
Abstract
United Nations Security Council Resolution 1325 highlights the distinct needs of women in security and well-being. Few studies explore how peacekeeping affects women’s access to health and education. Yet, women’s access to public services such as health is a form of gender inequality in post-conflict countries leading to unbalanced distribution of resources. We argue that peacekeeping operations (PKOs) have both a direct and an important indirect impact on maternal health and women’s well-being. First, peacekeeping can have a direct effect by providing medical and training facilities. Second, peacekeeping has an indirect effect as improvement in the overall level of security facilitates women’s access to medical services and education. We evaluate our argument by combining evidence from different levels of analysis. First, we use a difference-in-difference analysis of 45 African countries with data between 1990 and 2013, comparing the changes in maternal mortality rates (MMR) for countries with and without PKOs. Second, we look at within-country variations across areas with and without UN peacekeeping deployment in three countries with integrative PKOs, combining geo-coded peacekeeping data with individual data on maternal health and education from the Demographic and Health Surveys (DHS) in the Democratic Republic of Congo, Côte D’Ivoire, and Liberia. We find strong empirical support for a positive relationship between peacekeeping presence and maternal health outcomes and access to services.
Introduction
UN peacekeeping missions (PKOs) often have mandates that extend beyond short-term security objectives, aiming at peacebuilding and social transformation. Complex and ambitious UN peacekeeping missions often raise questions about ‘whose peace’ is to be established, and the distributional consequences for vulnerable groups such as women.
Existing research offers two different understandings of gender equality. Some normative approaches emphasize how a more balanced distribution of resources between men and women is fair and just. Others see gender inequality as an indicator of social capacity, where less female disadvantage relative to men reflects higher human and social capital and a more equitable distribution of resources (Forsberg & Olsson, 2016). For instance, recent studies suggest that improving female political representation increases the durability and quality of post-conflict peace (Demeritt, Nichols & Kelly, 2014; Shair-Rosenfield & Wood, 2017).
Women’s access to public services such as health and education is a form of gender inequality in post-conflict countries, since adverse conditions often affect women more than men (Liebling-Kalifani & Baker, 2010). 1 We argue that UN PKOs have both a direct and an important indirect impact on maternal health and women’s well-being. The indirect impact implies that PKOs can create a ‘peacekeeping dividend’ through improving security. A signal that fighting has subsided allows for improved infrastructure such as medical facilities and schools, safer access to medical facilities and other services such as schools.
We evaluate our argument using evidence from different levels of analysis. First, we use a difference-in-difference analysis to compare changes in maternal mortality rates (MMR) across 45 African countries with and without PKOs. Second, we look at within-country variations across areas with and without UN peacekeeping deployment in three countries with integrative PKOs – the Democratic Republic of Congo, Côte D’Ivoire, and Liberia – combining geo-coded peacekeeping data with individual data on maternal health and education from the Demographic and Health Surveys (DHS). We find that countries with UN PKOs see much higher improvement in MMR, while women in locations where peacekeepers have been deployed gained improved access to public services.
UN peacekeeping and the quality of peace
Peacekeeping has become the main method to contain civil wars (Fortna, 2008; Howard, 2008). Although some question the effectiveness of peacekeeping missions (Autesserre, 2010; Barnett, Fang & Zürcher, 2014; Beber et al., 2017; Pouligny, 2006), other studies suggest that PKOs promote peace and peacebuilding, strengthening the capacity of governments (Doyle & Sambanis, 2000; Dorussen & Gizelis, 2013). Empirical studies on peacekeeping have so far focused more on ‘negative’ peace, or the absence of armed conflict, than ‘positive’ peace including the well-being of civilians (Galtung, 1964). The definition of ‘positive’ peace as ‘the integration of human society’ goes beyond the protection of civilians and highlights the ‘quality’ of peace in post conflict societies. Crucially, the ‘quality’ of peace can have different implications for the well-being of men and women, linked to post-conflict distribution of resources (Barnett, Fang & Zürcher, 2014; Joshi & Wallensteen, 2018; Olsson & Gizelis, 2015; Olsson, 2009).
The persistent high female mortality rate in sub-Saharan Africa is partly attributable to the indirect effects of conflict on the distribution of services such as health and education (Guha-Sapir & D’Aoust, 2010). Conflict undermines maternal health and well-being because of deteriorating health care, higher rates of abortion and pregnancy terminations, shortage of skilled health professionals, greater risks of contracting infections, and more malnutrition during pregnancies and after childbirth. Increased fertility and weakened public health institutions further exacerbate conditions for women (McCarthy & Main, 1992; Ronsmans & Graham, 2006).
The decline in funding for health provision started before the outbreak of wars, as resources were diverted from public services to military expenditures (O’Hare & Southall, 2007). Diseases spread easily through contaminated water and lack of access to clean water, while medical personnel either are killed or flee (Li & Wen, 2005: 473). Health facilities, schools, and roads are often destroyed during conflicts (Plümper & Neumayer, 2006: 729).
Resources redirected towards destructive use leave legacies disrupting the provision of basic services in post-conflict countries. In Liberia, for example, the civil wars in 1989–96 and 1999–2003 killed approximately 250,000 (10% of the population), displaced around a million people, and dismantled the national economy, infrastructure, and a reasonably effective state. After 14 years of civil war, only 51 out of 293 pre-war medical facilities remained functional in 2003 (Kruk, Freedman & Anglin, 2010).
