
Abstract
Despite the importance of recovery in mental health treatment, the role of love in the delivery of services is rarely explicitly stated. Similarly, the role of love in development has rarely been clearly explicated. Yet the two are closely intertwined, based on certain aspects of love that can be called the continuum of love, involving a dialectical sequence of development—autistic love (all about me), empathetic love (all about you), and integral love (all about us)—the last combining the prior two. Unfortunately, this ideal state is constantly undermined by traumatic forces in the world. This article claims that disruption brought on by trauma is best treated by what can be called the cycle of love, manifesting as the three pillars of recovery: awareness, acceptance, and integration.
Introduction
There is an old story about recovery: A man was walking along the beach and saw another man down at the shore throwing starfish out into the surf. It was low tide and the retreating water had exposed thousands of their vulnerable skins to the brutal sun. As they lay dying under the withering heat, he picked up one after the other, tossing them back into the consoling embrace of the sea. Noting the enormous multitude of starfish, the first man went down to the shore and confronted the other, demanding to know why he bothered: “What does it matter how many you save? You could never save them all!” Bending over and securing another in his grip, the other man flicked his wrist, sailing the starfish out into the surf: “Well, it mattered to that one.”
Recovery is like that. Perhaps more to the point, it is like blindly tossing starfish out the window, without ever knowing if they have even hit the water. Or like planting a seed, without knowing what kind of plant will eventually grow from the soil. In this way, recovery is characterized by certain attributes and aspirations, applicable to any approach to treatment (Ridgway, McDiarmid, Davidson, Bayes, & Ratzlaff, 2002):
An ongoing journey of self-healing and transformation
Reclaiming a meaningful life despite a mental health condition
Actively managing one’s life to minimize mental health symptoms
Enjoying the benefits and good company of a caring support system
Creating a positive lifestyle that achieves higher levels of wellness
All approaches to recovery have two things in common: fostering hope and empowerment. Although these approaches do so in different ways, they share certain features: “discover and embellish, explore and exploit client’s strengths and resources in the service of assisting them to achieve their goals” (Saleebey, 1997, p. 38). Strength-based treatment is unwavering in its focus on optimism and hope as crucial factors in recovery, emphasizing those innate capabilities and potentials for well-being temporarily obscured by the presenting problem. Simply put, recovery restores one’s innate tendency toward self-actualization, compromised by the difficult ordeal of trauma taking place during development. Having regained this crucial propensity, all that remains is the fundamental purpose of development: learn to love—better said: learn to love well.
The Continuum of Love
The prospects for recovery are significantly complicated by the fact that love can have so many different meanings, such as the way one loves his or her car or job, over against the way one loves his or her family, for example. Indeed, love can be thought of as involving different types, as said of infatuation, romance, friendship, or attachment (Ainsworth, 1982; Berscheid, 1989), or else comprising different features, such as passion, intimacy, or commitment (Sternberg & Barnes, 1989), all of which combining in any number of possible ways. Nonetheless, love can be most fundamentally said to exist in three interrelated dimensions, all of which are essential to the happiness and mental health of any human being. These three dimensions emerge in a developmental sequence that can be called the Continuum of Love (see Sleeth, 2010):
Autistic love: directed toward self and all about me—that is, being loved. This love cares for, simply enjoying what others offer. For example, “I care for certain qualities of yours and want you to take care of me.”
Empathetic love: directed toward others and all about you—that is, being loving. This love cares about, valuing or appreciating others. For example, “I care about your welfare and want you taken care of.”
Integral love: directed toward both and all about us—that is, simply being love. This love takes care of, reciprocating with others. For example, “I care about both our welfare and want us taken care of.”
A pattern can be seen operating here, involving ever greater inclusion of who really matters—first self, then others, then us—the latter combining the prior two into an integrated whole. Unfortunately, most accounts of love fail to include the final, most sophisticated member of the continuum: integral love. Indeed, empathetic love is commonly favored over autistic love, and thought not only more relational but morally superior (e.g., agape). But the two must operate together, conjointly, for each complements the other. Rather than supplant one another, they are meant to provide context for each other, as could be said of figure and ground. It is only when the two are fully integrated that one’s most profound nature can finally emerge. Until then, this arrangement holds one in a vice grips of competing forces.
What integral love offers is the binding together of the two sides, without which they simply lapse into disarray. Take a teeter-tooter. One side goes up, the other side goes down. So long as each moves in unison, it is fun to do. A sense of balance and harmony exists between them. Yet this is not an accurate depiction of human beings generally speaking. Rather, the plank of wood of the teeter-tooter stretching out into polar opposites is more likely severed. As a result, the two sides go ker-plunk onto the ground. From here, a surly battle erupts over which will be king of the hill, each forcefully advocating their side, seeking dominion over the other. Obviously, this is not a workable arrangement. Better would be the conjoining of the two into a single strip of wood, hooked together amicably by virtue of the way in which each influences the other reciprocally. This is how balance and harmony ultimately ensue.
