
Abstract
The Department of Veterans Affairs (VA) has recently increased support for inclusion of Veterans and family caregivers as collaborators on the research that affects them. In this article, the authors—two VA investigators, two Veterans, and two caregivers—draw from nearly a decade of participatory action research to highlight the methods we have employed to build and sustain collaboration. These methods include the following: using ethnographic approaches to engender trust, treating informed consent as an ongoing process, and sustaining engagement through shared dissemination of findings. We also consider impacts of engaged research that lie outside the parameters of what traditionally “count” as outcomes and that have helped us maintain our collaborative relationships even during periods between funding. We provide examples of how community engagement has bridged Veteran communities and VA, and how the use of visual and narrative methods of dissemination has led to social connectedness and repurposing of Veterans’ and caregivers’ mission as advocates. Our goal is to inform those who wish to conduct this type of research, to further pull research efforts in this direction, and to demonstrate the value of collaborative research from the point of view of those who have been engaged in it.
Keywords
Introduction: A Scenic Overlook
A busy area in the lobby of the Department of Veterans Affairs (VA) Medical Center in New Orleans is traveled by hundreds of patients, family members, and staff daily. Along one hallway is a permanent installation of photographs and stories from U.S. Veterans of the wars in Iraq and Afghanistan (Operations Iraqi Freedom and Enduring Freedom [OIF/OEF]), titled From War to Home: Through the Veteran’s Lens (Figures 1 and 2). Nearby, a second installation called From War to Home: The Impact of Invisible Injuries, highlights photographs and stories from OEF/OIF Veterans with traumatic brain injury and their family caregivers (Figures 3 and 4).

First exhibition installation.

First exhibit close-up.

Second exhibit installation.

Second exhibit close-up.
Although these exhibits are the products of two VA-funded research studies, they diverge from most health services research in several notable ways: in their use of visual, arts-based methods to disseminate study findings; in their public sharing of personally identifiable information (names and faces) and protected health information (e.g., suicidal thoughts, episodes of homelessness, psychiatric hospitalizations); and in their privileging of personal and collective reflections on the impacts and experiences of military service and war (e.g., camaraderie and sense of purpose, moral injury and survivor guilt, family disruptions and loss) over academic theories and texts.
The first exhibit, Through the Veteran’s Lens, has traveled in one form or another continuously since 2012, with installations in dozens of hospitals, universities, art galleries, and other public venues across the United States. Along with a website (www.va.gov/FromWarToHome; Figure 5) and a self-published photobook (Figure 6), the exhibit is a physical manifestation of 7 years (and counting) of a participatory action research (PAR) collaboration between a VA investigator who coauthored this article (Gala True) and a group of 40 Veterans from Southeastern Pennsylvania (including coauthors Ray Facundo and Lawrence Davidson). Over time, this partnership has led to a larger, multisite research award involving another VA investigator (coauthor Sarah S. Ono) and a new group of 45 Veteran collaborators (OIF/OEF Veterans with a traumatic brain injury) and 26 of their caregivers (including coauthors Sharon Urbina and David V. Meyer) from Southeastern Louisiana and Northwestern Oregon. It is this study that led to development of the second exhibit, The Impact of Invisible Injuries.
FWTH website.
FWTH book.
Writing this article together has allowed the authors to reflect on what we have learned from a long-term collaboration that crosses the boundaries of academic, clinical, and public scholarship and to consider the implications for community-engaged research (CEnR) more broadly, as well as the impacts of research using visual and narrative-based approaches. Our goal is for the knowledge we have gained and created—both in a near-decade of experience and through the process of reflection for this article—to be informative to those who wish to conduct this type of research, to further pull research efforts focused on service members, Veterans, and caregivers in this direction, and to demonstrate the value of collaborative research to those who might question the positive ratio in a cost-benefit analysis of CEnR approaches.
Context: Our Lane Along the Community Engagement Highway
CEnR—defined as a continuum of approaches focused on including community stakeholders as collaborators on research that affects them—has developed a robust history in health services and public health research over the past several decades. Rooted in consumer-led activism, such as the disability rights movement “Nothing About Us Without Us,” CEnR is grounded in the recognition that community members “ . . . know their own situation, are motivated to solve their own problems, and see things from a fresh perspective” (World Health Organization, 1978, p. 50). Compared with a more traditional research approach, in which individuals and communities are subjects, the focus in CEnR is on establishing and sustaining research partnerships between researchers, community members, and organizations (Israel, 2005). CEnR approaches go by a variety of names—including PAR, community-based participatory research, and stakeholder- or patient-engaged research—that follow a common set of principles designed to support community members as equal partners in all stages of research (Concannon et al., 2012; Shippee et al., 2015). When done properly, CEnR builds the foundation for robust and meaningful academic–community partnerships by developing individual and community capacity to engage in or colead research while expanding researchers’ understanding of how problems and solutions exist in the context of individual lives and communities (Cargo & Mercer, 2008; True, Alexander, & Fisher, 2017).
Uptake of CEnR approaches within VA-funded research has been somewhat slower compared with other federal agencies such as the Patient-Centered Outcomes Research Institute (Sheridan, Schrandt, Forsythe, Hilliard, & Paez, 2017). Over the past 10 years, however, several academic–community research teams around the country, including our own, have collaborated on research focused on diverse health topics such as increasing access to postdeployment mental health services (Franco, Hooyer, et al., 2016; Franco, Logan, et al., 2016; Kirchner, Farmer, Shue, Blevins, & Sullivan, 2011; Rizia et al., 2014; True, Rigg, & Butler, 2015); using narrative methods to explore impacts of trauma (Hooyer, 2017; Hooyer & Kasza, 2018); and improving engagement in care for women Veterans (Hamilton et al., 2017). More recently, HSR&D—the branch of VA research focusing on translating research findings into clinical practice and health care policy—has increased its investment in engagement activities involving Veterans and their family members (whom we refer to as caregivers) as consultants or partners in the research process. This includes formation of a national VA working group in health services research to provide guidance for such efforts and funding development of a toolkit, titled “Strengthening Excellence in Research through Veteran Engagement” (SERVE; https://www.hsrd.research.va.gov/for_researchers/serve/; Arnett et al., 2015; Hyde et al., 2018).
As with CEnR more generally, one impetus for engaging Veterans and caregivers in research is a desire to enhance the quality and integrity of health research and to support the uptake of evidence-based practices from research to real-world settings (Brett et al., 2014a, 2014b; Dillon, Tuzzio, Madrid, Olden, & Greenlee, 2017; Esmail, Moore, & Rein, 2015). In the case of VA-funded research, an additional driver is the relatively high visibility and power of Veterans’ groups or Service Organizations (VSOs) to lobby for health research on deployment-related conditions. Few, if any, other patient populations have representation at the Cabinet level or Congressional committees focused on oversight of the health care organization that serves them. Furthermore, the past few years have seen significant erosion of trust between Veterans and the VA, including the 2014 “access scandal” and a recent report of improper denial of benefits to survivors of military sexual assault (Hayward, 2017; Wentling, 2018). Meaningful engagement of Veterans and their family members in research is one pathway toward rebuilding that trust (Frerichs et al., 2017; Getrich et al., 2013). Many Veterans rely on the VA as a sole source of health care and, thus, have an investment in high-quality research informing the services and programs they receive. Additionally, service members recognize the importance of timely research into deployment-related health conditions—for example, sequelae of burn pit exposures—and VSOs play a key role in lobbying for research in these areas (Sisk, 2018). Thus, the VA has ample motivation to make a case for the value of research directly to Veterans, and Veterans and families have a stake in ensuring VA-sponsored research is relevant to their needs and realities.
