
Abstract
The purpose of the current study was to evaluate the turn-taking skills of children with and without disabilities who participated in a social communication intervention targeting peer-directed initiations and responses. Eight children met the selection criteria for inclusion in the study. A multiple baseline design across participants (dyads) was used to determine the effects of the social communication intervention. All eight participants showed increases of initiations with an immediate peer response. Follow-up assessments showed that the effects were maintained in the return to baseline condition but did not generalize into the classroom setting. Classroom teachers found the intervention procedures and the behavioral changes in participants to be socially valid. Several implications for practice can be derived from the findings of the present study.
Social competence is defined as the ability to initiate, develop, and maintain satisfying relationships with adults and peers (Odom, McConnell, & Brown, 2008). Through building and sustaining various types of social relationships and experiences, children acquire knowledge of essential developmental abilities such as social, language, and cognitive competencies that become a critical focus when children make the transition from preschool to kindergarten. Critical skills children need to know for a successful transition to kindergarten include letter identification, number sense, sharing, following rules and directions, and playing appropriately with peers and classroom materials (Missall & Hojnoski, 2008).
After learning the link between social competence and later school achievement, the National Research Council (2000) called for an increased focus on developing effective, evidence-based strategies to promote children’s social-emotional competence and healthy development. Demographic and socioeconomic changes during the past 30 years have resulted in increased risk factors affecting young children, thus placing a tremendous burden on preschool programs to meet children’s needs (Fantuzzo et al., 1996). Early childhood leaders have advocated for the development of validated prevention and intervention packages to address young children’s emotional and behavioral needs, to foster their development of social competence, and to promote their resilience and future success (Lopez, Tarullo, Forness, & Boyce, 2000; Yoshikawa & Zigler, 2000). Such efforts, however, are predicated on the assumption that preschool teachers recognize the value of promoting social-emotional skills and regularly address these skills in their classrooms. If preschool teachers are to understand and improve children’s social competence, they need specific intervention strategies to address these skills in their classrooms during sociodramatic play.
Sociodramatic play is a type of group pretend play with a common goal or theme (Bagley & Klass, 1997). Typically, preschool programs provide opportunities for sociodramatic play during center time in the classroom schedule. Many classrooms support sociodramatic play by providing a house center in which primary props include kitchen equipment (e.g., stove, refrigerator), kitchen utensils (e.g., dishes, cooking equipment), and baby dolls (Bagley & Klass, 1997). Occasionally, classrooms also include thematic play themes such as doctor, construction, and grocery store. Teachers assume that availability of these toys will be beneficial for all children in the setting including those with disabilities. However, Nabors, Badawi, and Cheney (1997) showed that children with disabilities spent the least amount of time in cooperative peer play, interacted more with teachers, and spent more time in sociodramatic centers that were teacher directed. Intervention strategies to promote successful peer interactions in the context of sociodramatic play may be needed for young children who demonstrate challenges in this area.
Intervention strategies targeting children with disabilities in the preschool classroom are often referred to as naturalistic intervention strategies (Rule, Losardo, Dinnebeil, Kaiser, & Rowland, 1998) because they are implemented within the context of routine classroom activities. Naturalistic intervention strategies have been effective for many preschoolers with disabilities (see Brown, McEvoy, & Bishop, 1991; Brown & Odom, 1994; Frea, Craig-Unkefer, Odom, & Johnson, 1999), but these interventions are not always sufficient to promote social interactions between peers for all children with disabilities. Children with social communication disorders, in particular, may need more explicit, structured, and intensive interventions to improve peer interactions and peer relations. These children may not have the essential language skills to make peer interactions meaningful and effective, they tend to be less preferred play partners, and they tend to be lonelier than their typical peers (Schneider & Goldstein, 2008). Targeted social communication skills in explicit social skills interventions include sharing, initiating, play organizing, and responding to a peer (Odom & McConnell, 1993).
Social integration activities are one form of explicit social skills intervention strategies found to be effective with preschoolers with disabilities, including those with social communication delays. Social integration activities include four components (Odom et al., 1988): (a) the selection of children with a disability and socially responsive peers willing to participate in teacher structured play activities, (b) the implementation of social activities in a defined play center for 5 to 15 min, (c) the selection of play activities that encourage positive play and peer interactions, and (d) the introduction of play themes and prompting of interactions between children. Frea and colleagues (1999) compared whether a naturalistic intervention or a social integration activity intervention was more effective in increasing the social interactions of two young children with disabilities. One child responded more positively to the social integration activity intervention, whereas the second child responded more favorably to the naturalistic intervention. The authors concluded that the differences within the individual children may account for the obtained results. Robertson and Weismer (1997) matched 20 children with language delays with 10 typically developing peers and randomly assigned them to either a treatment or a control group. The children in the experimental group participated in four 15-min groups in a house theme play environment. The children with language delays were paired with different peer models for each play group. Peers in both groups were asked to play with designated toys without adult directions or prompting. Following intervention and a 3-week follow-up, the children in the experimental group produced significantly more words, different words, and play-theme-related acts between the two children.