Unfortunately, both sides have pros and cons, greatly complicating the issue. Autistic love represents the joyful, spontaneous innocence of childhood. Such unabashed delight is usually thought to be endearing. Indeed, a common way of characterizing children, especially as infants, is a little bundle of joy, although bundle of love is better said. Yet autistic love dominates one initially, such that delight is engaged in a self-serving manner, purposed toward the insatiable acquisition and consumption of desire. Getting what one wants is to be loved, and the only reason to be loving, despite any altruistic tendencies beginning to emerge. During this period, one is both ravenous and relentless, as their tissues clamor to be replenished. As Freud (1905/1953) puts it,
No one who has seen a baby sinking back satiated from the breast and falling asleep with flushed cheeks and a blissful smile can escape the reflection that this picture persists as a prototype of the expression of sexual satisfaction in later life. (p. 182)
Soon imposed on this innocent being, sadly, are the ravages of trauma, undermining their auspicious state. Consequently, the reverse is equally possible, for autistic love is anything but beatific when it comes to being selfish and self-serving. Yet, perhaps surprising for some, even those residing in the criminal underworld can be said to love their lives and the world they live in, at least to the extent their nefarious activities yield results to their liking. And not without good reason, as Nietzsche (1968) puts it, “In almost all crimes some qualities also find expression which ought not to be lacking in a man” (p. 386).
Even so, this is autonomy gone awry, overreacting and morphing into a desperate sense of superiority, not merely the province of psychopathy but also advocated in certain circles of ethics and politics. Nietzsche goes on to exhort the idea of the “will to power,” a spirited doctrine comprised essentially of two parts: because people can choose a different set of values, not bound by conventional morality, they ought to choose such a set of values. But, unfortunately, from this admirable proposition comes Nietzsche’s most notorious views—insisting a moral elite should appear and impose their standards on the rest of society:
EVERY elevation of the type “man,” has hitherto been the work of an aristocratic society and so it will always be—a society believing in a long scale of gradations of rank and differences of worth among human beings, and requiring slavery in some form or other. . . . At the commencement, the noble caste was always the barbarian caste: their superiority did not consist first of all in their physical, but in their psychical power—they were more COMPLETE men (which at every point also implies the same as “more complete beasts”). (Nietzsche, 2011, p. 111)
The idea is that certain people are superior to others and, therefore, entitled to determine not only their own fate but also that of others—the infamy inherent to such symbiotic relations is also seen in Hegel’s master/slave dialectic (see Kain, 2005), and the authoritarianism, destructiveness, and automaton conformity of Fromm (1941), as well as more homely circumstances found in family systems (e.g., Oedipal complex—perhaps better said simply incestuous complex). Needless to say, superiority of this sort has its foundation in autistic love, corrupting an otherwise noble cause, and rightly criticized for its role in discrimination and oppression when taken to extremes.
Becker (1997) graphically details the unabashed carnage to which autistic love is readily purposed, the dour lineage of which continually seen reported in various outlets of the media:
At its most elemental level the human organism, like crawling life, has a mouth, digestive tract, and anus, a skin to keep it intact, and appendages with which to acquire food. Existence is a constant struggle to feed—a struggle to incorporate whatever other organisms it can fit into its mouth and press down its gullet without choking, digestive tracts fitted with teeth at one end are tearing away at whatever flesh it can reach, and at the other end are piling up the fuming waste excrement as it moves along in search of more flesh and each organism raises its head over a field of corpses, smiles into the sun, and declares life good. (p. 1)
The admixture of self and other is a perplexing dilemma, going both ways in fact, such that either side can end up favored over the other. This is why some seem immune to learning, if not committed to sabotage or self-defeating behavior. Something about their lifestyle appeals to autistic or empathetic love. Indeed, the downside of empathetic love can be just as easily seen, for some people are subjugated to the point of even sacrificing their own self, in order to take care of others. Ravages inherent to empathetic love include codependency, enmeshment, and susceptibility to abuse or exploitation, no small matter as well.