It is against this backdrop that we have built our Veteran- and caregiver-engaged research collaboration. This effort began to take shape in 2011 (Figure 7) when the HSR&D pilot that became Through the Veteran’s Lens was funded. Prior to that, Gala had started making connections in the community that would prove essential to the success of the pilot study. Figure 7 provides key milestones for our collaboration and shows how the group has grown steadily over time.
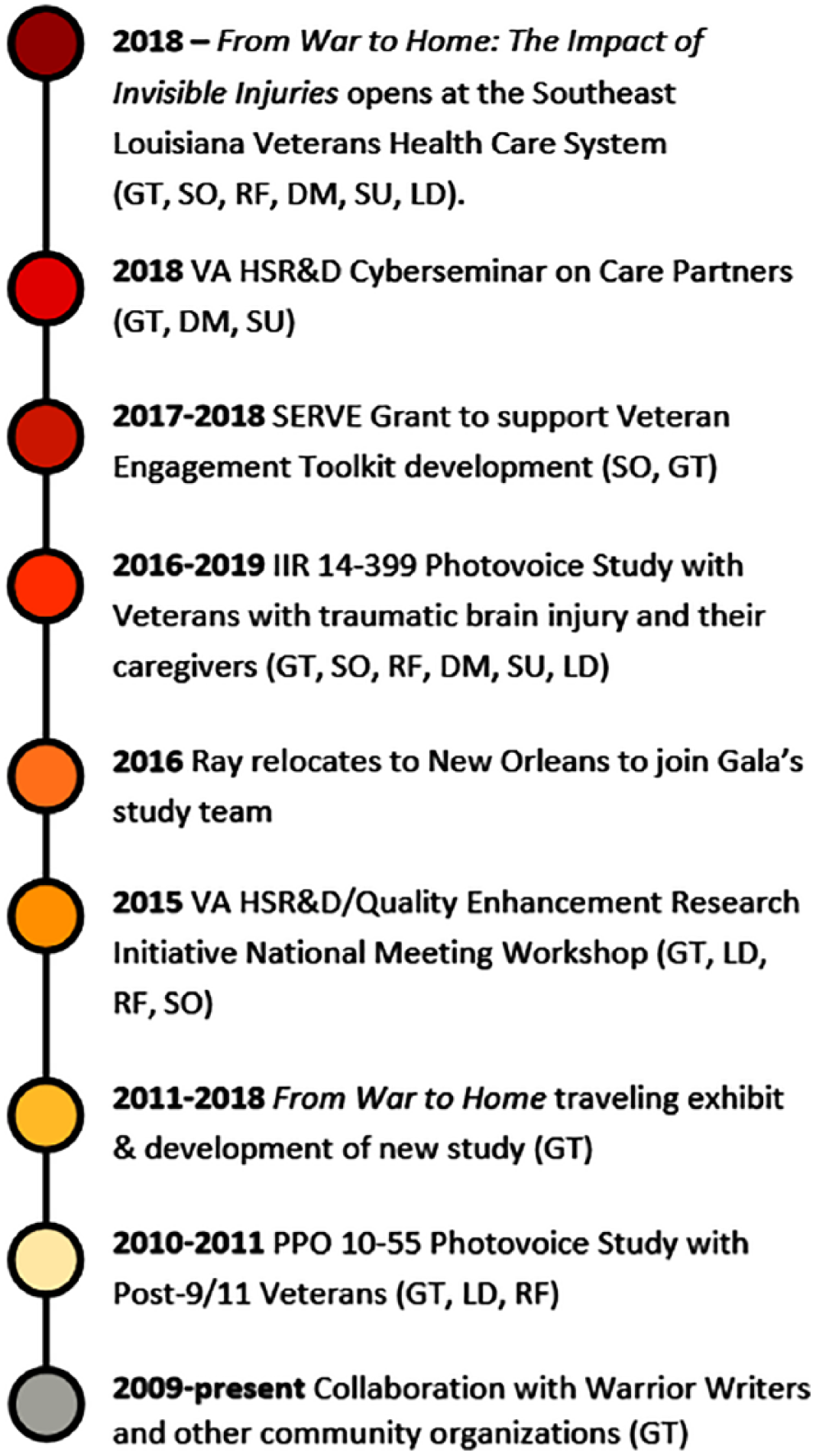
Collaboration timeline.
Among the pages of researchers’ fieldnotes, the reflections shared between researchers and Veteran and caregiver participants after the recorders are turned off, and the conversations between official study visits and during times in-between funded research, we have collectively and individually reflected on our different and shared perspectives through the lens of our respective roles. The author group had two 90-minute phone calls over 4 weeks while writing this piece. Between calls, we offered written reflections in e-mails and circulated text for comments and review of each new iteration. Below, we describe methods we have employed to build and sustain our collaboration and reflect on challenges we have encountered and ways we have attempted to negotiate these challenges to sustain and grow our research partnerships and personal relationships. We also consider impacts of our work that are not traditionally “counted” as measurable outcomes in research, but which nonetheless have been vital to each of us and to other Veterans, caregivers, and researchers with whom we collaborate. Throughout, we use direct quotes from our conversations to illustrate our points and represent multiple perspectives and personal voices.
Building the Road We’re Driving On: Our Approach to Collaborative Research
CEnR has been conceptualized as a range of approaches, including an advisory model, in which patients and community members provide input on various stages of the research as invited by the researchers; an employment model, in which patients and community members with personal experience in the topic being studied are employed on the research team; and a partner model, in which persons affected by a health condition help shape all aspects of the research from conceptualization to dissemination (Cashman et al., 2008; Israel, 2005; Roche, Guta, & Flicker, 2010; True et al., 2017). Over the years, our research collaboration has evolved to incorporate all three models, such that our current VA study includes Gala and Sarah as VA investigators, Lawrence on the Advisory Committee, Ray as the VA research manager, and Sharon and David among the participant–collaborators.
A core method of our partnership is “photovoice,” a PAR methodology in which people are given cameras and asked to document their daily realities around a specific challenge, with the goals of illustrating and reflecting on personal and community strengths and weaknesses, engaging in dialogue about personal or community concerns and goals for advocacy, and communicating findings with policy makers (Wang & Burris, 1997). The history and methods of photovoice have been well-documented (Lorenz & Kolb, 2009; Padgett, Smith, Derejko, Henwood, & Tiderington, 2013; Wang, 1999; Wang & Burris, 1997), and we have published a full description of our methods elsewhere (True et al., 2015). Below, we outline the three elements of our approach that we see as cornerstones to developing and sustaining our collaboration.
Creating and Sustaining Trust Through Ethnographic Approaches
As a folklorist and a feminist anthropologist, respectively, Gala and Sarah have drawn on principles of ethnographic fieldwork to inform all aspects of this research, including recruitment and data collection methods (Wolcott, 2005). Spending time outside the institutional walls of clinical and research settings by attending Veteran- and caregiver-focused events in the community and visiting with local Veteran student groups, for example, has allowed us as researchers to build relationships with VSOs and community-based organizations, including arts-focused nonprofits such as Warrior Writers (Calica & Basl, 2014) and to engage Veterans and caregivers who might not otherwise participate in research. Many times, we have found that a CBO or VSO can serve as a “proxy” to help build trust between researchers and Veterans. As Gala recalls about the importance of these relationships to recruitment for the first photovoice project: I had many Veterans tell me later that if I hadn’t approached them through Warrior Writers—if Lovella, the director of Warrior Writers hadn’t vouched for me—they never would have talked to me. These were Veterans who hadn’t participated in research before, and who usually avoided the VA completely. But they told me, “Lovella said you were okay, that you care, so I was willing to talk to you.”
