
Abstract
Objectives
The current study examined whether risk factors associated with recidivism also influence likelihood of early mortality. The baseline model and shelf-life models assess whether the level and timing of risk factor measurement is associated with differential mortality risk. The dynamic change model assesses whether within-individual change provides explanatory information beyond that obtained from single timepoint measures.
Methods
A cohort of 1,155 formerly incarcerated Canadian youth were followed into adulthood. Items from recidivism risk assessment tools (interpersonal support, antisocial attitudes, academic/vocational skills, substance use, and mental health instability) were used in a series of Cox proportional hazard models.
Results
Earlier baseline measurements of risk factors did not predict mortality, while those assessed closer to the time of death were significantly associated with increased mortality risk. Greater substance use increased mortality risk, while mental health instability unexpectedly decreased mortality risk. The dynamic change model found that within-individual increases in antisocial attitudes were associated with elevated mortality risk.
Conclusions
Timing and change in risk factors are more predictive of early mortality than static measures from adolescence. Future research should consider both community risk factors and correctional system monitoring to better understand the contribution of individual-level risk.
Based on evidence that criminal legal system-involved populations face an elevated risk of early mortality, research has explored whether established risk factors for offending (e.g., onset of offending, substance use, gang involvement) are also risk factors for early mortality (Binswanger et al., 2020; Kullgren et al., 1998; Laub & Vaillant, 2000; Lattimore et al., 1997; Lidberg et al., 1989; Pritchard et al., 1997; Skinner et al., 2022; Teplin et al., 2005). Although this literature has advanced the idenitification of risk factors for early mortality, focusing on statistical prediction can oversimplify how risk factors operate (Wikström, 2020). More precise means of identifying individuals at heightened risk of early mortality is an important step in responding to calls to reduce early mortality among criminal legal system-involved populations (Butler et al., 2023). The forensic psychology literature and developmental life-course paradigm have provided useful roadmaps for conceptualizing risk, not just in terms of (a) the level of a risk factor (i.e., propensity) but also (b) its temporal proximity in relation to the outcome of interest (i.e., timing; Viljoen et al., 2017a), and (c) whether the level of the risk factor has changed over time (i.e., within-individual change; Le Blanc & Loeber, 1998; Nagin & Paternoster, 2000). The latter two components of risk have been neglected in research on early mortality.
The current study used data on 1,155 participants from the Incarcerated Serious and Violent Young Offender Study (ISVYOS) to examine whether risk factors traditionally associated with recidivism (e.g., substance use, antisocial attitude, lack of social support) also influence the likelihood of early mortality. The analytic sample included participants followed into adulthood who had received a structured intake interview during adolescence and at least two evaluations on the Community Risk Needs Assessment, a tool used by the British Columbia Corrections Service for case management and planning. Approximately 12% of participants died during the follow-up period. A series of Cox proportional hazard models were used to examine whether level, timing, and within-individual change in risk factors were associated with early mortality. We applied two approaches to understanding risk factors for mortality: the shelf-life hypothesis and the dynamic change hypothesis (Vincent & Grisso, 2005).
Shelf-Life Hypothesis
A basic principle of the risk factor paradigm is that higher levels of risk correspond with a greater probability of adverse outcomes (Farrington, 2000). This level-based perspective reflects the dominant approach within the literature on risk factors for mortality, where studies have found that higher levels of gang involvement (Lattimore et al., 1997; Teplin et al., 2014), substance use (Chassin et al., 2013; Kinner et al., 2015; Stattin & Romelsjo, 1995; Stenbacka et al., 2012), and alcohol dependency (Laub & Vaillant, 2000; Teplin et al., 2014) increased risk of mortailty. However, in some cases, these risk factors were measured up to five decades prior to mortality (e.g., Laub & Vaillant, 2000; Piquero et al., 2014). For a static risk factor (e.g., age of offending onset), which does not change, the timing of risk factor measurement may be considered less consequential (Farrington, 2000). From a population heterogeneity perspective, static risk factors are assumed to reflect relatively stable underlying propensities, such as low self-control (Gottfredson & Hirschi, 1990), such that the period of the life-course in which a risk factor was measured may be considered trivial. However, some commonly studied risk factors for mortality (e.g., substance use, gang involvement) may not be static nor stable, suggesting that level alone represents only one component of understanding mortality.
The shelf-life hypothesis addresses the importance of timing by positing that the association between a risk factor and an outcome weakens as time passes between measurement and outcome (Vincent & Grisso, 2005). Although the level of a risk factor is still important, a risk factor measured more proximally to the outcome should exhibit a stronger association than the same risk factor measured further from the outcome. In other words, a risk factor has a shelf life, and waiting too long to reassess someone's risk implies that their risk status may “expire.” This premise justifies correctional practices that emphasize updating risk assessments, on the assumption that more recent assessments better reflect individuals’ current circumstances and risk status (Viljoen et al., 2017a). The shelf-life hypothesis aligns with developmental criminology principles that suggest proximal risk factors better capture individuals’ current situations and therefore may have a stronger impact on the outcome than the same risk factor measured months or years earlier (Chung et al., 2002; Losel & Bender, 2003).
The shelf-life hypothesis can be tested by examining whether risk assessments for reoffending taken more proximally to the occurrence of recidivism improved predictive validity (Davies et al., 2022; Lloyd et al., 2020). The hypothesis is not supported if the timing of risk factor measurement fails to improve statistical prediction, and the association with mortality remains stable regardless of measurement timing (Skinner et al., 2022; Zane et al., 2019). Chassin et al. (2013), using data from the Pathways to Desistance Study, found that some risk factors (i.e., substance use severity, gang membership, gun carrying) measured approximately 18 months prior to death explained mortality above and beyond risk factors measured at baseline, when participants were between the ages of 14 and 18. Although Chassin et al.'s (2013) study supported the importance of accounting for risk factor timing, this was not a direct test of the shelf-life hypothesis because the study did not compare the impact of the same risk factor measured at different points in the life-course. Thus, it remains to be seen whether measurement of the same risk factor more proximal to mortality would improve statistical prediction.