UN PKOS, security, and women’s well-being
External interventions from UN PKOs improve the provision of public services through a more secure environment, an essential component of post-conflict reconstruction. Provision of public services such as health and public education signal the accountability of the government to its citizens and its capacity to provide services and goods (Kruk, Freedman & Anglin, 2010; Southall, 2011; Lee, 2008). We argue that an inadvertent consequence of PKO presence is ‘the peacekeeping dividend’, associated with higher provision of and access to public services. This is especially the case for maternal health where better access to services can expand to reach more people much faster than other public services requiring more infrastructure and a longer planning horizon. The presence of peacekeepers, especially in integrative missions, increases overall security, here defined as absence of violent armed conflict. 2
Recent empirical studies show peacekeepers reduce the length of conflict, leading to fewer civilian and military deaths, and contain conflicts geographically (Hoeffler 2014; Gleditsch & Beardsley, 2015). Containing violence (i.e. ‘negative’ peace) helps generate ‘positive’ or higher ‘quality’ peace. PKOs signal that rebels and government are converging towards an agreement, and demand for peacekeeping by locals helps signal future intentions and better prospects for peace. Peacekeepers are costly for both governments and rebels because they raise the cost of continuing fighting, thus generating a credible signal that peace is achievable (Fortna & Martin, 2009; Ruggeri, Dorussen & Gizelis, 2017a).
Countries that have experienced conflict tend to discourage investment. Signalling that peace prevails indicates to a broader audience that the country is ‘open for business’, encouraging foreign direct investment in areas such as public services (Garriga & Phillips, 2014). The absence of violence also allows resources to be redirected to productive use, such as improving access to medical services, leading to lower maternal mortality and better overall health. The ending of fighting creates space for international organizations and nongovernmental organizations (NGOs) such as the United Nations International Children’s Emergency Fund (UNICEF), the World Health Organization (WHO), Save the Children, and the International Rescue Committee or private partners – for example the Bill & Melinda Gates Foundation, Kiwanis International, Pampers – to sponsor long-term medical programs leading to tangible improvements in human capital and infrastructure. Beyond fostering NGOs and intergovernmental organizations (IGOs) to become active in an area, the containment of conflict allows for synergies between government agencies and external partners. In Liberia, despite the fragility of the post-conflict health care system, international-private partnerships were successful in eradicating maternal and neonatal tetanus (MNT), one of the causes of maternal and neonatal death. The development of such partnerships relies on maintaining ‘negative’ peace and a sense of stability provided by the United Nations Mission in Liberia (UNMIL, 2012).
Another pathway through which UN presence leads to improvements in the provision of at least health is direct – often short-term and quick in terms of planning projects – focusing on emergency provision, support of local medical facilities, and reintroduction of new resources to replenish what was lost during conflict. UN quick impact projects (QIP) have been designed to win the hearts and minds of local populations. QIPs are not meant to be developmental or long-term but rather aim to build confidence in the mission, build on the peace dividend, support and extend the government’s authority, and strengthen ties with local stakeholders (UN DPKO, 2007). The QIPs are tools to fulfil the UN Security Council objective of ‘promoting economic and social rehabilitation and transformation of post-conflict societies’ with an emphasis on projects that target health, sanitation, rehabilitation of water pumps or building latrines (UN Security Council, 2001).
UN missions often establish medical camps to treat local communities, train local communities in hygiene, or provide emergency medical relief in remote communities. 3 As an example of a QIP, a medical camp was set up for three days in Sass Town, Kley District, 37 km outside the capital of Liberia, Monrovia, by the Pakistani contingency in January 2004. Other missions such as the United Nations–African Union Mission in Darfur (UNAMID) have targeted issues such as hygiene, sanitation, women’s empowerment and education using QIPs. In particular, projects that target sanitation, hygiene and women’s empowerment may have a direct impact on maternal and neonatal health.
We can evaluate whether UN missions improve actual health outcomes such as MMR, although separating the relative effects of direct interventions and security provision is hard without more detailed data. Ultimately, both mechanisms can occur simultaneously and are complementary. If UN missions have any impact on health outcomes such as maternal health, we should observe that countries with PKOs should outperform countries without PKOs in reducing MMR.
H1: Countries with peacekeeping missions experience greater improvements in maternal mortality than countries without.
Many studies show significant variation in health outcomes within countries (Luginaah et al., 2016). Research on the deployment of local PKOs suggests that the presence and considerable size of peacekeeping forces can reduce and contain armed conflict within countries (Ruggeri, Dorussen & Gizelis, 2017a). If integrative PKOs improve health outcomes and public services, one might expect to observe an association between localized peacekeeping presence and improvements in indicators of maternal health and well-being.
If PKOs have an indirect impact on the quality of peace and the peacekeeping dividend argument is correct, we may observe improvement across other public services besides health. Other indicators of the accrued ‘benefit’ of peace such as years of schooling should also increase over time in areas where peacekeepers are present. Observed changes in levels of education also allow us to tease out the direct and indirect impact of peacekeeping missions. If, however, peacekeeping missions only have direct impact through the quick impact projects, we should only observe improvements in one sector – that of women’s health.
Moreover, better education is a driver of improved maternal health linked with more frequent use of resources, access to information about fertility control and availability of resources, as well as the ability to follow sound medical advice. The deterioration of women’s education during conflict is one of the key mechanisms through which conflict leads to higher fertility rates and maternal mortality ratios. In areas where women face inequalities, they are less likely to use health services. These effects are compounded in countries and regions that have experienced civil wars (Chamarbagwala & Morán, 2011; Riyami, Afifi & Mabry, 2004).
Thus, at the subnational level we examine if the dividend of integrative PKOs expands antenatal care and education which many argue would lead to long-term overall improvement in maternal health. One advantage of looking at subnational variation is that we look at the same mission per country, keeping mission characteristics such as mandates, leadership, and troop composition constant. Thus, we develop the following two hypotheses on the link between PKO deployment and maternal health and education at the subnational level:
H2: In regions within countries where the UN peacekeepers are deployed, health outcomes for women should improve.
H3: In regions within countries where the UN peacekeepers are deployed, educational outcomes for women should improve.
