
Abstract
Although prior research documents adverse health consequences of precarious work, we know less about how chronic exposure to precarious work in midlife shapes health trajectories among aging adults. The present study uses longitudinal data from the Health and Retirement Study to consider how histories of precarious work in later midlife (ages 50–65) shape trajectories of health and mortality risk after age 65. Results show that greater exposure to unemployment, job insecurity, and insufficient work hours in midlife predicts more chronic conditions and functional limitations after age 65. Characteristics of precarious work also predict increased mortality risk in later life. Findings indicate few gender differences in linkages between precarious work and health; however, women are more likely than men to experience job insecurity throughout midlife. Because precarious work is unlikely to abate, results suggest the need to reduce the health consequences of working in precarious jobs.
Employment, especially long-term and consistent employment, is beneficial for health and longevity (Caputo, Pavalko, and Hardy 2020; Frech and Damaske 2012; Pavalko and Smith 1999; Raymo, Halpern-Manners, and Warren 2013; Ross and Mirowsky 1995). At the same time, precarious work—work that is uncertain, unstable, and insecure—is increasingly prevalent and threatens the health of employees. Indeed, prior research shows that working in precarious jobs undermines mental health (for reviews, see Benach et al. 2014; Cheng and Chan 2008; De Witte, Pienaar, and De Cuyper 2016; Kim and von dem Knesebeck 2016), especially when that precarity is chronic rather than episodic (e.g., Burgard, Brand, and House 2009; Burgard and Seelye 2017; Ferrie et al. 2002; Glavin 2015). Emerging evidence also suggests that precarious work may undermine physical health, including cardiometabolic conditions (e.g., Benach et al. 2014; Virtanen et al. 2013) and functional health (Scott-Marshall and Tompa 2011). Although prior research considers the health implications of precarious work, we know less about how histories of precarious work in midlife shape longer-term health trajectories among aging adults.
The present study uses longitudinal data from the Health and Retirement Study (1992–2016) to consider how histories of precarious work in later midlife (ages 50–65) shape trajectories of health and mortality risk after age 65. Because work histories often differ for women and men, the present study examines variation in linkages between precarious work and health by gender. The analysis focuses on physical health (chronic conditions, functional limitations) in addition to mortality risk to demonstrate the widespread long-term implications of experiencing precarious work in midlife. Moreover, the present study considers work characteristics related to unemployment, job security, and work hours as dimensions of precarious work that may be consequential for health and mortality. Guided by a stress and life course perspective (Pearlin et al. 2005), I suggest that precarious work is an often chronic stressor that proliferates across the life course and “gets under the skin” to influence health over time. The present study aims to understand whether health disparities by precarious work histories widen as adults enter later life or whether these disparities stabilize in later life.
Addressing these questions is important in light of a steady rise in precarious work (Fullerton and Wallace 2007; Kalleberg 2018) alongside increases in functional limitations (Martin and Schoeni 2014; Zajacova and Montez 2018) and midlife mortality rates (Case and Deaton 2015; Woolf et al. 2018) in the United States. Precarious work may be especially stressful for this cohort of adults that experienced the expansion of precarious work over much of their working career. Moreover, the present study contributes to research on work and health by harnessing years of longitudinal data to consider how histories of insecure and unstable work in midlife can shape long-term patterns of health and mortality in later life. This approach extends prior research that tends to focus on the consequences of precarious work for health at one point in time. With an aging and increasingly unhealthy population, the persistence of precarious work in the labor force is a substantial threat to population health in the twenty-first century.
Background
Precarious Work and Health
The declining health of Americans is of great concern. The prevalence of functional limitations and disability among nonelderly, midlife adults increased over the early twenty-first century (e.g., Martin and Schoeni 2014; Zajacova and Montez 2018), and mortality rates increased for midlife Americans across all racial-ethnic groups in recent years (Woolf et al. 2018). Scholars have long pointed to the importance of examining several dimensions of health and well-being given the multiple and intertwined ways that social exposures affect health (e.g., Kuh et al. 2003; Lynch and Smith 2005). Moreover, the disablement process framework (Verbrugge and Jette 1994) explicates how disease, disability, and death are interrelated: Pathological disruptions (e.g., health conditions) lead to impairments and functional limitations, which can be precursors to hospitalization and death. As such, the present study focuses on three outcomes corresponding to the disablement framework: chronic conditions, functional limitations, and mortality.
The disablement process framework further emphasizes that functional problems tend to manifest because of biopsychosocial and demographic risk factors, including broad social changes (Verbrugge 2016). The present study is guided by a conceptual framework wherein exposure to precarious work is a risk factor for subsequent health problems, functional limitations, and mortality risk. Indeed, the rise in precarious work marks a major social shift over the past 50 years. Compared to previous generations, contemporary working adults are more likely to experience job insecurity, unpredictable work hours, involuntary part-time employment, nonstandard work contracts, and limited workplace benefits during their careers (e.g., Benach et al. 2016; Kalleberg 2018; Lambert, Fugiel, and Henly 2014). In general, employment is increasingly unlikely to resemble the standard employment relationship of the past that guaranteed long-term stability and generous social benefits for employees. Instead, employers now strive for more flexible and profitable forms of employment, which often result in lower wages, fewer benefits, and more insecurity for workers (Hyman 2018; Kalleberg 2011).
In line with prior research, I focus on unemployment, job insecurity, and insufficient work hours as measures of precarious work in the present study. Experiences of frequent unemployment over time may tap into dimensions of employment instability that characterize precarious work. In addition to instability, job insecurity (both objective and perceived) is a defining feature precarious work (Kalleberg 2018), especially when experienced for many years. For example, the length of time a person has worked for an employer is an objective measure of job insecurity, and a history of short job tenure could indicate frequent changes in employment that contrast long-term, secure employment (e.g., Kalleberg 2018). Moreover, a vast literature documents the consequences of perceived job insecurity for workers (e.g., Benach et al. 2014; Burgard et al. 2009; Cheng and Chan 2008; De Witte et al. 2016; Ferrie et al. 2002; Heaney, Israel, and House 1994).
An examination of insufficient work hours may capture precarious arrangements related to employment contracts and/or wages. Indeed, low wages (Kalleberg, Reskin, and Hudson 2000), a lack of schedule control (Lambert et al. 2014), and part-time work (Kalleberg 2018; Peckham et al. 2019) are dimensions of precarious work examined in prior research, and these dimensions likely relate to insufficient work hours. Although not an exhaustive list of indicators of precarious work, unemployment, job insecurity, and insufficient work hours represent deviations from the standard employment relationship. Moreover, these forms of precarity may be particularly stressful and disruptive for workers. The present study harnesses these measures of precarious work to consider the long-term health implications of a history of precarious work for aging adults.