Dynamic Change Hypothesis
The dynamic change hypothesis posits that changes in risk may themselves be consequential, independent of absolute level. For example, two individuals may exhibit similarly high risk at age 21, yet the person whose risk increased from age 20 to 21 may have a different likelihood of an adverse outcome, than the individual whose risk remained consistently high from age 20 to 21 (Olver et al., 2007). The forensic psychology literature has conceptually distinguished between static (e.g., age of offending onset) and dynamic factors (e.g., substance use), as well as explored whether changes in dynamic factors corresponds to a change in the probability of an adverse outcome (Viljoen et al., 2017b). This distinction parallels the risk-need-responsivity (RNR) model (Andrews et al., 1990), which differentiates between static risk factors (i.e., fixed historical characteristics such as criminal history) and dynamic criminogenic needs (e.g., antisocial attitude, substance use) that are modifiable. While the RNR model focuses on reoffending, conceptually similar distinctions may be useful for thinking about the impact of static and dynamic risk factors on mortality. Tremblay and Pare (2003) had the RNR model in mind when describing how transitioning from prosocial peer relationships to antisocial peer relationships was a risk factor for early mortality.
Although the examination of within-individual change is a fundamental principle of developmental and life-course criminology, this dimension has been neglected in research on early mortality. Chassin et al. (2013) specified a conceptual distinction between static (distal) and dynamic 1 risk factors, but they did not examine whether changes to risk factors impacted the probability of mortality. While static risk factors were measured as a combination of demographic (e.g., race/ethnicity, parental education) and historical factors (e.g., prior offenses, substance use, or mental health disorder diagnosis), dynamic risk factors included measures thought to be modifiable, such as peer antisocial behavior, family cohabitation, and exposure to violence. However, dynamic risk factors were measured at a single time point (also see Teplin et al., 2014).
To reiterate, the shelf-life hypothesis and dynamic change hypothesis are distinct. The shelf-life hypothesis focuses on recency of a measure but does not consider whether the level of a risk factor changed or remained stable. The dynamic change hypothesis focuses on the degree of change between assessments rather than overall level of risk (e.g., moving from a score of “2” to “4” is equivalent to moving from a score of “5” to “7”). A recent measure may be temporally close to the outcome of interest, without reflecting substantial change. Conversely, substantial change may occur even when assessments are separated by a relatively short time interval. Thus, recency and change capture different aspects of risk.
Role of Risk Assessments in Preventing Early Mortality
The risk-need-responsivity model, which guides criminal legal decision making in many jurisdictions, is premised on the notion that changes in risk factors should inform changes in treatment needs and treatment intensity (Andrews et al., 1990; Bonta & Andrews, 2007). Despite this straightforward premise, the risk assessment literature has spent decades grappling with how to make use of multiple assessments of the same risk factor instrument (e.g., use the first score, use the most recent, use the lowest score, use the highest score, use the average; see Babchishin et al., 2024).
If the criminal legal system is to contribute to calls to reduce early mortality rates in its population (Butler et al., 2023), then it is crucial to know how to best identify a person's risk for early mortality. Testing the shelf-life hypothesis and dynamic change hypothesis directly evaluates this question (also see Chassin et al., 2013). Doing so clarifies, for example, whether it is important for risk assessment tools to be updated to account for changes to the timing and level of a risk factor. Correctional system professionals may need to consider the process of risk reduction beyond just the level of a person's risk. This would entail communicating risk in terms of timing, change, whether change occurred as a result of treatment and is expected to continue (Davies et al., 2023). Two people may have the same level of risk but differ in treatment needs if one person has remained at that same level of risk for months, whereas the other person recently shifted from low risk to high risk. On the other hand, if neither hypothesis is supported, then the criminal legal system can avoid intensive and costly procedures of reassessing risk.
Study Aims
The current study contributes to research on the overlap between risk factors for mortality and risk factors for offending by examining whether the level, timing, and change in risk factors relate to mortality. We measure these different dimensions of risk using three complementary models. The baseline model uses the first available risk assessment to measure risk factors at a single time-point, earlier in the follow-up period. The shelf-life model uses the most recent available risk assessment to assess risk factors for mortality at a single time-point, later in the follow-up period. The dynamic change model uses all available risk assessments to capture within-individual change in risk factors over time. Risk factors examined in the current study include substance use, mental health instability, interpersonal support, antisocial attitudes and vocational/academic skills. Although this study is not designed to determine which modeling approach best explains mortality, applying the same set of risk factors across models allows us to test both the shelf-life hypothesis and the dynamic change hypothesis. The baseline model and shelf-life models assess whether the level and timing of risk factor measurement is associated with differential mortality risk. The dynamic change model further assesses whether within-individual change provides explanatory information beyond that obtained from single time-point measures. While the goal of this paper is not to adjudicate between within-person or between-person approaches, it directly evaluates whether incorporating change in risk factors is informative for understanding mortality.
Considerable attention has been given to identifying risk factors for offending that may also be risk factors for early mortality (e.g., Fazel et al., 2014; McCandless et al., 2015; Piquero et al., 2005). Identifying a common cause of offending and mortality allows intervention strategies to simultaneously reduce both offending and mortality. For example, substance use is a risk factor for both offending and early mortality, making substance use treatment programs beneficial for mitigating multiple adverse outcomes (e.g., Decker et al., 2017; Pitkänen et al., 2020). The current study contributes to the search for shared risk factors by examining whether the risk/need factors used in reoffending risk assessment tools also help explain early mortality.
Method
Sample and Procedures
The ISVYOS obtained permission from the Ministry of Children and Family Development to recruit boys and girls (n = 1,719) held in custody centers in British Columbia, Canada, between 1998 and 2011. Among 1,719 youth recruited between 1998 and 2011, 1,640 participated in an intake interview conducted by research assistants (RAs). RAs typically approached youth to participate in the study within the first week of their incarceration. Interviews occurred in a private room away from other youth and custody staff. To obtain informed assent, youth were both read and provided with an information sheet detailing the study's objectives, data collection procedures, the voluntary nature of participation, and assurances that responses were kept confidential except in instances where participants directly threatened themselves or someone else. Participants were also informed that involvement in the study would not impact their status in custody (e.g., security level) nor sentencing outcome. Approximately 5 percent of youth declined to participate.