At many VSOs and CBOs, Veterans are employees or volunteers who act as informal gatekeepers by vetting researchers before passing on recruitment materials to other Veterans. This is partly why Lawrence decided to participate in the first photovoice project after meeting with Gala and why he decided to tell Ray about the project. As Ray recalls: I remember being really wary about being involved in research . . . Lawrence picked up this flyer off the desk, and he’s like, “Hey, I think I’m going to do this. I talked to this lady. She seems legit. You know, it seems like she gives a shit, and I’m going to do it.”
In our collective experience, a challenge to CEnR is the lack of trust in the VA among some Veterans and caregivers due to past negative experiences with having their health concerns recognized or with accessing needed medical care (Littman, True, Ashmore, Wellens, & Smith, 2018). Thinking back on his first impressions of Gala, Lawrence articulated how his growing trust in Gala mediated his reflexive hesitancy to trust federal institutions (i.e., Department of Defense and VA), and the positive impact this kind of trust could have on his willingness to answer questions honestly and, thus, improve the overall integrity of the research being conducted: . . . for me, it was this unmistakable gut sense . . . I feel your support. That you’re listening. To me, that is foundational to trust . . . and now you’re asking research questions, and I’m actually giving you an honest answer. “How many times a week do you drink? Once, twice, four times?” Do you really answer honestly when you don’t know the person asking the questions? The bottom line is that you’re paid by the VA, and there is significant institutional distrust. Some of it has nothing to do with the VA and it just comes from past military experiences [with] the Department of Defense and now the VA. . . . Some of it is very much based in reality, where I don’t trust the system for whatever reason.
As our approach to community engagement has expanded to include family members of Veterans, we have faced the challenge of gaining trust from these caregivers, who feel a responsibility to safeguard the emotional and mental health of their Veteran loved ones. We have learned the advantages of working in pairs; for example, when Ray and Gala travel to a community organization together to talk about recruitment or meet with potential participants for the first time. As the photo-ethnographers Philippe Bourgois and Jeffrey Schonberg (2009) have observed, this practice of working in pairs is safer and more fun, and enables each member of our research team to develop a range of relationships with our participant–collaborators and gain broader access to their lives, insights, and experiences.
As caregivers, Sharon and David had initial concerns around participating in the photovoice study with their Veteran partners. They describe how trust was built between themselves and members of the research team and how this trust led to positive outcomes in their study participation. As David commented, One of the challenges that I had to overcome [around trust] was allowing you to talk to my husband. I wasn’t sure about, ‘Who the hell are these people in my house, asking me these things?’ And because I am the principal caregiver, I’m very protective of him and didn’t know what the impact would be of his exposure to it. And it’s been nothing but extraordinary.
Sharon noted that I had the same fears: “What are they going to bring up, in terms of memories and language, that may trigger my husband?” They [the researchers] are going to leave to go back to work, but I’m going to be here and have to either calm him down or deal with him being irritated or agitated or frustrated or sad . . . from a caregiver perspective, I was fearful of the residual afterward of “what’s going to happen?”
There is extensive literature on the role of community researchers in health services and public health research as important “cultural brokers” who make essential contributions to the content and quality of data collected and whose “insider status” may be key to gaining access and building trust with individuals and communities who face stigma or other barriers to participating in research or accessing health care (True et al., 2017, p. 68). Sharon noted the impact of having Ray as a member of the research team on her trust and comfort with having her husband, Carlos, participate in the research: When Ray walked in [for the first study meeting], and here is another combat Veteran sitting across the table from my husband, I think that was just so sweet. And the whole experience was gentle, and that’s not always our experience with the VA. Carlos felt comfortable because Ray introduced [himself], “I’m not just the program manager; I’m also a Veteran,” and it almost immediately put Carlos at ease. And Ray had participated in [the first photovoice study]. [Carlos] was like, “Oh, if that dude can do it.” It just started the building of the trust and the relationship.
Sharon’s observations also touch on the role of stigma as a barrier to Carlos’ participation in research focused on mental health and how Ray’s presence on the team (and as a participant in the first photovoice study) helped destigmatize research participation for Carlos. Our experiences demonstrate how including a Veteran on the research team (when possible) and building connections with trusted community partners have enabled us to identify, engage, and follow up with Veterans and caregivers who might not otherwise participate in research.
Approaching Informed Consent as a Process
We approach informed consent as an ongoing process and dialogue, rather than a one-time event at an enrollment visit. We recognize the limitations of the traditional institutional review board (IRB) protocol, with its focus on safeguarding confidentiality and limiting institutional liability, in the context of research involving participants actively interested in telling and owning their stories (Bourgois & Schoenberg, 2009; Leisey, 2008; Wilson, Kenny, & Dickson-Swift, 2018). At the same time, we are mindful of how the very nature of participatory research using visual methods and public-facing dissemination (particularly in the digital age) requires careful consideration of potential consequences to participants of forgoing anonymity and having stories travel to unanticipated places (Clark, Prosser, & Wiles, 2010; Gubrium, 2013). We have developed a process whereby written informed consent is only the starting point. As each individual Veteran or caregiver contributes their photographs and narratives to the project, they decide whether, and how, they want to be identified in dissemination overall. In addition, study participants may withhold consent for a particular photograph and control the context in which it may be used or specify that it may be used only if attributed to “anonymous.”
As a form of member checking—the process of circling back to data sources to check interpretation (Birt, Scott, Cavers, Campbell, & Walter, 2016)—and coconstruction of knowledge, each participant reviews their entire photo-narrative (a “book” of their photographs and accompanying story for each photograph compiled by members of the research team), with the opportunity to add, omit, or revise. We strive to have participants maintain control and ownership of their data throughout, with full understanding that our ultimate goal is public dissemination to advocate for change at local and national levels. In this regard, our approach parallels what Caroline Brettell (1993) has described as “ethnographic co-authorship,” when researcher and participant make decisions about what will and will not be included with explicit awareness that the text will be a public document. We have, of course, faced challenges around the limitations of our ability to anticipate and control for every contingency related to consent and dissemination. Through this collaboration, we have been acutely aware of how the passing of time and changes in circumstances can affect choices that were good at the time they were made but may later need reconsideration. Over the years, Gala has encountered situations where she has needed to react to changing circumstances. For example, the first study included a Veteran who had contributed photographs of his son to illustrate the importance of his family. Later, he was going through a divorce and custody dispute and asked her to pull the photographs of his son from the project, which she did. In another example, a Veteran had shared photographs and stories from when he experienced homelessness and alcohol addiction. As the study progressed and he participated in dissemination of findings as a copresenter at conferences, he asked that Gala not include photos and quotes that depicted his struggles with addiction in his presentation slides because they did not align with his evolving self-identity and he did not want his past struggles to be the only focus of his presentation.
