents from different families. This type of approach is hindered by unobserved heterogeneity, a common data and methodological limitation. For example, disparities in obesity could be due to genetic heritability and other unobserved factors that vary across adolescents from different families. Indeed, much of the variation in body mass index (BMI) can be attributed to genetic vulnerability (Domingue et al. 2014; Seabrook and Avison 2010). This study addresses the problem of unobserved heterogeneity through an analysis of within-family socioeconomic disparities in overweight and obesity. Using a nationally representative data set with anthropometric measures of the height and weight of all household members—information that is rare in large-scale surveys in Brazil and most other countries—we estimate sibling fixed effects models to isolate the independent effects of individual-level socioeconomic characteristics (i.e., school enrollment and work) while controlling for all unobserved neighborhood, family, and genetic traits that are shared by siblings and that are related to overweight and obesity. Although unobserved factors that are not shared by siblings remain, we argue that holding constant shared family and neighborhood characteristics (i.e., parental characteristics, neighborhood crime) approximates a natural experiment. Moreover, despite the genetic heritability of obesity, social contexts such as SES can exacerbate or reduce genetic vulnerability (Boardman et al. 2014; Seabrook and Avison 2010).
The significance of this study is both conceptual and empirical. First, we examine the associations between overweight/obesity with several measures of individual adolescent SES separately from family SES, which to our knowledge, no previous study has done. Brazil provides an opportune setting for studying these relationships because, like many middle-income countries, Brazilian children from lower-SES backgrounds often leave school for work during adolescence, resulting in enough variation in adolescent school enrollment and work status to understand the implications of these intersecting statuses for obesity. Our second contribution is to provide new knowledge about the social stratification processes that give rise to health disparities in adolescence, which has important implications for understanding cumulative inequality over the life course (Seabrook and Avison 2012) because adolescence is a critical life course stage wherein lifelong socioeconomic and health trajectories tend to become established. A third contribution is the use of a within-family methodological approach. This approach represents a significant advancement because past studies have rarely accounted for genetic factors and other unmeasured predictors of obesity that are shared by siblings.
Background
Adolescent Overweight and Obesity in Brazil
Since the 1970s, childhood obesity has increased dramatically in most countries across the world (Ng et al. 2014). In Brazil, the proportion of children considered obese or overweight grew from 3.7% in 1970 to 21.7% in 2009 (IBGE 2010). This shift from a high prevalence of undernutrition to a predominance of overweight and obesity has occurred as part of Brazil’s rapid nutrition transition, in which the country has experienced unprecedented large-scale changes in dietary patterns, characterized primarily by increases in the consumption of ultraprocessed foods (Monteiro et al. 2010; Monteiro, Mondini, and Costa 2000).
The rising rate of obesity in Brazil, especially among children and adolescents, carries serious individual- and population-level health, social, and economic implications. Obesity is associated with a host of chronic conditions, including diabetes, hypertension, and cardiovascular disease, that can lead to work limitations and premature mortality and place large burdens on the health care systems (Centers for Disease Control and Prevention n.d.). In addition, obese children often face social stigma that may have negative psychosocial consequences (Crosnoe and Muller 2004). Obese children also have a higher likelihood of being obese adults (Freedman et al. 2005; The et al. 2010), and thus the health, social, and economic consequences of childhood obesity can persist throughout the life course.
Adolescence is also a critical stage for SES because early markers of individual SES based on school enrollment and work begin to emerge. Disadvantaged children who drop out of school and/or work outside the home may experience a heightened risk of overweight and obesity. Moreover, SES in childhood and adolescence has persistent effects on health disparities throughout the life course (Seabrook and Avison 2012) because disadvantage early in life launches pathways of risk that shape long-term trajectories of health. For all of these reasons, focusing on individual markers of SES in adolescence, such as school enrollment and work, can shed new light on the association between overweight and obesity and SES and the emergence of such an association early in the life course.
Schools and Adolescent Overweight and Obesity
In Brazil and many middle-income countries, obesity was once characterized as a disease of the rich but is now increasingly becoming a burden of the disadvantaged (Monteiro et al. 2007). Among Brazilian adults, a negative educational gradient emerged at the end of the twentieth century whereby higher levels of education are now associated with lower obesity risk. As such, education increasingly contributes to health disadvantages early in the life course. Moreover, educational stratification starts early in the life course among Brazilian children. By adolescence, close to 20% of school-age adolescents are not enrolled in secondary school, and only 55% of all young adults complete secondary school in Brazil (Ministry of Education 2015). “Push-out” factors associated with adolescent dropout in Brazil include poverty, child labor, and adolescent childbearing (Cardoso and Verner 2007). Because children and adolescents who are enrolled spend large amounts of time in school, schools and schooling have the potential to reduce overweight and obesity through a variety of mechanisms.
First, schools have the potential to become settings for promoting healthy habits. For example, children consume at least one of their daily meals in school, and schools can use this as an opportunity to promote healthy eating habits. School feeding programs are the most commonly known school-based food security interventions in low-, middle-, and high-income countries alike, providing food that has the potential to improve the nutrient intake and food security for vulnerable students and students at risk for overweight and obesity. Schools can also implement obesity prevention programs, and evidence from the United States suggests that these programs contribute to lower rates of overweight and obesity among students (Veugelers and Fitzgerald 2005). In Brazil, the role of schools as promoters of healthy nutrition is particularly important given that the country has the world’s oldest and most successful school feeding program, providing daily nutrition to over 43 million children across the country in all public K–12 institutions in the country (World Food Programme n.d.) and offering meals that can be more nutritious than the ones offered at home (Rocha 2009; Silva, Bortolini, and Jaime 2013).