Data were also collected through the Corrections Network (CORNET), a client management software program where criminal legal system professionals record information about their clients. CORNET includes youth and adult data for all persons involved in the criminal legal system in British Columbia. Excluding participants with sealed CORNET records or missing data resulted in a sample of 1,437, of whom 1,155 had completed a minimum of two risk assessments and were therefore included in the analysis. The analytic sample includes participants born between 1979 and 1997 and followed on average from age 15 to 32 (R = 12–42).
Measures
Descriptive statistics for all variables are presented in Table 1. The mi chained command in Stata (Statacorp, 2021) was used to impute missing values on all measures. Missing data were addressed with multiple imputation, generating 30 imputed datasets. Imputed variables included all risk assessment measures (i.e., substance use, mental health instability, antisocial attitude, academic/vocational skills, interpersonal support 2 ), and proportion of missing data for each imputed variable ranged from five observations (0.04%) to 31 observations (2.68%). Imputations were predicted based on complete demographic information (e.g., age, gender, race), criminal history (e.g., conviction rate, incarceration rate), risk assessment details (e.g., number of total assessments, order of risk assessments), and deceased status. Parameter estimates were then pooled across imputations using Rubin's (1987) rules. Global model fit statistics are not reported because these are not directly pooled across imputed datasets.
Descriptive Statistics for Participants (n = 1,155).
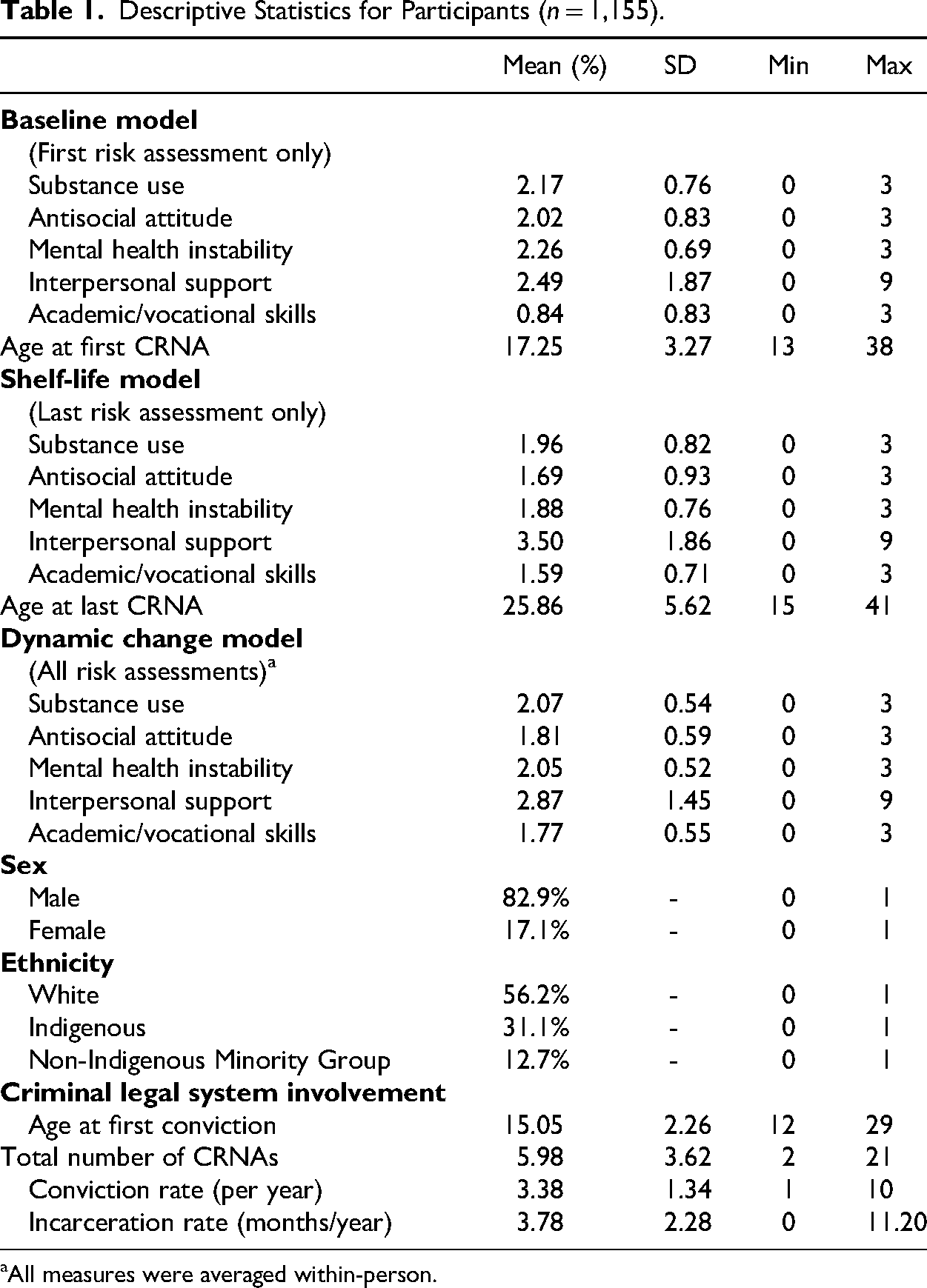
All measures were averaged within-person.
Mortality. Mortality status and date of death were obtained primarily through CORNET. For participants with active criminal legal system contact (i.e., custodial or community supervision), their criminal histories are maintained by correctional staff on CORNET, which listed date of death and occasionally, cause of death. For participants no longer subject to criminal legal system monitoring, names were further queried through online search engines. Deaths reported in online obituaries and news media were verified by cross-referencing with the participant's name, demographic details (e.g., place of residence, sex), and date of birth. If one of these factors did not match, we did not code the participant as deceased. By the end of the follow-up period (October 31, 2022), 142 participants (12.3%) were deceased. The rate of mortality in the current study is as high or higher when compared to studies that sampled from youth custody facilities (e.g., Chassin et al., 2013; Teplin et al., 2005). The mean age at death was 28.27 (SD = 5.15; R = 19.17–42.52). Due to the inconsistency in reported causes of death (available for 61.3% of deaths), analyses were restricted to mortality status and date of death. However, of the known causes of death (n = 87), overdose was the most common (n = 41; 47.1%), followed by homicide (n = 25; 28.7%). 3 These findings align with previous research indicating offending samples exhibit elevated mortality risk due to unnatural causes compared to nonoffending samples (Elonheimo et al., 2017; Skinner & Farrington, 2020; Teplin et al., 2005).