Gala and Ray faced a challenge related to a photograph that Ray himself had contributed to the first exhibit. It was of Ray and his brother in Iraq and was paired with Ray’s recounting of an experience his brother had during deployment; his brother initially gave permission to have the photo and story included in the exhibit but later contacted Ray and asked to have it removed. As Ray remembers, That was a challenge that we really had to quickly negotiate. It made me very uncomfortable, and we had to take care of it swiftly. When looking back on this, it was a lesson learned. I should have checked back in with him about this even though we had permission . . . [but] he didn’t want it there anymore. And it was our job to take it down.
In a similar vein, Lawrence reflected on his years of experience with seeing the first exhibit installed in various locations and taking part in dissemination activities, and noted the importance of transparent, ongoing communication between researchers and participants: I did not understand the extrapolation of what this could be; I’m not so sure that Gala did. Six years after the initial exhibit opening, I flew to the Columbus VA to speak at their suicide prevention event, and they had the exhibit set up in the hallway. So, you’re going down the hallway and boom—there it is. Those are my quotations; those are my nightmares. That’s me. It’s also a snapshot of me at a particular time and space, and I’m very different now than I was then, as I anticipate everybody will be, but you’re essentially frozen in time on a wall in a lot of different places.
While we have come to recognize the impossibility of articulating in advance how far a study will travel in terms of dissemination, or how an individual participant will feel as their stories are shared in different public and academic venues, we make every effort to ensure participants are aware of, understand, and are comfortable with each stage of dissemination. In this regard, informed consent is not a piece of paper signed at the front end of the study, but rather an ongoing and evolving conversation. This approach takes time and goes beyond what is required by an IRB, but we feel it is essential to ethical practice in the work we do; as Lawrence has observed about his own and other Veteran’s research participation, “you contribute pieces of yourself to the research, and deserve agency over those pieces.”
Sarah and Gala have discussed how doing community-engaged work complicates researchers’ feelings about and relationships to the concepts of consent and use of participants’ data in dissemination of findings. As Sarah has noted, What is at stake . . . ? There is always the risk of a privacy breach. This is complicated because what feels “private” may change over time, and, while the intent is to maintain a relationship so that these changes can be identified, there is also the risk that a breach has more significant impact as a result of a stronger connection. . . . Extended contact and a personal connection between the researchers and participants can also up the stakes for both.
Over years of working together, we six (and our other researcher, Veteran, and caregiver collaborators) have shared common research and advocacy goals, traveled to present at conferences, and marked important life events (births, marriages, hospitalizations) together. Our research relationships have developed into friendships, or what Maria Mayan and Christine Daum have termed “muddled relationships” (Mayan & Daum, 2016). Like Mayan and Daum (2016), we argue that such relationships have been key to achieving success in our research while also recognizing the need for a more nuanced and extended approach to consent than what is proscribed by IRBs and privacy rules.
Sharing Ownership and Sustaining Engagement Through Dissemination
Unlike more traditional forms of research, we have incorporated early opportunities for dissemination with study participants and researchers as copresenters. We have also supported Veteran and caregiver participants in presenting the research on their own or sharing their personal stories with health care providers and other audiences in alignment with the advocacy goals of photovoice (Corrigan & Shapiro, 2010; Knowles, Rabinowich, Gaines-Turner, & Chilton, 2015). We have developed processes to ensure that any participant–collaborator who wants to be involved in dissemination of findings can do so; we have shared templated PowerPoint slides with Veterans and caregivers to adapt for their own presentations, provided support and training in presentation skills when needed, and asked hosting organizations to provide honoraria or travel funds for copresenters when possible. As a result, our collaboration has led to dozens of presentations and panel discussions that include Veterans, caregivers, and researchers as copresenters over the years.
Ray has talked about how the exhibit, and seeing audience reactions to the exhibit, has connected him with the other Veterans in the study and provided a sense of ownership over the research and its impacts: I remember seeing the exhibition for the first time—I was looking at all of the stories and thinking to myself—“Wow, this is what I feel. These words could have come from my mouth.” I felt a connection to everyone else’s experience. When I was asked to help present the project, that feeling made it easier. I felt like I could take everyone else’s words and make them my own—I could take ownership over them and say, “Hey, this is what we are going through.” I felt grateful to everyone in the room who was listening, because it felt like it was the first time they were listening.
Lawrence extended this idea by talking about the challenge he faced of being one Veteran advocating on behalf of other Veterans he did not know personally, and how he negotiates that challenge through his involvement in the study: To be comfortable advocating and speaking, but also demonstrating or somehow explaining to the people you’re talking to, “I don’t represent every Veteran.” That shouldn’t make me hesitant to speak out about what I see as my Veteran experience, and if it is relatable to other Veterans, good. I think there’s always that hesitancy for Veterans, “I’m not going to get up there and talk about Veterans. I’m one Veteran, and I don’t want people to think I know everybody.” How do you do that? How do you navigate that? Understanding the value of my singular experience, shaping the vocabulary and voice that I can stand behind—both for an audience and for my inner monologue—that was a product of this research collaboration.
In the summer of 2015, between the photovoice pilot and the current study, Ray and Lawrence conducted a workshop with Gala and Sarah at the annual meeting for VA health services researchers (Figure 8).

HSR&D workshop presenters.
At the time, it was uncommon for Veterans who were not researchers or VA employees, to present at the meeting. We saw this as a significant opportunity and tipping point toward increasing visibility and collaboration with Veterans in venues conventionally marked as “research” spaces. The session (“Methods, Materials, and Ethics of Community-Engaged and PAR in VA: Learning from Ongoing Veteran–Researcher Collaborations”) was an early step toward the reflexive process that has led to this article. As Sarah commented, The room was packed, which was amazing, and Gala and I were both aware that David Atkins, the Director of VA’s Health Services Research and Development Service, was seated a few rows back on the center aisle. He asked good questions, and we observed the back and forth between him and Lawrence. Lawrence, to his credit, didn’t hold back; he shared what he thought. Only later, afterwards, did Lawrence say to Gala and me, “Yeah, I figured out that guy was probably kind of important . . . I hope I didn’t say anything that will cost you your jobs.”
We all remember this exchange a bit differently but understood that in that experience we had solidified our trust in each other and our confidence in the process of copresenting. Not only was there the hurdle of asking Veterans to get up in front of a room full of researchers and answer unprepped questions, but Lawrence and Ray also had to go through the lengthy, bureaucratic process of being “vendorized” by the VA so they could be reimbursed for travel. Yet these efforts provided a platform to amplify Veterans’ voices and a chance for an institution such as the VA to compensate for its inability to “hug.” David Atkins sent Lawrence a handwritten note of thanks for his participation in the panel. In the letter he expressed gratitude for the opportunity to exchange ideas and listen to Veterans; he concluded, “I’m committed to increasing what we do in HSR&D to ensure our research has the Veteran at its center.” We recognize there are a range of ways in which individuals and institutions can respond to these interfaces; here, the response allowed for human connection and created a doorway of trust between VA research and Veteran communities. While at the meeting, Ray and Lawrence were interviewed about their experience collaborating with research, and short videos were made. These videos are still available on HSR&D websites and have been used in multiple contexts. Links to videos can be found at https://www.hsrd.research.va.gov/news/video/RayFacundo.cfm and https://www.hsrd.research.va.gov/news/video/lawrencedavidson.cfm)
As Gala recalled, In my mind, that panel is significant because it’s the first time we all presented together . . . also, many of the questions asked by the attendees ended up being topics addressed in the SERVE Toolkit. VA investigators were looking for practical tips and “how to” at that time.
