
Abstract
Existing studies show a reliable association between literacy and mental health problems, such as anxiety and depressive symptoms. Much of this research has been conducted with primary school-age children, with less research focusing on adolescents and older adults. The current study included a sample of children (N = 478; Mage = 10.1, SDage = 1.9), adolescents (N = 438; Mage = 15.6, SDage = 1.7), and older adults (N = 111; Mage = 68.5, SDage = 6.0) who completed measures of self-reported literacy difficulties, anxiety (reading anxiety, social anxiety, generalised anxiety, panic, separation anxiety, and obsessive-compulsive symptoms) and depressive symptoms. Analyses included partial correlations and associations compared across age groups. We found significant and moderate-to-strong correlations between literacy and reading anxiety for children (parent and self-report), adolescents (parent and self-report), and older adults. There were moderate and significant associations between literacy and social anxiety for children (self-report) and older adults, but not for adolescents. There were moderate and significant associations between literacy and depressive symptoms for children (self-report). These results show associations between literacy and reading anxiety symptoms at various life stages, including childhood, adolescence, and older adulthood, and between literacy and depressive symptoms for children – highlighting the need for pathways of care to support individuals of all ages.
Introduction
Around one in three children struggle with literacy (e.g., reading and spelling; Hunter et al., 2023), and their literacy difficulties frequently persist in adolescence and adulthood (Shaywitz et al., 2008). These difficulties are clearly associated with poor educational outcomes, occupational attainment, and peer relationships (Maughan, 1995). There is also emerging evidence of an association between literacy difficulties with anxiety and depressive symptoms in children (Francis et al., 2019; Francis, Hudson et al., 2022). However, it is not yet clear whether these associations are evident at other stages of life, such as during adolescence (e.g., 13–18 years) or later in life (e.g., at least 60 years of age). Thus, the aim of this study is to understand if relationships between reported literacy (e.g., reading and spelling skills) and reported mental health (e.g., anxiety and depressive symptoms) differ between childhood, adolescence, and older adulthood.
Literacy Skills and Difficulties
Literacy is a very broad term with many definitions. Within the context of this study, it is defined as the ability to read and spell. Reading and spelling depend on a number of cognitive skills, including the ability to use letter-sound rules and sound-letter rules to read and spell words (phonological decoding and recoding, respectively); the ability to recognise or produce the spellings of whole words, or parts of words, from memory (orthographic recognition); and the ability to understand written words and texts (reading comprehension; Castles & Coltheart, 1993; McArthur et al., 2013; Nation et al., 2010).
While often identified during primary school, individuals can continue to struggle with one or more of these skills into adolescence and adulthood (Shaywitz et al., 2008; Snowling et al., 2020). However, little is known about the progression of literacy difficulties into older adulthood (i.e., 60 years +). Given developmental changes over the course of a lifespan, there are reasons why changes in the strength of associations between literacy skills and mental health might occur at different ages. For instance, given the increased self-consciousness of the adolescent period, it could be hypothesised that poor literacy might be associated with heightened anxiety and depressive symptoms compared with other age groups. In later life, it could be expected that after a lifetime of practising literacy skills, associations between literacy and mental health might be weaker as people have either improved their literacy skills or become more accepting of their skill level. However, to the best of our knowledge, no studies have evaluated associations between literacy and mental health outcomes for older adults or examined differences in these associations in different-age samples – highlighting the need for further research in this field.
Anxiety and Literacy
Anxiety is a common emotion characterised by the anticipation or perception of threat and a fearful emotional response. Although it is a natural experience, when it occurs frequently and intensely, it can be considered problematic because the experience of anxiety and accompanying symptoms interferes with a person’s life at home, at school or work, or with their friends (American Psychiatric Association [APA], 2013). Anxiety can arise in response to various threats across different situations and presentations of anxiety symptoms have been grouped accordingly into anxiety disorders as described in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013). Common types of anxiety disorders and symptoms likely to be associated with literacy difficulties are social anxiety disorder, where the individual fears being negatively evaluated by others; generalised anxiety disorder, where a person worries about a wide range of issues and circumstances; and panic attacks, where a person experiences a discrete period of intense fear that occurs with or without a trigger.
Research suggests that children with early reading and spelling difficulties (Grades 2 and 3) are at greater risk for social anxiety in later childhood (Grade 5) than their typically reading peers (Kargiotidis & Manolitsis, 2024). In addition, studies have shown that literacy difficulties can negatively impact self-concept, which in turn may contribute to heightened anxiety levels (Polychroni et al., 2024). For instance, social anxiety disorder may be linked to literacy difficulties, given the potential for negative evaluation or judgement from others associated with their literacy difficulties. Generalised anxiety disorder may be linked to literacy difficulties, given the constant worry one may experience about making a mistake during literacy tasks, and/or the impact literacy difficulties may have on school performance and/or the future. In turn, panic attacks may occur when presented with a literacy task. Interestingly, just one study has compared different types of literacy difficulties with different types of anxiety. The results showed a weak association between literacy (specifically reading accuracy) and social anxiety, but no clear associations with other forms of anxiety including generalised anxiety symptoms or panic attacks (Francis, Hudson et al., 2022). These findings align with broader research indicating that literacy difficulties can contribute to negative self-perceptions and increased anxiety in children and adolescents (Gibby-Leversuch et al., 2021).
Although not a distinct anxiety disorder, individuals with literacy difficulties often report anxiety around reading and spelling. More specifically, this may include fear of reading aloud or spelling in front of others (social reading anxiety) and worry about making mistakes or getting into trouble for poor performance on literacy tasks (generalised reading anxiety; Jones et al., 2025). The individual’s anxiety is specific to reading and is not captured in typical standardised questionnaires used to measure the different forms of anxiety mentioned above (Fishstrom et al., 2024). This concept of “reading anxiety” has been described in the literature as “an acute fear or apprehension related to situations that require the processing of textual information” (Ramirez et al., 2019). It overlaps with existing DSM-5 anxiety disorders such as social anxiety disorder in that one may worry about being negatively evaluated by others, given their difficulties, and generalised anxiety disorder, in that one may worry about making mistakes or getting into trouble related to their literacy difficulties. There may be some cases where anxiety related to reading occurs within the broader context of “social or generalised worries”, but there may be other situations where an individual has very specific anxiety related to reading alone. In this case, it may be more aligned with a specific phobia or “anxiety not otherwise specified” diagnosis.