Risk Factors. The Community Risk Needs Assessment (CRNA) is a structured assessment tool used in the case management practices of criminal legal system professionals in British Columbia, based on the central eight risk factors of the RNR model (Bonta & Andrews, 2007). The intention was for the CRNA to be administered every 6 months, typically by probation officers, to ensure criminal legal system professionals remained aware of changes to the risk and needs factors of individuals under supervision (Gress, 2010). CRNA items include indicators of antisocial attitudes and personality traits, crime-involved peers, family and intimate partner issues, education and employment challenges, substance use severity, and mental health instability. These measures can be considered dynamic given their potential to change with each reassessment, which we include in the dynamic change model. For each item, individuals are rated on a four-point scale. Probation officers rely on several sources of information to rate items, including self-report information obtained from interviews with their client, other reports and assessments (e.g., presentence reports), and communication with friends and family. Higher scores indicate greater likelihood of challenges during reintegration.
To measure substance use, we used a single CRNA item that assessed substance dependency as a risk factor for reoffending, with higher values indicating greater substance use. Both alcohol and drug use are major risk factors for mortality (Coffey et al., 2003; van de Weijer et al., 2016). Formerly incarcerated persons face a heightened risk of fatal overdose following release into the community (Patterson, 2013), which may be due to reduced substance use during incarceration and subsequent decreased tolerance (Pratt et al., 2006). Substance use may also exacerbate chronic health conditions (e.g., cardiovascular disease), which tend to be more prevalent among justice-involved populations (Vaughan et al., 2017; Zane et al., 2019).
To measure mental health instability, we used a single CRNA item that assessed behavioral and emotional difficulties, with higher values reflecting more severe mental health issues. Research suggests a strong association between diagnoses of psychiatric disorders and elevated mortality in offending samples (Sailas et al., 2006; Stenbacka et al., 2012), particularly due to suicide (Kullgren et al., 1998; Marks et al., 2024). Furthermore, experiences of incarceration have been shown to exacerbate preexisting mental health conditions (Schnittker et al., 2012; Sugie & Turney, 2017) and in many cases, result in inadequate access to treatment (Reingle Gonzalez & Connell, 2014), thereby compounding the risk of mortality.
To measure antisocial attitudes, we used a single CRNA item that rated an individual's resistance to change and problematic impulses, with higher values denoting stronger antisocial dispositions. Antisocial attitudes may increase mortality risk due to more frequent and persistent offending (Elonheimo et al., 2017; Skinner et al., 2022), which may expose individuals to fatal victimization by engaging in conflict-prone activity (Piquero et al., 2005). Individuals with antisocial attitudes may be inclined toward sensation seeking and risky behaviors (e.g., reckless driving, firearm use), which may in turn increase likelihood of fatal accidents (Tremblay & Pare, 2003).
To measure academic/vocational skills, we used a single reverse-coded CRNA item that rated an individual's degree of academic or vocation skills, with higher values indicating more skills. Skill sufficiency captures an individual's employment potential and readiness. Being able to maintain legitimate employment may embed an individual in prosocial work institutions and discourage risky or criminal behavior, through exposure to potential formal (e.g., management) and informal (e.g., coworker) social control (Hollinger & Clark, 1982; Sampson & Laub, 1990), which may lead to decreased mortality risks. Additionally, an individual who has gained academic and vocational skills may have participated in programs or benefited from reintegration resources, suggesting lower likelihood of reoffending and therefore decreased mortality risk.
To measure interpersonal support, we summed scores from three CRNA items: supportive family relationships, prosocial intimate partners and associations, and living arrangement stability (polychoric ordinal α = .71). We used a summed scale rather than individual items given prior research has emphasized that social bonds and supports tend to be cumulative rather than based on a single item (Nguyen & Loughran, 2018; Savolainen, 2009). CRNA items were reverse-coded so that higher scores indicated stronger interpersonal support. Interpersonal supports could lower mortality risk by providing emotional assistance and instrumental assistance (e.g., financial support, housing), which could buffer stress, facilitate access to health and social services, and foster healthier coping behaviors (Meisenhelder, 1977; Mowen et al., 2019; Taylor, 2016). Additionally, close prosocial relationships may provide informal monitoring and control (Laub & Sampson, 2003), such as discouraging association with antisocial peers (Visher & Travis, 2003), which can further reduce exposure to violent or dangerous situations.
Control Variables. To adjust for past criminal legal system involvement, two indicators captured participants’ cumulative exposure: incarceration rate (number of months incarcerated divided by number of years with any incarceration) and the conviction rate (number of convictions divided by follow-up period). 4 Standardizing exposure by individual observation time allows for comparison across participants of differing follow-up lengths. Periods in custody can reduce mortality in the short-term by providing stable shelter and legally mandated health care (Daigle & Naud, 2012). In contrast, a higher conviction rate indicates persistent offending, which may heighten risks of lethal conflicts (Binswanger et al., 2020).
To adjust for demographic disparities in mortality, we included self-identified race: White (55.4%), Indigenous (31.4%), and a non-Indigenous minority group (13.2%). Racialized individuals, particularly Indigenous peoples, face elevated mortality relative to White counterparts (Teplin et al., 2014; Zheng et al., 2023). Consistent with literature on incarcerated samples, Indigenous participants were overrepresented in the sample compared with their proportion in the Canadian population (e.g., Wiley et al., 2020). Additionally, we controlled for sex to account for the increased mortality risk that males experience compared to females in legal system-involved populations (Fitch et al., 2024; Kjelsberg & Laake, 2010). The sample was predominantly male (81.6%).