This article, and the process we used to write it, represents a part of our work not captured in a toolkit—feelings that are part of our relationships and the impact of our work on all of us at a very human level.
The Unanticipated Value of Traveling This Road Together
Great effort has gone into identifying and measuring the impacts of CEnR approaches on the quality of research, as well as on improved clinical practices and individual and population health outcomes (Brett et al., 2014a, 2014b; Dillon et al., 2017; Ellis & Kass, 2017). In our conversations over the years, we have also noted the impacts of our collaboration that are not commonly addressed in the literature and are challenging to measure in any standardized way but are essential to our individual reasons for remaining engaged in the work and continuing our partnerships during times in-between funding and through cross-country relocations. Here, we enumerate the impact of our CEnR in three areas not typically counted as outcomes of health research.
Community Engagement as a Bridge Between Veterans, Caregivers, and the VA
As noted above, some Veterans and their family members may distrust the VA for many reasons: prior negative experiences with aspects of military service, challenging circumstances surrounding their separation from service, or negative interactions with VA staff and procedures when seeking diagnosis, treatment, or benefits. Over the years, we have witnessed how Veteran–researcher collaborations can be a starting point for building more positive views by countering some of those negative experiences. As Lawrence has observed, It’s very easy to sit here and smash the VA with other Veterans, listening to secondhand stories and responding with corroborating anecdotes. But the reality is that oftentimes they’re the only dealer in town, and so this is our health care. When you’re trying to fix an organization, it can’t just be a constant tearing down, a competitive game of “gotcha.” There has got to be pieces and parts of it that are working. How do you [the VA] demonstrate that you’re listening? You put this exhibit, on Veterans Day, on the first floor of a VA medical center.
Because Veterans and caregivers have equal say in coproduction and sharing of knowledge, the study findings (in this case, the exhibits) are accessible and “ring true” to participants as an authentic and uncensored representation of their experiences and views. That this research was funded and supported by the VA, and that VA facilities are willing to install exhibits including stories that are at times highly critical of VA care, confers a measure of trust in the VA; as Lawrence goes on to note, [The exhibit] wasn’t a hug fest about people’s experiences within VA health care. It was the first kind of real [experience] where you begin to understand that the VA is not a ubiquitous brick machine, and that there are individuals within it that are working very hard and trying to do well for Veterans. I don’t know how many other opportunities you get to interface with the VA in that way . . . to be able to build a relationship. Institutions don’t hug people, so how do you get to know them and trust them when they already start with two strikes? When the VA opened the exhibit, it could not have been a better place to start building trust. I never lost sight of the fact that it was the VA that had conducted this research, and that it was the VA that produced this exhibit. It was not a highlight reel, but an honest self-reflection and gave a true sense they desired self-improvement.
Our collaboration over the years has resulted in many Veterans and caregivers becoming more involved in research as consultants and co-researchers. After participating in the first photovoice study and in dissemination of study findings over several years, Ray approached Gala with an interest in coming to work on VA-funded research; he observed that, based on his past experiences with VA as a patient and an advocate for other Veterans, he would never have considered working for VA if not for the experiences he had with CEnR. In this regard, Ray’s decision to move cross-country to become a research manager for the VA illustrates how our collaborative work aligns with principles of PAR, which calls for increased capacity for research involvement among individual patients and communities.
On our call, Gala and Sarah talked about how the nature of doing CEnR creates a sense of raised expectations for what the research can accomplish, and concerns about not being able to meet those expectations at times. Gala and Sarah observed how IRB protocols and VA policies focus on areas such as protecting against a data breach, but the greater area of concern is around the integrity of relationships with Veteran and caregiver collaborators and the possibility of inadvertently upsetting or harming a research partner. As an example, Gala reflected on how she struggled during the pilot study with concerns about how to be fair and inclusive when opportunities arose for Veteran participants to present findings, especially when those opportunities were accompanied by tangible benefits (e.g., monetary compensation, reimbursed travel) or intangible benefits (e.g., recognition from others, sense of mission). She commented, Nearly every Veteran expressed willing enthusiasm to give talks, be on panels, speak to the media . . . and I had to think hard about my role as “gatekeeper” to the benefits that came with these opportunities and how to be equitable and transparent so everyone understood how someone was offered a specific speaking opportunity . . . I also had to work against my own natural bias towards inviting Veterans who were particularly compelling or eloquent speakers.
As a practical solution, she developed a simple spreadsheet to track which participant–collaborators expressed interest in being part of dissemination, who had already presented, and who should be offered the next opportunity to present. She also consciously invited every Veteran participant to attend an event, even if they were not a featured speaker, and made it possible for any collaborator in the audience to contribute from the floor if they wanted to respond or add to the conversation. We have carried these practices forward into our current research. This is just one example of proactive practices we have built into our work. However, we recognize the impossibility of guaranteeing that we will never encounter misunderstandings or hurt feelings during our collaboration. No IRB protocol can anticipate all contingencies; the best we can do is focus on transparent, honest communication and hold up our part of the personal contracts we have made with each other.
We are realistic that engaging Veterans, caregivers, and other stakeholders in research is not a panacea to resolve all individual and community mistrust in VA; as Lawrence observed, “One negative interaction can set you back again.” However, our personal experiences indicate that VA’s investment in engaged research provides a platform for building relationships that can lead to improved individual Veteran and community participation and trust in research and in the VA.
Storytelling as a Path to Connectedness
As Robert Atkinson (1998) has noted, sharing our life stories increases self-knowledge through the process of reflection and articulation of events, experiences, and feelings to another. On one of our calls, Sharon and David talked about how creating their narrative for the study and sharing it with a researcher challenged them to work through painful emotions but was ultimately helpful in their personal growth. Sharon said, As a caregiver, I was so used to helping my husband engage his own coping skills to deal with his emotions. But I wasn’t ready to have to sit in my own emotions and work through that. And so it was an opportunity [and] a challenge that I had to work through. I wasn’t ready for that . . . it was a true surprise to me. I was holding tight for so long. And then, for the first time ever, somebody asked me to tell my story, and I started to loosen that grip . . . I wasn’t ready to sit in those emotions to think about them. So that was a challenge for me at the beginning.
David agreed and responded that he would add the word necessary, “ . . . to have the desire to acknowledge the challenge and persevere based upon the interactions with the research was a necessary component in our personal growth.”
Although photovoice is not intended as a therapeutic intervention, the experiences that are a central focus of our research—going to war, transitioning home to civilian life, living with visible and invisible injuries, or loving and caring for someone who has been through all these things and more—can cause deep feelings of dislocation, alienation, and isolation (Moriarty et al., 2016; Ramchand et al., 2014; Smith & True, 2014). The separations of deployment, as well as many Veterans’ tendency to avoid disclosing wartime experiences to family and friends, may disrupt key relationships and erode close social networks, while a lack of knowledge and understanding on the part of many civilians adds to the sense of loneliness and “otherness” for many Veterans and military families (Smith & True, 2014). Our approach has recognized and harnessed the power of private and public storytelling to make the invisible visible, engender self-awareness and empathy, and begin to create community (Atkinson, 1995, 1998; Maynes, Pierce, & Laslett, 2008; Potash, Ho, Chick, & Au Yeung, 2013; Ziebland & Wyke, 2012).