Regarding the link between literacy and anxiety, one causal model (originally termed the Poor Reading-Anxiety “PRAX” model and updated to the Wellbeing in Literacy “WiL” model) states that a child struggling with literacy (e.g., falling behind their peers in the classroom) develops a negative self-concept about their literacy skills, which results in anxiety and reduced engagement in literacy-related activities, which further reduces their ability to develop literacy skills and exacerbates their concerns with self-concept, anxiety, and engagement (McArthur, 2022). While this causal hypothesis presents one explanation for the link between literacy and anxiety for children, there may be other factors that explain potential associations between literacy and anxiety and depressive symptoms and disorders for adolescents and older adults. The cumulative risk and resilience model of dyslexia (Catts & Petscher, 2022) offers another way to understand these relationships, shifting the focus from identifying a single underlying cause to understanding literacy difficulties as the result of multiple interacting risk and protective factors (Haft et al., 2016; Stein et al., 2024). For example, adolescents and adults who have developed a negative self-concept about their literacy skills may be exposed to fewer situations where these beliefs are reinforced. Alternatively, adolescents and older adults engage in “other” activities that do not rely on “learning to read,” which may buffer or compensate against their literacy struggles. For example, Giovagnoli et al. (2020) found that positive relationships with peers were a protective factor associated with low internalising symptom severity. With the causal model and these findings in mind, factors such as feelings of sadness, peer relationships, school environment, and family support may be important contributors to the development of this association for adolescents and older adults. Thus, further research is needed to better understand the nature of the association between literacy and anxiety and depressive symptoms for individuals at different stages of life.
Depression and Literacy
Sadness is another common emotion, but as with anxiety, when feelings of sadness or low mood are frequent and persistent, it can become problematic and better defined as depression (APA, 2013). Depressive symptoms, or symptoms of low mood and sadness, may be linked to literacy difficulties due to the risk of developing a negative self-concept associated with repeated literacy failure in the classroom – particularly for primary school-age children – and rumination about past literacy failures. Research suggests that children with literacy difficulties experience higher rates of depression than their peers, reinforcing the link between negative academic experiences and emotional distress (Li et al., 2024).
This may then lead to feelings of sadness and withdrawal from school, peers, and their family, which further exacerbates one’s literacy difficulties. Research has shown that students with literacy difficulties feel sad, lonely, and struggle with peer interactions (Morgan et al., 2012). For adolescents and older adults, the link between depressive symptoms and literacy may persist due to unhelpful strategies (e.g., negative biases or rumination) or literacy-related stressors (e.g., school performance stressors for adolescents or occupational stressors for adults). Research also suggests that depressive symptoms in adolescence are associated with poorer educational and occupational outcomes in adulthood, highlighting the long-term impact of early mental health and literacy challenges (Keyes et al., 2024). However, these are speculative possibilities that require further investigation.
Literacy and Anxiety and Depression
The association between literacy and anxiety and depression is an emerging area of research. In 2019, a meta-analysis revealed a significant and moderate association with reading difficulties and anxiety (d = .41), and a significant but weaker association with depression (d = .23) across children, adolescents, and adults (Francis et al., 2019). Francis et al. discussed that the association with depression appears to be “complex.” Adding to this complexity is the fact that many studies fail to assess for depression during childhood, with the focus tending to be on anxiety. Since the last review, approximately 21 studies have examined associations between literacy and anxiety and/or depressive symptoms in children (k = 13), adolescents (k = 7), and older adults (k = 1).
Twelve studies have evaluated associations between literacy and anxiety in samples of children. Five of these studies have reported clear associations between literacy and anxiety (Barber et al., 2021; Grills et al., 2023; McArthur et al., 2021; Robidoux et al., 2024; Wang, 2021) while one did not (Li et al., 2024). More specific associations have been reported between literacy and reading anxiety (Fishstrom et al., 2024; Macdonald et al., 2021), general anxiety (Kargiotidis & Manolitsis, 2024; Macdonald et al., 2021), social anxiety (Francis et al., 2022; Kargiotidis & Manolitsis, 2024), somatic complaints and physical symptoms (Aro et al., 2022; Barnes et al., 2024), separation anxiety (Grills et al., 2023), and harm avoidance (Barnes et al., 2024; Grills et al., 2023). Just five of these studies with children evaluated associations between literacy and depressive symptoms – four of which found associations between literacy outcomes and depressive symptoms (Grills et al., 2023; Li et al., 2024; McArthur et al., 2021; Wang, 2021) while one did not (Robidoux et al., 2024). However, the small number of studies measuring depressive symptoms in child samples highlights the need for more research in this area.
Most studies evaluating associations between literacy and anxiety and/or depression in adolescents have included merged samples of children and adolescents (Boyes et al., 2020; Cristofani et al., 2023; Hossain et al., 2021; Ihbour et al., 2021; Lievore et al., 2024) or adolescents and young adults (Basta et al., 2022), making it difficult to interpret the true nature of the association between literacy and mental health for adolescents specifically. Just one study has evaluated associations between literacy and anxiety and depression with an adolescent sample, comparing symptoms between primary and secondary school students with developmental dyslexia to controls (Giovagnoli et al., 2020). The study found that adolescents with dyslexia had an increased level of anxiety, depression, and somatic symptoms compared with controls. The lack of studies evaluating associations between literacy and depressive symptoms for adolescents is again noted as an area of future research.
To the best of our knowledge, just one study has evaluated the association between reading difficulties and affective symptoms (e.g., depressive symptoms) in older adults. John and colleagues (2021) conducted an evaluation of longitudinal associations using data from the National Survey of Health and Development (British 1946 birth cohort) between reading (assessed using a reading accuracy test with a cut-off of 1.5 SD) in childhood and affective symptoms (assessed using standardised questionnaires) from adolescence (13 and 15 years of age) to early old age (69 years of age). The sample included 5362 men and women who were followed up 24 times, with the most recent data collected in 2015 when participants were of age 69. Results showed that reading problems in childhood (age 11) were significantly associated with higher affective symptoms in adolescence, but not in adulthood (ages 36, 43, 53, 60–64, and 69), adjusting for sex, education, externalising behaviour, and socioeconomic status. These findings were interpreted to suggest that the association between reading problems and affective symptoms do not persist into adulthood. However, this study did not explore associations between literacy and anxiety and does not shed light on the specific type of anxiety symptoms that may be linked with literacy difficulties. Thus, further research is needed to understand how literacy difficulties are associated with different types of anxiety.