Buddy skills training is another explicit social skills intervention often used with children with disabilities. In buddy skills training, teachers train children with and without disabilities in specific social behaviors and strategies to promote future peer interactions (Brown, Odom, McConnell, & Rathel, 2008). English, Goldstein, Shafer, and Kaczmarek (1997) implemented a peer intervention that taught typically developing peers the strategy “stay, play, and talk” with your buddy. Specifically, peers were taught to move into proximity to children with disabilities, say the child’s name to obtain his or her attention, and maintain proximity while talking and playing with the child. Teachers served as buddy coaches by monitoring the children’s social interactions during play and providing prompts to the typically developing peer as needed to promote social interactions between the dyad. The buddy skills intervention package was effective in improving the social communication skills (e.g., verbal requests, comments) of young children with disabilities. A similar study was conducted by Goldstein, English, Shafer, and Kaczmarek (1997). Children with disabilities improved their social communication skills as a result of the buddy skills training and also improved their sociometric status—a finding not demonstrated in the English et al. (1997) study.
Turn-taking skills are frequently targeted in explicit social skills interventions for young children with disabilities. Turn taking refers to “smooth interchanges between communicative partners” (Kaczmarek, 2002, p. 90). Characteristics of skilled turn taking include (a) rapid turning, where each turn begins a microsecond before the previous one ends; (b) avoidance of overlaps, interruptions, and dysfluencies (e.g., no interruptions of turns, only one speaker at a time); (c) observance of obligations to respond; (d) observance of obligations as a listener (e.g., display attentiveness, indicate comprehension or lack thereof, and give the speaker an opportunity to speak); and (e) topic relatedness, utterances should relate to their predecessor’s utterances (Ninio & Snow, 1996). Successful turn taking requires children to maintain their turn, often more challenging to do when interacting with peers than with adults. Sociodramatic play scripts have been used with preschool age children to improve turn taking during free play (Doctoroff, 1997; Goldstein & Cisar, 1992; Goldstein, Wickstrom, Hoyson, Jamieson, & Odom, 1988). Scripts are developed that contain specific motor and gestural or verbal responses to use in specific sociodramatic play sessions (e.g., hamburger stand), and children are taught in groups or individually to follow the scripts during play. During the play sessions, adults prompt children to stay in their roles or to provide specific responses.
The purpose of the current study was to evaluate the turn-taking skills of children with and without disabilities who participated in a social communication intervention targeting peer-directed initiations and responses. The current study was motivated by scientific and practical reasons—to better understand how a social communication intervention affects turn-taking skills in preschoolers, if the results are maintained in follow-up observations, and whether preschool teachers rated the intervention procedures as acceptable and produced socially important changes in behavior. This study pursued three research aims. The first aim was to examine the effects of a social communication intervention on children’s initiating play and conversation with a peer and this initiation receiving an immediate peer response. Several intervention studies targeting similar skills (Beilinson & Olswang, 2003; Craig-Unkefer & Kaiser, 2002, 2003; Stanton-Chapman, Denning, & Jamison, 2008; Stanton-Chapman, Jamison, & Denning, 2008; Stanton-Chapman, Kaiser, & Wolery, 2006; Thiemann & Goldstein, 2004; Timler, Olswang, & Coggins, 2005) tallied the number of initiations delivered by the target child to a peer regardless of the outcome (whether or not the peer responded to the target child). For the current study, the primary focus was initiations that were followed by an immediate peer response. The second aim was to investigate whether intervention effects were maintained to a condition similar to that of the baseline condition and in the classroom. Although previous research (e.g., Goldstein et al., 1988) has not successfully demonstrated generalization, we were hopeful that our instructional strategies would elicit results that would extend into the classroom context. The third aim was to explore the social validity of intervention findings: (a) Did preschool teachers find the intervention procedures to socially acceptable? and (b) Did preschool teachers rate the behavior changes as socially important? Hanley, Heal, Ingvarsson, and Tiger (2007) reported that using a classwide approach to teach prosocial skills (e.g., instruction following) during typical classroom activities was effective and rated highly by teachers. The program resulted in a more than fourfold increase in children’s social skills and a 74% reduction in problem behavior.