Prior research documents linkages between precarious work and mental and physical health. Indeed, the consequences of precarious work—especially job insecurity—for mental health are well established (for reviews, see Benach et al. 2014; Cheng and Chan 2008; De Witte et al. 2016; Kim and von dem Knesebeck 2016). Although prior research focuses less on how working in precarious jobs might influence physical health outcomes, existing evidence suggests that precarious work undermines self-rated health (e.g., Benach et al. 2014; Burgard et al. 2009; De Witte et al. 2016; Ferrie et al. 2002; Glavin 2015; Lewchuk 2017; Peckham et al. 2019) and cardiometabolic health (e.g., Benach et al. 2014; De Witte et al. 2016; Lee et al. 2004; Virtanen et al. 2013). However, much remains to be known about how precarious work influences other physical health outcomes, such as chronic conditions and functional limitations, and mortality risk.
Although evidence suggests that experiencing precarious work can take a toll on mental and physical health, we lack an understanding of how a history of precarious work in midlife can contribute to lasting health disparities in later life. Scholars increasingly use longitudinal data to provide needed insights into the consequences of persistent and chronic job insecurity for psychological distress, self-rated health, and heart disease (e.g., Burgard et al. 2009; Burgard and Seelye 2017; Ferrie et al. 2002; Glavin 2015; Lee et al. 2004). Although these studies highlight the importance of stress duration, they tend to focus on health outcomes at only one or two follow-up periods. For example, in a review of longitudinal research on job insecurity and health and well-being (De Witte et al. 2016), only one study (Scott-Marshall 2010) examined health trajectories relative to precarious work. Scott-Marshall (2010) found that exposure to workplace insecurity resulted in a deviation in self-rated health over time for Canadian workers, especially for midlife adults compared to younger workers. As such, the present study addresses a knowledge gap by examining how a midlife career characterized by a history of precarious work (i.e., ages 50–65) shapes long-term trajectories of health and mortality risk in later life (i.e., after age 65). That is, histories of precarious work in midlife may create health disparities between workers with stable, secure employment and those with instability and insecurity at work, and that health disparity may persist as adults enter later life.
The present study relies on a blended stress and life course perspective to understand how exposure to precarious work throughout midlife shapes trajectories of health and mortality risk after age 65. A stress and life course perspective suggests that stress, such as the stress from precarious work, proliferates across the life course to impact long-term health patterns (Pearlin et al. 2005; Pearlin and Skaff 1996). For example, job insecurity can lead to feelings of hopelessness and a lack of personal control among workers (Benach et al. 2014), and these psychological responses have well-documented adverse consequences for health and well-being (Mirowsky and Ross 2003). In addition to the stress of working in an insecure or unstable job, precarious work may involve greater material deprivation and physical exposures that compromise the mental and physical health of workers (Benach et al. 2016; Burgard and Lin 2013; Peckham et al. 2019; Scott-Marshall and Tompa 2011), especially when sustained over time.
A central component of a stress and life course perspective requires attention to how these stress processes unfold over the life course. Put differently, does the amount of exposure to precarious work in midlife create diverging trajectories of health in later life? By considering trajectories of health and mortality risk in later life, the present study aims to understand whether health disparities by precarious work histories continue to widen in later life or whether these disparities stabilize once workers enter late life. Theories of cumulative (dis)advantage imply that risks and resources accumulate over time to produce diverging trajectories of health with age (e.g., Hatch 2005; Willson, Shuey, and Elder 2007). This theory suggests that the risks of consistent precarity and the rewards of stable and secure employment would lead to diverging patterns of health for aging adults. That is, the health risks from low wages, physical exposure, and chronic stress likely accumulate and act as chains of risk over the life course. Disparities in health and well-being between workers in precarious jobs and workers in stable jobs, then, could be expected to widen throughout the life course. However, prior research does not consider whether a history of precarious work in midlife will create health disparities that subsequently widen, narrow, or remain stable as adults age. This gap in the literature necessitates an examination of long-term health trajectories across later life.
Gender, Precarious Work, and Health
Because gender structures experiences in the labor force, the present study considers whether histories of precarious work shape health trajectories in different ways for women and men. Historically, women have been more likely than men to work in less secure and less stable jobs (e.g., Hatton 2008; Kalleberg 2018). With the return of men in need of employment after World War II, women were encouraged to give up their wartime jobs and to work in temporary positions instead. Companies conveyed this temporary work as desirable for women—work that was respectable but still marginal and secondary to the domestic sphere (Hatton 2008). In more recent decades, with increased labor force participation among women, many hypothesized that the emergence of flexible work would be beneficial for women, allowing them to have self-directed careers and to easily balance family and work demands (e.g., Goldin 2014; Hewlett 2007). Workplace flexibility can be a double-edged sword, however, when it is accompanied by low wages, few social benefits, unpredictable work schedules, and job insecurity.
Gender differences in exposure to precarious work continue to evolve as men are increasingly likely to experience insecurity and instability in their careers as precarious work becomes more widespread (Kalleberg 2018). The transformations of work in the twentieth century characterized by flexible work arrangements, temporary contracts, job insecurity, and stagnant wages likely affect men and women alike. Whereas men may retain some of their societal advantages, they may simply be on a “higher ring in hell” in the context of unstable and insecure work (Williams 2013:623). Despite these contemporary changes in the likelihood of precarious work, the current generation of older adults likely experienced gendered work histories wherein women’s careers were characterized by a longer history of insecurity and instability compared to men.
Differences between men and women in exposure to precarious work has myriad implications for health. For example, if women experience more insecure and unstable work throughout midlife, differential exposure to precarious work could add to already higher rates of physical morbidities among women (Case and Paxson 2005). Men and women may also react differently to precarious work with differential consequences for health, but prior research produces inconsistent findings (e.g., Benach et al. 2014; Kivimäki and Kawachi 2015; Scott-Marshall 2010). On the one hand, women may experience more severe health consequences of precarious work if the stress from precarity is accompanied by additional gender-based stressors such as workplace discrimination, family demands, and work–family conflict (Menéndez et al. 2007). Indeed, workplace flexibility that requires constant availability and/or an unpredictable work schedules could make it challenging for women to balance family demands (Williams 2013) in ways that create a greater stress burden and more adverse health outcomes for women compared to men. On the other hand, men in precarious work may experience a feeling of relative deprivation when working in precarious jobs because their advantaged status had previously protected them from this kind of work (Kalleberg 2018). As such, compared to women, men may experience more adverse health consequences when working in precarious jobs. These competing possibilities necessitate an examination of whether linkages between precarious work and health differ for women and for men.
