
Abstract
The research tradition on social relationships, social networks, and health dates back to the beginning of sociology. As exemplified in the classic work of Durkheim, Simmel, and Tönnies, social relationships and social networks play a double-edged—protective and detrimental—role for health. However, this double-edged role has been given unbalanced attention. In comparison to the salubrious role, the deleterious role has received less scrutiny and needs a focused review and conceptual integration. This article selectively reviews the post-2000 studies that demonstrate the harmful physical and mental health consequences of social relationships (intimate relationships and parenthood) and social networks. It uses a parsimonious three-category typology—structural forms, structural composition, and contents—to categorize relationship and network properties and proposes the social cost model, in contrast to the social resource model, to synthesize and integrate the adverse aspects of these properties. It concludes with future research directions.
Social relationships and social networks matter. “The real nature of man is the totality of social relations” (Marx 1963:83). Individuals dwell in “social ties” or a “network of overlapping group-affiliations” (Simmel [1922] 1955). A social relationship is a tie linking two individuals. A web of social relationships constitutes a social network, that is, “a specific set of linkages among a defined set of persons, with the additional property that the characteristics of these linkages as a whole may be used to interpret the social behavior of the persons involved” (Mitchell 1969:2). Social relationships and social networks are important because of not only their influences on individuals but also their mesolevel positions in mediating between macrolevel social structures and microlevel individual actions (Cook and Whitmeyer 1992; Lin 2001).
Social relationships and social networks matter to health as a double-edged sword. The research tradition on social relationships, social networks, and health dates back to the beginning of sociology. Durkheim ([1897] 1951) demonstrates the protective and detrimental effects of social integration and social regulation on suicide. Simmel ([1922] 1955) discusses the positive and negative duality of social interaction and the salubrious and harmful impacts of the multiplicity of group affiliations on mental well-being. Tönnies ([1887] 1957) emphasizes the coexistence of protection and constraint from social ties. Despite the substantial developments of this 13-decades-long research tradition, the double-edged role of social relationships and social networks has been given unbalanced attention. In comparison to their protective role, their detrimental role has received less scrutiny and needs a focused review and conceptual integration (Berkman et al. 2000; Brooks and Schetter 2011; Lin and Peek 1999; Pescosolido 2006a; Smith and Christakis 2008; Song 2019; Song and Chen 2021; Thoits 2011; Umberson, Crosnoe, and Reczek 2010).
This article selectively reviews the post-2000 studies that demonstrate the harmful physical and mental health consequences of social relationships and social networks. It uses a parsimonious three-category typology—structural forms, structural composition, and contents—to categorize relationship and network properties and proposes the social cost model, in contrast to the social resource model, to synthesize and integrate the adverse aspects of these properties. It concludes with future research directions. Given the limited space, it focuses on the two most salient types of social relationships, intimate relationships and parenthood. For the purpose of generalizability and representativeness, it centers on studies of nationally representative data of the general population, unless noted otherwise.
Typology And Theoretical Perspectives
Social relationships and social networks are not theories but perspectives from which concepts and theories are derived (Pescosolido 2006b). The social network perspective is closely related to the social relationship perspective, theoretically and methodologically, but is broader (Lin and Peek 1999; Smith and Christakis 2008). It allows one to analyze the properties of a whole set of social ties. Scholars typologize network properties differently (Lin and Peek 1999; Perry, Pescosolido, and Borgatti 2018; Pescosolido 2006a; Valente 2010). This article employs a parsimonious three-category typology: structural forms, structural composition, and contents (see Figure 1 and Appendix Figure 1). Structural forms are the patterns and attributes of social ties between one (ego) and one’s network members (alters), such as network size, density, and relationship type. Structural composition represents the attributes of ego and alters, such as their sociodemographic characteristics and homophily. Contents refer to the interpersonal processes between ego and alters, such as social support flowing from alters to ego. In the theoretical causal chain linking the three types of properties, structural forms are most upstream and shape structural composition and contents; contents are most downstream and under the influence of structural forms and composition. Note that the social network perspective conceives of social support as one content of the social network structure, whereas the social support perspective sees social networks as the structural component of social support and focuses more on domestic relationships (House, Umberson, and Landis 1988; Lin 1986; Pescosolido 2006b; Thoits 1995; Wellman 1981). This three-category typology also applies to dyadic social relationships: structural forms (e.g., marriage, cohabitation, and parenthood), structural composition (e.g., spousal attributes, homogamy, and attributes of parents and children), and contents (e.g., spousal or children’s support).