Method
Participants
Sample
All children (N = 18) enrolled in a preschool classroom at one rural elementary school were screened for possible participation in the study. Parent consent to participate was obtained following the guidelines of the university’s institutional review board. All children were screened for problem behavior, poor social skills, and language delays. Teachers were asked to complete the teacher form of the Child Behavior Checklist (CTRF; Achenbach, 1997) and the teacher form of the Social Skills Rating System (SSRS; Gresham & Elliott, 1990). Children were assessed on the Preschool Language Scale–4 (PLS-4; Zimmerman & Pond, 2002).
Criteria for participant inclusion
Participants were selected based on one or more of the following criteria: (a) children were 3, 4, or 5 years old at the introduction of the study, (b) they scored at least one SD below the normative mean (a total standard score of 80 or below) on the total language score of the PLS-4 (Zimmerman & Pond, 2002), (c) they were rated by teachers to have clinical levels of problem behavior (either internalizing or externalizing; a total score of 60 or above on either scale) on the CTRF (Achenbach, 1997), and/or (d) they demonstrated poor social skills (a Total Social Skill subscale score of 85 or below) as indicated by the teacher report on the SSRS (Gresham & Elliott, 1990). Children selected were considered at risk for language delays, problem behavior, or poor social skills. Children were excluded from participation if they had significant sensory impairments or a previous diagnosis of mental retardation or pervasive developmental disorder.
Eight children met the selection criteria for inclusion in the study. Children A1, B1, C1, and D1 were receiving special education services at the onset of the study under the categories of developmental delay or specific language impairment based on individualized education programs (IEPs) from the 2006-2007 school year. The children were assigned to dyads based on a predetermined protocol. First, the children had to meet the criteria for participant inclusion discussed previously. Second, each dyad had to consist of one child with an IEP and one child without an IEP. Third, both children had to be available during free play on the same days and times. Children requiring speech and language therapy were often seen by the speech-language pathologist during free play. Many children without IEPs were enrolled in the program on a part-time basis, so these children had to be present at the same time as the child with an IEP. Finally, attempts were made to pair the children by birthday. Six children were placed in same-gender dyads, and Dyad D was a girl–boy dyad. The characteristics of the eight children are presented in Table 1.
Characteristics of Participants
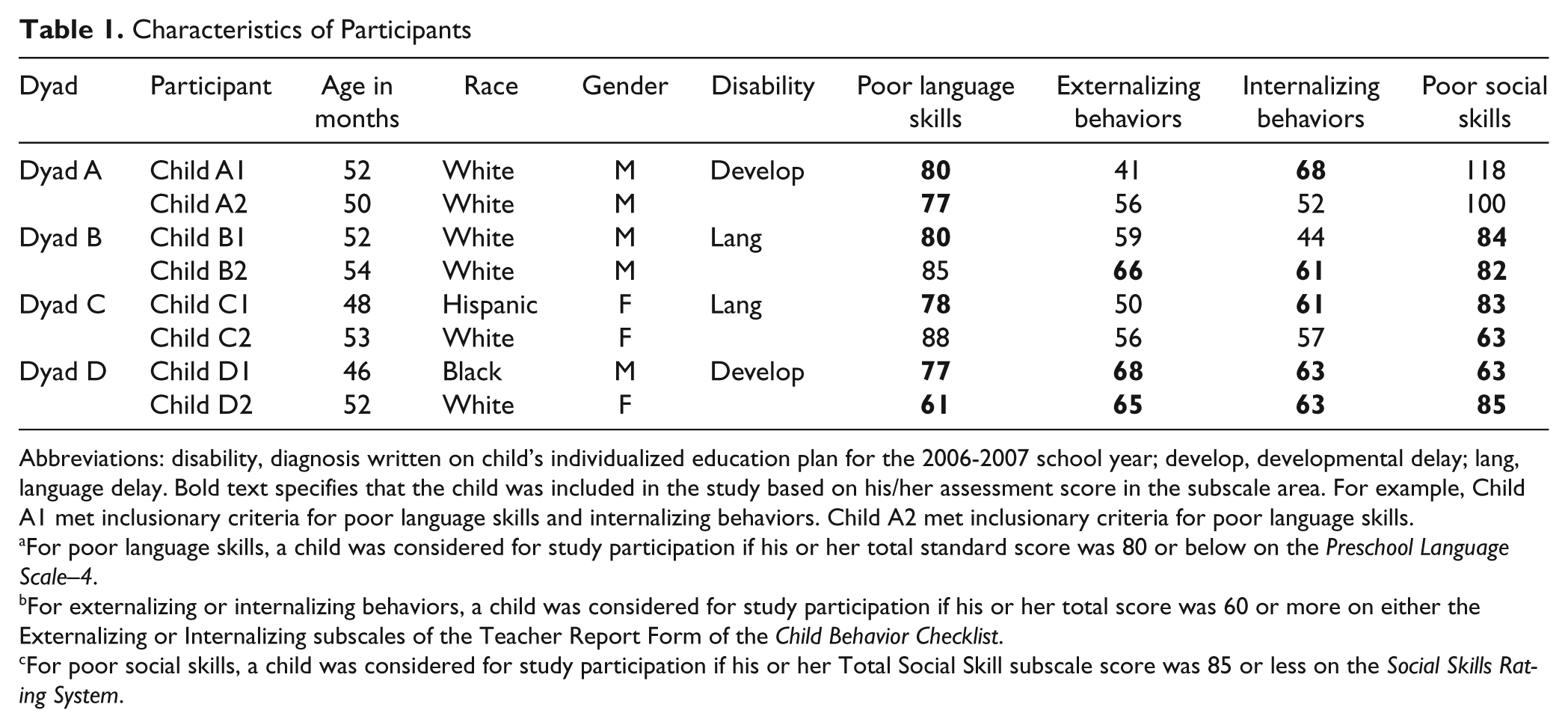
Abbreviations: disability, diagnosis written on child’s individualized education plan for the 2006-2007 school year; develop, developmental delay; lang, language delay. Bold text specifies that the child was included in the study based on his/her assessment score in the subscale area. For example, Child A1 met inclusionary criteria for poor language skills and internalizing behaviors. Child A2 met inclusionary criteria for poor language skills.