Empirical analysis
Difference-in-differences (DID) between countries
We first use difference-in-differences (DID) to calculate the effect of peacekeeping presence on maternal mortality ratios at the country-year level. DID compares the average change over time in maternal mortality ratios in the treatment group (countries that had a peacekeeping mission) to the average change in maternal mortality ratios in the control group (countries without peacekeeping operations). DID is not free from biases such as reversion to the mean and other influences of policies. 4 DID is also based on strong assumptions. For example, the parallel trend assumption posits that the average change in the control group represents the counterfactual change in the treatment group if there were no treatment. 5
DID analysis with two time periods
To assess H1, we first look at 45 African countries using maternal mortality ratio (MMR) from the Global Health Observatory (GHO) by the World Health Organization (2014). GHO covers the time period 1990–2013. MMR shows the risk of maternal health relative to the frequency of births. It is included as one of the Millennium Development Goals (MDGs), an indicator of maternal health. Figure 1 shows the MMR for the 45 countries included in the country-level analysis in 1990 and 2013. The main treatment is the presence of peacekeeping forces in a country within the period 1990–2013. The variable takes a value of 1 if there was a peacekeeping operation at some point in the country between 1990 and 2013; and 0 otherwise. In these 45 countries, eight had integrative missions: Angola, Central African Republic, Chad, Côte d’Ivoire, Liberia, Sierra Leone, Democratic Republic of Congo and Burundi at least for a few years during the specified time period (Figure 2(a)). 6 During the same period another six countries had first generation missions: Chad, Rwanda, Namibia, Mozambique, Uganda, Eritrea and Ethiopia (Figure 2(b)). 7
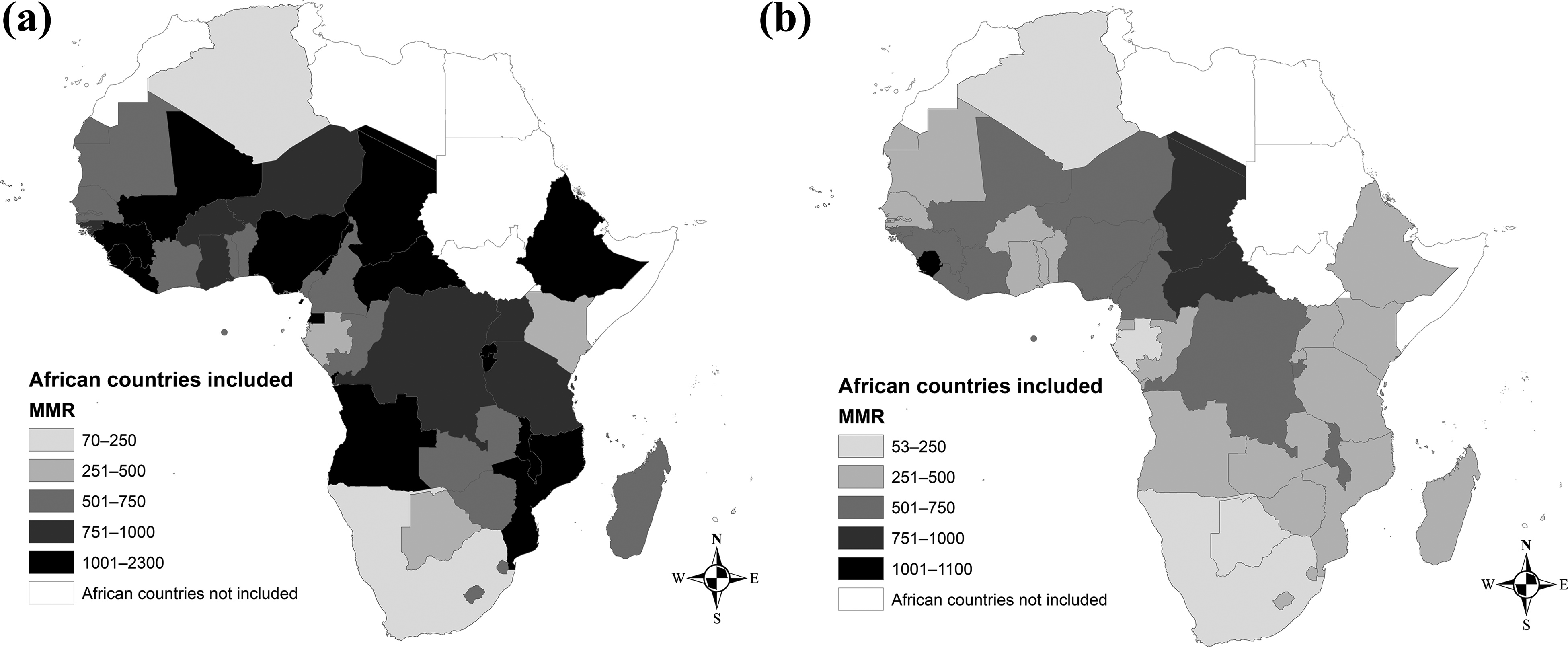
Maternal mortality rates (MMR) in 45 African countries in the DID – (a): 1990, (b): 2013

Integrative and first generation PKOs – (a): integrative PKOs, (b): first generation PKOs
Traditional PKOs aim to monitor a ceasefire or peace agreement and make it more difficult for the parties to return to violence (Fortna, 2008). By contrast, integrative missions combine security, political reform and development concerns to support comprehensive treaty agreements (Dorussen & Gizelis, 2013; Durch et al., 2003; Goulding, 1993; Brahimi, 2000). Traditional PKOs are smaller in size (usually 200–300 personnel) with limited deployment capabilities primarily concentrated in the capital or very localized urban areas. Integrative missions have broader mandates and more ambitious goals aiming to protect civilians and support the peacebuilding process (Di Salvatore, 2017; Hultman, Kathman & Shannon, 2013, 2014). The deployment of troops follows the conflict where fighting occurs, usually in the periphery of a country. These missions are significantly larger responding to demands posed by complex emergencies (Eide et al., 2005; Dorussen & Gizelis, 2013). 8
Based on a simple regression analysis of only two cross-sections of data (1990 and 2013), we test the significance of a DID estimator,
One complication when defining the PKO treatment is that both first-generation and the integrative PKO existed between 1990 and 2013. To provide a more comprehensive test, we define three types of treatment group (and control group accordingly): first-generation and integrative PKO (i.e. all PKO) vs. no PKO; first-generation PKO vs. no PKO; integrative PKO vs. no PKO.