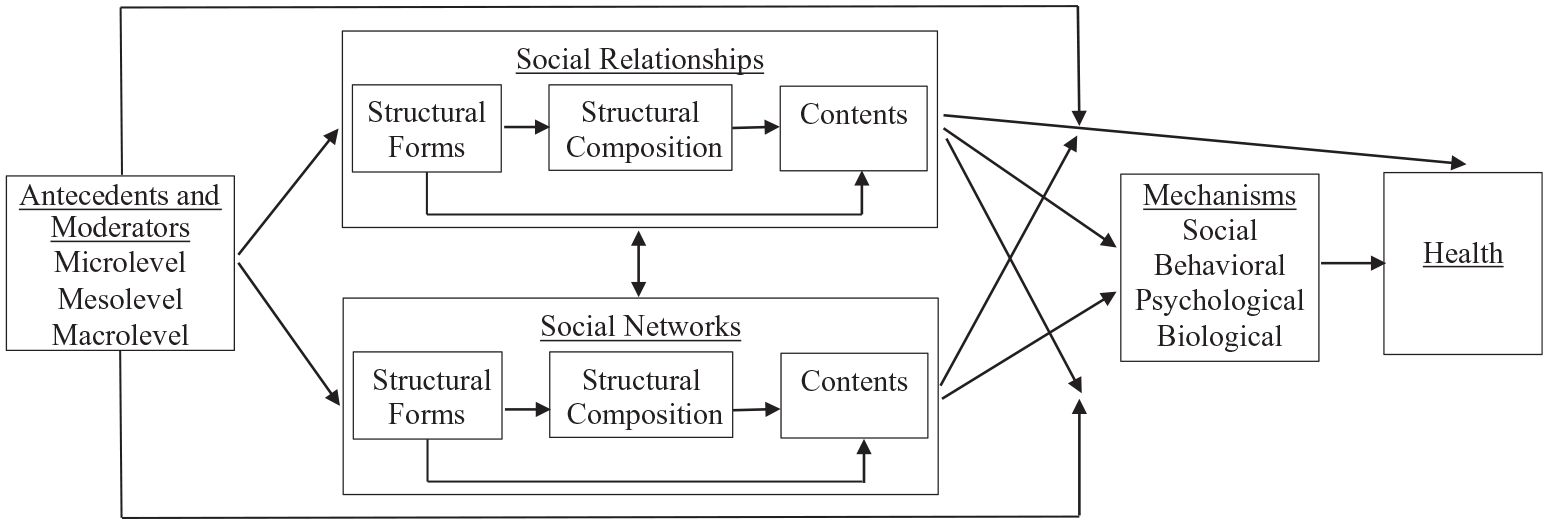
The Simplified Conceptual Diagram of Social Relationships, Social Networks, and Health.
Theoretical explanations of the double-edged impacts of social relationships and social networks are developed logically around the contrast and balance between their benefits and costs. Under the benefit logic, the social resource model is the dominant explanation. It expects relationship and network properties to protect ego’s health as salubrious resources or sources of such resources. These resources are embedded within social ties and thus framed as social resources or social capital, in contrast with personal resources or personal capital (Lin 1986, 1992, 2001; Song and Lin 2009). Social resources are under the control of alters, whereas personal resources are in ego’s ownership. There are different views on the operationalization of social resources. In the broad catch-all view, any facilitating feature of social relationships and social networks is social resources (Coleman 1990). In the content view, the salubrious relationship and network contents (e.g., social support and social control) indicate social resources ego receives or perceives from alters, and more upstream relationship and network properties serve as sources of such resources (Lin 1986; Umberson 1987). In the structural composition view, alters’ status or resources indicate social resources, and more upstream relationship and network properties work as sources of such resources (Lin 1992, 2001; Song 2011). Note that the social resource model develops from the social support tradition, which originally conceives of social support only as protective resources but later recognizes its harmful side (Eckenrode and Wethington 1990; House et al. 1988; Lin 1986; Thoits 1995; Wellman 1981).
In comparison to the benefit logic, the cost logic has been given relatively less attention, and relevant work lacks conceptual integration. Multiple theories and explanations apply the cost logic, including those on ambivalence, lay referral system, life course, life course development, network episode, role strain, social capital, social comparison, social contagion, social control, social exchange, social resources, social support, stress, and stress crossover (Barrera 1980; Caspi, Bem, and Elder 1989; Eckenrode and Wethington 1990; Elder 1974; Festinger 1954; Freidson 1960; George 1986; Good 1960; Lin 1992; Lüscher and Pillemer 1998; Moen, Dempster-McClain, and Williams 1989; Pearlin 1989; Pescosolido et al. 1998; Rook 1984, 1987; Smith and Christakis 2008; Thoits 1995, 2011; Wethington 2000; Wheaton 1990). Among them, the stress process paradigm is most widely used (Pearlin 1989).