The Current Study
Much is already known about the link between literacy difficulties and anxiety in children (Fishstrom et al., 2024; Francis, Hudson et al., 2022; Kargiotidis & Manolitsis, 2024; Polychroni et al., 2024). Far less research has examined these associations in adolescents and older adults, and even fewer studies have investigated the association between literacy and depressive symptoms at any age (John et al., 2021). This gap highlights the need to explore associations between literacy and mental health across different age groups, and particularly with older adults, who have mostly been ignored in the literature.
John et al.’s (2021) results suggest that the associations between literacy and mental health may change across the lifespan. In primary school, there is an intense focus on developing foundation literacy skills (especially up to grade 3). In secondary school, literacy is used to access the curriculum and students face increasing scrutiny through grades, rankings, and assessment pressures. Adolescence is also a period of intense self-focused attention and self-esteem development, suggesting that the link between literacy and anxiety may be as strong – or stronger – than in childhood.
Evidence for older adults remains limited, despite the practical importance of understanding and supporting ageing populations. Some emerging evidence suggests that literacy-related activities in older adulthood may reduce stress and anxiety, enhance social connectedness (Currie et al., 2025), and slow cognitive decline (Stine-Morrow et al., 2022). This points to literacy as a potentially modifiable protective factor in later life, which could be integrated into existing theoretical models such as cumulative risk and resilience framework (Catts & Petscher, 2022), cognitive reserve theory, and the scaffolding theory of ageing and cognition (Oosterhuis et al., 2023).
The aim of the present study is to examine the associations between reported literacy (e.g., reading and spelling skills) and mental health (e.g., anxiety and depressive symptoms) in children, adolescents, and older adults to better understand the strength of these associations for different age groups. Specifically, we hypothesise moderate and significant associations between literacy and anxiety (particularly reading anxiety and social anxiety) for children, adolescents, and older adults. This hypothesis is based on research with children and young people (Fishstrom et al., 2024; Francis, Hudson et al., 2022; Kargiotidis & Manolitsis, 2024; Macdonald et al., 2021), and we hypothesise that the relationship is maintained across the lifespan into older adulthood. We also predict significant and weak associations between literacy and depressive symptoms for children (Grills et al., 2023; Li et al., 2024; McArthur et al., 2021; Wang, 2021), adolescents (Giovagnoli et al., 2020), and older adults (John et al., 2021). Finally, we plan to evaluate if associations between literacy and anxiety show the same patterns for different
The unique contribution of this study is its lifespan perspective on the associations between literacy and mental health. Whereas prior research has largely focused on children, with only scattered investigations in adolescents and older adults, our study directly compares these three age groups within the same framework. By examining both anxiety and depressive symptoms, and by differentiating between types of anxiety (e.g., reading anxiety, social anxiety), this study extends existing models of literacy and well-being beyond childhood. In doing so, it provides new evidence on whether associations between literacy difficulties and mental health are developmentally stable or vary across the lifespan, offering insights that can inform both theoretical models and practical interventions for diverse age groups.
Method
The methods for this study were approved by the Macquarie University Human Ethics Committee (Reference: 52019587712546, 52021618126362).
Participants
Children were invited to participate in this study if they attended primary school (N = 478). The sample ranged between 4.9 and 12.9 years of age (Mage = 10.1, SDage = 1.9 years) and 31.9% of the sample identified as female, 67.7% identified as male, and 0.4% identified as other. Of this sample, 425 children spoke English as a first language, and 11 children spoke English as a second language. Language status was unknown for 19 children. Familial cultural identity included Aboriginal and Torres Strait Islander (N = 21), Australian/New Zealander (N = 157), other (N = 105) or unknown (N = 169). Parents were asked to report if their child experienced literacy difficulties. In terms of self-reported literacy, three questions assessed whether a child struggled with literacy (two parent-report and one child-report question). If the answer was “yes” to any of these questions, then the child was deemed to have struggled with literacy. In terms of literacy support, one parent and one child report question asked about literacy support. If the answer was “yes” to either question, then the child was deemed to have received support. In summary, 7% of children struggled with literacy, 16% reported receiving additional literacy support, 68% reported no literacy difficulties, and there were 9% children for whom responses were unclear (neither parent nor child replied “yes” to any items, and replied “I don’t know” to some items).
Adolescents were invited to participate if they attended high school (N = 438). The sample ranged between 13 and 18.9 years of age (Mage = 15.6, SDage = 1.7 years) and 52.9% identified as female, 45.1% identified as male, and 1.9% identified as non-binary or other. Adolescents spoke English as a first language (N = 385), English as a second language (ESL; N = 4), or not reported (N = 23). Familial cultural identity included Aboriginal or Torres Strait Islander (N = 23), Australian/New Zealander (N = 125), other (N = 75) or unknown (N = 189). In terms of literacy, 5% reported literacy difficulties, 14% received literacy support, 74% had no literacy difficulties, and 7% of adolescent’s literacy level was unknown.
The data for the children and adolescents included in this study were collected as part of a larger study evaluating the reliability and validity of the Reading Anxiety Test (Francis al., 2023a, 2023b, 2023c, 2023d), and of the associations between reading anxiety and other emotional and behavioural symptoms (Jones et al., 2025).
Older adults were recruited through the Older Adult Database of Research Volunteers at Macquarie University (N = 111) and were age between 60 and 86 years (Mage = 68.5, SDage = 6.0). Eligibility criteria included the reported age range and the ability to complete a 30-min survey (with or without assistance) on reading ability, habits and attitudes, and emotional well-being. A total of 116 participants provided consent, but five participants were excluded due to incomplete data. Participants identified as 85.6% female and 14.4% male. In terms of demographics, the vast majority were native English speakers from Australia: 68.5% spoke English as a first language (9.9% ESL; rest missing), and 81.1% identified as Australian/New Zealander (1% Aboriginal Torres Strait Islander, 17.1% Other; 1% missing). In terms of literacy, 2% of the sample reported “quite a bit” of difficulty with literacy as a child, 4% reported receiving help for literacy from a parent, teacher, friend, or sibling, and 7% reported a family history of literacy difficulties. The remainder of the sample did not receive literacy assistance, did not indicate a family history of literacy difficulties, and did not report “quite a bit of difficulty” with literacy.