The Present Study
Taken together, the present study extends prior research on work and health by (1) examining how histories of exposure to precarious work throughout midlife contribute to adverse health outcomes over a longer period among adults entering later life, (2) considering the consequences for physical health (chronic conditions, functional limitations) and mortality risk, and (3) exploring differences in these processes for women and for men. I analyze nationally representative longitudinal data from the Health and Retirement Study to address the following specific research questions:
Research Question 1: How is precarious work history throughout later midlife (ages 50–65) associated with trajectories of physical health and mortality risk after age 65?
Research Question 2: Is there variation in these associations by gender?
Midlife is an important time in the life course when considering the implications of work. The likelihood of experiencing job insecurity increases midcareer (Fullerton and Wallace 2007), and older workers tend to work in lower quality jobs when they are reemployed after losing a job (Lippmann 2008). Midlife workers may also experience more stress when faced with insecure and unstable work because midlife is a time marked by significant responsibilities (e.g., family obligations, health care costs, etc.) that may amplify the consequences of precarious work. Indeed, midlife workers report greater distress and worse self-rated health in response to persistent insecurity compared to younger workers (Glavin 2015; Scott-Marshall 2010). As such, the present study focuses on experiences of precarious work throughout midlife because these experiences likely shape long-term patterns of health for aging adults.
Data and Methods
Sample
Data came from the 1992 to 2016 waves of the Health and Retirement Study (HRS), a nationally representative sample of the U.S. population over age 50. The HRS is an ongoing, biannual survey that began in 1992 with a sample of adults ages 51 to 61 and adds a new cohort of adults ages 51 to 56 every 6 years. The HRS also surveys the spouses of focal respondents, some of whom are younger or older than the age range of focal respondents. The analysis of the present study focused on how precarious work histories from ages 50 to 65 shape trajectories of health and mortality risk after age 65. Respondents needed to meet two key criteria for inclusion in the analytic sample: (1) They must have been less than 65 years old for at least two waves to estimate work history measures, and (2) they must have remained in the study until age 65 to assess health trajectories after age 65.
The analytic sample necessarily excluded respondents who were unemployed or out of the labor force in every wave between ages 50 and 65 because these respondents did not answer questions related to precarious work. The present study also excluded respondents who were missing data on chronic conditions and functional limitations and any of the measures of precarious work described in the following. The analytic sample was comprised of 8,283 adults. Because of the survey design of the HRS, respondents who entered the study in a later cohort had a shorter follow-up period to observe health trajectories.
Measures
Health and mortality
Chronic conditions counted the number of doctor-diagnosed conditions, including high blood pressure or hypertension, diabetes or high blood sugar, cancer or a malignant tumor (excluding skin cancer), chronic lung disease (excluding asthma), heart attack or other heart problems, stroke or transient ischemic attack, and arthritis or rheumatism. Affirmative responses were summed, with higher values indicating more chronic conditions (range = 0–7). Chronic conditions had a fairly normal distribution in this aging sample (M = 2.18, SD = 1.33, skewness = .36).
Functional limitations counted the number of activities a respondent had some difficulty completing: walking one block; sitting for about 2 hours; getting up from a chair after sitting for long periods; climbing one flight of stairs without resting; stooping, kneeling, or crouching; lifting or carrying weights over 10 pounds; picking up a dime from the table; reaching arms above shoulder level; and pushing or pulling large objects. Affirmative responses were summed, with higher values indicating more functional limitations (range = 0–9). This approach aligns with prior research examining functional limitations in adult populations (e.g., Caputo et al. 2020; Verbrugge, Brown, and Zajacova 2017; Verbrugge and Yang 2002). The distribution of functional limitations was slightly skewed (skewness = .99; M = 2.09, SD = 2.32).
The present study also assessed all-cause mortality after age 65. Measurement of mortality came from the National Death Index and proxy reports from living family members, capturing deaths occurring from 1992 to 2016. The mortality data in the HRS have been validated by comparisons to life tables and are considered effectively complete (Weir 2016).
Precarious work history in midlife
Analyses also examined respondents’ histories of precarious work between ages 50 and 65, including the proportion of waves unemployed, the proportion of waves with short job tenure, the proportion of waves with high job insecurity, and the proportion of waves with insufficient work hours. For each of these measures, I divided the number of waves workers experienced the precarious characteristic by the number of nonmissing waves between ages 50 and 65 to accurately compare workers with unequal rates of participation in the HRS. This approach prevented the exclusion of respondents who missed a wave between ages 50 to 65 or respondents who entered the study at age 55 instead of age 50, for example.
At each wave, respondents reported their employment status, including employed, unemployed, retired, and out of the labor force (disabled, homemaker). Workers who were precariously employed may have experienced spells of unemployment. Therefore, the present study considered a midlife history of unemployment as a measure of precarious work history. For each wave, a dichotomous measure equaled 1 if the respondent was unemployed and 0 if employed and working for pay. Respondents who were out of the labor force at the time of the survey were coded as missing. The proportion of waves unemployed reflected the average number of waves between ages 50 and 65 that respondents were unemployed. Because I excluded respondents who were unemployed at every wave, this measure ranged from 0 to .75, where 0 indicated that the respondent was working for pay in every surveyed wave, and values closer to .75 indicated more frequent experiences of unemployment in nonmissing waves.
Employer tenure, a measure of objective job insecurity, was assessed in the HRS by asking respondents how many years they have worked in their current job. For each wave, I created a dichotomous indicator of short job tenure by classifying 2 years or less as short job tenure (the lowest quintile of the distribution), with a job tenure of 3 or more years as the reference group. The proportion of waves with short tenure reflected the average number of waves between ages 50 and 65 that respondents were classified as having short job tenure. This measure ranged from 0 to 1, where 0 indicated that the respondent never experienced short job tenure and 1 indicated that the respondent experienced short job tenure at every nonmissing wave.
Perceived job insecurity is a common measure of subjective job insecurity. Respondents answered the question, “What are the chances that you will lose your job during the next year?” by providing a number between 0 (absolutely no chance) and 100 (absolutely certain). I created a dichotomous measure so that a value of 1 indicated high job insecurity (≥50% chance that they will lose their job; the highest quintile of the distribution) and 0 indicated little job insecurity (<50% chance). To measure the proportion of waves with high job insecurity, I took the average of waves with high job insecurity between ages 50 and 65 (range = 0–1).