Despite their contributions, these theories and explanations emphasize different aspects of costs. An integrative perspective is necessary but missing. Therefore, this article proposes the social cost model to fill this gap (Song 2019, 2020; Song and Chen 2021; Song and Pettis 2020). Parallel to the distinction between personal and social resources is the distinction between personal and social costs. Personal costs are the costs ego bears due to ego’s own actions, attitudes, and needs (e.g., ego’s health care expenses), whereas social costs refer to the costs ego endures due to ego’s embeddedness in social ties and connection with alters (e.g., ego’s spousal health care expenses). The social cost model states that the properties of social relationships and social networks can harm ego’s health as detrimental social costs or precursors of such costs (see Figure 1 and Appendix Figure 1). Based on prior work, diverse relationship and network contents indicate detrimental social costs, including ambivalent social interaction, asymmetric social exchange, deleterious social control, harmful social support, negative or upward social comparison, relationship strain or negative social interaction (e.g., conflict, interference, and alters’ failure to provide support), continuities of relationship strain, burdensome relationship investment, relationship violence, and demanding social obligations (e.g., alters’ demands for social support). Some aspects of the structural composition of social relationships and social networks also capture social costs such as alters’ resource shortage, detrimental network norms (e.g., alters’ antihealth attitudes), and alters’ stressors and problems that lead to crossover stress and risky social contagion. More upstream relationship and network properties serve as the precursors of social costs.
The concept of social costs helps synthesize and integrate the adverse aspects of social relationships and social networks and, together with the concept of social resources, form a balanced and comprehensive framework that interprets the double-edged role of social relationships and social networks. The direction and magnitude of the impact of a given relationship or network property rest on the rivalry between involved social resources and social costs. This property is beneficial when social resources outweigh social costs, detrimental when social costs overwhelm social resources, and null when they offset each other. The impact of this property can be moderated by other factors and be dynamic over space and time because its involved social resources and social costs can vary by other factors, including space and time. We next apply the three-category typology and selectively review health studies on intimate relationships, parenthood, and social networks that support the social cost model.
Intimate Relationships
Structural Forms
Among the structural forms of intimate relationships, marriage is given the most attention, followed by cohabitation and other romantic relationships. Although most studies on marriage demonstrate its protective effects, some studies report its detrimental effects. The continuously or currently married suffer from more depression, a higher risk of cardiovascular disease, and poorer functional and self-reported health compared to the never married and from poorer self-rated health compared to the divorced (Solazzo, Gorman, and Denney 2020; Williams and Umberson 2004; Wu and Hart 2002). Early marriage is positively related to mortality risks (Dupre, Beck, and Meadows 2009). In a longitudinal community study, higher order marriage (second or more marriage) harms mental health (Barrett 2000).
The harmful impacts of marriage vary by gender, race-ethnicity, age, parenthood status, and society. The married have a higher risk of health limitations than the never married among white women, whereas the opposite applies to white men (Teachman 2010). The remarriage transition is associated with depression positively for women but negatively for men (Williams 2003). Early first marriage is positively associated with the risk of chronic inflammation among men only (McFarland, Hayward, and Brown 2013). Remarriage is detrimental to self-rated health for the oldest but protective for the younger (Williams and Umberson 2004). Marriage undermines self-rated health for single mothers (compared to childless women) partly via their greater perceived marital instability (Williams, Sassler, and Nicholson 2008). The health disadvantage of marriage, especially for women, appears in East Germany but not West Germany, where the model of a marital union between a male breadwinner and female housewife may buffer marital costs (Hank 2010). In a community study of young women in rural China, the married have a higher risk of suicide than the unmarried, possibly due to relationship strain, low family status, excessive social control, and value strain (Zhang 2010).
Although most studies on cohabitation (compared to singlehood) demonstrate its positive effects, some studies find its negative effects. Cohabitation is related to increased depression and higher risk of health limitations among women, particularly white women (Booth, Rustenbach, and McHale 2008; Teachman 2010; Wu and Hart 2002). Its negative effect on self-reported health is stronger for women than for men, and its positive effects on bed days and distress appear among women only (Fuller 2010).
Romantic relationships can hurt adolescents. They lead to more psychological distress and depression to a greater degree for girls than for boys (Joyner and Udry 2000; Olson and Crosnoe 2017; Ueno 2005).
Structural Composition
The attributes of the two individuals in intimate relationships, including age, gender, sexuality, race-ethnicity, employment and paid work, division of labor, stressors, and health, determine the amount of social costs. Dating older partners (vs. those with similar age) leads to depression among younger adolescent girls (Loftus, Kelly, and Mustillo 2011). Same-sex cohabitation can be harmful, especially for lesbians and racial-ethnic minorities. Self-rated health is worse among lesbian cohabitors (compared to different-sex cohabiting, married, or never married women), black lesbian cohabitors (compared to different-sex cohabiting and never married black women), and Hispanic lesbian cohabitors (compared to never married Hispanic women; Liu, Reczek, and Brown 2013; Reczek, Liu, and Spiker 2017).
Racial-ethnic minority spouses and same-minority marriages involve more social costs. People with racial-ethnic minority spouses or minorities in same-race marriages report worse self-rated health than those married to whites (Miller and Kail 2016). Entering an interracial marriage or cohabitation with a nonwhite Hispanic partner (compared to staying unmarried) is associated with more depression among white women (Wong and Penner 2018).