Procedure
Children and Adolescents
Data was collected via LimeSurvey – an online survey platform. Data were collected from parents only for children ages 4 to 6 years given that they were too young to complete self-report measures. Parent and self-report measures (described below) were administered to the remainder of the sample. Children and adolescents were recruited from two independent schools (Grades 3–10), the community, an online panel provider (Cint), and an anxiety clinic. For the school sample, principals were contacted by the researchers and after agreeing to participate, parents were sent information about the study with opt-out consent forms. The community and panel groups were recruited via online advertisements. Children seeking anxiety treatment and their parents were invited to participate during a clinical assessment. Researchers were available to assist children and adolescents to complete the measures if needed (for the school and clinic samples) – 28.3% of participants requested help for technical issues (3.5%), reading questions (8.5%), and understanding questions (75%). Participants were entered into a draw to win an iPad valued at $529.
Older Adults
Participants responded to study advertisements to complete the online questionnaire. Data were collected via the Qualtrics survey platform where participants were invited to complete an online survey (approximately 1 hr) via a web-link that could be accessed on their own personal device of their choosing. Participants were invited to contact the research team for assistance completing and reading questions if required; however, none of the participants sought assistance.
Measures
Literacy Ability
Literacy ability for children, adolescents, and older adults was assessed using items from the Adult Reading History Questionnaire-Revised (ARHQ-R; Parrila et al., 2003). The ARHQ-R has been used to determine the presence of a significant history of literacy difficulties and comprises 10 questions about an individual’s literacy and educational experiences – and was selected for this study given the convenience of testing large samples and the ability to capture lifetime reading experiences. Each item receives a score from 0 to 4, and raw scores are tallied to a total score ranging from 0 to 28, with high scores indicating greater literacy difficulty. Research has shown that the ARHQ-R has high internal consistency in university student samples when differentiating students with and without a history of literacy problems (α = .90; Parrila et al., 2007), and that students who report high scores are significantly less accurate and slower readers (Deacon et al., 2012) and spellers (Kemp et al., 2009) than students who report low scores. Seven questions were selected and worded appropriately for children, adolescents, and older adults (see Table 1 for the reworded items). In the present sample, the internal consistency was acceptable (α = .80–.88).
Adult Reading History Questionnaire-Revised Questions Selected and Modified for Children, Adolescents, and Older Adults.

Anxiety and Depressive Symptoms
Children and Adolescents
Children, adolescents, and/or their parents completed the Revised Child Anxiety and Depression Scales-Child and Parent short versions (RCADS-C-25/RCADS-P-25; Ebesutani et al., 2017), which includes 25 statements that relate to five anxiety domains (e.g., generalised, social, separation, panic, obsessive-compulsive symptoms) and depressive symptoms. Although the measure includes obsessive-compulsive symptoms among its anxiety domains, it is important to note that in the DSM-5, obsessive-compulsive disorder is categorised separately from anxiety disorders. Participants read each item and recorded how often they experienced each symptom using a 4-point Likert scale with anchors (never = 0, sometimes = 1, often = 2, always = 3). Item scores for anxiety and depressive symptoms were summed separately to produce an anxiety raw score and a depressive symptom raw score as per the normative sample. The RCADS-C-25 anxiety and depressive scales have acceptable reliability in clinic and school samples (anxiety: α = .94–.96; depression: α = .79–.80; Ebesutani et al., 2012). In the present sample, the internal consistency was acceptable for depressive scales (α = .87–.94) and anxiety scales (α = .63–.86).
Older Adults
Participants completed the Brief Fear of Negative Evaluation Scale (BFNE; Leary, 1983), which includes 12 items that assess social anxiety (e.g., “I am afraid that people will find fault with me”). Four items are reverse scored (e.g., “other people’s opinions of me do not bother me”). Participants read each item and select the response that best describes their symptoms (0 = not at all, 1 = slightly, 2 = moderately, 3 = very, 4 = extremely). The responses are tallied out of a total of 48 (M = 35.7, SD = 8.10; Leary, 1983), with high scores indicating greater social anxiety. The inter-item reliability of the BFNE is high and consistent with the original version (α = .90–.92; Leary, 1983). In the present sample, the internal consistency was acceptable (α = .88).
Older adults also completed the Generalised Anxiety Disorder 2-item (GAD-2; Kroenke et al., 2007) to assess generalised anxiety (i.e., “feeling nervous, anxious, or on edge” and “not being able to stop or control worrying”). Participants read each item and indicated how often the symptoms occurred in the last 2 weeks. Participants respond on a 4-point scale (0 = not at all, 1 = several days, 2 = more than half the days, 3 = nearly every day). The GAD-2 total score is calculated by adding the score for each question. A score of 3 or greater indicates possible concerns with generalised anxiety. Research suggests that this cut-off score has a sensitivity of 86% and specificity of 83% for the diagnosis of generalised anxiety disorder (Kroenke et al., 2007). In the present sample, the internal consistency was acceptable (α = .78).
Older adults completed the Patient Health Questionnaire-2 (PHQ-2; Kroenke et al., 2003) to measure depressive symptoms in older adults. The PHQ-2 comprises two items about the degree to which an individual has experienced depressive symptoms over the past 2 weeks. Participants read each item and indicate the frequency of symptoms (0 = not at all to 3 = nearly every day). In reference to a structured clinical interview, the PHQ-2 had 87% sensitivity and 78% for major depressive disorder, and 79% sensitivity and 86% specificity for any depressive disorder (Löwe et al., 2005). In the present sample, the internal consistency was acceptable (α = .84).
Reading Anxiety
Reading anxiety was assessed using the Reading Anxiety Test (RAT; Francis et al., 2023a, 2023b, 2023c, 2023d). We selected this additional measure of anxiety given that the previous anxiety measures do not assess for anxiety related to literacy, and it is possible that there is a close association between literacy and anxiety reading anxiety than other types of anxiety symptoms and disorders (Francis, Hudson et al., 2022).
Children and Adolescents
The RAT comprises 21 items reworded appropriately for the respondent–children, adolescents, and parents completed the relevant version (RAT-C for children; Francis et al., 2023a; RAT-Ad for adolescents; Francis et al., 2023b; RAT-C/P for parents of children; Francis et al., 2023c; RAT-Ad/P for parents of adolescents; Francis et al., 2023d). The RAT comprises three subscales: social reading anxiety (e.g., reading aloud in front of the class), generalised reading anxiety (e.g., worry about being a poor reader), and physical symptoms of reading anxiety (e.g., feeling shaky when reading). Participants select the most relevant response (0 = never, 1 = sometimes, 2 = often, 3 = always), raw scores are tallied (0–63), and higher scores indicate greater reading anxiety. The 84th percentile is a cut-off to indicate elevated reading anxiety. The RAT has good internal consistency (Cronbach’s α = .96–.97) and convergent validity with the existing anxiety questionnaires (r = .59–.60; Jones et al., 2025). In the present sample, the internal consistency was acceptable (α = .96–.97).