In each wave, respondents were asked whether they would like to increase the number of hours they work each week (with earnings increasing proportionally). An affirmative response to this question indicated that the respondent experienced insufficient work hours and was coded as 1. Respondents could report insufficient work hours for a number of reasons; for example, they could be working part-time when they would rather be working full-time, or they may live in a lower income household that would benefit from additional income regardless of work status. To understand this measure better, I examined the distribution of part-time work, mean hourly wages, and household income when respondents reported insufficient work hours in midlife. Household income emerged as the biggest factor determining the report of insufficient work hours. Household income and part-time work also intersected such that low-income part-time workers were most likely to report insufficient work hours. To assess the proportion of waves with insufficient work hours, I calculated the average number of waves respondents wanted to increase their work hours between ages 50 and 65 (range = 0–1).
These four measures of precarious work history demonstrated weak correlations with each other, suggesting that they likely reflect distinct dimensions of precarious work. Perhaps unsurprisingly, the two strongest correlations were between unemployment and short job tenure (r = .28) and short job tenure and high job insecurity (r = .21).
Covariates
All analyses accounted for sociodemographic covariates that may be associated with work and health. These covariates included age (in years), race (non-Hispanic white [reference], non-Hispanic Black, Hispanic, “other” non-Hispanic race), gender (1 = female), and educational attainment (less than high school [reference], high school diploma, some college, college degree or more). To account for some of the selection of healthier people into work, I included an indicator of whether respondents reported at their baseline interview that an impairment or health problem limited the kind or amount of paid work they can do (1 = yes). I further controlled for whether respondents rated their health in childhood as fair or poor (1 = yes) to control for some selection occurring earlier in the life course.
Analyses also accounted for marital status at age 65 (married [reference], divorced, widowed, never married), region of residence at age 65 (Northeast [reference], Midwest, South, West), the longest tenure occupation by age 65 (white collar [reference], blue collar, and other/farm/military), and standardized household wealth at age 65. Because the present study examines work in the later midlife period when adults are approaching retirement, analyses included an indicator of whether the respondent reported being fully retired in at least one wave between ages 50 and 65 (1 = yes). Models also included a measure of the proportion of waves between ages 50 and 65 when the respondent reported that their job required lots of physical effort (1 = most of the time/almost all the time) to account for different burdens of physical exposures in midlife. Finally, I included measures of each health outcome at baseline to account for health status in midlife.
Analytic Strategy
The aim of the present study is to assess whether and how histories of precarious work in midlife shape longer-term health trajectories and mortality risk after age 65. As such, I used linear growth models to examine changes in chronic conditions and functional limitations after age 65. For the linear growth models, an interaction of age (centered at 65) with the precarious work measure was included to test whether differences in health by precarious work history widen, narrow, or remain stable after age 65. Thus, the main effect for each measure of precarious work represents the difference in health by precarious work history at age 65; the interaction represents differences in the rate of change after age 65 by precarious work history. Age was also included as a random effect in the linear growth models.
To examine mortality risk, I used discrete-time event history modeling to examine how a history of precarious work in midlife was associated with mortality risk after age 65. Age (in years; centered at 65) was used as the time metric. For the linear growth models and the discrete-time models, the oldest participants were observed until age 86. Participants contributed an average of 4.7 waves of data after age 65, with approximately 70% of respondents in the analytic sample providing three or more waves of data after age 65.
All analyses accounted for the complex survey design of the HRS. The descriptive statistics in Table 1 include the respondent-level baseline weights. The growth curve and event history analyses did not include weights because the models included covariates related to sample selection (e.g., age, race, gender), and this approach tends to produce unbiased coefficients without weights (Heeringa, West, and Berglund 2017; Winship and Radbill 1994). The key coefficients of interest are presented in Tables 2 through 4, and full tables are available on request.
Selection
The present study contended with at least two issues of selection. One concern was that by examining experiences of precarious work in midlife (i.e., age 50 and older), the present study could not account for the selection of unhealthy individuals into precarious jobs earlier in the life course. This issue was more difficult to address using the HRS, and I discuss limitations of this approach below. However, analyses included a measure of childhood health to account for some of the selection into precarious work that might have occurred before participants entered the study. Analyses also included a measure of whether the respondent’s health limited their work at the baseline interview to account for selection into precarious work during midlife.
A second issue concerned nonrandom attrition during the study period. Because the analyses examined health and mortality after age 65, one concern was that participants in the HRS who died or dropped out of the study before age 65 (n = 3,176) were not included in the analytic sample. As a sensitivity test, I compared the attrited sample to the analytic sample based on sociodemographic covariates. Appendix A in the online version of the article shows some differences by age, educational attainment, marital status, and household income. Notably, respondents in the attrited sample were more likely to report that health limits their ability to work at baseline, more chronic conditions at baseline, and more functional limitations at baseline. To test whether nonrandom attrition biased results in the present study, I used inverse probability weights to adjust the analytic sample. Results in Appendix B in the online version of the article present the relevant coefficients for each measure of precarious work when including these weights. Findings were similar to results without inverse probability weights, suggesting that nonrandom attrition did not substantially change the pattern of results.
Results
Descriptive Results
Descriptive statistics for the analytic sample are presented in Table 1. On average, unemployment during midlife (ages 50–65) is not common in the sample. However, experiences of job insecurity and insufficient work hours in midlife are relatively common. Respondents reported short job tenure, high job insecurity, and insufficient work hours in about 20% of their working waves during midlife (ages 50–65). Table 1 shows notable differences in work and health for men and women. Precarious work histories looked slightly different for women and men wherein women experienced more short job tenure and high job insecurity throughout midlife. Turning to health outcomes, descriptive results demonstrate that women report more functional limitations than men. However, a greater percentage of men died during the study (17%) compared to women (13%). These patterns align with prior research suggesting that women experience worse physical health compared to men despite living longer lives (e.g., Case and Paxson 2005).
Weighted Descriptive Data for the Analytic Sample, by Gender with Data from Health and Retirement Study, Waves 1992–2016 (n = 8,283).

Note: Asterik indicates significant differences between women and men, p < .05.
Precarious Work History and Health Trajectories in Later Life
Table 2 presents results from linear growth models testing associations between precarious work history in midlife (ages 50–65) and health trajectories after age 65. Starting with chronic conditions, Panel A shows that the proportion of waves unemployed is positively associated with chronic conditions at age 65 (Model 1, p < .01) such that adults who experienced more waves of unemployment throughout later midlife reported about one-third more chronic conditions at age 65 than adults who did not experience unemployment in midlife, net of covariates. The interaction term between age and the proportion of waves unemployed is significant and negative, indicating that this disparity in chronic conditions narrows slightly after age 65. Moreover, the proportion of waves with high job insecurity (Model 3, p < .01) and insufficient work hours (Model 4, p < .05) is associated with chronic conditions at age 65, net of covariates. These disparities in chronic conditions persist after age 65, as indicated by the nonsignificant interaction terms with age. The proportion of waves with short job tenure (Model 2) was not a significant predictor of chronic conditions as adults enter later life.