The integration of love requires considerable commitment to overcome its inherent polarity. Unfortunately, these two tracks of human development are not well intertwined usually. So few have actually accomplished this task, it has yet to become established as a societal norm. Rollo May claims the way in which humans tend to live out their lives results in a peculiar kind of dilemma—the capacity to view ourselves as both self and other. This paradox pulls us in two directions, defining not only our greatest sorrow but also our greatest joy:
The paradox of love is that it is the highest degree of awareness of the self as a person and the highest degree of absorption in the other. Pierre Teilhard de Chardin asks, in The Phenomenon of Man, “At what moment do lovers come into the most complete possession of themselves, if not when they are lost in each other?” (May, 1969, p. 311)
Freud, too, was impressed by this paradox, where the boundary between self and other seems to melt away: “Against all the evidence of his senses, a man who is in love declares that ‘I’ and ‘you’ are one, and is prepared to behave as if it were a fact” (Freud, 1930/1961, p. 66). Yet Freud seems overly impressed by the internalized representations of this paradox (or psychic structure), thereby minimizing the verity of its nature, which literally is a fact.
May (1967/1996), on the other hand, has no interest in shying away:
My point is that both are necessary—necessary for psychological science, for effective therapy, and for meaningful living. I am also proposing that in the dialectical process between these two poles lies the development, and the deepening and widening, of human consciousness. The error on both sides . . . is the assumption that one can avoid the dilemma by taking one of its two poles. (p. 20)
This dialectical process is better said simply integral love. And the deepening and widening of human consciousness is precisely the case. As Bugental (1981) puts it, “By authenticity I mean a central genuineness and awareness of being. Authenticity is that presence of an individual in his living in which he is fully aware in the present moment, in the present situation” (p. 102).
Kirk Schneider (2008; Schneider & May, 1995) offers a compelling account of the dynamic underlying this dilemma, referred to as an expansive/constrictive continuum. Trauma does not occur in a vacuum but afflicts one’s already existing hopes, dreams, and volitional intention. This dilemma is core to the treatment he calls existential-integrative therapy, operating according to a trio of principles:
A continuum that is at one end expansive, yet subjected to constriction coming from the other end, only by degrees accessible to awareness
Dread of either end promotes dysfunction, exaggeration, or polarization, each of which equal to one’s dread
Confrontation with and integration of these poles promotes optimal living
According to Schneider, centering is the capacity to be aware of and direct the integration of these possibilities. It is only when one lives within his or her “centric mode,” or “fluid center,” that he or she has the capacity for a fully functional life. It is for this reason that existential-integrative therapy focuses on awareness and will, emphasizing their role in recovery:
What I term one’s centric mode . . . is a broadened version of Freud’s “ego.” The centric, like the ego, is the directive core of consciousness. . . . Specifically, the centric refers to one’s capacity (courage) to be aware of and direct one’s constrictive and expansive potentialities. (Schneider, 1999, pp. 31-32)
Despite the recognition that love plays an important role in treatment, exactly how love should be engaged clinically has been hotly debated. Nonetheless, the method whereby love might be delivered can be simply stated: the way in is the way out. As can be seen, love comprises a triumvirate of processes: awareness, acceptance, and integration. These aspects of love can be thought of as the Three Pillars of Recovery (see Bohart & Greenberg, 1997; Elliott, Goldman, Greenberg, & Watson, 2003; Linehan, 1993). One does not have to go about creating or generating these aspects of love, for they already exist as an intricate harmony of forces, albeit easily disrupted by trauma. Recovery is simply a matter of aligning to their already existing presence.
The Cycle of Love
Recovery as described thus far requires greater explication. After all, to whom does recovery happen? To illustrate, ask yourself: Are you a mind, or do you have a mind? Likewise, you could ask: Are you a body, or do you have a body? Are you a car, or do you have a car? Obviously, very few people confuse themselves for their car, never mind how intimately they might be related to it as they sit inside and operate the controls. Still many people have a hard time appreciating the difference between self and mind, or consciousness and cognition, conflating the two. Nonetheless, the self must be understood according to its own features. This difference allows the essential nature of self to emerge:
If you get a sense of your self right now—simply notice what it is that you call “you”—you might notice at least two parts to this “self”: one, there is some sort of observing self (an inner subject or watcher); and two, there is some sort of observed self (some objective things that you can see or know about yourself—I am a father, mother, doctor, clerk; I weigh so many pounds, have blond hair etc.). The first is experienced as an “I,” the second as a “me” (or even “mine”). I call the first the proximate self (since it is closer to “you”), and the second the distal self (since it is objective and “farther away”). (Wilber, 2000, p. 33)
As can be seen, a crucial distinction separates the two. Yet these meanings are poorly conceived placed along such a continuum. The proximate self is not simply closer to you—it is you. And the distal “self” is not simply farther from you—it is not you. Rather, the mind is your possession, and its memories merely a representation of that possession, along with your body and the life you have lived with it. In other words, the distal “self” is not rightly thought of as self. The mind and its memories are not the living person—or self—of whom they are representations, anymore than a photograph is a distal version of that person.