To account for the increased mortality risk that accompanies aging (Aalsma et al., 2016; Piquero et al., 2005), we included age at the time of CRNA completion, as well as a squared term to account for a potential curvilinear relationship (Kariminia et al., 2007). The mean age at first risk assessment was 17.86 (SD = 3.29, R = 13.03–38.56) and at last risk assessment was 26.32 (SD = 5.61, R = 15.14–41.92), with a mean interval between first and last assessments of 8.46 years (SD = 5.81, R = 0.17–24.92). Accounting for aging is critical when evaluating the dynamic perspective because a likely explanation for mixed results with respect to the importance of change in risk factors has to do with whether risk factor change is measured in short intervals in adolescence when change is more common (Viljoen et al., 2017a) or longer intervals in adulthood when stability is more common (Olver et al., 2007).
We also controlled for total number of risk assessments, 5 given that individuals with greater offending may be more likely to receive repeated CRNAs. Participants were assessed an average of 5.98 times (SD = 3.62; R = 2–21) during the follow-up period, resulting in a total of 6,903 assessments across all participants.
Analytic Strategy
To estimate the relationship between risk factors and mortality, we used the Cox proportional hazard model (Cox, 1972), a semiparametric form of survival analysis designed to examine the time until an event occurs (Allison, 2014). The Cox model estimates the hazard function, which in the current study reflected the instantaneous risk of experiencing mortality at time t, given survival up to that point, as a function of covariates (Kleinbaum & Klein, 2012). The Cox model accommodates both time-invariant covariates (used in the baseline and shelf-life models) and time-varying covariates (used in the dynamic change model). An assumption of the Cox model is proportional hazards, meaning the ratio of hazards remains constant between subjects over the follow-up period (Cox, 1972). The assumption was tested 6 using a combination of Schoenfeld residuals tests and visual inspections of partial residual plots (Grambsch & Therneau, 1994). Mental health instability and antisocial attitude failed the Schoenfeld residuals test (p < 0.05), but visual inspections indicated no discernable departures from the horizontal line in the residuals (see Figures S1–S3 in the Supplemental Materials).
Survival analysis is well-suited for studying early mortality because it addresses right-censoring situations where some participants have not experienced the event of interest by the end of their individual follow-up period. Survival analysis accounts for this partial information by incorporating participant follow-up times into the model, reflecting the fact that they remain at-risk. This is particularly important in studies of mortality, where participants will experience the event given sufficient time. Figure 1 shows the survival proportion of the sample at each age, without accounting for censoring. The survival proportion begins to decrease at age 19, with a steeper drop between age 23 (n = 35; 97.0%) and age 30 (n = 107; 90.7%). Subsequent declines are more gradual, with survival at 88.8% (n = 129) by age 35, and 87.7% (n = 142) by age 42.

Survival proportion by age for the sample, not accounting for censoring.
Given the strong relationship between offending and mortality, participants were considered to be at-risk for mortality beginning at the age of first contact with the criminal legal system (i.e., earliest age at conviction or custody). The survival period ends at the age of death or the end of the participant's follow-up period (i.e., censoring). On average, participants’ first CRNA occurred 3.20 years (SD = 3.05; R = 0.03–22.89) into the survival period (i.e., after age at first criminal legal system contact) and 10.91 years (SD = 5.34; R = 1.73–25.09) before death. On average, participants’ last CRNA occurred 3.10 years prior to death (SD = 3.45; R = 0–13.71) 7 or 7.11 years prior to end of follow-up for the nondeceased (SD = 4.87; R = 0–22.73). The Supplemental Materials provide a detailed explanation of the coding strategy as well as an example data structuring for the baseline, shelf-life, and dynamic change models (see Table S1 in the Supplemental Materials).
For the baseline model and shelf-life model, all risk factors were treated as fixed. These two models differ only in terms of whether risk factors were measured based on the first CRNA rating or last CRNA rating. When testing each of these perspectives, the hazard of death for participant i at time t was modeled as:
For the dynamic change model, the hazard function allows for time-varying covariates:
Results
Table 2 presents pooled HRs and 95% confidence intervals from three Cox proportional hazard models examining predictors of mortality across the baseline, shelf-life, and dynamic change models. HRs for key risk factors across each of the three models are summarized in Figure 2.
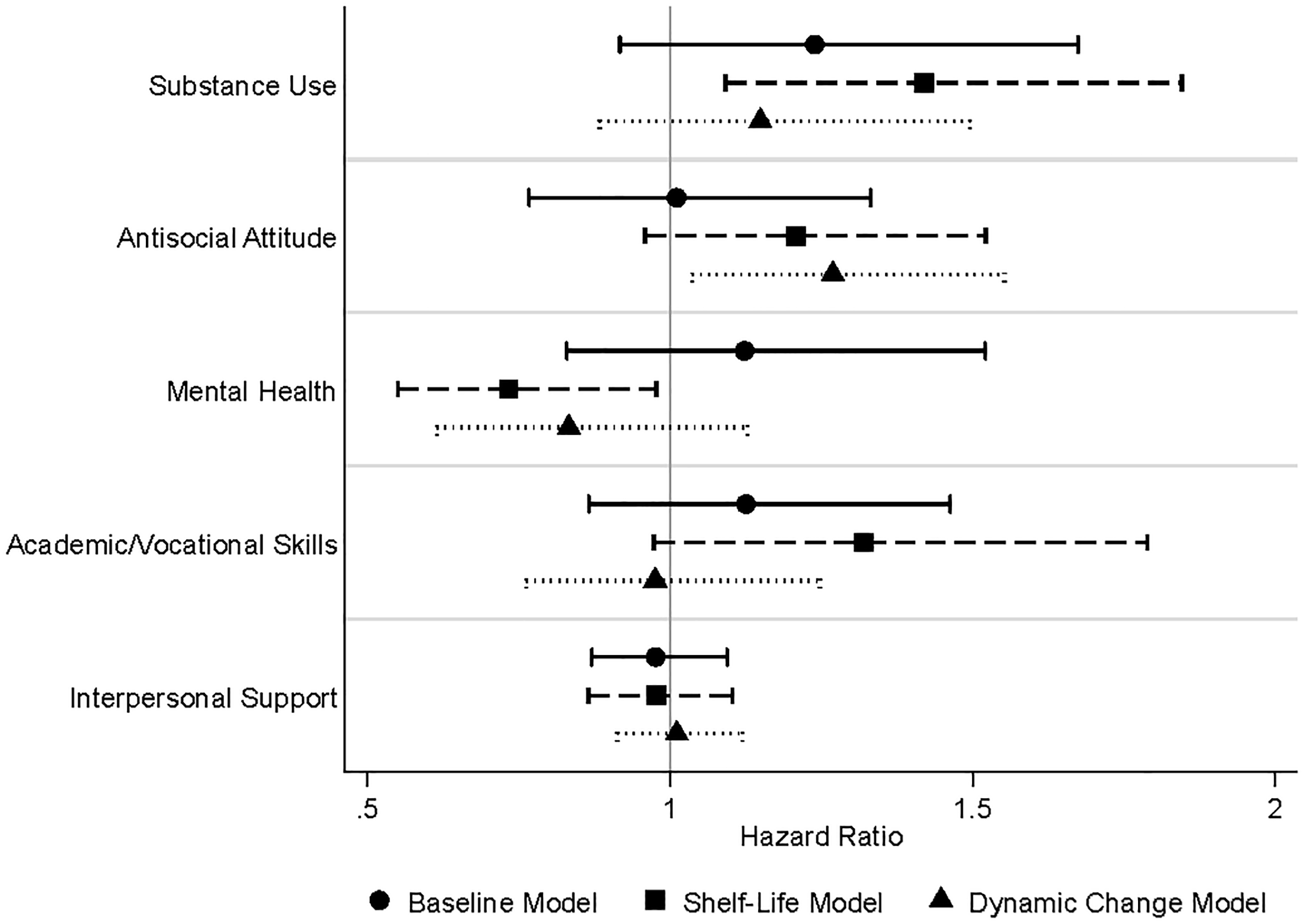
CRNA risk factor hazard ratios with 95% confidence intervals for baseline, shelf-life, and dynamic change models.