In keeping with traditional photovoice methods, participants begin by reflecting on which photographs to take for the project and deciding what to share with the research team in an individual photovoice interview. During two photovoice studies, Gala has observed how the use of visual images as the focal point of the interview—with researcher and participant looking mostly at the images rather than directly at each other—allows participants to share their stories of trauma and loss with the researcher, and the researcher to receive these stories, in a way that might not be possible using conventional qualitative interviewing methods. As one Veteran—who disclosed multiple traumatic combat experiences, years dealing with opioid addiction and methadone maintenance treatment, and the dissolution of his marriage—said to her at the conclusion of a 2-hour interview: “I never told anyone all of these stories before . . . to be honest, I kind of forgot you were even here.” Another participant, Michael, shared a photo of a bottle of vodka next to a bottle of ZzzQuil (an over-the-counter sleep aid) to reflect on combat traumas he had not previously shared with anyone and on the negative impact of his attempts to numb himself through self-medicating (Figure 9).
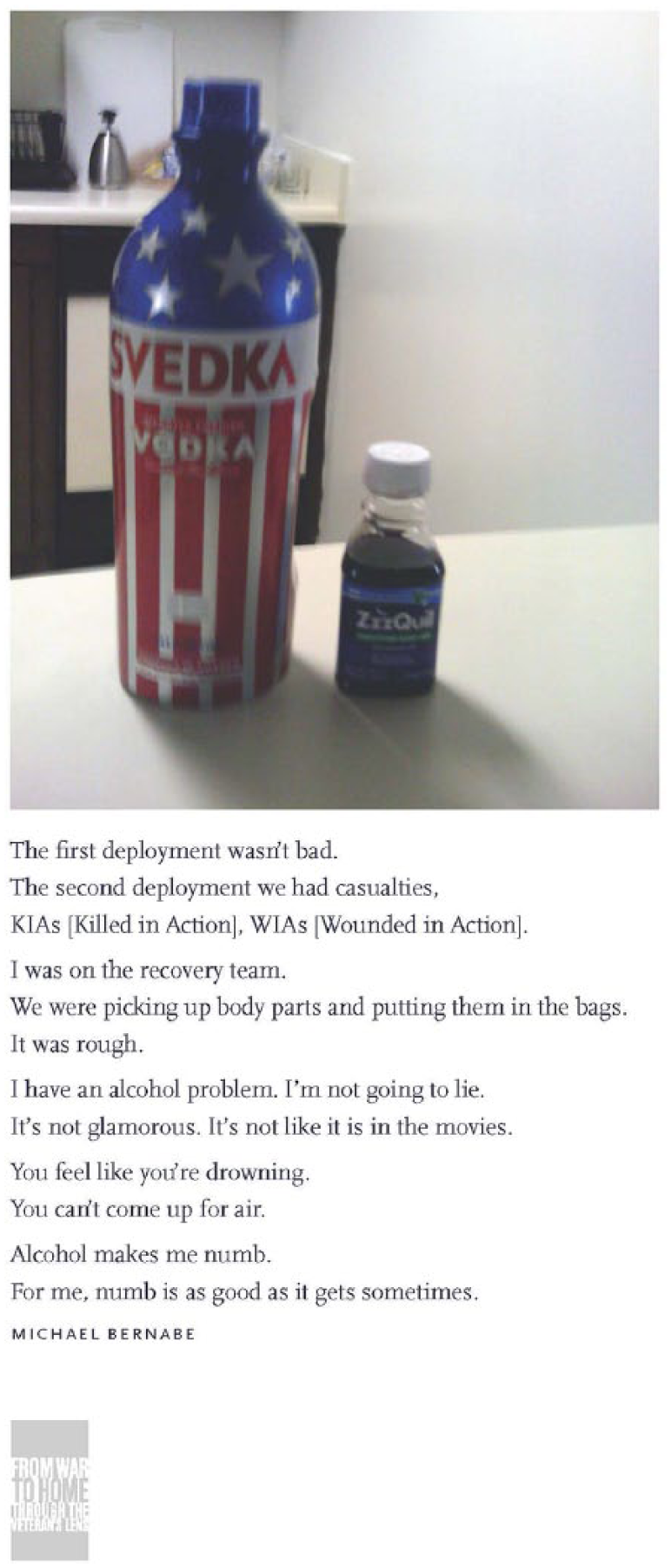
Michael B seeking numbness.
Echoing the experiences of other participants, Sharon has observed how engaging in this process helped her: Photovoice gave me a voice and helped me put my story into chronological order, because we did photovoice less than six months into our transition out of active duty and at a very intense emotional time. It was the start of my personal healing process.
Over the years, we have been struck by hearing something similar from every photovoice participant; how reflecting on, creating, and sharing their narrative with others has led to greater awareness of challenges they are facing, their unmet needs, the strengths and sources of support that exist in their lives, and the necessity of seeking out further help and support to move forward in healthy ways. As a caregiver, David spent several years completely focused on understanding and addressing the significant health care needs of his husband. Thinking about the impact of his participation in the photovoice project, he said, I was thinking back . . . and I didn’t realize before participation that I had, or felt a need, to do this. I was completely unaware. But then, once it happens, the light clicked on and “Oh shit, this is awesome,” and it fills a gaping hole that needs something to address it.
Like many participants, Sharon contributed a photograph to the project that is particularly meaningful to her for its power to articulate painful and otherwise hidden thoughts and experiences, both to herself and to others. She took a photograph of an abandoned, rusted boat with a storm looming in the background (Figure 10); it explores and explains the loneliness and isolation she has felt as a caregiver: It’s my favorite photo out of any photos from the project. It captured that part of my journey as a caregiver; it depicts something I’m not always comfortable talking about—how isolating and how lonely it is. It was the image for how I was feeling. When I talk about photovoice, I show that photo. I’m very proud of that photo and how it helps me talk about something difficult.