Linear Growth Models Predicting Chronic Conditions and Functional Limitations by Precarious Work History with Data from Health and Retirement Study, Waves 1992–2016 (n = 8,283).
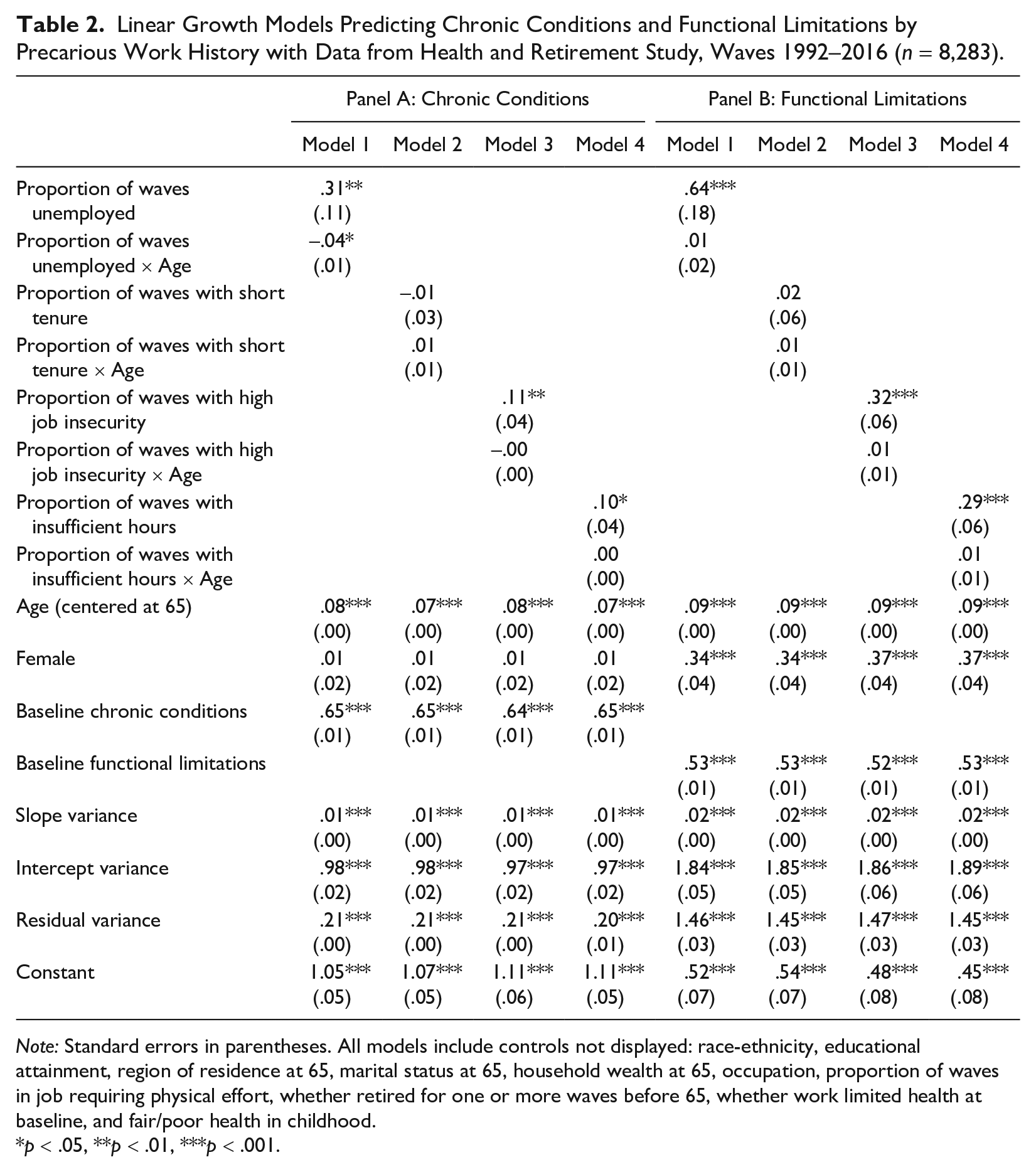
Note: Standard errors in parentheses. All models include controls not displayed: race-ethnicity, educational attainment, region of residence at 65, marital status at 65, household wealth at 65, occupation, proportion of waves in job requiring physical effort, whether retired for one or more waves before 65, whether work limited health at baseline, and fair/poor health in childhood.
p < .05, **p < .01, ***p < .001.
Panel B of Table 2 presents the results for linear growth models estimating the association between midlife precarious work histories (ages 50–65) and functional limitations after age 65. Results again point to the importance of histories of unemployment, high job insecurity, and insufficient work hours. That is, the proportions of waves unemployed (Model 1, p < .001), with high job insecurity (Model 3, p < .001), and with insufficient work hours (Model 4, p < .001) are positively associated with functional limitations at age 65, net of covariates. For example, adults who experienced more waves with insufficient work hours in midlife had functional limitation scores .29 points higher than adults who never experienced insufficient work hours in midlife at age 65. Moreover, the nonsignificant interaction terms with age indicate that the disparities in functional limitations by precarious work histories remain stable after age 65. The proportion of waves with short job tenure during midlife (Model 2) was not associated with functional limitations in later life.
Overall, findings in Table 2 suggested that precarious work in midlife—primarily unemployment, high job insecurity, and insufficient work hours—is associated with more chronic conditions and functional limitations as adults enter later life. Importantly, the positive associations between precarious work history and health outcomes persist when accounting for sociodemographic characteristics, childhood and baseline health measures, physical exposure risks, and socioeconomic conditions by age 65 (e.g., household wealth, occupation, midlife retirement history).
Precarious Work History and Mortality Risk in Later Life
Table 3 presents the results from discrete-time event history models predicting mortality risk after age 65; age (centered at 65) is used as the metric of time. Results in Model 1 show that the proportion of waves unemployed is associated with increased mortality risk (p < .05) such that adults with more waves of unemployment throughout later midlife have 46% greater odds of subsequent mortality after age 65 compared to adults without unemployment in midlife (coefficient = .38; odds ratio [OR] = 1.46). Moreover, experiencing insufficient work hours in midlife is associated with mortality risk (Model 4, p < .01), net of covariates. That is, adults who wanted to increase their work hours throughout later midlife had almost 30% greater odds of mortality compared to adults who never wanted to increase their work hours in later midlife (coefficient = .24; OR = 1.27). A history of short job tenure and a history of high job insecurity throughout midlife (ages 50–65) are not associated with heightened mortality risk, net of covariates. Overall, Table 3 provides evidence that precarious work in midlife—primarily unemployment and insufficient work hours—is associated with higher mortality risk among aging adults.