The regression results are in Table I: in the model specifications 3 and 4, we leave out countries with first generation PKOs to compare the difference-in-differences between countries with integrative PKOs and countries without PKOs; in Models 5 and 6, we leave out countries with integrative PKOs to compare the difference-in-differences between first-generation PKO ‘treated’ countries and countries without PKOs. 10
In this DID, the coefficients of the treatment group dummy variables
The coefficients of the post-treatment period variable (Post-PKO period) captures the expected mean change in MMR from before to after the onset of the treatment period in the absence of the treatment. In Models 1, 3 and 5, we do not include the polity variable: the coefficients of the Post-PKO period variable are negative and statistically significant, suggesting negative baseline time trends in MMR without PKO treatment. However, once the polity score is included in Models 2, 4 and 6, the coefficients are not statistically different from zero. At the same time, the polity score has a negative and highly statistically significant association with MMR: between 1990 and 2013, polity scores for many of the 45 countries included in our analysis increased significantly; it seems that negative baseline time trends in MMR are explained largely by improvements in polity scores.
What most interests us is the DID estimator,
DID with two time periods, 1990 and 2013
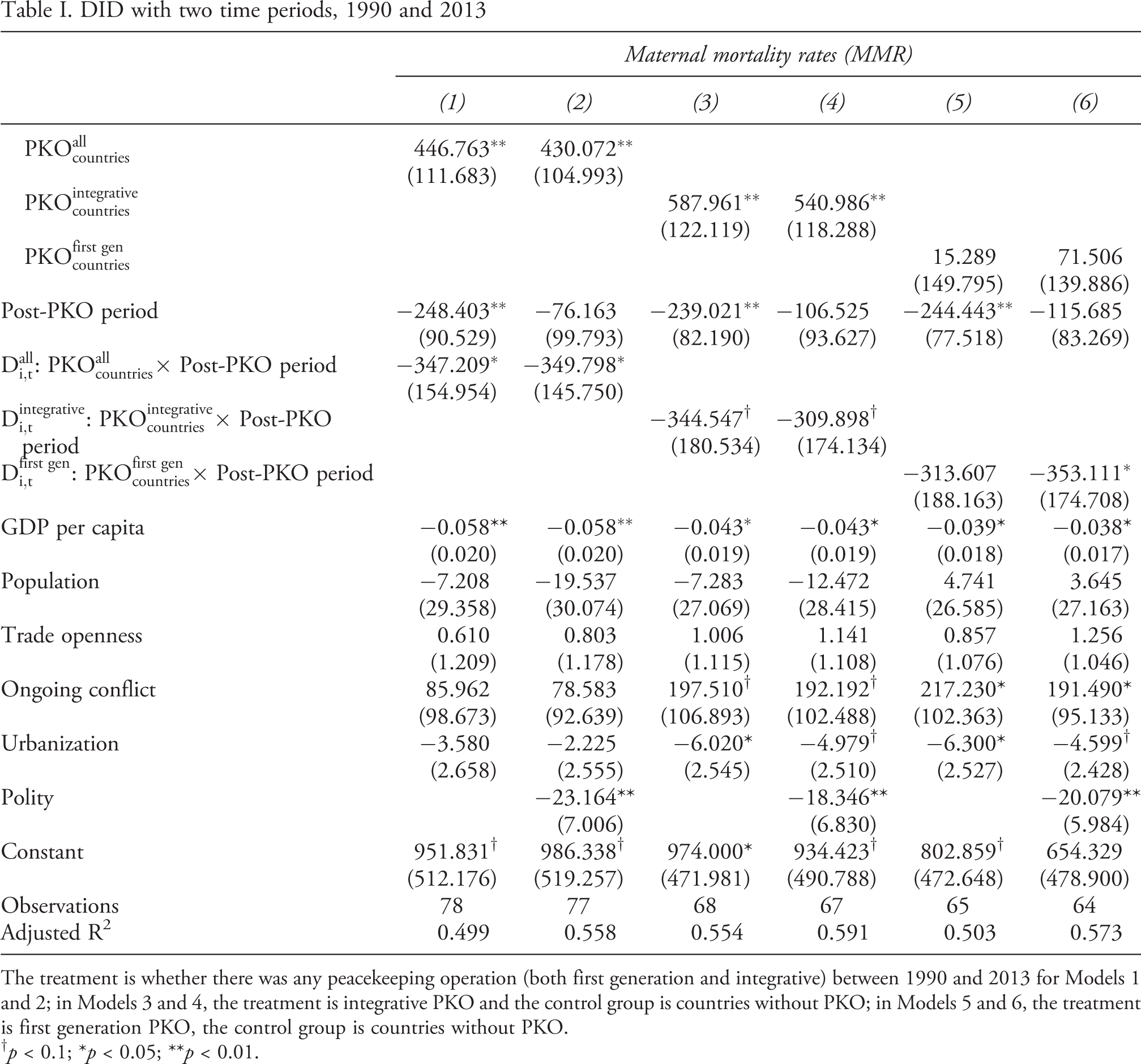
The treatment is whether there was any peacekeeping operation (both first generation and integrative) between 1990 and 2013 for Models 1 and 2; in Models 3 and 4, the treatment is integrative PKO and the control group is countries without PKO; in Models 5 and 6, the treatment is first generation PKO, the control group is countries without PKO.
† p < 0.1; *p < 0.05; **p < 0.01.
A panel DID analysis
DID models with a panel data, 1990–2013

The treatment is whether there was any peacekeeping operation (first generation and integrative types) for Models 1 and 2; in Models 3 and 4, the treatment is integrative PKO, the control group is countries without PKO; in Models 5 and 6, the treatment is first generation PKO, the control group is countries without PKO.
† p < 0.1; *p < 0.05; **p < 0.01.