If this seems odd or confusing, consider the integral approach to treatment of Marsha Linehan (1993), in which she stresses a certain dialectic: “The reconciliation of opposites [is] a continual process of synthesis. The most fundamental dialectic is the necessity of accepting patients just as they are within a context of trying to teach them to change” (p. 19). Providers are constantly caught in a precarious balancing act involving accepting and valuing clients, all the while changing them in some way, precisely because something about them is problematic. Yet this conundrum is easily resolved, for the dialectic is purposed toward the two fundamentally different aspects of the whole person: self and “self”—accepting clients for who they are (their ongoing, living presence as self) over against changing what they are (internal representations of “self”).
Unfortunately, people end up confusing these aspects of psyche, mistaking the contents of their memories for who they really are. But doing so only confuses the map for the terrain. This is no trivial matter. It represents the most profound distinction for human beings possible. Memory cannot experience life. It cannot even record life all that reliably. Worse, every attribute in identity exists as part of a range of possible referents, from positive to negative—honest versus dishonest, charitable versus indulgent—for which one has some preference. There is no way to get around it, some of these qualities are not going to be positively held. Only self as conscious awareness can be unconditionally positively regarded (Rogers, 1961), for this is one’s living being. No attributes sully its presence.
Trauma recovery is further complicated by a particular difficulty with mental ailment: self collapsed on the mind. Collapsing on the mind means the self has abdicated its innate presence, thereby identifying with mind. Or as certain Buddhist traditions put it, self gets attached to mind. Actually, enmeshed is probably better said. Although not formally designated a disorder in clinical practice, this state is a principal source and symptom of dis-ease: “Fusion, or having an attachment to your thoughts . . . may be more pronounced when you experience great stress” (Coyne & Murrell, 2009, p. 102). Collapsing this way, self is mistaken for the mind, whereas consciousness gets conflated with cognition into the bargain, as well as the body the mind is intended to serve. As a result of which, one ends up picking either autistic or empathetic love over the other.
Yet the mind will not release its hold over the self until a crucial condition is unequivocally established: the self can handle the stress. To recover the capacity to love, one must accept and allow traumatic residue to be felt. Ultimately, freedom is the capacity to allow all possibilities to occur, without regard to the consequences of any of them. However, such acceptance is only accomplished in stages, or what could be called an acceptance sequence. As acceptance unfolds, each phase leads to the next in the sequence (adapted from Kübler-Ross, 1997):
Autistic love: “I want what I want.”
Denial (flight): “Oh no, not me. It can’t be true!” Denial (fight): “Oh no . . . why me? Damn you!” Bargaining (collusion): “I promise anything, if you’ll only . . . ”
Empathetic love: “I will if I have to.”
Bargaining (delusion): “I’ll believe anything, if only . . . ” Bargaining (deception): “If only I can get you to believe . . . ” Resignation: “OK I give up. [Sigh.]”
Integral love: “What will be, will be.”
Acceptance: “I release and let go . . . and move on.” Awareness: “I live fully in the moment, while aware of past and future.” Integration: “I embrace all aspects of my self.”
As a result of this process, disowned and fragmented aspects of “self” begin to enter awareness and come more into focus. In this new freedom and opening to reality, all sorts of realizations emerge as one enjoys new levels of wisdom and maturity. Memory and ongoing cognition are no longer split between essentially incompatible purposes—both processing and warding off reality. Only by enduring the ordeal of what was once considered unbearable can trauma survivors free themselves and, thereby, do something inexplicable, even abhorrent for some: accept evil. However, this does not mean to condone evil. Rather, acceptance is something perhaps even more threatening and difficult to achieve: allow evil, in the event it should happen to occur. Accepting evil merely acknowledges an already existing state of reality.
More important, accepting evil means to refrain from evil. Accepting evil is to endure evil, allowing it to pass through one uneventfully—ultimately, without being made evil by it. This is no doubt what Jesus means by turning the other cheek and loving one’s enemy. It is only in appreciating the value of that which seems odious and vile that one can be free of the trauma inherent to it, thereby recover from it. To truly accept something is to let it go. And in so doing, mind releases volition back to self, and faithfully await its next set of instructions. Overall, the clinical situation can be put this way: the mind makes a better servant than master.
Although awareness has a well-established history within existential literature, it has recently been referred to by way of an ancient spiritual tenet:
For clinical purposes, mindfulness can be considered a distinct state of consciousness distinguished from the ordinary consciousness of everyday living (Johanson & Kurtz, 1991). In general, a mindful state of consciousness is characterized by awareness turned inward toward the present felt experience. It is passive, alert, open, curious, and exploratory. It seeks to simply be aware of what is, as opposed to attempting to do or confirm anything. (Johanson, 2006, p. 2)
Mindfulness has become accepted in clinical practice, albeit by usurping a tenet of the spiritual tradition known as nondualism (see Sleeth, 2009). A crucial clinical dictum of recovery follows from this doctrine: the greater the awareness, the greater the love. Yet why a connection should exist between these two has never been made explicit in psychology. But one way of answering is simple enough: If all experiences are found acceptable and allowed to freely enter awareness, love is free to enter awareness too. Otherwise, love is filtered out right along with everything else. The secret to treatment comes down to this: If one can keep awareness firmly focused on love—especially integral love—unpleasant experiences eventually wither away, finally lost to obsolescence. It is in this way that one is able to organize his or her existence in a meaningful manner, which is to say, according to love, the ultimate measure of all meaning.