In addition to promoting healthy eating, schools can also offer dedicated time for physical activity, promote knowledge about health behaviors, and structure children’s time throughout the day, which can reduce snacking. Perhaps for these reasons, studies have found that school-age children in the United States gained more weight during summer vacation compared to the school year, suggesting that nonschool environments may contribute more to childhood obesity compared to school environments (von Hippel et al. 2007; von Hippel and Lynch 2014; von Hippel and Workman 2016). Although the school calendar in Brazil is similar to the United States, with a summer and winter break, the role of schools remains unclear for Brazil.
Beyond the school environment, schooling—the process of acquiring education—can change young people’s cognitive orientations in ways that influence healthy behaviors. More years of education are associated with lower probabilities of obesity in adults in high-income countries (Nayga 2000; von Hippel and Lynch 2014). Although the association between education and obesity is partly attributed to the greater economic resources that education affords, such as jobs and income, it is also a function of cognitive skills, such as learned effectiveness and a sense of control, that are acquired throughout the process of schooling (Mirowsky and Ross 1998). Evidence based on natural experiments conducted in Ecuador suggests that when people received opportunities to attend school (through random assignment), the way they perceived and responded to health risks improved (Baker et al. 2011). Education leads people to become more future oriented, more literate about health risks and prevention programs, and better able to evaluate and avoid long-term risks. Other studies find support for the idea that education improves an understanding and avoidance of health risks, including risks related to obesity (e.g., Salinas and Baker 2014). Thus, school enrollment might protect against overweight and obesity because of the promotion of healthy behaviors, the provision of free meals and often more nutritious meals than those provided in most Brazilian homes, and the cultivation of cognitive orientations acquired through schooling.
On the other hand, school enrollment might be associated with higher overweight and obesity risk if school culture and peers promote unhealthy behaviors, such as the consumption of ultraprocessed junk foods that lead to overweight and obesity. A positive association between school enrollment and higher overweight and obesity risk would align with previous research that has found a positive association between education level and overweight/obesity among adults in lower- and middle-income countries (Cohen et al. 2013). However, few studies in middle- and lower-income countries have considered confounding variables when examining the association between education and obesity (Cohen et al. 2013). We examine whether school enrollment acts as a risk or protective factor for adolescent overweight and obesity independent of family SES.
Work and Adolescent Overweight and Obesity
In Brazil and around the world, many adolescents participate in part-time or full-time work at some point during the school year, and an existing literature has aimed to understand the consequences of adolescent work for a number of well-being outcomes (Staff, Messersmith, and Schulenberg 2009). In 2008, around one-fourth of the adolescents ages 12 to 17 in Brazil worked (Barros and Mendonça 2010). Most of the adolescents working are doing so in irregular, or informal work, with no paperwork “carteira assinada” (Barros and Mendonça 2010; Hoek et al. 2009). Among those ages 16 and 17, for example, 70.8% were in irregular situations (Barros and Mendonça 2010).
Although too much intensive work has negative consequences for school attendance (Emerson and Souza 2007), learning (Emerson, Ponczek, and Souza 2017), and health outcomes (for a review, see Staff et al. 2009), the consequences for obesity are not well understood. Almost no literature to date has examined the association between adolescent work status and obesity, so we discuss the potential mechanisms through which adolescent work might affect obesity—eating habits and physical activity, two important determinants of obesity.
Adolescent work has the potential to increase the risk of overweight and obesity through a number of mechanisms. Studies show that working contributes to more time constraints among young adults, leading them to skip some meals or consume preprocessed and ready-to-eat meals, in addition to fast food (Escoto et al. 2012; Pelletier and Laska 2012). These types of meals are likely to be more calorically dense with lower nutritional value than home-cooked meals (Cutler, Glaeser, and Shapiro 2003). Indeed, studies have found a significant association in adults between long hours of work and higher consumption of energy, sugar, and fat in addition to an increasing use of fast food and eating out (Devine et al. 2009; Jones et al. 2007; Wardle et al. 2000). Specifically, work can cut into lunchtime, which in Brazil is the most nutritious and longest meal of the day and is often eaten at home. Work also provides adolescents with their own disposable income, allowing them to purchase their own food outside of the home. Studies have suggested that adolescents’ choices of food away from home are often unhealthy (French et al. 2001).
Work may also affect adolescents’ obesity through its effect on physical activity and sedentary behavior. Because of time constraints arising from juggling school and work, adolescents may be less likely to find enough time to exercise. Adolescent work reduces the amount of leisure time, and one study found that work intensity reduced the likelihood of exercising for adolescents (Bachman and Schulenberg 1993), which could contribute to higher rates of obesity among working adolescents. On the other hand, if the work involved manual labor, it could increase physical activity and thus be associated with lower overweight/obesity risk.
The Intersection of School and Work
It is also important to consider how school and work status interact with each other. One hypothesis is that adolescents who both attend school and work might be at the lowest risk for overweight or obesity. Research shows that there are some benefits of working in adolescence. For example, working a modest amount of hours in addition to attending school is associated with improved academic performance (Mortimer and Johnson 1998; Staff, Schulenberg, and Bachman 2010). Moreover, a study of Brazilian children and adolescents points to the benefits of working part-time while remaining in school for adult earnings (Emerson and Souza 2011).