Spousal employment and paid work damages men’s health. Spousal employment and long work hours damage self-rated health only for husbands (Stolzenberg 2001). Wives’ moderately long work hours predict worse self-rated general and physical health for husbands partly due to husbands’ reduced exercise time (Kleiner and Pavalko 2014).
The division of paid and unpaid labor is harmful when violating the equity norm and gender norms. Underbenefiting and overbenefiting are positively associated with depression among both wives and husbands (Kalmijn and Monden 2011). The transition from the husband acting as the breadwinner to the wife acting as the breadwinner leads to husbands’ poorer physical health and high risk of cardiometabolic and stress-related diseases (Springer, Lee, and Carr 2019). Husbands’ and wives’ psychological well-being is worst when husbands are unemployed but wives permanently employed (Inanc 2018).
Spousal (or partner) stressors and health problems are damaging through crossover stress and risky social contagion. Spousal (or partner) work–family conflict is associated with ego’s greater psychological distress and worse mental health through family stressors and ego’s work–family conflict (Young, Schieman, and Milkie 2014; Yucel and Fan 2019). Spousal severe health condition damages women’s mental health and men’s self-reported health (Valle et al. 2013). Depression transmits from wives to husbands (Thomeer, Umberson, and Pudrovska 2013). Spousal hospitalization is associated with the elderly’s increased risk of death (Christakis and Allison 2006).
Contents
The interpersonal process between intimate partners entails social costs, including relationship strain, relationship violence, and demanding social obligations. Marital or partner strain is positively associated with cardiovascular risks, depression, psychological distress, poor self-rated health, and lower survival rates (Birditt and Antonucci 2008; Liu and Waite 2014; Meadows and Arber 2015; Umberson et al. 2006; Williams 2003). Its detrimental effects apply more to older people and women, especially women living in poverty and different-sex marriages (Garcia and Umberson 2019; Liu and Chen 2006; Liu and Waite 2014; Umberson et al. 2006). Sleep problems link marital strain to poorer self-rated health (Meadows and Arber 2015). In a longitudinal community study, the worst physical and mental health outcomes appear among couples with husbands experiencing more marital strength than marital strain and wives reporting the opposite (Wickrama et al. 2020). Also, in a longitudinal community study, partner violence is positively related to ego’s depression with relationship strain as the mechanism (Longmore et al. 2014). Reciprocal partner violence is more depressing for women than men (Anderson 2002).
Demanding social obligations are damaging. Providing care to spouses or partners increases depression, especially for men with part-time work (Glauber and Day 2018). In a diary study, providing emotion work is inversely associated with psychological well-being to a greater degree for those married to a man than for those married to a woman (Umberson et al. 2020).
Parenthood
Structural Forms
Diverse forms of parenthood can be harmful: having children or too many children, early parenting, having stepchildren, and having a coresidential adult child. Parents, including full-nest parents, noncustodial parents, and those with nonresidential adult stepchildren, report more depression than nonparents (Evenson and Simon 2005; Pudrovska 2008). High parity (having four vs. two children) is associated with poorer self-rated health and higher risk of health limitation (Read, Grundy, and Wolf 2011). In a longitudinal community study, financial strain and sense of control link early parents (vs. nonparents or later parents) to more depression (Falci, Mortimer, and Noel 2010). Mothers with both biological children and stepchildren report higher distress than biological-only mothers partially due to relationship strain and economic hardship (Pritchard and Falci 2020). Parents with a newly coresidential adult child experience increased depression (Caputo 2019).
The social costs of parenthood vary by gender, race-ethnicity, and society. The parenthood–depression association exists in more countries for women than for men (Huijts, Kraaykamp, and Subramanian 2013). High-parity black women are more likely to experience disability than high-parity white women (Latham and Holcomb 2014). The parenthood–depression association appears more in countries with tolerant norms toward childlessness and higher levels of social contacts (Huijts et al. 2013). The positive associations of having coresident children with depression, poor self-rated health, and chronic conditions are stronger in nonfamilistic nations or nations with lower public pensions (Mair 2013). The negative association between high parity and physical health applies to women in East Germany but not in West Germany, suggesting that East German mothers bear the double burdens of family obligations and paid employment (Hank 2010).
Structural Composition
The attributes of parents and children affect the social costs of parenthood, including parental gender/sexuality, marital status, socioeconomic status (SES), and stressors and children’s age, gender, stressors, and problems. Mothers report more depression than fathers (Nelson-Coffey et al. 2019). Lesbian parents have worse self-rated health than different-sex married mothers (Denney, Gorman, and Barrera 2013). Unmarried parents have more depression than their childless counterparts (Nomaguchi and Milkie 2003). Mothers with low-status part-time jobs or without paid employment have higher stress than childless women with professional jobs (Lippert and Damaske 2019). Social stressors such as incarceration increase the social costs of parenthood, especially motherhood. Incarcerated parents are more distressed than incarcerated nonparents, and those with children in foster care are more distressed than other parents (Roxburgh and Fitch 2014). Mothers of minor children are more distressed than other inmates. Child living arrangements and frequency of contact with children are mechanisms for distress among incarcerated parents. Paternal incarceration increases a mother’s risk of a major depressive episode with undermined economic well-being and parenting stress and experiences as the mechanisms (Wildeman, Schnittker, and Turney 2012).