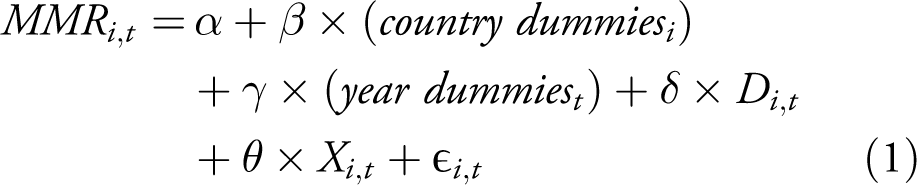
Another significant difference is that the model in Equation (1) does not include a dummy variable for the post-treatment period, because it is absorbed by the year fixed effects (
Table II presents several model specifications from this panel DID. Following Table I, in Models 1 and 2, we define
One advantage of a panel DID is that it allows a statistical test for the parallel trend assumption (e.g. Autor, 2003). More specifically, this is to interact the DID treatment variable with time dummies: here one set of dummy variables indicate whether for a country-year included in the analysis, this year is one year (t–1) before the PKO started, two years (t–2) before PKO, three years (t–3),…, and so on, for years before PKO – their interactions with the DID indicator are often called leads; another set of dummy variables indicate for years after PKO, whether this is one year (t+1) after a PKO started, two years (t+2) after PKO, three years (t+3) after,…, – their interactions with the DID indicator are called lags.
The idea is that one can include the interactions of the time dummies and the treatment indicator for all the periods except one (due to the dummy variable trap). Now all the other interactions are expressed relative to the omitted period which serves as the baseline. If the outcome trends between treatment and control group before treatment are the same, that is, the parallel trend assumption holds, the coefficients associated with the leads should all be statistically insignificant, that is, the difference in differences is not significantly different between the two groups in the pre-treatment periods. This is indeed what we find in Table B-4 of the Online appendix, which lends strong empirical support that the parallel trend assumption holds. 14
Explaining within-country variation with matching
We often see significant within-country variation in public health outcomes. For example, grid-level (55 km by 55 km) average percentages of women who received at least one tetanus injection in Liberia 2007 range from 24.3 to 98.15 with a standard deviation of 18.80. Direct measures of maternal mortality rate are not always available from the DHS. 15 When they are, there is often too much noise in this measure. Indeed, an official report from the DHS (Stanton, Abderrahim & Hill, 1997) concludes that ‘[t]he sampling errors associated with maternal mortality ratios are substantially larger than those associated with other frequently used DHS indicators. This lack of precision precludes the use of these data for trend analysis and has led to the recommendation that this DHS module not be used more than once every ten years in the same country.’ Therefore, we use indirect measures of women’s health from the DHS – two indicators on women’s access to antenatal care and two indicators on women’s education: if women have better access to antenatal care and education, mortality rates will be lower.
At the subnational level, we use data on maternal heath indicators from DHS for Liberia, Côte d’Ivoire and Democratic Republic of Congo. We use PRIO grids as the unit of analysis: these are grid-cells with 0.5 × 0.5 decimal degree cell resolution of the world (Tollefsen, Strand & Buhaug, 2012). 16 We use GPS files from the US Department of Homeland Security (DHS), which give the longitudes and latitudes of survey clusters, to locate surveys to specific grid-cells; 17 this enables us to calculate, for grid-cells that have DHS clusters, average measures of public health indicators. 18
We use four indicators that are comparable across surveys and countries. The first variable (m1_n) measures tetanus injections before giving birth; 19 we make this binary, that is, whether one has received a tetanus injection. We then calculate, as our first dependent variable, the grid-level average percentage of women who have received at least one tetanus injection before giving birth. The second dependent variable is antenatal care (m14_1n): similarly, we calculate the grid-cell level percentage of women who have had at least one antenatal visit. 20 The other two dependent variables are human capital variables that are linked to maternal health. The first one, based on the v106n variable from the DHS, captures the grid-level average of women’s level of education where we define no education as 0, primary education as 1, secondary education as 2 and higher education as 3. The second variable (v107n) measures the grid average of women’s years of education.
We do not choose to use DID at the grid level for these countries because first, the Democratic Republic of Congo has no DHS prior to the initiation of the United Nations Missions in the DRC in 1999; it cannot be included in a DID analysis because there is no pre-treatment period. Second, even though Liberia and Côte d’Ivoire have DHS data before and after the civil wars and the presence of UN missions, using only information from Liberia and Côte d’Ivoire, and selecting grids that have been included in the initial and the more recent DHS surveys, we would have in total only 172 observations.
Finally, in the context of peacekeeping, UN peacekeepers tend to locate in urban centres; it is likely the time trends between urban and rural areas, without the treatment of peacekeeping operations, are different. To deal with such a potential selection bias of PKO locations, we use a matching model to approximate randomized experiments. The basic idea is to select a subset of the observational data wherein the treatment and control units are matched so that they have same characteristics, that is, the same distributions for pre-treatment covariates. In this way, the link between pre-treatment covariates and treatment assignment (peacekeeping) might be broken (approximately) in a way that brings us much closer to the ideal situation where the treatment and control units had been assigned randomly from a single population. Imai & van Dyk (2004) have developed the broad notion of using propensity scores as a means of managing sample matching in parametric studies. However, it is important to note that matching cannot replace randomized experiments because there may be unobserved variables related to both treatment assignment and the outcome; matching (and other non-experimental study) can only match on the observables, which might result in biased treatment effect estimates (Stuart 2010).