The benefits of working while attending school might also extend to overweight and obesity risk. Adolescents who both attend school and work might have better time-allocation skills and less unstructured time to engage in snacking or sedentary activity that could lead to overweight and obesity (Schoenhals, Tienda, and Schneider 1998). Furthermore, their combined school and work commitments might also improve their sense of self-efficacy and control, even more so than schooling alone.
Conversely, adolescents who attend neither school nor work might be at the highest risk of overweight/obesity. Disconnection from both school and work increases adolescents’ vulnerability to a host of negative outcomes (Burd-Sharps and Lewis 2018). In fact, the literature on adolescents and young adults who are not in employment, education, or training (NEET) in developing countries suggests that inactivity is the most consequential status for this group, not work. NEET adolescents and young adults have worse outcomes in general than those who are in school and work, with negative prospects later on (OECD 2018). Further research shows that young men who are neither in school nor working are more likely to engage in risky behaviors (Edelman, Holzer, and Offner 2006). This association might extend to obesity because adolescents who neither attend school nor work will have large amounts of unstructured time that could be associated with increased snacking and sedentary activity. For these reasons, it is important to consider how school and work might operate both independently and in tandem to influence overweight/obesity risk among adolescents.
In the present study, we test two sets of competing hypotheses to determine whether school and work status serve as risk or protective factors for adolescent obesity and a third hypothesis to test whether school and work status interact to shape adolescent obesity.
Hypothesis 1: School
Hypothesis 1a: School enrollment will be associated with lower odds of overweight and obesity among Brazilian adolescents.
Hypothesis 1b: School enrollment will be associated with higher odds of overweight and obesity among Brazilian adolescents.
Hypothesis 2: Work
Hypothesis 2a: Work will be associated with lower odds of overweight and obesity.
Hypothesis 2b: Work will be associated with higher odds of overweight and obesity.
Hypothesis 3: School and Work Interaction
Hypothesis 3: Adolescents who neither work nor are enrolled in school will have the highest obesity risk.
Data And Methods
Data
We used data from the 2003–2004 and 2008–2009 Pesquisa de Orçamentos Familiares (POF) Household Expenditure Survey to assess the influences of adolescent socioeconomic conditions on overweight and obesity. The POF is a nationally representative household survey conducted by the Brazilian Census Bureau (Instituto Brasileiro de Geografia e Estatística). A probability-based, stratified, multistage data set, the POF follows a three-step probabilistic sampling procedure based first on counties, then census tracts within counties, and finally households within sectors. An agreement with the Brazilian Ministry of Health ensures the collection of a multitude of indicators of the health status of every household member, including anthropometric measures of weight and height collected by trained interviewers.
Analytical Sample
Our analytical sample consisted of subsamples of adolescents ages 12 to 17: all adolescents, all siblings, and same-sex siblings. The initial data set had 45,964 adolescents ages 12 to 17 who were not pregnant. We dropped 409 cases reporting weight less than 5 kg and/or height below 80 cm because of implausibility and 303 adolescents with missing information on work and/or school enrollment. To accurately identify siblings for our within-family analyses, we examined only children of the head of the household because those are the only children for which we have a parental identifier. Children of the head of household represented 83.78% of the sample, bringing the final sample size to 37,884. In sensitivity analyses, we tested for differences in the samples of children who do belong and children who do not belong to the head of the household and did not find significant differences between the two groups. We used multiple imputation to handle observations with missing values on parental education (6.82%) and mother’s weight status (8.39%). Results using multiply imputed data produced substantively similar results to those using listwise deletion.
From the overall sample of adolescent children of the household head, we identified siblings in this age range (n = 17,430) using the month and year of birth of children who live in the same household, an approach that has been applied extensively in research using household survey data (e.g., Levison et al. 2007; Marteleto and Dondero 2017). In some analyses, we examined a subsample of same-sex siblings (n = 1,656) to eliminate gender differences in overweight/obesity, school enrollment, and work. To create the sibling samples, we appended sibling variables (i.e., school dropout and work status) to each adolescent as the unit of analysis and randomly selected sibling pairs within each household. The siblings fixed effects logistic (explained in detail in the following) modeled variation among only those sibling pairs with discordant overweight/obesity statuses. We weighted all analyses with the individual weights provided by IBGE.
To establish the feasibility of our sibling models, Table 1 shows obesity, school enrollment, and work status between sibling pairs for all and same-sex siblings. Among all siblings, in 3.19% of the cases, both siblings were obese, whereas in 20.50% of the cases, only one sibling was obese. There was a similar level of discordance between siblings regarding work, with only one sibling working in 22.59% of the sibling pairs. In 11.12% of the pairs, only one sibling was out of school. The proportions among same-sex siblings were similar.
Obesity, School Enrollment, and Work among Sibling Pairs with Data from Pesquisa de Orçamentos Familiares, 2003 and 2008 Waves.

Measures
Our dependent variable was a dichotomous indicator of overweight or obesity. We created BMI z scores based on BMI by age and sex using the Box-Cox transformation-based semiparametric approach (Cole 1988; Cole and Green 1992). We then used the (adjusted) height and weight measurements to estimate adolescent BMI percentiles according to the World Health Organization. We categorized children with a BMI above the 95th percentile as obese and those between the 85th and 94th percentiles as overweight.