Older Adults
Older adults completed the RAT-Older Adult (RAT-OA) questionnaire that was adapted from the RAT-Adult questionnaire (Francis, Soares et al., 2022) for the purpose of this study. The RAT-OA comprises 15 items that assess anxiety related to daily literacy tasks (e.g., I worry that I’ll make a mistake paying bills/writing emails/letters because of my reading). Participants select the response that best describes their reading anxiety (0 = never, 1 = sometimes, 2 = often, 3 = always), raw scores are tallied (0–45), and higher scores indicate greater reading anxiety. While the RAT has been administered to 169 university students ages 18 to 57 years (Soares et al., 2023), they do not provide relevant normative data for our current sample of older adults (age >65 years). In the present sample, the internal consistency was acceptable (α = .97).
Data Analysis
Partial correlational analyses were used to examine the strength of the associations between literacy and type of anxiety and depressive symptoms in children, adolescents, and older adults, whilst controlling for age and sex. The partial correlations between literacy and anxiety and depressive symptoms for children, adolescents, and older adults, controlling for age and sex, are reported in Table 3. Given the large number of correlations undertaken here, we report significance based on unadjusted p-values (*≤.05, **<.01, ***<.001) but focus our conclusions and discussion on correlations that exceeded .30 in magnitude and with p-values less than .001 (which would remain significant after Holm-Bonferroni corrections).
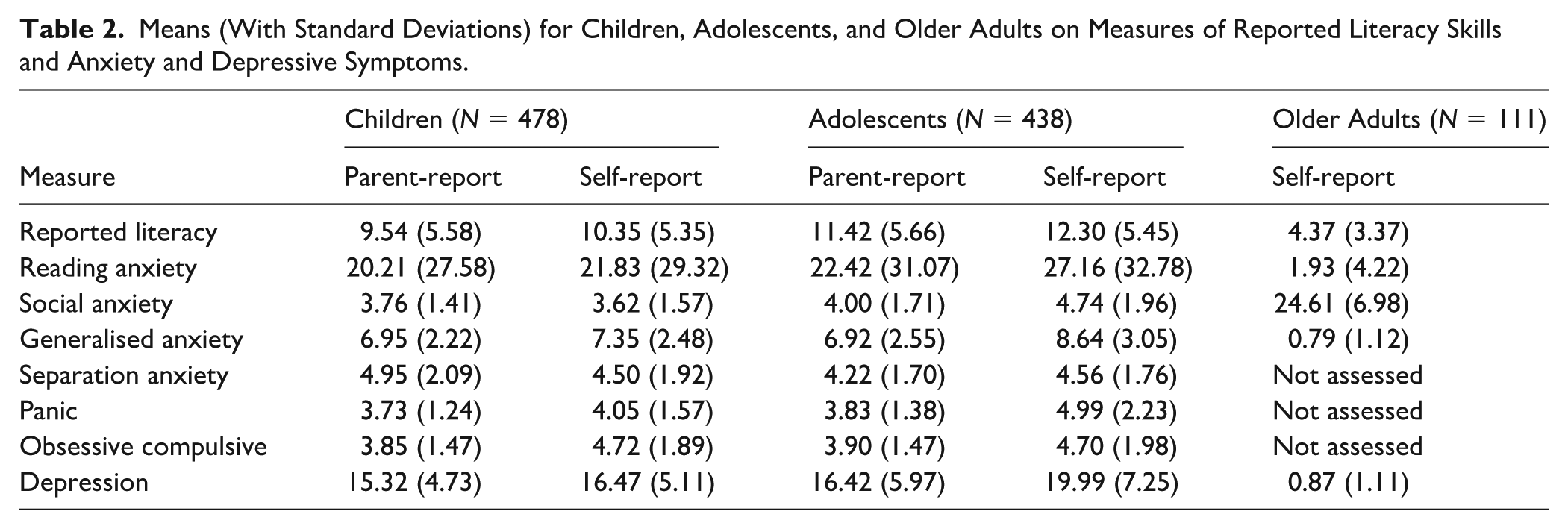
Fisher’s z transformation was used to test for differences among the correlations across age groups – children, adolescents, and older adults. The strength of the association is interpreted as weak (r = .1–.29), moderate (r = .3–.49), and strong (r = .5–1.0; Cohen, 1988). For children and adolescents, many scales were collected either from the children themselves, their parents, or, in some cases, both. We report data for children and parents separately. The older adult data includes responses from older adults themselves. Means and standard deviations for children, adolescents, and older adults’ responses for literacy, anxiety and depressive symptom measures are reported in Table 2.
Means (With Standard Deviations) for Children, Adolescents, and Older Adults on Measures of Reported Literacy Skills and Anxiety and Depressive Symptoms.
Results
Partial Correlations
The results showed significant and moderate-to-strong correlations between literacy and reading anxiety (r = .36–.61) for children (parent and self-report), adolescents (parent and self-report), and older adults. Moderate and significant associations were also observed between literacy and social anxiety for children (self-report; r = .33) and older adults (r = .32). For depressive symptoms, a moderate and significant association was found in children (parent-report; r = .31). Children’s self-report (r = .27) and adolescents’ parent- and self-reports (r =.27 and .20, respectively) showed weaker but significant correlations with literacy. In contrast, the correlation with depressive symptoms in older adults was weak (r = .16) and nonsignificant, consistent with limited statistical power in this subsample (see Tables 3 and 4 for correlations and significance values).
Partial Correlations (With Sample Sizes) Between Literacy and Anxiety and Depressive Symptoms for Children, Adolescents, and Older Adults, Controlling for Gender (All Groups) and Age (Children and Adolescents).