Along these lines, Linehan (1993) makes the core of her treatment the curative properties of nonjudgmental awareness and radical acceptance: “The goal is to develop a lifestyle of participating with awareness . . . in the moment, whatever is happening. . . . Radical acceptance does not choose what to accept and what not to accept” (pp. 144-145, 517). In this way, acceptance becomes a kind of radical truth, seeing life as it really is, without the distorting haze superimposed by what one might prefer reality to be. To help explain the nature of radical acceptance, Linehan draws on a distinction involving willingness and willfulness, where one stands off from life according to the former, but immerses within the deepest processes of life with the latter, allowing self to be attracted toward and guided by those aspects of life aligned to their own most meaningful values.
Past decisions by the self (no doubt appropriate enough in their time, often while one was still young, although typically useless now) are often blindly recycled by the mind. When self is overwhelmed by circumstances (or trauma), one abdicates responsibility and the obligation for conscious choice—to the mind. This is what it means for the self to be collapsed on the mind. Take, for example, young children being told on a daily basis they are no good or will never amount to anything. If they love the ones telling them this, and extrapolate out the implications, the results could be disastrous. Reaching a point where they just cannot take it anymore, succumbing to despair, they may finally give up on disputing the fact. In the wake of this collapse, yielding volition, the mind’s endless repetition will inevitably take their place, reducing them to essentially a bystander, merely along for the ride. Who knows what callous deeds might come from such a coup after a while.
Frankly, if the self cannot rise to the occasion and make a decision, the mind will. In this way the mind takes over the psyche, stepping in when the self is overwhelmed. Still the purpose is to protect the self, not that the process cannot go awry. After all, the mind is merely a machine and simply does not know any better. In the end, a layer of abstraction finally gets inserted into one’s inherently phenomenological state, whereby expectations piggy-back on evaluations, the combined amalgam of which ultimately displayed to awareness, indicating their best understanding. One’s acceptance—as modified by expectation—provides the impetus driving their response, downloading into expressions of behavior.
This overall arrangement can be diagrammed as in Figure 1.
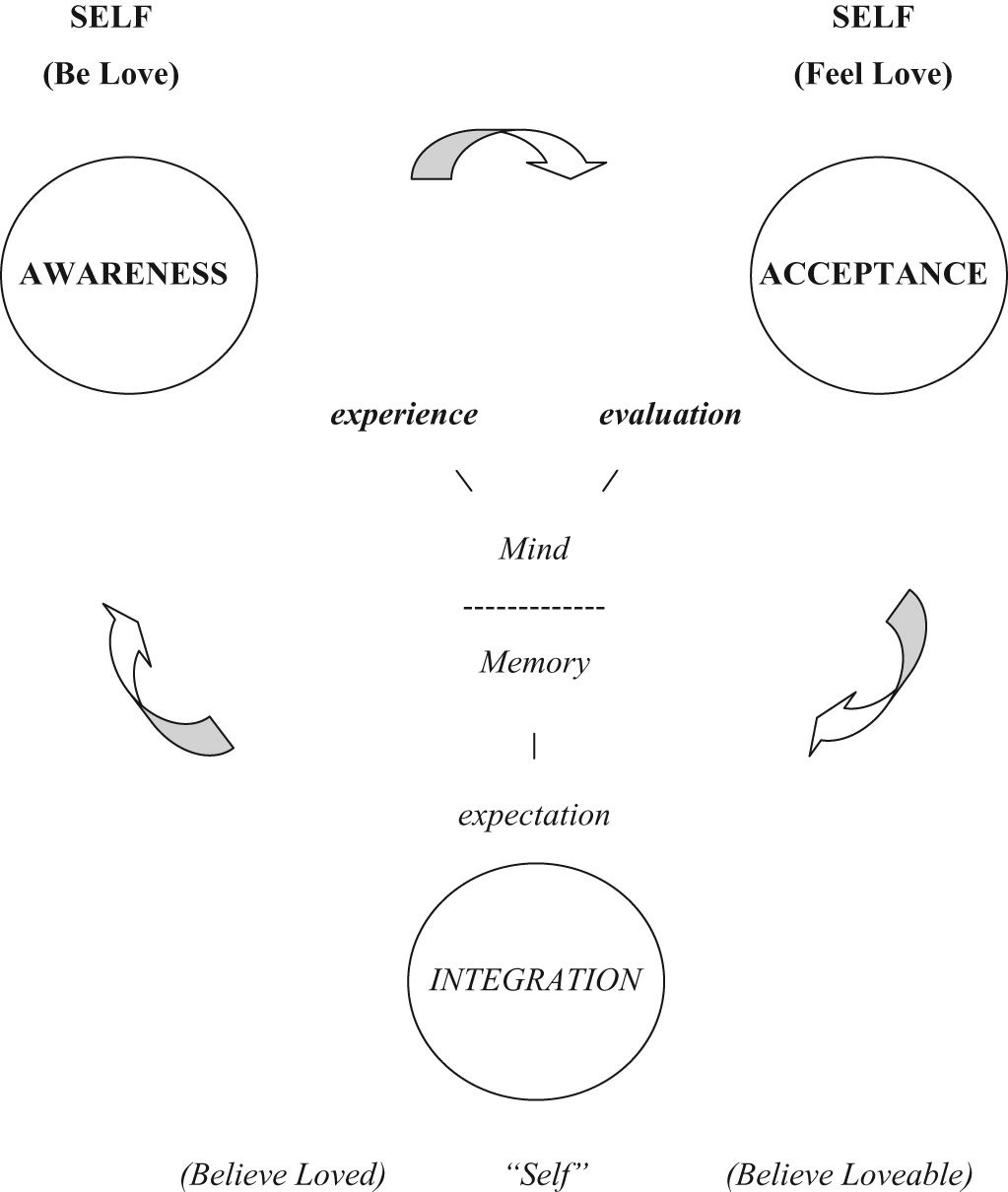
The cycle of love (three pillars of recovery)
The cycle of love is a reciprocal and interactive process, requiring full participation in respect to all its aspects. To illustrate, “self” influences the way one loves as follows: depending on the way one is treated, he or she will draw conclusions about his or her own value, as said of conditions of worth (Rogers, 1961) and mirroring (Bacal & Newman, 1990). The memory of these conclusions now dictate how loveable one believes himself or herself to be, determined as a consequence of how loved he or she believes he or she has been. Simply put, if one believes he or she is loved, he or she will feel loveable. Conversely, if one believes he or she is not loved, he or she will likely draw the opposite conclusion: he or she is not loveable. Once these representations becomes an immutable part of “self,” one might even tweak or distort ongoing reality to conform to their conclusions, perhaps even despite times in which present circumstances are actually being loving.