School enrollment and work status served as our key independent variables representing individual nascent SES. School enrollment measured whether an adolescent was enrolled in school at the time of the survey. Work status measured whether the adolescent was working at the time of the survey. Respondents were asked whether they worked some time during the last 12 months, a standard measure of current work status. We also controlled for age because that is one of the only relevant observed characteristics besides gender, work, school enrollment, and weight that varies between siblings. Other variables that are shared between siblings (e.g., parental obesity status, household income) dropped out of the fixed effects equation (described in detail in the following). Finally, we included interactions between school enrollment and work to assess how the combination of school and work is associated with overweight/obesity risk.
Methods
We estimated models using the three different analytical samples—all adolescents, all siblings, and same-sex siblings. We included the first analytical sample of all adolescents for methodological and substantive reasons. This sample represents the more standard modeling approach, which assesses variation in adolescent overweight and obesity among adolescents from different families. We also included these models because they generated a coefficient for family SES indicators (parental education and household income), which allowed us to assess whether individual SES and family SES were similarly associated with overweight/obesity for adolescents. We then ran our focal siblings fixed effects models to assess school enrollment and work status differences in overweight/obesity between all and same-sex sibling pairs.
We ran two models for the sample including all adolescents and four sets of models for the sibling analytical samples. For each analytical sample, we first included standard logit estimates for comparison purposes. In the logit models, we controlled for relevant observed characteristics that vary between individuals: race (dummy with nonwhite as the omitted category), parental education (complete years of schooling of the parent with the highest educational level), household income (per capita household income), mother’s overweight/obesity status (not obese = reference), region of residence (a combination of Brazil’s main regions with south and southeast omitted), and year. In the next model, we included an interaction term between school enrollment and work.
We then estimated two sets of fixed effects models for each of the sibling samples, adding the interaction term for school and work in the second model. In the siblings fixed effects models (all siblings and same-sex siblings), we modeled sibling-specific factors that vary across sibling pairs. Sibling fixed effects models allowed us to control for unobserved variables, including genetic predisposition to overweight/obesity and household factors shared by siblings (e.g., household food environment). The same-sex sibling fixed effects models go beyond the all-siblings fixed effects models in that they account for unobserved variables that are shared by siblings of the same sex but vary across different sex siblings (e.g., gendered eating behaviors). The logic behind sibling fixed effects models is to differentiate estimates across pairs of siblings. The analogous logistic regression formulation is:

where Yij corresponds to school enrollment or work status for adolescent j in family i, X is a vector of explanatory variables, and

Although this paired-difference values approach eliminates the unobserved family fixed effect, this method does not eliminate errors that are specific to each sibling j in family i. If such errors are correlated with the explanatory variables, estimates from sibling fixed effects models may still be biased. An additional limitation of sibling fixed effects models is that these models only capture variation in explanatory variables and obesity status that occurs within families and between siblings (Allison 2009). Thus, sibling fixed effects models can yield inefficient estimators in that variation between families is not captured. As a way to minimize this issue, we tested the robustness of the fixed effects estimates for the full sample by estimating the corresponding models across different subgroups of years and levels of mother’s education (available on request). In supplemental analyses (discussed in the following), we also used a sample of twins to more stringently control for factors shared by twins that are not shared by siblings (i.e., additional genetic characteristics).
Results
Table 2 presents the characteristics of adolescents in the different analytical samples: all adolescents, all siblings, and same-sex siblings. We also include descriptive statistics for the sample of siblings used in the fixed effects logistic regression models (i.e., only sibling pairs with discordant overweight/obesity status). Focusing on the sample of all siblings, approximately 13% are overweight or obese. About 8% were out of school, whereas nearly 20% were working. In anticipation of the models that interact school enrollment and work status, we also report the share of adolescents who are in each of the combined school enrollment–work status groups. Across all samples, the large majority of adolescents (approximately 75%–78%) are enrolled in school and not working. The percentage who are enrolled in school and working ranges between approximately 13% and 17%, depending on the sample. Adolescents who are not enrolled and working comprise the smallest group (approximately 3%–3.5% of each sample).
Descriptive Statistics, Adolescents Ages 12–17 with Data from Pesquisa de Orçamentos Familiares, 2003 and 2008 Waves.