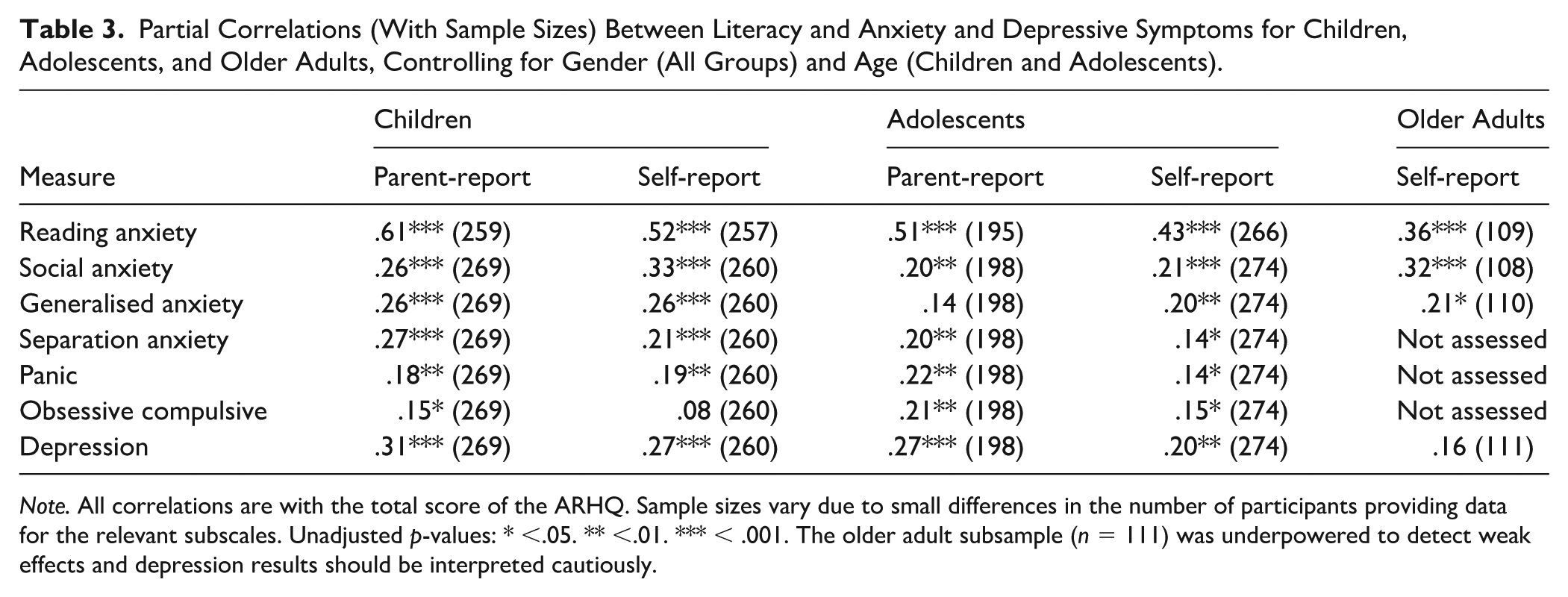
Note. All correlations are with the total score of the ARHQ. Sample sizes vary due to small differences in the number of participants providing data for the relevant subscales. Unadjusted p-values: * <.05. ** <.01. *** < .001. The older adult subsample (n = 111) was underpowered to detect weak effects and depression results should be interpreted cautiously.
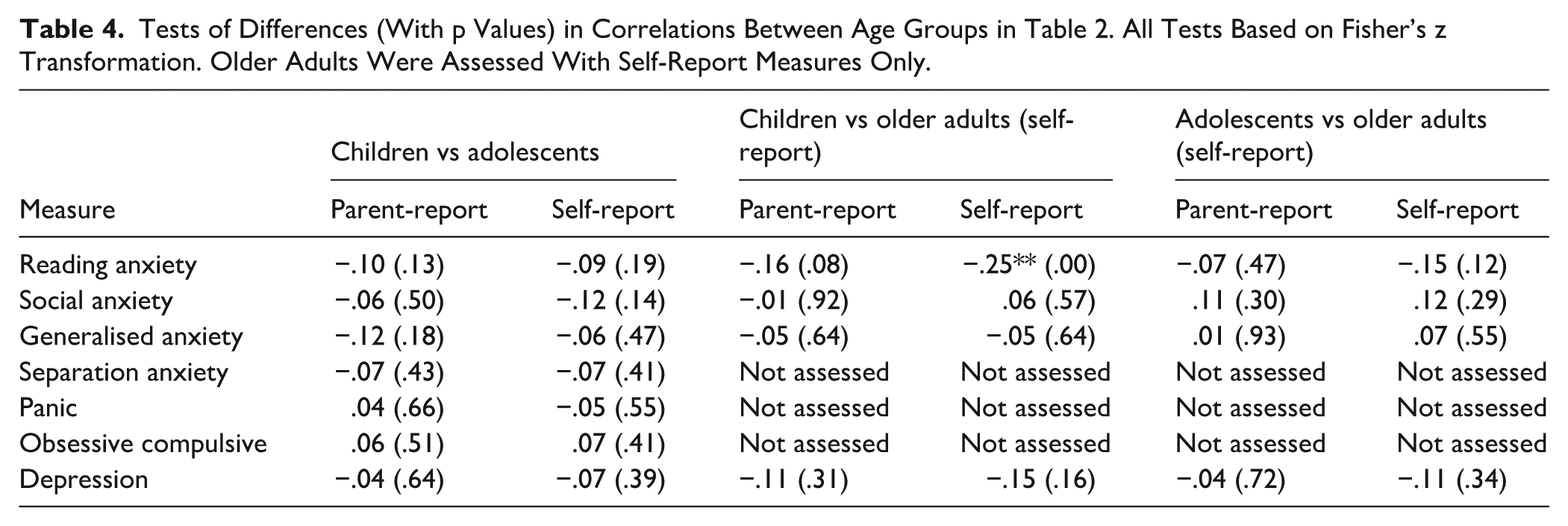
Tests of Differences (With p Values) in Correlations Between Age Groups in Table 2. All Tests Based on Fisher’s z Transformation. Older Adults Were Assessed With Self-Report Measures Only.
Group Comparisons
Partial correlations and Fisher’s z transformation were used to test differences among the correlations across age groups. There was only one significant difference between the groups (child self-report and older adults), indicating a stronger association between self-reported reading anxiety for children compared with older adults. There were no significant differences between children and adolescents, adolescents and older adults, or children and older adults in the strengths of associations between literacy and anxiety or depressive symptoms. However, given the smaller sample for older adults, these comparisons should be interpreted with caution,
Discussion
The aim of this study was to examine the strength of associations between literacy (e.g., reported reading and spelling skills) and mental health (e.g., anxiety and depressive symptoms) for children, adolescents, and older adults to better understand the strength of the associations for these different age groups. Associations between literacy, anxiety symptoms, and depressive symptoms were evaluated using partial correlational analysis, controlling for age and gender in children, and gender in older adults and associations were compared across age groups. Below, we discuss the results for each hypothesis in turn, followed by a discussion of strengths and limitations, implications, and future research.