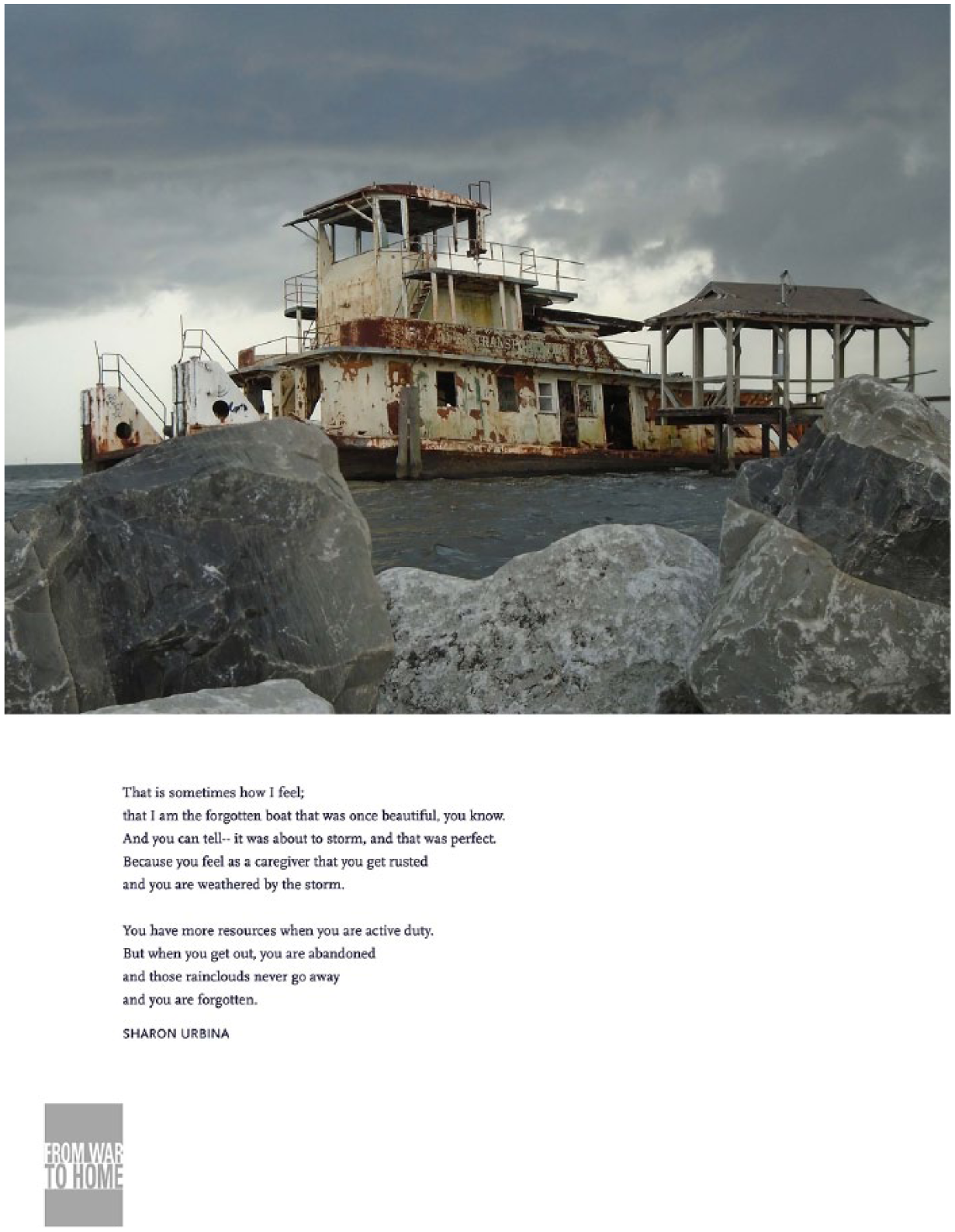
Abandoned boat.
In response to feedback from Veterans who participated in the pilot study, and their family members who came to see the exhibit and said it was the first time they had heard about many of their loved-one’s experiences and thoughts, we adapted photovoice methods for our second study. Specifically, Veterans and caregivers who participated as a dyad were asked to share their photo-narratives with each other and then be interviewed by researchers about that process and its impact. Later, Veterans and caregivers met in small groups with the research team to reflect and comment on each other’s stories and discuss goals for using study data and findings.
During one of our calls, Sharon and David reflected on how participation in the project had affected them as individuals, as well as the impact on their respective marriages. As Sharon commented, . . . but what [study participation] did for our marriage was also important. It was a way for me and my husband to communicate the struggles we had been through, but also kind of a check-in of, this is where we are now separately, emotionally, and what we’re going through. And because of that, we were able to work through larger issues. And I can’t put a number on that. There’s no way to express how important that was. I mean, it was life-altering for us.
David agreed and went on to observe how the research collaboration led to him and his husband, Donny, feeling less isolated: I’d add that photovoice made me actively realize that I was not alone. It was very serendipitous to be included in the research, because at that exact moment in time I didn’t know what was going on, or what we were going to do, or how to even begin to move forward again after having just treaded water for so long. And the other thing is realizing that the pressures we were and are facing are not isolated to just us; some things that Donny experiences, Carlos experiences, Tyler experiences, or Drew experiences, maybe not in the exact same way, but they are all permutations of similar conditions.
As an unexpected outgrowth of our ongoing collaboration, Veteran and caregiver participants have created a sense of community and informal support networks among themselves. They have exchanged contact information at dissemination events or group meetings and stayed connected through social media, texting, and in person get-togethers where they celebrate each other’s life events, share information about therapeutic interventions and benefits, and support each other through challenging times.
Sharon noted the personal importance of these relationships and interactions, which spring from the research but take root and grow outside official research-sponsored activities: The friendships that I’ve made and been able to develop through the project are invaluable to me, and I can’t put a number on how important they are . . . those relationships all came out of photovoice, nowhere else. And I don’t feel I would ever have made those connections with that particular group or with those friends anywhere else in the VA . . . it will bring me to tears sometimes, because it’s so important to have a community and a support system. And when you are able to grow that community and that support system with true genuine friends, that is invaluable.
Although these connections are not officially recognized as part of the research, those of us employed as VA researchers recognize and appreciate their value as both a source of support to individual Veterans and caregivers and as a means to strengthen and sustain the collaboration. We also value knowing the work we are doing is having an immediate, positive impact on the lives of some of the families with whom we interact. As Gala remarked on a call: These impacts don’t typically get counted in research, but they are significant for all of us. I can say it’s one reason I keep doing research . . . the relationships with you all, and hearing about how you are supporting each other. I found a note that Sharon wrote us a while back, about the impact of the project on you all. I had saved it so I can look at it anytime I need encouragement. So, that’s the impact on the researchers, and we don’t get to write about that or think about it very often. We talk about it amongst ourselves, but we don’t talk about it in academic journals. And David, you gave me a picture of all of you [Veterans and caregivers] together, celebrating a birthday, and it means everything to me. It’s the fact that you have this community that you’ve created, and you did that outside the project. I mean, we got you together at first, but you did everything after that.
David agreed, saying, “You all [the research team] were the genesis, but we kept it going organically, and we’re all the better for it.”
Over time, Ray and Gala have built connections with VSOs and arts-based nonprofits in New Orleans and around the country. Recognizing the need for more community events that bring together Veterans, their families, and civilian allies in safe spaces for dialogue and creative expression, they cofounded the NOLA Veterans Arts and Humanities Alliance, a group of local Veterans, artists, VA colleagues, and representatives from arts nonprofit organizations. This group has organized several free events open to the public, including the annual Get Your Art On event, where Veterans and caregivers from the photovoice study spend the day with others engaging in art-making, writing, playing music, and other creative outlets. Gala and Ray conduct these activities during their personal time but see these efforts as essential to building and sustaining community engagement in their professional work (Figure 11).

FWTH community event.
Advocacy and Finding New Purpose
The literature and our own personal experiences highlight the struggle many Veterans face when it comes to finding meaning and purpose after military service (Calica & Basl, 2014; Smith & True, 2014). Likewise, many caregivers give up aspects of their personal identity (e.g., careers) to care for their loved one (Moriarty et al., 2016; Ramchand et al., 2014). A central goal of PAR, including photovoice, is to provide a platform and the tools for people affected by a problem to identify and advocate for solutions. Veterans and caregivers in our collaboration have observed how engaging in dissemination efforts and sharing their stories as part of advocacy activities has helped them find new meaning and purpose. As an outgrowth of her collaboration with the project, Sharon decided to apply for, and was selected as, an Elizabeth Dole Foundation Fellow, giving her a platform to continue to advocate on behalf of the needs of other military caregivers. Sharon says about her collaboration, “Photovoice gave me my voice to tell my story, and I’ve really come into my own.”