From here, certain outcomes are inevitable: If you believe you are loveable, you will behave in a loving manner; conversely, if you believe you are not loveable, you will not behave in a loving manner. Indeed, you may behave in a decidedly unfriendly manner, perhaps even pay others back for not loving you. You might even give up any hope of being loved and opt for self-serving coping strategies, such as indulgence, exploitation, or indifference to others, never mind how self-defeating this might be for any prospects of being loved. Clearly, there is a catch-22 to this arrangement: To be loved, one must be loving; but to be loving, one believe he or she is loveable; and to believe one is loveable, he or she must first believe he or she is loved; and to believe one is loved, he or she must first be loved—whereby he or she feel love—which is ensured only if one is loving, starting the whole cycle all over again.
The Three Pillars of Recovery
Awareness and acceptance are crucial features of recovery, working in tandem. To recover from trauma, awareness must be shored up with an abiding courage and capacity for acceptance (Tillich, 1952). But, obviously, this is no easy matter. Indeed, abreaction per se could mean being stuck in the painful emotional state prompting one’s mental ailment in the first place, resulting in an unwelcome state of secondary trauma, to be avoided if at all possible (i.e., resistance). Nonetheless, a direct correlation exists between one’s underlying emotional state and cognitive insight. As a result, unacceptable memories can be integrated into the overall memory system, altering the onerous fact of the trauma into something palatable.
Interestingly, just as Linehan focuses her treatment approach on awareness and acceptance, Schneider focuses on two aspects of the recovery triumvirate as well: awareness and integration. Although he calls his treatment approach existential-integrative, the existential part refers to experience—as it enters awareness. Consequently, it could be said that both these pioneering integral therapists give priority to awareness, while splitting the remaining two aspects of the recovery triumvirate between them. Indeed, existentialism has a long history of extolling the virtues of awareness, as well as advocating its role in recovery:
The aim of Gestalt therapy is the awareness continuum, the freely ongoing Gestalt formation where what is of greatest concern and interest to the organism, the relationship, the group or society becomes Gestalt, comes into the foreground where it can be fully experienced and coped with (acknowledged, worked through, sorted out, changed, disposed of, etc.) so that then it can melt into the background (be forgotten or assimilate and integrated) and leave the foreground free for the next relevant Gestalt. (Perls, 1973, p. 2)
As can be seen, memory is the source of the endless procession of gestalten (bits of unresolved “self”) entering awareness. Self, on the other hand, is precisely that presence of awareness to which the various gestalten appear and are experienced, as a result of which finally worked through and assimilated or integrated back into memory by the mind.