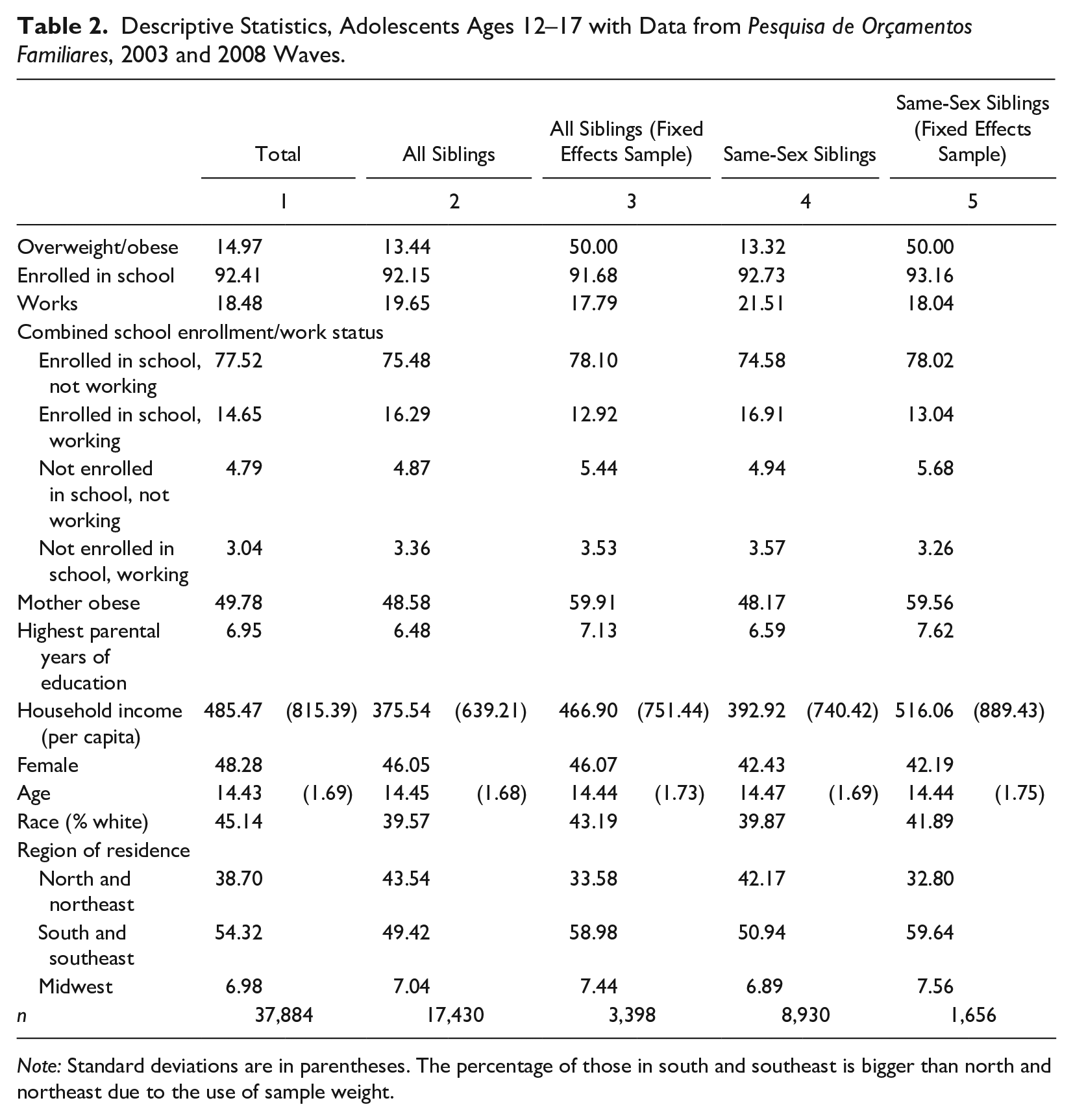
Note: Standard deviations are in parentheses. The percentage of those in south and southeast is bigger than north and northeast due to the use of sample weight.
To provide further context about the composition of the samples, it is worth noting that about 40% of the adolescents in the sibling sample are white, about half had an obese or overweight mother, and about half live in the south and southeast regions. We also note that although the sibling samples used in the fixed effects regression analyses include only those siblings with discordant overweight/obesity statuses, these samples do not differ substantively from all adolescents or the other sibling samples on most characteristics. The fact that exactly half of the siblings in the fixed effects samples are overweight/obese is by design because the sibling pairs must be discordant on the outcome for the fixed effects models.
Table 3 shows standard logit and sibling fixed effects models for each analytic subsample: all adolescents (Columns 1 and 2), all siblings (Columns 3–6), and same-sex siblings (Columns 7–10). The first two columns of each analytical sample (Columns 1 and 2, 3 and 4, and 7 and 8) show results from standard logit models. The next two columns of each of the sibling samples (Columns 5 and 6 and 9 and 10) show results from fixed effects logit models. We introduce the interaction term between school enrollment and work in the second model of each analysis.
Odds Ratios from Logit and Fixed Effects Logit Models Predicting Overweight/Obesity with Data from Pesquisa de Orçamentos Familiares, 2003 and 2008 Waves.

p < .05, **p < .01, ***p < .001.
Column 1 shows that school enrollment is negatively associated with overweight and obesity (odds ratio [OR] = .687; p < .001) among the sample of all adolescents, suggesting that school enrollment is associated with over 30% lower odds of overweight/obesity and providing support for Hypothesis 1a. In contrast to both hypotheses about work (Hypotheses 2a and 2b), the association between working and overweight/obesity is not statistically significant. This model also shows another important finding that is not directly related to our hypotheses but is relevant nonetheless. The two measures of household SES—highest parental years of education and household income—are both associated with statistically significant higher odds of overweight/obesity. That is, these associations with household SES characteristics work in the opposite direction to that of the association between the individual SES characteristic of school enrollment.
To compare the relative size of the effects of school enrollment and family SES, we calculated predicted probabilities for a child with average characteristics using Stata’s margins commands. For the average child in our sample, 13% of those enrolled in school are predicted to be overweight/obese, compared with 18% of their counterparts not enrolled in school (predicted probabilities not shown), or a difference of 5 percentage points. This differs for the patterns of predicted probabilities for the two measures of family SES. The probability for children with parents in the highest quartile of years of education is .15, compared to .14 among children with parents in the lowest quartile. For family income, children in the highest quartile have a .16 probability of overweight/obesity, compared to .10 for children in the lowest quartile.