Discrete-Time Hazard Models Predicting Mortality Risk after Age 65 by Precarious Work History with Data from Health and Retirement Study, Waves 1992–2016 (n = 8,283).

Note: Standard errors in parentheses. All models include controls not displayed: race-ethnicity, educational attainment, region of residence at 65, marital status at 65, household wealth at 65, occupation, proportion of waves in job requiring physical effort, whether retired for one or more waves before 65, whether work limited health at baseline, and fair/poor health in childhood.
p < .05, **p < .01, ***p < .001.
Gender Differences in Precarious Work History and Health
To understand whether associations between precarious work history and health differ for women and for men, I include an interaction of gender with measures of precarious work history. Growth curve models also include an interaction of gender, precarious work history, and age. Starting with chronic conditions, findings suggest that the disparity in chronic conditions at age 65 by unemployment history is greater for women compared to men. For short job tenure, a higher proportion of waves with short job tenure in midlife is associated with an increase in chronic conditions after age 65 for men but not for women.
Turning to functional limitations, a consistent pattern emerges when examining gender differences in the consequences of short job tenure, high job insecurity, and insufficient work hours. For men, a history of these characteristics of precarious work is associated with a faster increase in functional limitations after age 65 compared to men who did not experience a history of short job tenure, high job insecurity, and insufficient work hours (as indicated by the significant interaction of precarious work and age). For women, experiencing more exposure to precarious work in midlife is associated with more functional limitations at age 65 compared to women who did not experience precarious work; however, this disparity remains stable after age 65.
For mortality risk, interactions of gender with measures of precarious work history test whether associations between precarious work history and mortality risk after age 65 differ for women and for men. None of the interaction terms are statistically significant, suggesting similar consequences of precarious work for mortality risk for women and men.
I present the predicted scores of functional limitations by midlife job insecurity for women (dashed lines) and for men (solid lines) in Figure 1. These results are based on estimates from Table 4, Panel B. For ease of interpretation, I show three experiences of midlife job insecurity: workers who never experienced high job insecurity in midlife, workers who experienced high job insecurity half of the time in midlife, and workers who experienced high job insecurity in every wave that they were working in midlife. I highlight three main findings from this figure. First, Figure 1 shows a bigger difference in functional limitations at age 65 by a history of job insecurity for women compared to men. Women who never experienced high job insecurity between ages 50 and 65 report fewer functional limitations at age 65 compared to women who experienced high job insecurity in half or all their working waves in later midlife. Second, Figure 1 shows that these disparities in functional limitations by job insecurity remain stable in later life for women, whereas the disparity widens for men. Although men do not experience a disparity in functional limitations by job insecurity history at age 65, by their late 70s, men exhibit a similar gradient in functional limitations as women. Finally, Figure 1 shows that women report more functional limitations than men at the same level of job insecurity.
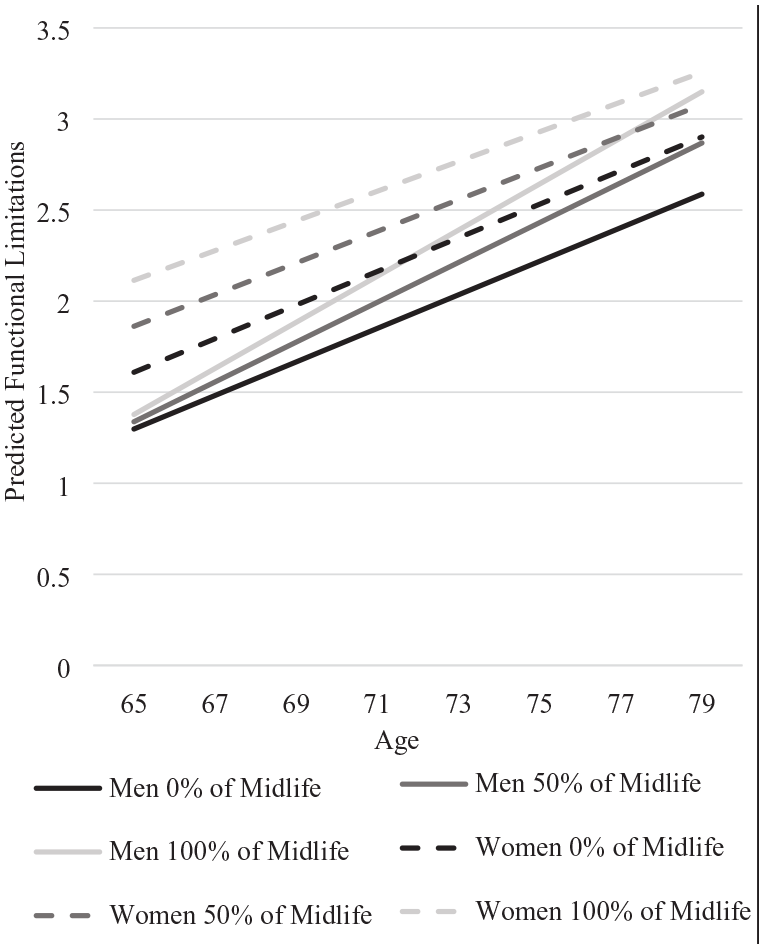
Predicted Number of Functional Limitations by Proportion of Waves with High Job Insecurity in Midlife for Women and Men with Data from the Health and Retirement Study, Waves 1992–2016.
Results from Growth Models (Chronic Conditions, Functional Limitations) and Discrete-Time Hazard Models (Mortality) on Precarious Work and Gender with Data from Health and Retirement Study, Waves 1992–2016 (n = 8,283).