Literacy and Anxiety Symptoms in Children, Adolescents, and Older Adults
We predicted moderate and significant associations between literacy and anxiety (particularly reading anxiety and social anxiety) for children, adolescents, and older adults. This hypothesis was based on research with children and young people (Fishstrom et al., 2024; Francis et al., 2022; Kargiotidis & Manolitsis, 2024; Macdonald et al., 2021). We found partial support for this hypothesis. The results showed moderate-to-strong and significant associations between literacy and reading anxiety symptoms for children (parent and child report) and adolescents (parent-report), and moderate and significant associations between literacy and reading anxiety symptoms for adolescents (self-report) and older adults. The results also showed moderate and significant associations between literacy and social anxiety for children (self-report) and older adults, but not for adolescents (self or parent There were no significant moderate-to-strong associations between literacy and generalised anxiety, separation anxiety, panic, or obsessive-compulsive symptoms for children, adolescents, or older adults.
These findings are consistent with previous studies that have reported associations between literacy and reading anxiety (Fishstrom et al., 2024; Macdonald et al., 2021) and social anxiety (Francis et al., 2022; Kargiotidis & Manolitsis, 2024) and highlight that a clear social performance element of literacy tasks is relevant across the lifespan. This is particularly true for children and older adults, highlighting that at least some parts of anxiety related to literacy are due to concerns about negative evaluation from other people.
Comparison of the size of correlations for children, adolescents, and older adults revealed just one significant difference – with a significantly stronger child-reported literacy-reading anxiety association compared with older adults. A similar group difference was observed when the same correlation was calculated using parent-report versus child-report, but this did not reach significance. These results suggest that there may be a stronger association between literacy and anxiety symptoms for children, possibly due to the intensity and focus on literacy instruction during this period. However, the results do not suggest any clear differences in the strength of associations between literacy and other types of anxiety symptoms for these three groups. In addition, given the smaller sample size for older adults, these findings should be interpreted cautiously, as weak associations may not have been detectable in this group. Thus, while the pattern of results is broadly consistent across age groups, the evidence for older adults should be considered preliminary.
Given the clear persistence of an association between literacy difficulties and anxiety and depressive symptoms across the lifespan, it is important to consider the lifelong implications of literacy difficulties. Consistent with the existing causal WiL model (e.g., literacy difficulties → negative self-concept → reduced engagement in literacy activities → further exacerbation of literacy difficulties; McArthur, 2022), it is likely that the repeated failure related to literacy difficulties that is experienced during the formative primary school years leads to the development of a negative self-concept that, once established, is difficult to modify and contributes to ongoing difficulties with mental health and literacy that persist well into adulthood. These findings also align with the cumulative risk model (e.g., Catts & Petscher, 2022), which posits that the accumulation of multiple risk factors – such as early academic struggles, low self-efficacy, and emotional distress – can compound over time to increase vulnerability to adverse outcomes. While these models offer a framework to understand the findings, it is essential to acknowledge that the cross-sectional nature of the data limits causal inference. Alternative explanations, such as anxiety contributing to reduced literacy engagement or the co-occurrence of third variables, are also plausible. These results nevertheless underscore the importance of implementing treatment programmes that target both anxiety symptoms and literacy skills to reduce the risk of long-term psychological difficulties associated with struggling literacy skills. In addition, while the concept of “reading anxiety” is clearly related to literacy, it is important to evaluate other aspects of anxiety that frequently co-occur with literacy difficulties (e.g., social and generalised anxiety) to inform treatment planning and provide adequate support for those experiencing literacy difficulties and anxiety, as well as report the correlation between reading anxiety and other types of anxiety symptoms evaluated.
Literacy and Depressive Symptoms in Children, Adolescents, and Older Adults
We predicted significant associations between literacy and depressive symptoms for children (Grills et al., 2023; Li et al., 2024; McArthur et al., 2021; Wang, 2021), adolescents (Giovagnoli et al., 2020), and older adults (John et al., 2021). There was partial support for this hypothesis. The results showed a significant and moderate association between literacy and parent-reported depressive symptoms for children, with significant yet weak associations for self-reported child depressive symptoms, and parent and self-reported adolescent depressive symptoms. The association between literacy and depressive symptoms for older adults was nonsignificant, consistent with limited statistical power in this subsample. As such, we interpret the older adult findings as inconclusive.
These are important findings and highlight that there is indeed an association between literacy and depressive symptoms – particularly for children. These results are consistent with the few studies that have clearly assessed for depressive symptoms in samples of children with literacy difficulties (e.g., Grills et al., 2023; Li et al., 2024; McArthur et al., 2021; Wang, 2021). Depressive symptoms commonly occur and present in childhood, but many studies fail to assess for these symptoms or rely on parent report only that may miss many children who experience these symptoms. Thus, these results clearly show that there is an association between literacy and depressive symptoms for children, highlighting that treatment targeting depressive symptoms (in addition to anxiety) is also needed to support those struggling with literacy. Incorporating depressive symptoms into intervention planning is important, as depression may reduce motivation, self-efficacy, and cognitive engagement – factors that can hinder participation in literacy activities and negatively impact academic progress over time.
Overall, the results underscore the importance of considering both anxiety and depression in relation to literacy difficulties, but also highlight the need for future research with larger, more representative samples of older adults to clarify whether these associations persist into later life.
Limitations and Future Directions
The results from this study should be interpreted alongside the study strengths and limitations. First, this is a cross-sectional correlational study that examined the strength of associations between literacy and anxiety and depressive symptoms in children, adolescents, and older adults. The cross-sectional nature of this data precludes claims about the developmental trajectory of anxiety and depressive symptoms. It remains unclear whether literacy difficulties contribute to later anxiety and depression, whether anxiety and depression reduce literacy engagement, or whether both are influenced by shared risk factors. Longitudinal research is needed to evaluate the temporal ordering of these relationships, evaluate bidirectional effects, and track how associations evolve across the lifespan. Such studies would be particularly valuable for establishing causal links between literacy and later mental health outcomes (McArthur et al., 2021).