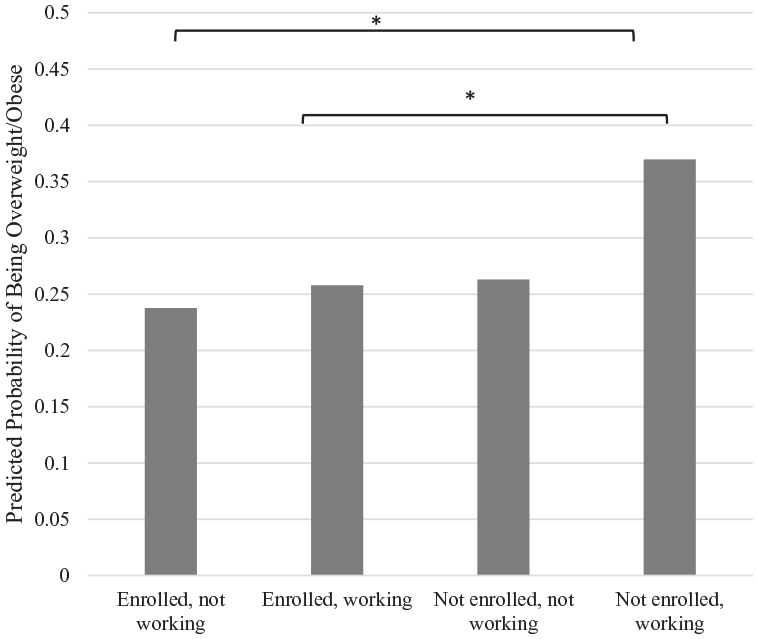
In the standard logit model with the interaction term between school enrollment and work (Column 2), the interaction term between school enrollment and work status is negative and statistically significant (OR = .676, p < .01), suggesting that the association between school enrollment and overweight/obesity varies by work status. Because this is a categorical model, we confirm the statistical and substantive significance of the interaction term with pairwise comparisons of group differences in the predicted probabilities of overweight/obesity based on these models (Mize 2019). The predicted probabilities based on these models, displayed in Figure 1, show that adolescents who are not enrolled but working have the highest probability of overweight/obesity, followed by those who are neither enrolled nor working, although these two groups are not significantly different from each other. In contrast, those who are enrolled in school, both those who are working and those who are not, have similarly low probabilities of overweight/obesity. Pairwise comparison tests of the predicted probabilities confirm the following group differences: (1) Adolescents who are not enrolled but working have a statistically significant higher predicted probability of overweight/obesity than their enrolled counterparts regardless of work status, and (2) adolescents who are neither enrolled nor working have a higher probability than their counterparts who are both enrolled and working.

Predicted Probabilities of Overweight/Obesity (Based on All-Adolescents Logistic Models in Table 3, Column 2) with Data from Pesquisa de Orçamentos Familiares, 2003 and 2008 Waves.
Columns 3 and 4 show results for the standard logit models with the sample of all siblings. The odds ratios are similar in direction and magnitude as in the standard logit models for all adolescents. In this model, we again find that household income is positively and significantly associated with overweight/obesity. However, parental education level is not significantly associated with overweight/obesity in this model.
Results from the fixed effects models among all siblings in Columns 5 and 6 are particularly noteworthy because they suggest that even when holding relevant observable characteristics and shared unobservable family variables constant, adolescents enrolled in school have 27% lower odds of being overweight or obese compared to their siblings who dropped out of school (OR = .725, p < .001). As in the model with all adolescents, the main effect of work is not significantly associated with overweight/obesity in this model with all siblings either.
Column 6 adds the interaction term between school enrollment and work. Although the interaction term itself is not statistically significant, pairwise comparisons testing group differences in the predicted probabilities of overweight/obesity show statistically significant differences between certain groups. Figure 1 shows predicted probabilities from the model in Column 6. Of the four school enrollment–work combinations, adolescents who are not enrolled in school but are working have the highest probability of overweight/obesity (.36) and significantly differ from those who are enrolled in school but not working (.24) and from those who are enrolled in school and working (.26). There were no statistically significant differences in the predicted probabilities between any other groups.
In an additional, more stringent test of our hypotheses, we eliminate sex differences between siblings by using same-sex siblings fixed effects models, shown in Columns 9 and 10 (with the corresponding standard logit models for this sample shown for reference in Columns 7 and 8). However, because the sample size of adolescents not enrolled in school (n = 148) is small in this subsample, we present these results as an additional test of the main fixed effects models with all siblings and interpret the results, particularly those of the interaction model, with this caveat in mind. Mirroring results from other models, Column 9 shows that school enrollment (OR = .629, p < .001) is associated with lower odds of overweight/obesity but that work status is not significantly associated with overweight/obesity among the adolescents in our sample. Column 10 adds the interaction term, which is less than 1 and not statistically significant. The predicted probabilities based on this model, graphed in Figure 3, show a pattern similar to that of the all-siblings model in Figure 2: Adolescents who are not enrolled but work have the highest probability of overweight obesity, followed by those who are neither enrolled nor working, those who are enrolled and working, and those who are enrolled but not working, respectively. However, pairwise comparisons of predicted probabilities from this model revealed no statistically significant differences between any groups, likely due to small sample sizes in the not-enrolled groups.
Predicted Probabilities of Overweight/Obesity (Based on All-Siblings Fixed Effects Models in Table 3, Column 6) with Data from Pesquisa de Orçamentos Familiares, 2003 and 2008 Waves.