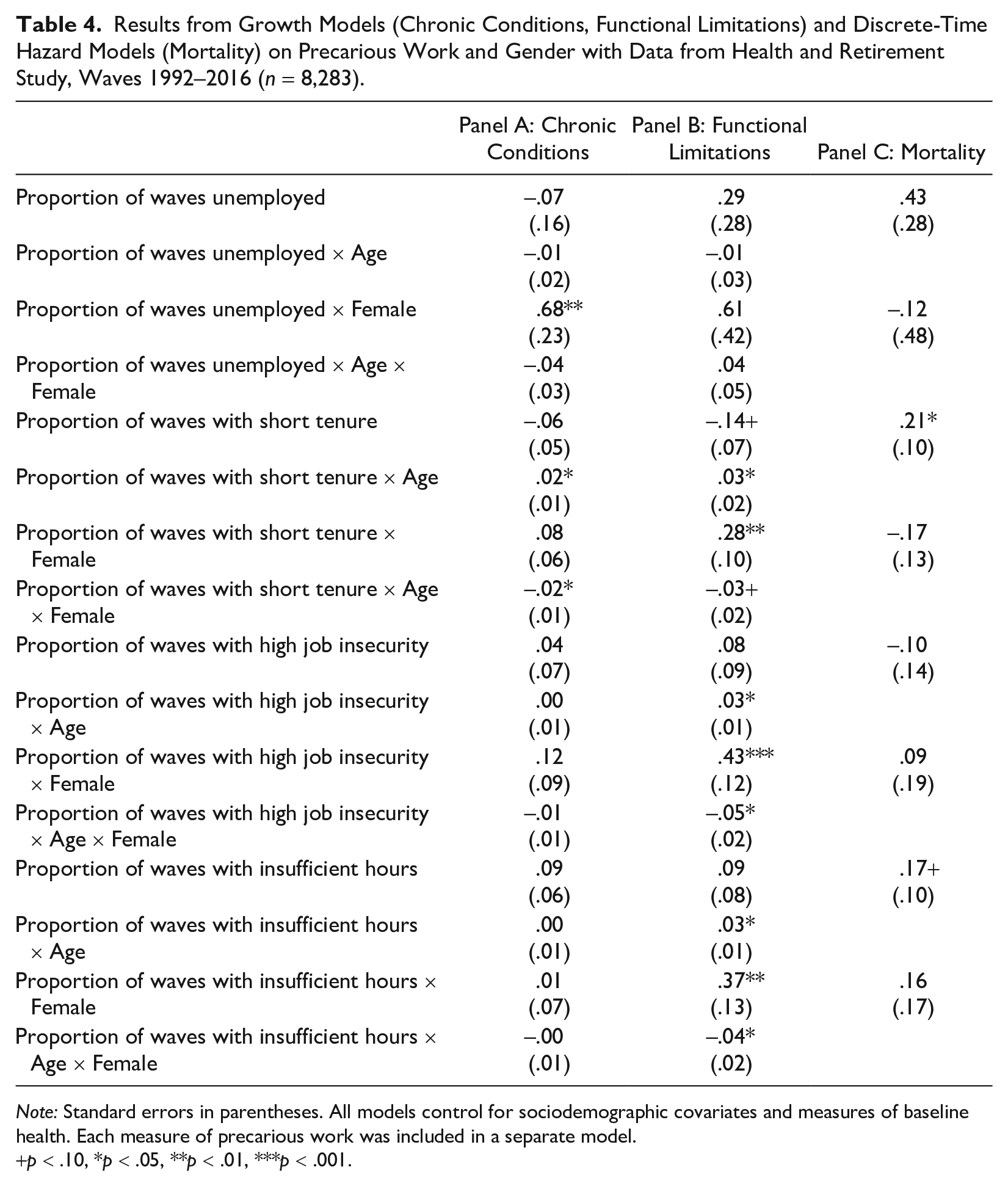
Note: Standard errors in parentheses. All models control for sociodemographic covariates and measures of baseline health. Each measure of precarious work was included in a separate model.
p < .10, *p < .05, **p < .01, ***p < .001.
Sensitivity Analyses
As a sensitivity check, I consider mean job tenure in midlife by averaging job tenure (in years) across all nonmissing waves (M = 13 years, range = 0–48). I also consider mean job insecurity by averaging perceived job insecurity across nonmissing waves (M = 14, range = 0–100). This approach tests whether the results in the present study are sensitive to the assigned cutoff for short job tenure and high job insecurity. The pattern of results (available on request) is similar with these measures. The only difference is that mean job tenure in midlife is associated with functional limitations such that each 10 years of additional mean tenure is associated with .04 fewer limitations at age 65, with a stable disparity after age 65.
Because changes to work and retirement are likely to become more common after age 60, I ensure that the pattern of results does not change when examining precarious work history from age 50 to 60 and the consequences for health and mortality after age 60. This approach also allows more observation points and includes respondents who died between 60 and 65 by modeling trajectories after age 60 instead of age 65 (n = 10,422). The pattern of results is similar to the results in the present study, and key coefficients are presented in Appendix C in the online version of the article.
Discussion
Precarious work is ever more common in the United States, and workers are increasingly likely to experience some form of insecure or unstable employment during their career. Prior research documents that working in precarious jobs undermines mental health (for reviews, see Benach et al. 2014; Cheng and Chan 2008; De Witte et al. 2016; Kim and von dem Knesebeck 2016; Virtanen et al. 2005) and some physical health outcomes (e.g., Benach et al. 2014; Scott-Marshall and Tompa 2011; Virtanen et al. 2013). As such, the well-documented benefits of paid employment for health (e.g., Pavalko and Smith 1999; Raymo et al. 2013; Ross and Mirowsky 1995) may be complicated when workers experience chronic precarity during their career. The present study examined how histories of precarious work in later midlife (ages 50–65) shape longer-term health trajectories and mortality risk among aging adults. I highlight three major themes from the findings in the following.
First, exposure to precarious work in multiple waves throughout later midlife, primarily unemployment, high perceived job insecurity, and insufficient work hours, has lasting consequences for chronic conditions and functional limitations after age 65. Moreover, a history of unemployment and insufficient work hours in later midlife is associated with increased mortality risk after age 65. A history of short job tenure in midlife—a measure of objective job insecurity—was not associated with health and mortality in later life, suggesting that perceived job insecurity may be a more meaningful determinant of long-term health outcomes. Although prior research documents that chronic precarity undermines health at one point in time (e.g., Burgard et al. 2009; Burgard and Seelye 2017; Ferrie et al. 2002; Glavin 2015; Lee et al. 2004), the present study builds on this research to show that exposure to precarious work in midlife shapes long-term patterns of health and mortality in later life. The present study also builds on research documenting the benefits of consistent employment for long-term health trajectories (e.g., Caputo et al. 2020; Frech and Damaske 2012; Raymo et al. 2013) by emphasizing the health risks stemming from long-term exposure to precarious work. Although paid work provides health-enhancing resources, the rise in precarious work threatens traditional understandings of the association between work and health.