Cox Model Results (n = 1,155).

Note: Conviction rate is standardized by length of follow-up period.
Reference category.
All CRNA risk factors are first-differenced (subtract CRNA value at t–1 from the value at t).
* p < 0.05, ** p < 0.01, *** p < 0.001.
The baseline model (Model 1) used only the earliest CRNA measurement. None of the CRNA-measured risk factors significantly impacted the likelihood of mortality. However, male participants exhibited significantly elevated mortality risk compared to female participants. Each additional risk assessment was associated with a 9% reduction in the hazard of death.
The shelf-life model (Model 2) used the most recent CRNA available. 8 Each one-unit increase in substance use score was associated with a 42% increase in the hazard of mortality. Mental health instability was unexpectedly negatively related to mortality, with a one-unit increase associated with a 27% reduction in the hazard of death. As was the case in Model 1, male participants exhibited a higher risk of mortality. Each additional conviction per year observed was associated with a 17% increase in mortality risk.
To compare the performance of the baseline and shelf-life models, predictive discrimination was assessed using Uno's C-statistic, which represents a model's ability to correctly distinguish between participants who will experience the outcome (e.g., 0.5 refers to discriminative ability equal to a coin flip; 1.0 indicates perfect discrimination). Uno's C uses inverse probability of censoring weights to correct for unequal follow-up periods across participants (Uno et al., 2011). Uno's C indices were pooled across 30 multiple imputations (Rubin 1987). Uno's C requires the specification of truncation time (tau), beyond which comparisons between pairs are not made. This is necessary because as follow-up extends, fewer participants remain under observation, making pairwise comparisons increasingly unreliable. Tau was set to age 38, by which point 96% of all observed deaths in the sample had occurred, ensuring that the discrimination statistic reflects nearly the full mortality experience of the sample while remaining statistically stable. At age 38, the shelf-life model (C = 0.79; 95% CI [0.73, 0.84]) demonstrated significantly (p < 0.01) greater discriminative ability than the baseline model (C = 0.68; 95% CI [0.62, 0.74]). An increase of 0.11 indicates that the shelf-life model correctly stratifies risk for an additional 11% of all possible subject pairs compared to the baseline model. Sensitivity analyses at ages 28 and 30 produced consistent findings. 9
The dynamic change model (Model 3) accounted for repeated assessments of dynamic factors by using first-differencing to capture wave-over-wave change in time-varying covariates. Antisocial attitude was the only significant CRNA risk factor. A one-unit increase in antisocial attitudes between time t–1 and time t was associated with a 27% increase in mortality risk between time t and time t + 1. Male participants and conviction rate remained significantly related to increased mortality risk, with each one-unit wave-over-wave increase in convictions subsequently increasing the wave-over-wave mortality hazard by 18%. Each additional risk assessment was associated with a 16% reduction in the hazard of death.
Discussion
Early mortality among individuals involved in the criminal legal system represents a persistent public health concern (Fischer et al., 2019; Jannetto, 2021). In response, researchers have explored the overlap between offending and early mortality by identifying shared risk factors. Although relying on criminological theory and the risk factor paradigm has contributed to identifying risk factors statistically associated with early mortality (Kullgren et al., 1998; Lidberg et al., 1989; Zheng et al., 2023), statistical prediction is not the same as explanation (Wikström, 2020). Using data on 1,155 incarcerated youth who were followed into adulthood, the goal of the current study was to move towards a better understanding of the association between risk factors and mortality. We addressed this goal by examining the impact of a given risk factor on mortality through the lens of baseline, shelf-life, and dynamic models. The baseline model proposes that the level of a risk factor determines the strength of its association with mortality, irrespective of the timing of measurement. The shelf-life model holds that the timing of the risk factor measurement relative to the mortality event is what matters most, not the level itself. The dynamic change model emphasizes the importance of directly examining whether change impacts the outcome of interest. Findings are interpreted with a focus on (a) the implications for the shelf-life hypothesis and the dynamic change hypothesis, and (b) the implications of risk factors identified as significantly associated with early mortality.
Evaluating Temporal Dynamics of Risk for Early Mortality
The current study found that risk factors measured at baseline, temporally distant from the mortality event, were generally not informative. However, when these same risk factors were measured closer to the timing of mortality (i.e., average 3.04 years from the event instead of 11.01 years from the event), several emerged as significantly associated with an increased risk of mortality. A comparison of the baseline model and shelf-life models using Harrell's C-indices also indicates an increase in performance of the shelf-life model.