Predicted Probabilities of Overweight/Obesity (Based on Same-Sex Siblings Fixed Effects Models in Table 3, Column 10) with Data from Pesquisa de Orçamentos Familiares, 2003 and 2008 Waves.
Robustness Checks
We conducted three types of robustness checks (results available on request). First, we used a sample of twins to examine twins fixed effects models as a more stringent test of our research questions because twins share age and, in the case of monozygotic twins, genetic characteristics beyond those shared by siblings. We included the twins results as supplemental analyses rather than main analyses due to the limited statistical power resulting from the small number of twin pairs in our sample. The odds ratios for school enrollment and work status operated in the same direction in the twin models as in the siblings fixed effects models but did not reach statistical significance due to small sample sizes.
In our second set of sensitivity checks, we estimated a set of linear probability fixed effects models using age- and sex-specific BMI z scores and obtained similar findings as in the models with categorical variables. We also analyzed models with obesity only as the dependent variable. As expected, the small sample in the obese category limit statistical significance of some coefficients that are statistically significant in the obesity/overweight models, but the direction of the coefficients remains the same.
In our third set of sensitivity tests, we tested for additional variation by potentially relevant sociodemographic characteristics: family SES, age, and gender. First, we examined whether the association between school enrollment and work status and overweight/obesity differs by family SES. In models with subsamples of low- versus high-SES adolescents, the odds ratios for school enrollment remain statistically significant but are larger among low-SES adolescents, suggesting that school enrollment may be more beneficial for the odds of obesity among low-SES adolescents. Similarly, the magnitude of the interaction term for those in school and working is much higher among low-SES adolescents than among all other adolescents.
Second, acknowledging that there may be age differences in physical and cognitive development as well as in opportunities to work, we examined adolescents ages 12 to 14 versus 15 to 17 separately. The school coefficients in both sets of models remain statistically significant but reach a larger magnitude among older adolescents, which could suggest that school enrollment may be more protective of obesity/overweight for this age group. However, it could also reflect that there was a smaller number of 12- to 14-year-olds who are not enrolled in school.
Finally, we conducted sensitivity analyses focusing on gender to evaluate whether school enrollment and/or work status is more consequential for boys’ or girls’ obesity risk. To do this, we tested interactions between gender and school enrollment and between gender and work status in standard logit models for the all-adolescents and all-siblings samples and in siblings fixed effects models. We did not find any statistically significant gender interactions in the models or any statistically significant differences in the predicted probabilities of overweight/obesity by gender, school enrollment, and work status. In other words, the disparities in the probabilities of overweight and obesity by school enrollment and by work status are similar for boys and girls.
Discussion
Socioeconomic and health disadvantages are intertwined, and such linkages likely emerge early in the life course, particularly for a country like Brazil that is characterized by high socioeconomic inequality and increasing rates of obesity at all ages. Focusing on common individual markers of adolescent socioeconomic status (i.e., school enrollment and work) instead of family SES (i.e., household income and parental education) provides insight into the socioeconomic risk and protective factors for adolescent overweight and obesity early in the life course. Moreover, because of recent economic and nutritional changes in Brazil, adolescent SES and family SES may have substantially different consequences for adolescent obesity. We used sibling fixed effects models to account for unobserved genetic and environmental factors shared by siblings that may be confounders in the association between socioeconomic disadvantage and adolescent overweight and obesity. We highlight four main findings that emerge from this study.
Our first major finding concerns the role that schools and schooling play in adolescent obesity and overweight in Brazil. In line with Hypothesis 1a, we find that adolescent school enrollment is associated with lower odds of adolescent obesity and overweight. We speculate that the protective role of school enrollment may be because schools have the potential to promote healthy habits. For example, school feeding programs can provide food security to vulnerable students and healthy options for students at risk of obesity and overweight. Because Brazil’s feeding program is well established and successful (Rocha 2009; World Food Programme n.d.), school enrollment may be especially important for maintaining healthy weight status among Brazilian adolescents. Moreover, education promotes knowledge of healthy behaviors and increases effective agency (Mirowsky and Ross 1998), increasing the likelihood that adolescents will live healthy lives. In a country where high levels of inequality and disadvantage are common and where rates of obesity are rapidly increasing, these findings indicate that school enrollment is associated with an overweight/obesity health advantage early in the life course.
Our second major finding concerns the role that work plays in adolescent obesity and overweight in Brazil. This is a pressing issue because most adolescents in low- and middle-income countries work and because obesity rates are rapidly rising. But because previous studies have not explicitly examined the association between work status and adolescent obesity/overweight, the consequences of adolescent work for obesity/overweight are not well understood. In contrast to Hypotheses 2a and 2b, we find no evidence that work status itself is significantly associated with either higher or lower odds of overweight/obesity.
However, our third key finding offers more insight into this question by considering how school and work intersect to shape adolescent overweight and obesity in Brazil. Results from standard logit and all-siblings fixed effects models with interactions suggest that adolescents who are enrolled in school—both those who work and those who do not—have the lowest probabilities of overweight/obesity. In contrast, adolescents who are not enrolled but work are at the greatest risk of overweight/obesity. Thus, our findings suggest that work per se is not adversely associated with adolescent overweight obesity; rather, because school enrollment is the more important individual SES predictor of overweight/obesity among adolescents, working while not enrolled in school appears to be associated with an obesity disadvantage. However, we acknowledge that it is possible that the effects of work are mixed because of differences in the type of work rather than in school enrollment. Adolescents who are not enrolled in school but work may be employed in jobs that place them at greater risk of overweight/obesity than the types of jobs taken by adolescents who are enrolled in school. Additional research should examine whether number of hours and type of work—information unavailable in the POF data set—mediate the association between work and obesity among adolescents.