Children’s age and gender influence social costs for parents. Parents with minor children have more anxiety, depression, and physical limitations (Evenson and Simon 2005; Pudrovska 2008; Simon and Caputo 2019). In China, compared to those with both sons and daughters, parents with only sons or daughters report more depression; parents with only daughters are less depressed in urban China but more so in rural China, which has a stronger son-preference culture (Djundeva, Emery, and Dykstra 2017).
Children’s problems and stressors can cross over to parents, especially for mothers and black parents. Parents of children with a disability have more somatic symptoms, especially among younger parents (Ha et al. 2008). Child activity limitations lead to maternal health limitations directly and indirectly via health status (Garbarski 2014). In a longitudinal community study, stressors that blacks encounter during the adulthood transition elevate mothers’ cumulative biological risk for chronic diseases, psychological distress, and poor self-reported health, especially for mothers of male young adult children and children experiencing challenges at older ages (Barr et al. 2018). In another longitudinal community study, for black parents, adult children becoming ill or unemployed increases depression (Milkie, Bierman, and Schieman 2008).
Contents
The interpersonal process between parents and children can generate social costs for parents, including relationship strain, continuities of relationship strain, burdensome relationship investment, ambivalent social interaction, and harmful received social support. The parent–child relationship strain predicts parents’ increased depression, fair or poor self-rated health, and higher mortality rates (Birditt and Antonucci 2008; Koropeckyj-Cox 2002; Lantz et al. 2005; Song and Marks 2006). It costs more for mothers and minority parents. It is related to more cognitive limitations only among mothers (Thomas and Umberson 2018). In a longitudinal community study, it increases depression only for black parents (Milkie et al. 2008). In another longitudinal community study, earlier parental rejection reported by adult children indirectly leads to more later life depression among their mothers and fathers, respectively, through strain and low affection in the contemporary parent–child relationship (Whitbeck, Hoyt, and Tyler 2001). Time investment in children brings more stress and greater fatigue for mothers than for fathers (Musick, Meier, and Flood 2016). In a community study, mothers’ ambivalence toward their adult children is positively associated with their depressive symptoms (Suitor, Gilligan, and Pillemer 2011).
Social support from children can be detrimental. Companionship from adult children leads to more depression for married retired parents (Song and Marks 2006). In a longitudinal community study in rural China, where daughters-in-law are the culturally appropriate support providers, daughters’ and sons’ assistance with household chores increases depression, respectively, for mothers and fathers, and sons’ assistance with personal care increases depression for mothers living together with their daughters-in-law (Cong and Silverstein 2008).
Social Networks
Structural Forms
Multiple structural forms of social networks can be detrimental: size, density (the extent to which alters are friends with each other), centralization (the extent to which a few alters are highly central), type, partner network, partner betweenness (the partner’s having more contact with ego’s alters than ego does), social participation, and daily contacts. Network size is positively related to the risk of undiagnosed and uncontrolled hypertension for those who are unlikely to discuss health problems or medical treatment with alters (Cornwell and Waite 2012). The size of ties that discuss religion is positively associated with depression for those with a low religious salience (Upenieks 2020). Among hurricane victims, network size is positively related to depression only for women (Haines, Beggs, and Hurlbert 2008).
Adolescents with too large a network have more depression (Falci and McNeely 2009). Boys with too large, dense networks report more depression, whereas girls with too large, fragmented networks do the same. Girls with fragmented networks are at greater risk for suicidal ideation, whereas boys attending schools with fragmented networks are at greater risk for suicide attempts (Bearman and Moody 2004). Centralization of school class networks is positively related to minor psychiatric disorders in childhood and fair or poor self-rated health in adulthood (Almquist 2011). Compared to the diversified network type, the family-focused and restricted network types are associated with more difficulties in activities of daily living and worse cognitive function, psychological well-being, self-rated health, and overall health (Li and Zhang 2015). Also, the family-focused (vs. friend-focused) network type is associated with worse physical outcomes. Husbands’ greater talk frequency with their alters is negatively associated with wives’ emotional well-being, and the same is true for wives in regard to husbands’ self-rated health (Ermer and Proulx 2020). Among heterosexual men, partner betweenness is positively associated with erectile dysfunction, especially among the youngest (Cornwell and Laumann 2011).