Specifically, higher levels of substance use increased mortality risk (the unanticipated protective effect of mental health instability is discussed in the next section). The emergence of substance use as a significant predictor only when measured closer in time to the mortality event supports the shelf-life hypothesis (Vincent & Grisso, 2005). This hypothesis posits that risk factors lose their predictive validity over time. Therefore, it is important to update risk assessments as individuals may fall out of risk when earlier issues resolve or become less relevant, rendering historical profiles that are less informative.
Cox regression with time-varying covariates was used to evaluate the impact of dynamic change in risk factors on early mortality. This approach differed from the shelf-life model by accounting for all reassessments of dynamic factors as opposed to only the assessment in closest temporal proximity to the outcome of interest. Using this approach, higher levels of antisocial attitudes emerged as significantly associated with increased mortality risk. The emergence of antisocial attitudes as a theoretically consistent risk factor for mortality in the dynamic change model but not the shelf-life model implies that the relevance of a certain risk factor to early mortality may only be detected if examined through the appropriate lens. The dynamic change model, which uses repeated measurements, is suited especially for instances where acute risk factors (i.e., those that may change over shorter windows of time; Etzler & Rettenberger, 2019) increase the risk of early mortality. The measurement of antisocial attitudes in the current study may reflect the type of hostility considered to be an acute factor (see Hanson & Harris, 2007) that is subject to quicker changes (e.g., following incarceration, connection to new peer group, response to intervention) that need to be captured from a dynamic perspective.
Risk Factors Associated with Early Mortality
Substance use has been consistently recognized as a major risk factor for early mortality (Binswanger et al., 2020; Chen et al., 2010; Kinner et al., 2015; Kullgren et al., 1998; Teplin et al., 2014). Looking more closely at this relationship, we found that it might be too simplistic to claim that lifetime substance use matters for early mortality. Instead, public health policies aiming to disrupt the link between substance use and mortality should consider those with recent substance use issues as especially high-risk. These findings are particularly salient given the ongoing opioid epidemic in North America, which has contributed to substantial increases in overdose deaths and disproportionately affects criminal legal system-involved populations (Binswanger et al., 2007; Kariminia et al., 2007; Merrall et al., 2010).
The protective effect of mental health instability on mortality contrasts with existing research, which has typically found that individuals with psychiatric diagnoses are at elevated mortality risk (Sailas et al., 2006; Stenbacka et al., 2012). One explanation for this unanticipated finding is the visibility of higher needs in individuals with these risk factors. Individuals who display emotional dysregulation are more likely to trigger clinical concern, receive psychiatric referrals, or be placed under intensive supervision (Swartz et al., 1998), all of which may decrease mortality risk. Unfortunately, the current study lacked data on the level of resources each participant received from the criminal legal system.
Antisocial attitude emerged as a significant risk factor only within the dynamic perspective. Antisocial attitudes have been shown to be predictors for reoffending (Andrews et al., 1990; Mills et al., 2004), which in turn are linked to greater risk of violent deaths (Kariminia et al., 2007; Lattimore et al., 1997; Paanila et al., 1999). Antisocial attitudes may be context-dependent, such as being exacerbated by greater exposure to others with antisocial attitudes during incarceration, or from being frustrated by reintegration challenges (e.g., obtaining housing or employment). Conversely, new intimate relationships or obtaining legitimate employment may encourage more prosocial attitudes (Laub & Sampson, 2001; Maruna, 2001).
Consistent with existing research, conviction rate was also positively associated with mortality risk, further supporting a robust offending–mortality relationship evident in literature (Lidberg et al., 1989; Pritchard et al., 1997; Skinner & Farrington, 2020; Teplin et al., 2014). Conversely, the total number of risk assessments was associated with a reduced risk of mortality. Assessment frequency is expected to be positively related with offending, because risk assessments are routinely performed by probation officers as part of case planning and management, and therefore continued offending should result in more assessments. However, number of risk assessments and conviction counts were only moderately correlated (r = 0.56), suggesting that assessment frequency is not merely a proxy for offending. Instead, this inverse association may reflect other aspects of heightened system contact, which could attenuate mortality risk, such as closer supervision and monitoring, or more diligent and proactive probation officers. Increased contact likely facilitates higher levels of service engagement and identification of unmet needs, creating opportunities for target interventions (e.g., referrals to detox programs, housing assistance, medical care) that ultimately mitigate mortality risk.
Implications for Criminal Legal System Practices
Although the CRNA was not designed to identify a person's risk for mortality, its associations with offending in other studies (e.g., McCuish & Lussier, 2023) and mortality in this study reinforce the long-recognized overlap between offending and mortality. Results from the shelf-life and dynamic change models point to the importance of reassessment to maintain an accurate understanding of an individual's current risk profile and to inform relevant interventions. Acute dynamic risk factors are liable to change over short intervals. Without reassessment, outdated evaluations may obscure important needs.
Beyond simply capturing a new level of risk, reassessments should track whether a risk factor has increased or decreased relative to previous assessments. Findings from the first-differenced model suggest that it is not only the level of a risk factor but also its change over time (e.g., worsening antisocial attitudes) that indicate an increased risk of mortality. Integrating change-sensitive assessments into correctional practice would allow practitioners to intervene earlier, potentially preventing further deterioration from moderate to high risk, and reducing the likelihood of adverse outcomes.
Given the strong link between substance use and mortality (Kinner et al., 2020; Lidberg et al., 1989; Stenbacka et al., 2012), evidence-based substance use interventions should be prioritized within criminal legal systems. Because substance use is a risk factor for both offending and early mortality (Zane et al., 2019), targeted treatment programs can simultaneously address both public health and public safety concerns. Incorporating substance use treatment into community re-entry planning, probation supervision, and institutional programming could improve long-term outcomes and interrupt cycles of addiction, offending, and health deterioration.