We follow Ho et al., (2004) and use MatchIt to find subsamples of the data where the assignment of treatments is not correlated with pre-treatment covariates. Whether there were peacekeeping operations within a grid cell is used to decide whether it has received a treatment (Figure 3 shows PKO distribution within the three countries). We use peacekeeping deployment data from Ruggeri, Dorussen & Gizelis (2017b). The location of the deployment of peacekeeping forces is based on UN Distribution of PKOs, buffer zones, and grids ‘treated’ – (a): Liberia (left) and Côte d’Ivoire, (b): Democratic Republic of Congo
OLS estimates on the matched sample for maternal health access and women education variables
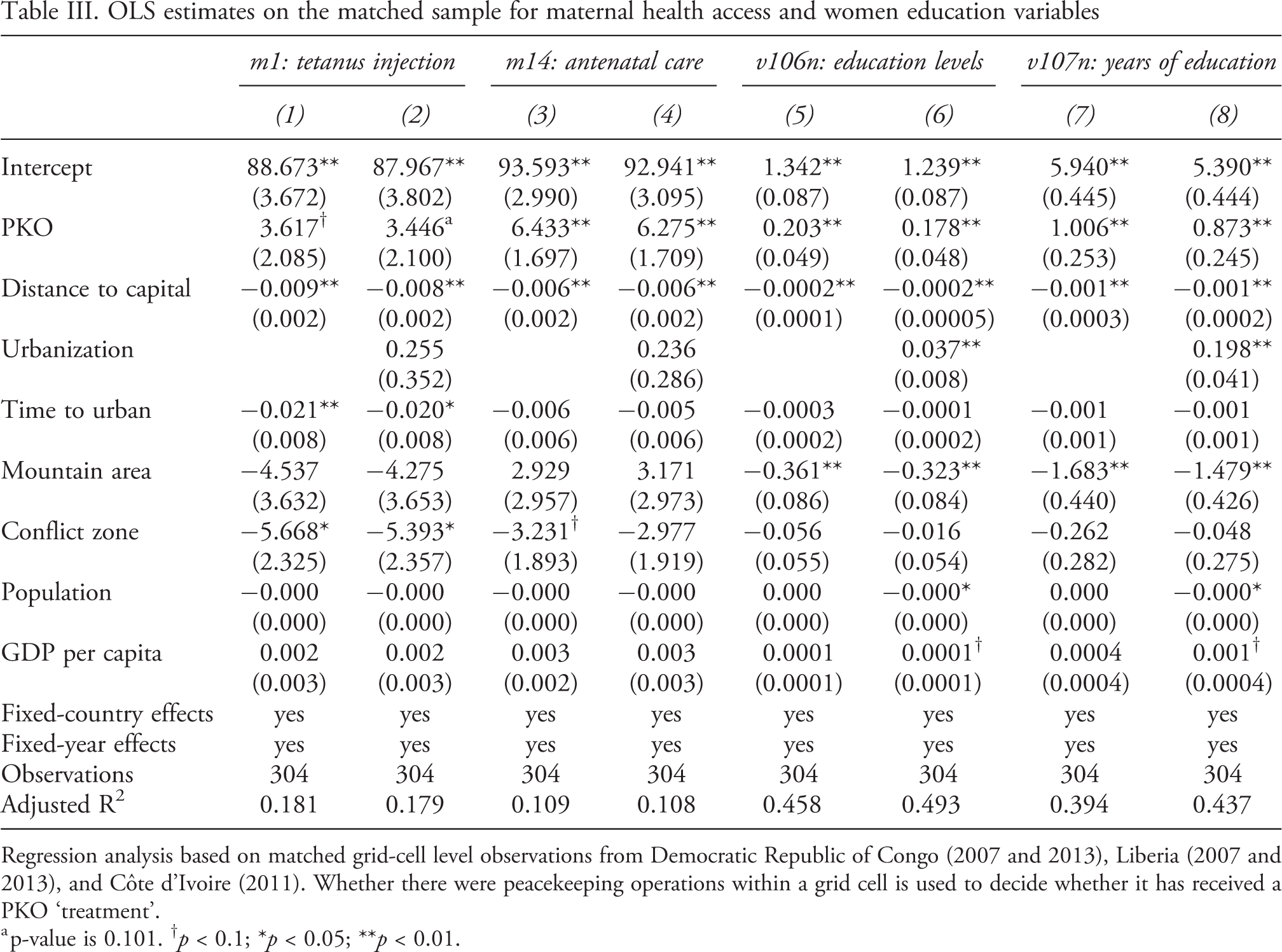
Regression analysis based on matched grid-cell level observations from Democratic Republic of Congo (2007 and 2013), Liberia (2007 and 2013), and Côte d’Ivoire (2011). Whether there were peacekeeping operations within a grid cell is used to decide whether it has received a PKO ‘treatment’.
a p-value is 0.101. † p < 0.1; *p < 0.05; **p < 0.01.
OLS estimates on the matched sample for maternal health access and women education variables, using 25 km buffer zone
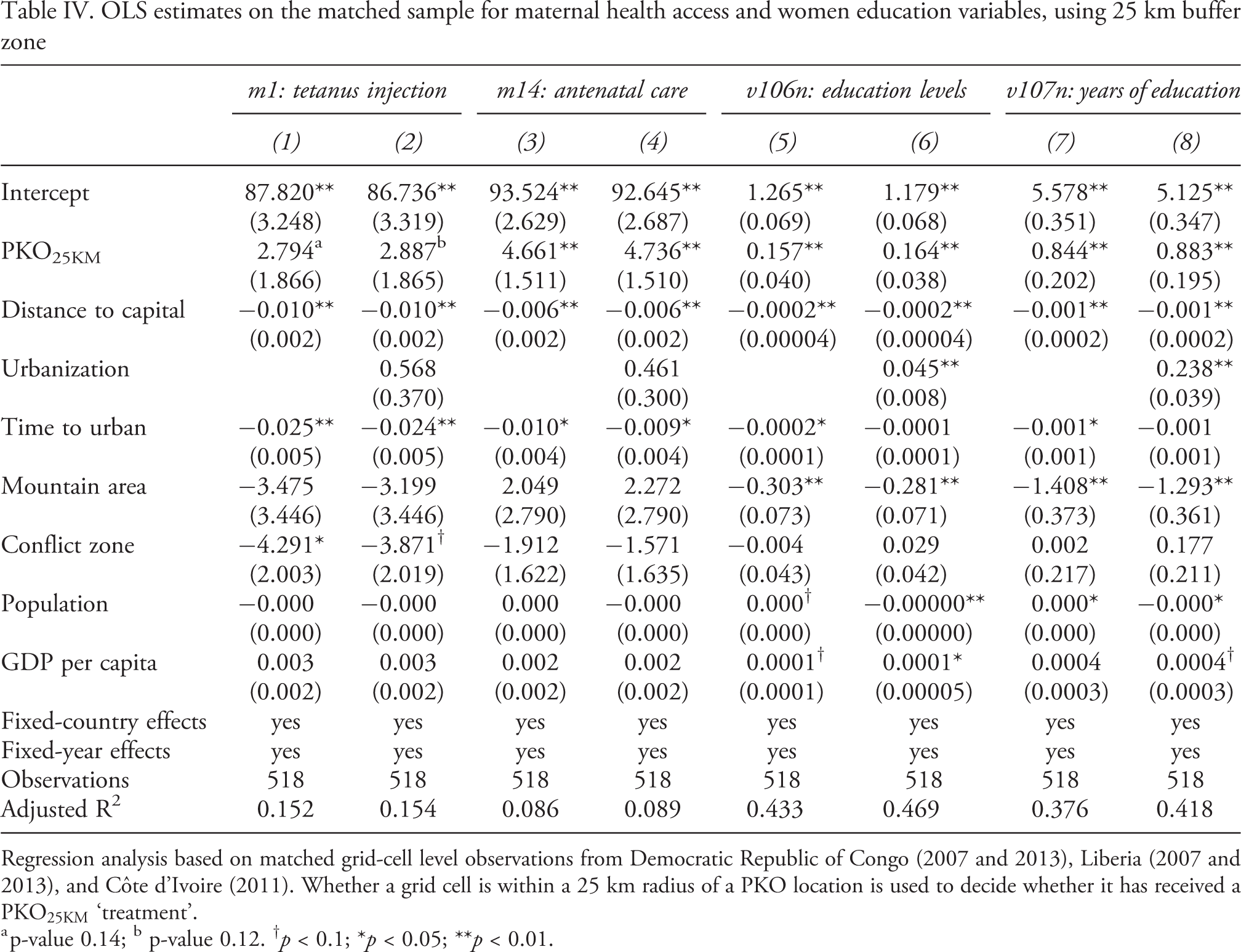
Regression analysis based on matched grid-cell level observations from Democratic Republic of Congo (2007 and 2013), Liberia (2007 and 2013), and Côte d’Ivoire (2011). Whether a grid cell is within a 25 km radius of a PKO location is used to decide whether it has received a
a p-value 0.14; b p-value 0.12. † p < 0.1; *p < 0.05; **p < 0.01.
We find strong effects of PKO on both maternal health indicators in Models 1–4 in Table III. For the first model specification, everything else equal, the percentage of women who had at least one tetanus injection is about 3.617% higher in grid cells with PKO than in grid cells without PKO. The third model specification reveals an even stronger effect of PKO on antenatal care: having PKO increases the percentage of women who have received antenatal care by almost 6.433%.
We further test whether PKO also affects women’s education. Models 5–6 of Table III suggest that PKO is associated with a higher grid-cell-level average in education levels for women. Having a PKO within a grid is associated with an increase in education levels by about 0.178 to 0.203, depending whether we add in the urbanization variable. It is hard to get a concrete sense of the substantive effect since these are levels of education (no education: 0; primary: 1; secondary: 2; higher: 3). The last two models in Table III provide a much more intuitive sense of the substantive effect. After matching, a grid with a PKO is associated with an increase in women’s education of around one year.