Social participation and daily contacts can also be harmful. Total annual social participation predicts worse mental health, especially for older women (Myroniuk and Anglewicz 2015). Memberships in organizations are associated with increased risks of physical health problems (Musalia 2016). High-attending evangelical Protestants report more depression than low-attending ones in Nebraska (Schwadel and Falci 2012). There is a U-shaped curvilinear relation between religious service attendance and distress among non-Hispanic whites (Tabak and Mickelson 2009). Having daily contacts is associated with worse physical health in central and southern Europe but not in northern Europe, where publicly funded formal support services are available, and that association is weaker for higher SES people in southern Europe (Craveiro 2017).
Structural Composition
The attributes of ego and alters can influence the social costs of social networks, including homophily, alters’ status or accessed status, and alters’ stressors and problems. Migrant homophily (a high proportion of migrants among alters) is related to poorer health for migrants, especially for those with denser networks (Rostila 2010). Unhealthy behaviors and low SES are mediators. Having most alters involved in the military is associated with worse mental health for service leavers (Hatch et al. 2013).
Accessed status has two dimensions: absolute (alters’ absolute status) and relative (alters’ status compared to ego’s). Social cost theory expects absolute and relative higher accessed status to damage health (Song 2019, 2020; Song and Pettis 2020). Consistent with this theory, knowing the leader of the work organization is positively associated with depression indirectly through financial dissatisfaction and receipt of unsolicited job leads in urban China (Song 2015a). Relative higher accessed status is associated with worse self-rated physical health and mobility, increased overall disease burden, and increased reporting of cardiovascular morbidity (Pham-Kanter 2009). It is positively associated with depression, especially for men, in South Korea (Lee and Kawachi 2017). Consistent with the collectivistic disadvantage explanation and the inequality structure explanation, the positive associations of absolute and relative higher accessed status with depression and self-reported health limitations, respectively, apply more to collectivistic and less egalitarian societies (Song 2015b; Song and Pettis 2020).
Alters’ stressors and problems can lead to crossover stress and risky social contagion. Alters’ stressors are positively associated with psychological distress through family-to-work conflict and exacerbate the distressing effect of family-to-work conflict (Young and Schieman 2012). The positive association between alters’ and ego’s depression extends up to three degrees of separation in a longitudinal community study (Rosenquist, Fowler, and Christakis 2011). Adolescents with delinquent friends have a higher risk of suicidal ideation, especially in well-off neighborhoods (Kim and Chang 2018). Adolescents, especially girls, are at higher risk of suicidal ideation and attempts when alters, especially friends, attempt suicide or disclose suicide attempts (Abrutyn and Mueller 2014; Bearman and Moody 2004; Mueller and Abrutyn 2015). At-risk adolescents are more likely to have suicidal thoughts when a friend of a friend attempts suicide (Baller and Richardson 2009). Exposure to suicide attempts by same-sex grademates’ family members is positively associated with adolescents’ suicidal thoughts, particularly for girls (Fletcher 2017).
Contents
The interpersonal process between ego and alters can generate social costs for ego, including relationship strain, ambivalent social interaction, harmful received social support, demanding social obligations, asymmetric social exchange, and deleterious social control. Relationship strain is positively associated with depression partly through diminishing perceived support (Liang, Krause, and Bennett 2001). It is also positively associated with poor self-rated health, functional limitations, and the number of health conditions (Newsom et al. 2008). Relationship strain with church members increases psychological distress (Ellison et al. 2009). Having exclusively problematic kin and nonkin ties is positively associated with depression, whereas having ambivalent kin ties is positively associated with both depression and functional health limitations (Rook et al. 2012).
The detrimental impact of relationship strain varies by role relationship, age, race-ethnicity, and SES. Increased (vs. consistently high) relationship strain involving spouses or partners rather than children, friends, or relatives is associated with increased mortality (Birditt and Antonucci 2008). In two community studies of two age cohorts, the number of difficult or demanding alters and having difficult partners and adult children is positively associated with psychological distress only among older adults (Child and Lawton 2020; Offer 2020). Relationship strain with relatives is positively related to psychological distress directly for whites but indirectly for blacks through personal control (Lincoln, Chatters, and Taylor 2003). Relationship strain is associated with increased risk of heart disease only for those with lower education (Krause 2005).
Receiving social support can be detrimental, depending on its unsolicitedness, contents, and sources. Receipt of unsolicited job leads is positively associated with depression directly in the United States, especially for those with better-off financial situations, and indirectly in urban China through financial dissatisfaction (Song 2014; Song and Chen 2014). Receipt of prayer is positively associated with depression for those with a low religious salience (Upenieks 2020). In contrast to the protective effects of support from parents and teachers, higher levels of peer support increase depression among adolescents (Meadows 2007).