Although incarcerated youth represent a relatively small fraction of the overall youth population, they are among the most vulnerable to early mortality, which warrants focused research and policy attention. Prior research has shown that criminal legal system-involved youth face significantly higher rates of mortality compared to their non-system-involved peers, particularly due to homicides and suicides (Aalsma et al., 2016; Lindberg et al., 2017; Zheng et al., 2023). These elevated risks persist into adulthood (Skardhamar & Skirbekk, 2013; Teplin et al., 2014), suggesting long-term consequences of early criminal legal system involvement. Avoiding research on this population risks overlooking a group for whom well-timed interventions could reduce preventable deaths and mitigate long-term harms. While no single agency is currently mandated to monitor or reduce mortality among criminal legal system-involved individuals, correctional systems regularly administer risk assessment instruments that identify the very factors shown here to predict early death. Correctional agencies internationally have implemented the risk-need-responsivity model, which targets dynamic criminogenic needs, such as substance use and antisocial attitudes, through cognitive-behavioral interventions (Andrews & Bonta, 2015; Andrews et al., 1990). Agencies that target criminogenic needs in the interest of reducing reoffending are therefore, by extension, already reducing mortality risk whether or not that is an explicit goal. Making mortality reduction an explicit correctional goal would not require systemic changes, but simply a recognition of what existing practice already has the capacity to achieve. For some youth agencies (e.g., Ministry of Children and Family Development in British Columbia), the goals of child well-being and youth corrections already coexist within a single mandate, demonstrating that public safety and health outcomes can be pursued together within the same organization.
Limitations and Future Research
As CRNAs are administered only during periods of supervision, individuals who desist from offending or otherwise refrain from having criminal legal system contact have fewer assessments. As a result, both the shelf-life model, which used the last available risk assessment, and the dynamic change model, which incorporated all available risk assessments, are more sensitive to risk patterns among individuals with prolonged system involvement. Therefore, mortality risk may be underestimated for individuals with shorter or less visible supervision histories, even if they continue to experience significant adversity. On average, participants’ last CRNA occurred 3.10 years prior to death or 7.11 years prior to the end of follow-up (for nondeceased), indicating that this limitation may have introduced greater bias for participants who did not die during the observation period.
The finding that the last assessment outperforms the first may not solely indicate that the person has changed over time, but may also reflect what could be termed a familiarity hypothesis: that repeated contact between a probation officer and the same individual produces more accurate assessments over time, as the officer develops a deeper understanding of the individual's background and circumstances. Therefore, improvement in predictive accuracy may reflect greater assessment reliability. These explanations are not mutually exclusive, but they carry different theoretical implications: one pointing to reassessment as a mechanism for capturing genuine risk change, and the other highlighting the role of assessor familiarity in producing accurate risk assessments. Future research could disentangle these mechanisms by examining whether predictive accuracy improves more rapidly when the same probation officer conducts repeated assessments compared to when different officers assess the same individual.
This imbalance in the CRNA data connects to a broader conceptual concern about the interpretation of individual-level risk factors. Items indexed in the CRNA reflected individual-level risk factors. However, these factors may instead serve as proxies for structural disadvantage, including systemic poverty, residential segregation, inadequate access to healthcare, and cumulative exposure to institutional neglect. The current study did not account for the broader social environment (e.g., social networks, the schools they attend, where they live, quality and access to healthcare in their jurisdiction). Accounting for such factors may change the interpretation of the contribution of individual-level risk factors to early mortality. Future research should address this limitation by integrating contextual variables, such as through multilevel models and data linkage projects. Also missing from the CRNA was direct measures of self-control and other individual-level risk factors more appropriate for testing questions about the impact of antisocial propensity on early mortality (Tremblay & Pare, 2003).
In the current study, mental health instability unexpectedly decreased the risk of early mortality, which is inconsistent with the majority of literature (Kullgren et al., 1998; Sailas et al., 2006; Siponen et al., 2023). This discrepancy may reflect differences in how mental health was measured. In this study, mental health was measured through a risk assessment item, while other studies typically use formal psychiatric diagnoses (e.g., Kullgren et al., 1998; Stenbacka et al., 2012). Measuring mental health in different ways could result in different correctional system responses to mental health issues. For instance, individuals with diagnosed psychiatric disorders are more often placed into solitary confinement (Clark, 2018; Stewart & Wilton, 2014), which may in turn exacerbate mortality risk (Wildeman & Andersen, 2020). Meanwhile, changes in mental health deterioration as indicated by repeated risk assessments may trigger responses and interventions that reduce mortality risk. Furthermore, formal diagnoses are made by psychiatrists, while probation officers complete CRNAs. Both groups differ in training and experiences with individuals who struggle with mental health, which may result in different perceptions of what mental health instability looks like. To explore the potential impact of correctional system staff on mortality, a next step is to analyze whether probation officers’ discretionary responses to perceived instability acts as a protective intervention. For example, future research could investigate if higher CRNA scores trigger escalation in supervision, such as increased home visits or program referrals.
Conclusion
This study followed a cohort of 1,155 formerly incarcerated Canadian youth into adulthood to examine the relationship between risk factors and early mortality. The same risk factor can be modeled in different ways, and the current study explored the ways in which the likelihood of mortality was impacted by a person's level of risk at baseline assessment, their level of risk closest to the outcome of interest (shelf-life hypothesis; Vincent & Grisso, 2005), and their change in level of risk. The results were most supportive of the shelf-life and dynamic change models. Consistent with the “shelf-life” hypothesis (Vincent & Grisso, 2005), earlier baseline measurements of risk factors did not predict mortality, while those assessed closer to the time of death were significantly associated with increased mortality risk. Specifically, greater substance use increased mortality risk, while mental health instability unexpectedly decreased mortality risk. The dynamic change model, which used time-varying covariates to evaluate the effects of changes in risk factors over time with first-differenced scores, found that within-individual increases in antisocial attitudes were associated with elevated mortality risk. These findings highlight the importance of repeated assessment and the value of modeling change over time when examining mortality among legal system-involved populations.
Supplemental Material
sj-docx-1-jrc-10.1177_00224278261459468 - Supplemental material for Beyond Risk Level: Timing and Change in Risk Factors as Predictors of Early Mortality Among Formerly Incarcerated Youth
Supplemental material, sj-docx-1-jrc-10.1177_00224278261459468 for Beyond Risk Level: Timing and Change in Risk Factors as Predictors of Early Mortality Among Formerly Incarcerated Youth by Jen-Li Shen and Evan C. McCuish in Journal of Research in Crime and Delinquency
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada (grant number 435-2020-0150).
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.