Up to this point, we have defined treatment units as those grid cells that include at least one peacekeeping station. However, people might be able to travel from other grid cells to a PKO location to seek help. PKO might affect maternal health conditions of locations outside the grid cell in which it is located. Therefore, as a robustness check, we redefine treatment units as those grid cells that are within a 25 km radius of a PKO location: 25 km is often the maximum travel distance by foot within a day. Figure 3 shows the newly defined treatment units (grid-cells in blue) when we use the 25 km buffers.
We repeat our analysis based on newly matched sample in Table IV. In the first model specifications, the effect of PKO on tetanus injection is still positive, but the significance level drops to 0.12–0.14. PKO’s effect on antenatal care is significant (Models 3 and 4); PKO treatment effects as a function of buffer zone size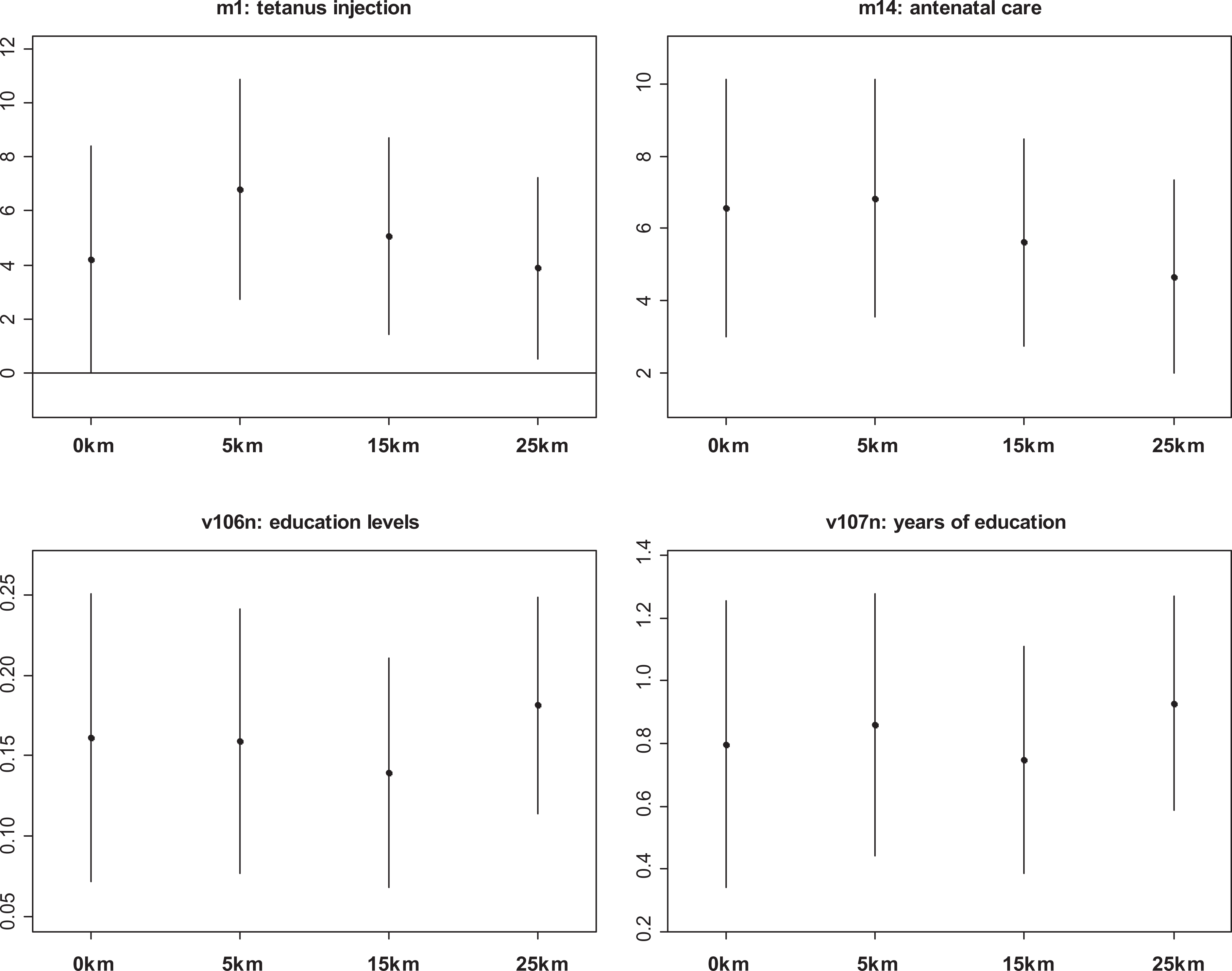
We have conducted further robustness checks. The first motivation has to do with grids on national borders. Up to this point, we have included a grid cell into our sample if a part of the grid is in one of the three countries. This is different from the original PRIO-GRID rule that grid cells that cover the territory of two or more independent states (i.e. the cell intersects with multiple country polygons) are assigned to the country that covers the largest share of the cell’s area. The second motivation is to try additional radius for the buffer around PKO locations: 0, 5 km, 15 km and 25 km – to identify treatment grids which are those intersecting or falling within the buffer accordingly defined. We want to see whether the treatment effects are sensitive to the size of buffer zones.
We repeat the same matching procedure and run regression analysis based on matched samples using the model specification that includes the urbanization variable. Because of space limit, we choose to only present the 95% confidence intervals of the estimated coefficients for the PKO variable, which is the treatment effect on the maternal health and education variables. Figure 4 presents these treatment effects: as we change the size of the buffer zones from 0 to 25 km, more grids would intersect or fall within the buffer zones and be considered as treatment units. It seems that the treatment effects on all four variables are robust to the changes in buffer size around PKO locations. Moreover, after we followed the PRIO-GRID rule, which is more stringent, to decide which bordering grids belong to those three countries, the treatment effect becomes more significant even though we have a lower number of observations. For example, the treatment effect on tetanus injections (m1_n) from Table IV is less than borderline significant; now, its 95% confidence interval does not include zero (see higher left plot of Figure 4).
Finally, in Online appendix C, we report regression results based on matched samples after including grid-cell-level foreign aid as a pre-treatment covariate and a control variable. This partly addresses the concern that PKOs co-occur with other international assistance efforts. After controlling for grid-cell level pre-peacekeeping cumulative aid, we still find that PKOs increase maternal health services and women’s education.