Over the years, Gala has seen Veterans use their collaboration on the first photovoice study to achieve their personal goals. Veterans have used their photo-narrative as part of an application for admission to graduate school or for a scholarship, requested recommendations from her for job and school applications, and developed research presentations based on study findings as capstone projects for school. More than one person has gone into advocacy, research, or service-related work. Although their collaboration on the research is not the only reason for this—Veterans often seek positions that serve the greater good of society, including helping other Veterans, after they leave military service—photovoice participation has served as a catalyst for many. Lawrence reflected on past conversations about comparisons between large-scale quantitative research studies, valued for yielding more generalizable findings, and CEnR, often conducted on a much smaller scale: . . . the idea that what you’re finding isn’t generalizable because you only have two collection sites in Portland and New Orleans. . . . Well, if we’ve done community-engaged research in this manner across seven years . . . I don’t know if it’s generalizable to say it has activated people, it’s given them a voice, but that’s consistently what I hear from people who participated. . . . If you take a survey-based, quantitative piece of research that touched 15,000 data points nationwide . . . and you asked 15,000 of those people, “Did that research study impact your life, positive or negative, and if so, to what degree?” I would argue there’s going to be a vast majority, if not all, who would say, “I don’t even remember the question, I didn’t see the results, and as far as I know it didn’t impact me whatsoever.”
Lawrence’s observations illustrate the value and impact of CEnR to empower participants and “activate” them in order to identify gaps in services and to advocate for change for themselves and others in their community and also highlight the importance of conveying research findings back to individual participants and communities impacted by the research topic (Littman et al., 2018; McDavitt et al., 2016).
PAR, by developing pathways for participants to be advocates, begins the important work of helping people see the connections between research being conducted in their communities and the treatments and services available to them. Photovoice, like other arts-based research methods, furthers that connection by allowing production and dissemination of research findings in ways that are accessible beyond traditional academic venues. As Ray said, I’ve seen where the photovoice exhibition has gone, and the way the project has been disseminated. I’m not somebody who’s going to sit around and read academic papers. Most of these papers, the lay population is never really going to see. As the Veteran, as a part of this community that was being studied, I’ve watched this exhibition go from universities to different VAs, from the opening of a play to a social work conference that I was presenting at, to classrooms, to webinars that are attended by VA employees across the country. It’s been so cool to work on the second project as someone who had participated in the pilot, because I do have a sense of ownership over this. . . . Now we have this community of folks who were impacted, making us better self-advocates and community advocates. You can see what we’re all doing these days, and it’s directly attributed to our participation in the photovoice projects. We are able to tell our own stories and listen to how other people tell their stories. Through participation in this project, we found effective ways of communicating our needs.
Concluding Thoughts
Photovoice is similar to other methods that incorporate visual data into research (e.g., photo-elicitation), as well as approaches that enable research participants to control the telling and sharing of their own stories (e.g., Life Story, timelines). However, we particularly value photovoice for its emphasis on what Lisa Bowleg (2017) has described as “ . . . the dismantling of oppressive structures and catalytic validity—the extent to which the research process prompts participants to understand their lives and experiences in order to transform them” (p. 679). At the same time, we recognize the ways in which CEnR approaches such as photovoice can be limited in both their implementation and their impact. Working within the challenging bureaucratic environment of institutions such as the VA can impose constraints on coproduction and sharing of knowledge; for example, when we are not allowed to use social media to disseminate findings more widely or connect research participants to support each other and facilitate collaboration. We see irony in the fact that our findings can be most powerfully disseminated through photographs paired with brief explicatory text, and yet we have been unable to get permission for a VA-sanctioned account on Instagram—a platform where “Humans of New York” has over 8 million followers—to disseminate our findings to a wider audience. As Veterans and caregivers—many of whom are inveterate users of social media and Internet support groups to find information and connect with each other—gain traction as advisors and partners in VA-funded research, we hope they will push the VA to increase its use of technology to reach Veteran and military communities for research recruitment, data collection, and sharing of findings. We believe, as Bowleg has pointed out, that adherence to conventionally accepted ways of knowing and building knowledge—whether conscious or unconscious—is a primary barrier to innovation and a block to the transformational leaps necessary to improve our health care systems. Our focus on public-facing dissemination and building capacity for community–researcher partnerships to influence shifts in policies and processes of care is aligned with Bowleg’s observation that research alone is not enough to advance health equity.
The past decade has seen the emergence of “altmetrics,” a field that describes efforts to track the broader scientific impact of scholarly works beyond citations in other scholarly articles (i.e., impact factor) to encompass additional measures such as number of online views and downloads or mentions in blog posts, tweets, and other social media (Mehrazar, Kling, Lemke, Mazarakis, & Peters, 2018; Rees, 2016; Troja, 2017). We argue that there is also a need for more humanistic measures to capture the impact of collaborations such as ours on both researchers and community partners in areas such as trust, human connection, compassion, and resilience (Hooyer, 2017; Lee et al., 2016). Research rarely offers social connections as a benefit of participation, but perhaps it is a benefit that should be given greater consideration. In research, we identify cohorts of individuals with something in common—whether that is a health condition or a shared experience that affects health—and focus on privacy and other measures to ensure that participants cannot be identified. But what if participants opt into identification and the opportunity to connect with others who have something in common? Photovoice allows participants to set their own parameters on privacy and make connections that extend beyond the scope of the research and into people’s lives. CEnR approaches can provide a space where we can think beyond the research needs and also strive to address the human needs of all involved.
On one of our calls, Sarah and Gala listened as other coauthors summarized the impact of the research experience and public display of their stories. Lawrence said, I say it all the time. After the military, there’s not a whole lot to hang on the refrigerator for a lot of folks. It’s hard. I mean, how do you demonstrate to other people what you’re doing . . . the exhibit is really kind of, “this is where I’m at, and this is what I’m doing.”
Ray said, “The exhibit is a giant, ‘I love me wall.’”
David agreed, So much courage. The word courage just comes to mind . . . that it takes a lot of courage for all of us to put our words onto a recording and then to see them come up on the wall. That was a big deal.
Ray concurred, “To show yourself that you can do that. Yeah, that’s a big deal.”
In academic writing, researchers typically get the last word—the final interpretation or framing of the data, designed to answer the research questions and (hopefully) set them up for the next round of funding. We have tried to do something different in this article, in the hope that it illustrates what is significant and special about this research and the relationships that have come from it. Perhaps this kind of shared reflection can advance collective thinking about what constitutes research and our measures of success. This work has brought us so much more than any publication or product can offer; it has brought us into contact with each other in a way that is deeply human.
Footnotes
Acknowledgements
We wish to acknowledge the essential contributions of the other Veterans, military caregivers, and research staff with whom we have collaborated over the past several years and our colleagues and friends from community organizations and clinical settings who have supported this work and enabled the two From War to Home exhibits to travel. We also thank John Marmion, MPH, for his help in preparing this article and the anonymous reviewers for their helpful feedback and suggestions.
Authors’ Note
The views shared in this article are those of the authors and do not represent the views of the Department of Veterans Affairs, the U.S. government, or others who work within this organization.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Primary funding for this work is from two VA HSR&D awards to Dr. True (PPO 10-55 and IIR 14-399). Dr. True is also supported by the South Central MIRECC. Exhibit production and travel for From War to Home: Through the Veteran’s Lens was supported by the Center for Health Equity Research and Promotion and the Center for Evaluation of Patient Aligned Care Teams. Dr. Ono is supported by CIVIC (VA HSR&D CIN 13-404).