Unfortunately, although accounts such as these point out the downside of the paradoxical potential of the psyche, they are somewhat remiss in stating how the process of assimilation and integration might actually occur in clinical practice. However, Schneider (1999) describes such interventions this way: “(1) survey the associational network of clients’ extremism—the patterns and situations in which clients perceive in a ‘hyper’ [or skewed] manner; and (2) engage the constrictive or expansive alternatives available to rearrange (or integrate) that network” (p. 188; see also Schneider, 2008, for an update on this approach to treatment). However, by this, Schneider does not intend the resolution to be a static state, somehow carved into stone at the median point between the two extremes. Rather, integration of the two results in a fluid state, where the two extremes exist in a relatively balanced, even discriminating manner relative to one another:
[S]uch folks are comparatively able to direct and be aware of their excesses rather than being compelled by them, and this moves them to a vivacious position I call the “fluid center.” Hence, the ideal in my view is not straight centrism between extremes, but a dynamic . . . [that] can expand out with spontaneity and openness but also reign in as warranted with discipline and focus. (Schneider, personal communication, May 18, 2011)
Like the Madhyamika, or Middle Way, of Buddhism, integral love embraces both ends of the polarity, thereby allowing full and free access to all points along the continuum. Consequently, this arrangement develops a set versus subset quality: integration results in high functioning for most people, yet without the converse necessarily being true. Indeed, unfortunately, it is common enough for high functioning people to be narrowly constricted or wildly expansive, not at all well integrated. Such people rely on excess, precisely for the sake of success. Our own recent string of presidents might well provide some striking examples, or else CEOs of certain savings and loan companies, if not celebrities in general.
Needless to say, the liabilities of being skewed are legion, such that the dynamic of the fluid center ends up corrupted, compromising one’s ability to move freely in either direction. These liabilities result in the various diagnostic categories of clinical practice and even appear in certain literary “case studies,” such as Nietzsche’s übermensch or any number of exaggerated heroic figures, as could be said of Zorba the Greek, for example (accounting for cultural norms). Perhaps the most noteworthy literary example for our present purpose is the renowned split personality of Robert Louis Stevenson’s infamous novel—Dr. Jekyll and Mr. Hyde. Clearly, this represents an early intuition of the troubles potentially besetting one skewed toward either empathetic or autistic love; the former sapping the passion from one’s otherwise accomplished presence, the latter erupting in passion, overriding any sense of reason or conscience. Freud likewise gives voice to this conflict within the psyche, lamenting the tussle between the ego and the id (as well as superego).
[T]he development of the individual seems . . . to be a product of the interaction between two [fundamental] urges, the urge towards happiness, which we usually call “egoistic,” and the urge towards union with others in the community, which we call “altruistic.” (Freud, 1930/1961, p. 140)
According to Freud, whereas the narcissistic person is involved primarily with an egoistic urge toward their own happiness, or gratification, the erotic person gives priority to a more altruistic urge for union with others. As can be seen, Freud recognizes the distinction between autistic and empathetic love (even if within the limiting context of his sexual theory). However, he does so without seeing their mutually interactive nature, resulting in integral love, which most auspiciously defines the relationship between them. Indeed, the contrast is thought to be decisive and held in a most unfavorable light: “[T]he two processes of individual and of cultural development must stand in hostile opposition to each other and mutually dispute the ground” (Freud, 1930/1961, p. 141). Nonetheless, a far more fortuitous outcome is available than this. Indeed, it is possible to integrate these aspects of “self,” never mind the imposing nature of the clinical task.
In sum, when others pay attention to and appreciate you, as said of accurate empathy and unconditional positive regard (Rogers, 1961), you will tend to respond in kind, with nonjudgmental awareness and radical acceptance (Linehan, 1993)—the Cycle of Love. It has sometimes naively been said that all you need is love, as if one could feed his or her belly with happy thoughts. Of course, this is far removed from what John Lennon meant with his iconic song. Yet even Maslow claims you must work your way up a need hierarchy, first satisfying corporeal needs such as food and shelter, only later reaching the more lofty realms of belonging and love. Unfortunately, this is a skewed way of understanding love. To put it simply, people love food and shelter. You do not have to wait around for rungs on the ladder to appear before you start loving. People love life from the very beginning, not only its splendor generally, but also for the brute sake of continuing one more gasp of precious air, should the supply start to run out. Is there any doubt about this? Autistic love is love, never mind how often overlooked as such. But to dismiss autistic love does a disservice to the realities within which we live. Autistic love is where the passion lies, instilling life with vivacity.