It is also important to acknowledge that only a small proportion (although, similar to the prevalence of literacy difficulties in the general population) of our sample struggled with literacy as indicated on the self-report questionnaire. Approximately 22% of children, 18% of adolescents, and 14% of older adults reported a history of literacy difficulties or required support. Despite comprising a relatively small percentage of the sample, it is unclear whether their self-reported literacy difficulties limited their capacity to complete the questionnaires in some way. We can be confident that it did not pose too much of a barrier, given that (a) all items were completed, (b) assistance was provided to children and adolescents who asked for help, and (c) the researchers did not receive any requests for assistance from older adults. However, future studies should continue to acknowledge the limits of literacy difficulties and provide support to young people and their parents to complete study tasks that involve reading and spelling or writing. Future studies should also explore accessibility features, such as text-to-speech, to afford those struggling with literacy the ability to participate in research.
Another consideration of the current study is the reliance on self-reported literacy difficulties using the ARHQ-R (Parrila et al., 2007) rather than using a standardised assessment of literacy. While the ARHQ-R was selected for its practicality in assessing large samples and has demonstrated strong discriminative validity across literacy levels (Deacon et al., 2012; Kemp et al., 2009), it remains a self-report instrument and is therefore susceptible to response biases. In particular, individuals with elevated anxiety may underestimate their literacy ability due to negative self-appraisal tendencies (Cole et al., 1999), which could inflate observed associations between anxiety and perceived literacy difficulties. Thus, the measure may capture a blend of actual ability and subjective attitudes towards reading. This limitation highlights the need for future research that combines standardised assessments of literacy (e.g., reading accuracy or fluency tests) with self-report measures to disentangle ability from perception and provide a more comprehensive evaluation across developmental stages. Finally, the ARHQ-R items were reworded for the current study compared with prior reliability studies, underscoring the importance of further validation work.
The next limitation relates to the questionnaires that were used to measure anxiety and depressive symptoms – and the fact that we measured symptoms rather than clinical levels or anxiety and depression disorders. The gold standard approach requires that multi-informant responses are obtained (i.e., from the young person, parent, and/or teacher). In the current study, the person completing the questionnaires varied across the child and adolescent groups. While most children had parent-report data and most adolescents had self-report data, there were few complete “sets” of self- and parent- report data. It is critical that studies continue to assess anxiety and depressive symptoms in children, adolescents, and adults with literacy difficulties and ensure to capture responses from both the young person and parents for children and adolescents. It would also be worthwhile to capture responses from teachers (for children and adolescence) in the future to better understand the anxiety and depressive symptoms that may be observable in the school environment, as well as assess for clinical levels of anxiety and depression in these samples.
We also acknowledge the relatively small sample of older adults (n = 111), which limits the statistical power and raises questions about the representativeness of this group. This means that reliance on statistical significance will lead to a bias towards finding associations in children and adolescents and failing to find associations in older adults. Power analyses indicate that this sample size is sufficient to detect moderate correlations with 80% power at α = .05, but underpowered to detect weak correlations. Accordingly, findings for older adults are interpreted cautiously, and analyses of depressive symptoms were not emphasised given limited statistical power. This approach ensures that the analyses are robust when adequately powered, while acknowledging the need for future research with larger and more representative samples of older adults. Despite these limitations, the inclusion of older adults provides rare and valuable insight into literacy-mental health associations later in life, offering an important foundation for future research.
A final limitation of this study is that we did not recruit participants between the ages of 19 and 59 – limiting our understanding of the association between literacy and anxiety and depressive symptoms for this cohort of adults. This represents a broadly general limitation across the field: previous studies evaluating associations between literacy and anxiety and depressive symptoms have largely focused on children or mixed samples of children and adolescents. Thus, more research is needed to understand these associations across a broader range of ages to better understand these associations across different age groups.
Clinical Implications and Future Directions
There are moderate-to-strong and significant associations between literacy and reading anxiety symptoms for children, adolescents, and older adults, as well as moderate and significant associations between literacy and social anxiety (self-reported) and depressive symptoms (parent-reported) for children. These results suggest that children, adolescents, and older adults may experience difficulties with anxiety (reading anxiety, social anxiety) and depressive symptoms, highlighting the importance of assessing for these common mental health problems for individuals struggling with literacy. For example, if a child or adolescent is struggling with literacy (at school or seeking additional support) then administering questionnaires such as the RAT (Francis et al., 2023a, 2023b, 2023c, 2023d) and RCADS (Ebesutani et al., 2017) would be helpful to determine if they are experiencing elevated levels of anxiety and/or depressive symptoms that warrant further assessment and intervention. If so, then they should be referred to a psychologist for cognitive behavioural therapy that is modified to their needs (e.g., reducing the reading and writing demands from the therapy), or referred to a suitably tailored programme (e.g., Francis et al., 2021).
For the first time, this study has established an association between literacy and reading anxiety for adolescents and older adults. Adolescence is a period of complex development, and it is possible that the association between literacy and reading anxiety interacts with other factors – beyond those specified in the current model (McArthur, 2022) - that impact the developmental trajectory of difficulties into adulthood. Similarly, we also need to understand how this association presents and how to support older adults. Future research is needed to understand what type of intervention is needed (i.e., literacy and mental health intervention tailored to children with reading difficulties; Francis et al., 2021) and when this intervention is most effective (i.e., childhood) to better support individuals struggling with literacy and their mental health.
Conclusion
In sum, the goal of this study was to investigate the association between literacy and anxiety and depressive symptoms in samples of children, adolescents, and older adults. The results showed significant and moderate-to-strong correlations between literacy and reading anxiety for children (parent and self-report), adolescents (parent and self-report), and older adults. There were moderate and significant associations between literacy and social anxiety for children (self-report) and older adults, but not adolescents. There were moderate and significant associations between literacy and depressive symptoms for children (self-report). Based on age-group comparisons rather than longitudinal tracking, these results highlight that associations between literacy and anxiety symptoms persist across childhood, adolescents, and older adulthood – particularly for reading and social anxiety symptoms. The results also show that there is a clear association between literacy and depressive symptoms in childhood. This study adds to a limited body of research on literacy and reading anxiety, and for the first time, provides insight to the association in adolescence and older adults. By understanding the co-occurrence of these problems, we can better understand the complex nature of literacy, and anxiety and depressive symptoms to create pathways for care and support.
Footnotes
Ethical Considerations
This research was approved by Macquarie University HREC.
Funding
This research was supported by ARC DP200102241.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data that support the findings of this study are available from the corresponding author upon reasonable request.