Conclusion
We suggest that peacekeeping has an effect, beyond containing conflict, on maternal health and women’s education in areas with deployment. Peacekeepers might contribute to a surge in resources that improve the provision of medical services. Furthermore, the presence of peacekeepers can increase the overall levels of security within a country indirectly leading to an improvement of maternal health access and women’s education. We conduct analysis at both country and within-country levels, with the latter using geo-referenced UN deployment data and the DHS data in three sub-Saharan countries. We find strong empirical support for a positive effect of peacekeeping presence on maternal health in national-level maternal mortality rates and subnational maternal health service indicators (such as antenatal care and vaccination), as well as levels and years of women’s education.
However, our empirical results need to be interpreted with caution because of built-in limitations of the DID and matching methods. For instance, DID is based on assumptions, such as parallel trend, postulating that the average change in the control group represents the counterfactual change in the treatment group if there were no treatment. For the matching method, one major limitation is that we can only match on observables. Our hope is that by using different empirical methods (DID and matching) and by conducting analysis at both national and subnational levels, we can increase our confidence that peacekeeping improves women’s access to health services and improves education outcomes.
Our study is one of the first to explore the impact of peacekeeping missions on women’s well-being in the aftermath of conflicts. Thus, it moves beyond concepts of ‘negative’ peace and absence of violent conflict to ‘quality’ of peace (Wallensteen, 2015). Despite challenges, PKOs might lead to tangible improvements in the quality of life for women at least in health and education. Both health and education are linked to long-term sustainable developmental goals and women’s empowerment. Our study also suggests that provision of security can lead to significant dividends by creating the necessary space for improving health and education in post-conflict countries.
Our findings do not imply that the emerging structures are sustainable long-term or more equitable. There is a risk that the peacekeeping dividend can be lost if countries lack either the capacity or the will to invest sufficiently in health and education when peacekeeping forces start the drawdown process or pull out altogether. The devastation of the recent Ebola epidemic in Liberia and Sierra Leone highlighted the perils of weak and over-dependent health care systems for the population and especially pregnant women. Still, given the low amount of resources invested to peacekeeping, our analysis suggests remarkable payoffs.
Footnotes
Replication data
Acknowledgements
We would like to thank Brian Phillips and the three anonymous reviewers for their constructive comments and suggestions.