Consider this: Every aspect of life is rightly thought of as an instance of love. That is to say, all you need is integral love. It is not the same as saying love merely. It is only by reducing love to its empathetic state (or else autistic state) that any confusion occurs. Both sides are required. Indeed, self-actualization is the integration of love. Without the altruism of empathetic love no integrity exists by which to support the intimacy inherent to one’s passion and vivacity. Others must play as pivotal a role in love as the self, resulting thereby in the sense of us—all of us, ultimately. The encounter of this juxtaposition of intimacy and integrity provides the interplay necessary for integration to take place, especially integral love, ultimately leading to successful adaptation and recovery, without which one remains under the sway of every kind of mental health ailment, skewed toward autistic or empathetic love, if not an enmeshment of the two. All three aspects of the recovery triumvirate are intimately related, interacting in a fluid and endlessly reciprocal Cycle of Love—perhaps best referred to altogether as mindfulness and the Middle Way, given the popularity of recent trends in clinical practice.
Conclusion
Human beings live out their lives in a perplexing dilemma, resulting from a particular kind of tension: the capacity to be both self and other, ultimately defining not only our greatest sorrow but also our greatest joy. The problem, of course, is letting one side or the other get lost in the shuffle, losing track of self either way. The error that people make is in assuming the dilemma can be avoided simply by picking one side over the other.
One of the most misunderstood features of human existence is a subtle irony played out between the two spheres of love: what one regards as evil, others take to be good, both held at arm’s length, tussling in an apparently intractable struggle of righteousness for final dominion. In a famous dialogue with Carl Rogers, Rollo May (1992) urges a particular understanding of evil:
I am pleading for a realistic approach to human evil. . . . “Man is basically good—and evil.” . . . I am arguing that we must include a view of the evil in our world and in ourselves no matter how much that evil offends our narcissism. (p. 312)
May develops this idea, drawing on earlier work:
We are the “nice” people and, like the cultivated citizens of Athens in Socrates’ time, we don’t like to be publicly reminded, whether we secretly admit it to ourselves or not, that we are motivated even in our love by lust for power, anger, and revenge [or autistic love]. While the daimonic cannot be said to be evil in itself, it confronts us with the troublesome dilemma of whether it is to be used with awareness, a sense of responsibility and the significance of life, or blindly and rashly. When the daimonic is repressed, it tends to erupt in some form. (May, 1969, p. 129)
Yet what does it mean to use autistic love (or the daimonic) blindly or rashly? And what does it mean to say that autistic love is not evil in itself but must be used with awareness, a sense of responsibility, and the significance of life? The answer to the latter is simple enough: integrated with empathetic love. Likewise, the answer to the former can be put just as succinctly: without empathetic love—such that integral love does not result. Indeed, languishing forlornly in isolation, even empathetic love can erupt in some way, as might be said of enmeshment, codependency, or even willing gullibility and susceptibility to exploitation.
Yet the two are never truly severed, and one must find their proper unity. Consequently, merely juxtaposing the two is no answer. Love is a single reality, in which one or the other aspect may emerge more clearly within this respective context at different times. Integral love is the precise term for this conjoining. Indeed, integral love is the missing link in the evolution of love, the lynchpin potentially holding the two sides of humanity’s affection for each other together. The Continuum of Love is the developmental transformation whereby excesses of autistic love are purified and new dimensions of empathy and altruism revealed. It is essential that integral love be explicitly stated and advocated, or there is no way of knowing what must happen next in the proper course of development, not to say treatment. Recovery only takes place within this context. If the two sides of love are not “hooked” together through integration, they will not hold up, but degenerate back into their respective sides under duress.
Put bluntly, evil is in the skew. Preferring one end of the polarity over the other is the skew. Any antinomy of good and evil is ultimately misguided, for their polarity always goes both ways. Consequently, their respective moral certainty is a chimera, only maintained at the expense of the other. Evil is the very state of good versus evil. It is only in clearly articulating the nature of their transcendent state that integral love and the good have a chance to appear. Or as Schneider and Krug (2010) put it,
The great question . . . is how to help clients become emancipated from their polarized conditions . . . to integrate freedom and limits. . . . [T]he path to greater freedom is paradoxically found through an encounter with the ways in which we are bound. (p. 15)
And, in so doing, liberate one from their debilitating skew, providing thereby whatever piece is missing. Integration is liberation. And liberation is integral love. It is just that an unflinching awareness of self must happen to create the opportunity for that to occur, while acceptance provides the rationale, ultimately preserving as a result some stability in one’s “self” structure. Such are the Three Pillars of Recovery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.