A likely explanation for diverging health between workers experiencing long-term precarity and workers with long-term stability is that the health risks associated with low wages, physical exposure, and chronic stress accumulate and unfold over the life course, contributing to health disparities by retirement. Indeed, cumulative (dis)advantage theory posits that risks accumulate over time to produce diverging trajectories of health with age (e.g., Hatch 2005; Willson et al. 2007). Notably, the magnitude of some coefficients was modest, especially for associations between precarious work history and chronic conditions. However, results provide evidence for the lasting effects of precarious work in midlife net of childhood and baseline health. Findings were robust to many hypothesized mechanisms, such as occupation, wealth, and physical exposure, indicating that the health risks of precarious work extend beyond low wages and physical exposure. Thus, chronic stress (Pearlin et al. 2005; Pearlin and Skaff 1996) may be a key reason why histories of precarious work have enduring consequences for health and mortality. Moreover, prior research finds that exposure to precarious work can have greater health consequences for midlife workers compared to younger workers (Glavin 2015; Scott-Marshall 2010), pointing to the importance of examining histories of precarious work in midlife. Linkages between precarious work and health are likely dynamic and multifaceted, and an avenue for future research is to explore the specific mechanisms linking long-term histories of precarious work and long-term patterns of health.
A second theme concerns the persistence of health differences between workers with precarious work experiences and those without such experiences after age 65. One possibility is that the stress from precarious work lessens or dissipates after retirement, halting the accumulation of risk and disadvantage in later life. Another possibility is that social programs that target older adults (e.g., Medicare and Social Security) successfully counter some of the disadvantages associated with precarious work, resulting in stable health disparities after age 65. A final possible explanation is that workers who experience decades of instability and insecurity and survive to age 65 may be more resilient, which would suggest an underestimated disparity between those with histories of precarious work and those with long-term work stability. This possibility highlights the importance of examining exposure to precarious work throughout the entire working career in future research.
A final theme involves gendered experiences of precarious work history and long-term health outcomes given that associations between precarious work and chronic conditions and mortality were mostly similar for women and men in the present study. The overall lack of gender differences aligns with prior research on the similar effects of job insecurity and work stress for cardiovascular disease (Kivimäki and Kawachi 2015; Virtanen et al. 2013) and self-rated health (Scott-Marshall 2010). A possible explanation for the relatively similar health consequences of precarious work may be due to gendered responses to work that ultimately balance out over time. For example, women may experience more severe health consequences if the stress from precarious work is accompanied by additional gender-based stressors such as workplace discrimination and family demands (Menéndez et al. 2007). Conversely, experiencing chronic instability and insecurity could be especially distressing and health-damaging for men, given their historical advantage in the workplace (Kalleberg 2018). Another possibility is that precarious work truly affects the health of women and men in similar ways. Exposure to flexible work arrangements, job insecurity, and stagnating wages likely affects women and men alike because precarious work tends to be detrimental for all workers (Williams 2013). Indeed, although women have historically been more likely to work in insecure and unstable jobs (e.g., Hatton 2008; Kalleberg 2018), the rise in precarious work may “defeminize” this kind of work.
Although the adverse health consequences of precarious work are mostly similar for women and for men in the present study, gender differences in exposure can unequally burden the health of women. Compared to men, women in the present study were slightly more likely to experience high job insecurity throughout midlife. Moreover, we know from prior research that women are less likely than men to experience long-term and consistent employment throughout their lives (e.g., Raymo et al. 2013; Ross and Mirowsky 1995). The unequal exposure to inconsistent employment and precarious work could add to women’s worse physical health (Case and Paxson 2005). This is especially true for functional limitations wherein women experience greater exposure and vulnerability to a history of precarious work in later midlife.
The present study provides new insight into how histories of precarious work in midlife shape longer-term health trajectories among aging adults; however, limitations must be noted. First, because the HRS samples adults over age 50, the present study cannot account for work histories earlier in the life course. As such, I cannot examine or account for early life course experiences that shape selection into precarious work by midlife. Moreover, in light of the health consequences of precarious work, people who experience precarious work from a young age have a greater chance of being too sick to participate in the study or may be deceased by midlife. Although supplemental analyses (see Appendix B in the online version of the article) account for selective attrition between ages 50 and 65, this study cannot account for selection bias prior to age 50. I include controls for poor health in childhood and whether health limits the respondent’s ability to work in their baseline interview, but findings must be interpreted with consideration of this limitation.
A second limitation concerns the measure of diagnosed chronic conditions. These conditions must be diagnosed by a doctor or medical professional, which often necessitates health insurance coverage and/or the ability to miss work to see a doctor. Future research should examine biomarker data to assess biological indicators of health that do not require a diagnosis. A final limitation related to the measures of precarious work should be noted. Nationally representative studies must continue to ask more detailed questions about characteristics of work beyond employment status and occupation. Although the HRS includes several important measures of precarious work, it lacks information about measures commonly used in studies of precarious work, such as temporary work contracts, the (in)flexibility of work schedules, and whether part-time employment is voluntary or involuntary—all of which are increasingly prevalent (Kalleberg 2018; Katz and Krueger 2016; Lambert et al. 2014). Thus, there are likely more dimensions of precarious work than the four measures in the present study that undermine long-term health.
Overall, the present study highlights how a history of precarious work in midlife—unemployment, job insecurity, and insufficient work hours—can be detrimental for physical health and longevity in later life. These findings are particularly concerning in the context of the changing nature of work over the past 50 years, wherein insecure and unstable work is increasingly common (e.g., Fullerton and Wallace 2007; Kalleberg 2018; Lambert et al. 2014). Because precarious work is unlikely to abate, reducing the consequences of precarious work for people’s health is of utmost importance. Indeed, nothing inherent to these jobs necessarily makes them precarious—the precarity is often derived from the sociopolitical context. For instance, the health implications of precarious work are often less severe in countries that have protections for workers through labor laws, regulatory protections, and labor rights (Kalleberg 2018; Kim et al. 2012). The political context has great potential to alleviate some of the health consequences of working in precarious jobs, and the present study emphasizes the need for action. With an aging and increasingly unhealthy population, precarious work is a threat for individuals, families, and countries.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465211055090 – Supplemental material for Precarious Work in Midlife: Long-Term Implications for the Health and Mortality of Women and Men
Supplemental material, sj-docx-1-hsb-10.1177_00221465211055090 for Precarious Work in Midlife: Long-Term Implications for the Health and Mortality of Women and Men by Rachel Donnelly in Journal of Health and Social Behavior
Footnotes
Acknowledgements
I thank Debra Umberson, Jennifer Glass, Mark Hayward, Sarah Burgard, and Tetyana Pudrovska for their helpful comments, guidance, and support.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported, in part, by Grant 1802628 awarded by the National Science Foundation.
Supplemental Material
Appendices A through C are available in the online version of the article.
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.