We also note that the finding that work is not associated with greater overweight/obesity risk when combined with school enrollment aligns with prior work on the benefits of combining work with school. For example, attending school while working is associated with improved academic performance in the United States (Mortimer and Johnson 1998; Staff et al. 2010) and increased adult earnings in Brazil (Emerson and Souza 2011). We speculate that combining school and work might be a way to gain skills that promote healthy eating habits.
Yet this interpretation is not entirely consistent with our finding that adolescents who are the most inactive—those who are neither enrolled in school nor work—fall in the middle in terms of risk. In contrast to Hypotheses 3, which predicted that adolescents who are neither enrolled in school nor working would have the highest risk of overweight/obesity, we find that their predicted probability is lower than those who are not enrolled and working, although it does not significantly differ from this group in any of the models. We suspect that this finding could partly reflect selection into this group, which might be made up of adolescents who are out of both school and work for reasons such as illness, poverty, and/or early childbearing that might also affect their overweight/obesity risk.
The fourth important finding is not one that is a focal, hypothesized part of our study, but we highlight it because it informs understanding of our main findings. In the standard logit models (i.e., those without fixed effects), we estimate odds ratios for family SES characteristics because these factors vary across families. These models showed that individual SES (school and work) and family SES (parental education and household income) have different associations with adolescent overweight and obesity. Whereas indicators of an adolescent’s nascent SES in the form of school enrollment is associated with lower risk of overweight and obesity, indicators of an earlier generation’s SES—parental education and household income—are associated with higher risk. This may mean that parental and adolescent SES carry different risks, or it may mean that the risks of low SES are likely to be different for today’s youth than it was for their parents’ generation. It would be interesting to explore whether these associations can be observed during earlier time periods or are unique to the early twenty-first century when the association between SES and obesity was changing from positive to negative (Monteiro et al. 2007). If the latter, it may suggest that the cohorts of adolescents in this sample represent the first generation for whom overweight/obesity disproportionately afflicts the lower class.
This study advances understanding of the role of school enrollment and work status for adolescent overweight/obesity as well as an interplay of social stratification and health inequalities, but limitations should be noted. First, the research focuses on a single country with a specific context related to overweight and obesity (i.e., school lunch program, specific meal types, family dynamics, and the job opportunities for adolescents). Although this research contributes to the understanding of the role of adolescent SES on overweight and obesity, the association between school enrollment and work status and adolescent overweight and obesity may differ by country. Second, although sibling fixed effects models are beneficial for accounting for unobserved heterogeneity, their generalizability may be limited. Nevertheless, we find similar results for all adolescents when using standard logit models. Third, although we are able to hold constant unobserved family and neighborhood characteristics shared by siblings, we cannot account for unobserved factors inside or outside the home (e.g., food consumption, school attendance) that are not shared by siblings. Additionally, older siblings may have experienced a different family or neighborhood environment at various points in their lives than their younger siblings. Fourth, because we use cross-sectional data, we cannot determine the causal order of the association between school dropout and work status and overweight/obesity. Although we have interpreted our findings through the lens of the risk and protective factors of schools and work, we acknowledge the possibility that overweight and obesity might contribute to adolescent socioeconomic conditions such as school dropout and work. For example, adolescents who are stigmatized by peers at school because of being overweight or obese might be more likely to drop out of school (Lanza and Huang 2015). However, regardless of the direction of the association, our results underscore the fact that overweight and obesity intertwine with socioeconomic disadvantage early in the life course, with implications that likely extend into adulthood. Finally, our data set lacks further detailed information about school and work—such as frequency of school attendance, number of hours of work, and type of work—all of which might moderate the association between school, work, and overweight/obesity.
By using sibling fixed effects models to account for shared genetic and environmental components in overweight and obesity, we advance understanding of how adolescent social disadvantage—independent of family characteristics shared by siblings—is related to adolescent obesity in Brazil. Future research that uses longitudinal data and a life course approach will help to further understanding of how this adolescent context may serve as a catalyst that launches adolescents into different health trajectories across the life course. Longitudinal data will help scholars to examine causal order and determine whether adolescent SES leads to higher rates of overweight and obesity. Moreover, future studies should aim to understand the mechanisms that link adolescent social disadvantage such as school dropout to overweight and obesity and how these mechanisms operate throughout the life course. Finally, future research should further contextualize social disadvantage by including measures of school, household, and neighborhood disadvantage that are not shared by siblings.
Overall, our study represents an important first step toward understanding the complex linkage between socioeconomic and health disadvantages among adolescents in a middle-income country and have important policy implications. Considering the rampant social inequality in Brazil (Bourguignon, Ferreira, and Menendez 2007) and the significant health risks associated with obesity (Ogden et al. 2010), our findings about the importance of school enrollment for protection against adolescent obesity support the need for policy that promotes school retention in Brazil throughout childhood and adolescence. Although we examine socioeconomic disadvantage in adolescence, trajectories of disadvantage are likely established even earlier in the life course and highlight the need for policy interventions at a young age.
Footnotes
Authors’ Note
Letícia J. Marteleto and Molly Dondero contributed equally to the article.