Demanding social obligations are harmful. Providing social support is positively associated with depression indirectly through negative interaction (Liang et al. 2001). Providing financial and instrumental support is associated with worse health (poor self-rated health, difficulties in activities of daily living, and chronic conditions) in central and southern Europe but not in northern Europe, where the strong publicly funded formal support services serve as a buffer (Craveiro 2017). In a longitudinal community study, the perceptions of alters’ emotional support needs lead to more psychological distress (Durden, Hill, and Angel 2007).
Asymmetric social exchange can affect health. Overbenefiting has a positive association with depression, whereas underbenefiting does the opposite (Liang et al. 2001). Receiving emotional support is positively related to depressive and somatic symptoms in overbenefiting exchanges but negatively in reciprocal exchanges (Nahum-Shani, Bamberger, and Bacharach 2011). A shift from reciprocal support to overbenefiting is positively associated with depression among women but negatively among men (Väänänen et al. 2008).
Informal social control from alters can be deleterious. In a community study, higher levels of perceived direct control from alters are associated with greater stress and shorter telomere length (Uchino et al. 2015).
Summary and Future Directions
Summary
This article typologizes relationship and network properties into three categories and proposes the social cost model to provide a long overdue focused review of the dark downside of social relationships and social networks. Studies in the past two decades have advanced the understanding of the deleterious consequences of intimate relationships, parenthood, and social networks in three major ways.
First, these studies support the theoretical utility of the social cost model and, together with earlier work, help map a conceptual diagram of health-damaging relationship and network properties (see Figure 1 and Appendix Figure 1). They find evidence for the deleterious impacts of not only each of the three types of relationship and network properties but also diverse properties within each type. The evidence pertains more to intimate relationships and social networks than to parenthood. Specifically, it applies more to the structural forms of intimate relationships and parenthood than to their structural composition and contents and more to the contents of social networks than to their structural forms and composition. Intimate relationships, parenthood, and social networks involve different natures and ranges of ties. Their structural forms and composition are measured more diversely and differently, whereas their contents have more consistent indicators and health consequences. Among the contents, the evidence relates most to relationship strain, followed by harmful received social support, demanding social obligations, asymmetric social exchange, ambivalent social interaction, and other contents. Some studies also report evidence for mechanisms linking relationship and network properties to poor health. Structural forms can damage health through socioeconomic disadvantages, relationship strain, other stressors, lack of coping resources, and low psychological resources. Structural compositions can be harmful via socioeconomic disadvantages, unhealthy lifestyles, relationship strain, other stressors, detrimental received social support, and low subjective well-being. Contents can be detrimental through risk factors such as sleep problems, low subjective well-being, perceived low support, and other contents.
Second, the explanatory power of the social cost model varies by sociodemographic factors (gender, sexuality, race-ethnicity, age and life course, and SES), which boosts the fruitful integration of this model with other perspectives. Gender is the most salient moderator. The social cost model is gendered. Women are more disadvantaged than men. Consistent with the traditional gender norms, women encounter more social costs than men in all three types of relationship and network properties. Their health suffers more than men’s when they are in intimate relationships, have unemployed spouses, encounter intimate relationship strain and violence, provide spousal or partner support, raise children, experience parental stressors, maintain network size and social participation, face fragmented networks, know alters who attempt suicide, and overbenefit from social exchanges. Among women, having intimate relationships is more detrimental for single mothers, lesbians, and racial-ethnic minority lesbians, and having children is more detrimental for the unmarried and lesbians. Also reflecting the traditional gender norms, men’s health suffers more from spousal or partner’s economic conditions, stress crossover, and accessed status. There is limited evidence for the moderating roles of race-ethnicity, age and life course, and SES. As for race-ethnicity, intimate relationships are more harmful for white women than black women, and strain in social networks is more noxious for whites. However, having racial-ethnic minority spouses and same-minority marriages is detrimental, and parenthood, children’s stressors, and parent-child relationship strain are more deleterious for blacks, especially black women. With regard to age and life course, marriage, parenthood, and partner betweenness hurt the younger more, but remarriage and strain in marital relationships and social networks harm the older more. In the case of SES, low-status people suffer more from intimate relationship strain, motherhood, having daily social contacts, and strain in social networks, whereas the opposite applies to unsolicited social support.
Third, the predictive power of the social cost model is contingent on macrolevel institutional contexts. Health is a consequence of double structural embeddedness. It is embedded in mesolevel network structures that are further embedded in macrolevel institutional structures. Among the three types of relationship and network properties, structural forms are under the greatest influence of institutional structures. Marriage is more likely to harm health, especially women’s health, in societies where marital institutions create more family–work conflict, create more relationship strains, and impose more social control. Parenthood is more likely to hurt health in societies with more tolerant norms regarding childlessness, high levels of social connections, weaker familistic culture, lower government support, and more family–work conflict. Having only daughters and having daily contacts is more likely to be deleterious in societies with son-preference culture and with less government support, respectively. The contents of parenthood, the structural composition, and contents of social networks also have effects that vary across societies. Receiving support from children is more likely to be deleterious in societies where daughters-in-law are considered legitimate support providers. Accessed status is more likely to be detrimental in collectivistic and less egalitarian societies, whereas unsolicited social support is more harmful in individualistic societies.
Future Directions
Future research in five areas is needed to achieve a more comprehensive understanding and application of the social cost model. First, certain types of relationship and network properties warrant more future research. Relatively speaking, the structural composition and contents of intimate relationships and parenthood and the structural forms and composition of social networks are underexplored. These two patterns may partly reflect methodological challenges. Data collection on these properties requires more time and effort. Mapping certain structural forms and composition of social networks, for example, requires the use of specific network instruments (Perry et al. 2018). In addition, among different indicators of social costs, some content-related (detrimental social control, negative social comparison, burdensome relationship investment) and composition-related (alters’ resource shortage and harmful network norms) costs warrant more direct examination, and diverse indicators of social costs deserve more simultaneous examination.
Second, the pathways linking different relationship and network properties to worse health need more direct and full examination through mediation analysis. In the theoretical causal chain linking the three types of relationship and network properties, contents are most downstream and expected to be most directly and closely related to health, followed by structural composition and structural forms. How contents mediate the effect of structural composition and how contents and structural composition together mediate the impact of structural forms remain understudied. Other possible mechanisms at the ego’s level (ego’s social, behavioral, psychological, and biological characteristics) are also underexplored. In addition, the life course developmental perspective demands more attention. The pathways for how the cumulative continuities of detrimental relationship and network properties operate to damage health over life stages and time are underexamined (Caspi et al. 1989; Whitbeck et al. 2001).
Third, the variation of the harmful impacts of social relationships and social networks deserves more scrutiny. With the exception of gender, other sociodemographic factors are given limited attention for their moderating roles, including sexuality, age, race-ethnicity, and SES. Studies comparing sexual orientation groups are limited to having intimate relationships and having children and neglect other relationship properties and network properties. Studies analyzing racial-ethnic groups ignore the structural forms and composition of social networks. Studies examining age and life course pay little attention to the structural composition of intimate relationships and social networks and the contents of parenthood. Studies examining SES overlook the structural forms, structural composition, and contents of intimate relationships; the structural forms and contents of parenthood; and the structural composition of social networks. Additionally, comparative studies across societies are limited and mainly focus on the structural forms of social relationships and social networks. Whether and how institutional arrangements shape the deleterious consequences of the structural composition and contents of social relationships and social networks remain largely unknown.
Furthermore, the interplay between relationship and network properties requires future research efforts. Despite their theoretical and methodological closeness, social relationships and social networks are rarely jointly examined for their interplay in the social production of social costs and deleterious consequences. They can interplay in damaging health in two ways. First, they can influence each other. One partner’s excessive involvement in social networks or the other partner’s social networks, for example, can create intimate relationship strain and harm the other partner’s health (Cornwell and Laumann 2011; Ermer and Proulx 2020). The other direction is also possible that obligations in intimate relationships may lead to less involvement and more relationship strain in social networks. Second, relationship and network properties can exacerbate each other’s harmful impacts. For instance, ego’s health may suffer more when relationship strain in social relationships and social networks reinforce each other.
In addition, future research needs to take on methodological challenges in three directions. Existing studies are mostly ego centered due to their data limitation. To better distinguish and compare the effects of egos, alters, and their shared attributes, future research on dyadic relationships requires data collection on both sides of such relationships, and future research on social networks should rely on data collection on both ego and alters or full networks (Baller and Richardson 2009; Inanc 2018; Umberson et al. 2020). Also, for the purpose of generalization and causal inferences, prospective longitudinal national data are needed, especially for social network research. In addition, to achieve more direct and causal examination of diverse institutional factors, future larger scale, national-level comparative data collection is necessary.
Finally, the social cost model in combination with the social resource model will stimulate future research on social determinants of health and health interventions. It will trigger more research on the harmful and doubled-edged impacts of relationship and network properties and their interplay with other social antecedents. It will inspire health intervention research to examine not only vulnerable groups who bear more social costs but also doubly disadvantaged groups who lack social resources and face more social costs. This form of double jeopardy has become more salient during the unprecedented COVID-19 pandemic. This pandemic isolates people and hinders the flow of social resources through social ties. Its associated economic and public health crises reinforce some forms of social costs (e.g., alters’ resource shortage, risky social contagion, crossover stress, and demanding social obligations).
Footnotes
Appendix
Acknowledgements
The authors thank the three anonymous reviewers for their extremely helpful comments and suggestions. The first author thanks Anthony R. Bardo, Yanjie Bian, Chih-Jou Jay Chen, Guixiang Chen, Daniel B. Cornfield, Linda K. George, Larry W. Isaac, Nan Lin, and Fu Song for their protective social support.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is partly supported by a Scholar Grant (GS010-A-19) from the Chiang Ching-kuo Foundation for International Scholarly Exchange (PI: Lijun Song).