For poor language skills, a child was considered for study participation if his or her total standard score was 80 or below on the Preschool Language Scale–4.
For externalizing or internalizing behaviors, a child was considered for study participation if his or her total score was 60 or more on either the Externalizing or Internalizing subscales of the Teacher Report Form of the Child Behavior Checklist.
For poor social skills, a child was considered for study participation if his or her Total Social Skill subscale score was 85 or less on the Social Skills Rating System.
Setting
The study took place in a rural elementary school serving preschoolers. All participants were enrolled in the same classroom. This classroom was collaborative in nature—meaning the program provided services to children at risk (Head Start) and children with special needs (early childhood special education; ECSE). Four teachers provided instruction within the classroom: (a) an at-risk teacher with a master’s degree in early childhood, (b) an ECSE teacher with a master’s degree in ECSE, and (c) two assistant teachers with child development associate’s degrees.
Baseline, intervention, and follow-up sessions took place in an empty classroom that was used for small group activities and meetings. All sessions took place in the morning during the classroom’s free play.
Materials
Play materials used in the baseline and intervention sessions were based on five dramatic play themes—grocery store, doctor, construction, animal doctor, and hair salon–barber. Each dramatic play theme had an accompanying storybook that provided instruction on the intervention’s target behaviors. The storybooks were designed to include pictures of participating children and the exact materials and props used during the intervention sessions. The books were computer generated using a digital camera and a template for the book format (interventionists inserted pictures of study participants into the storybooks and entered the names of the children in the story’s text). The storybooks (a) told a story that illustrated thematic play (e.g., a visit to the grocery store), (b) included models for verbalization during role playing (e.g., the grocery worker says, “Can I help you?”), (c) included specific theme vocabulary (e.g., money, cart), and (d) emphasized five social communication strategies (to be discussed later) illustrated in the stories with picture icons that served as visual cues to assist children in recalling the strategies (i.e., initiations and responses).
The thematic play materials were similar to the types of toys and activities available in preschool classrooms. Play materials matched pictures in the storybooks. To ensure that the materials were culturally appropriate and ethnically valid to many cultures (Barnett, Bell, & Carey, 1995), research staff and classroom teachers of various ethnic backgrounds assisted in selecting toys that were representative of several cultures. For example, in the hair salon–barbershop theme, toys included African American hair products such as empty bottles of detangling moisturizer and crème hair dress.
Study Personnel
Child interventionists
Two child interventionists conducted the baseline, intervention, and follow-up sessions. The first interventionist (first author) has educational degrees in early intervention and ECSE and 12 years of experience teaching children at risk and children with disabilities. The second interventionist (second author) has educational degrees in special education, 8 years of experience teaching children with disabilities in inclusive settings, and several years experience as a consultant providing educational services to children in the classroom.
Research staff
Transcribers and coders for observational data, treatment fidelity measures, and reliability coding were master’s degree students in ECSE. All research staff held bachelor’s degrees in psychology and had practicum hours in early childhood, at-risk, and ECSE classrooms. To reduce potential bias, all were blind to the study outcomes.
Social validity evaluators
Evaluators for the social validity measure included three early childhood teachers who held master’s degrees in ECSE. The teachers did not teach at the elementary school where the study took place. Their teaching experience varied from 2 years to 7 years. All teachers were blind to the purpose of the study and experimental conditions.
Experimental Design
A multiple baseline design across participants (dyads) was used to determine the effects of the social communication intervention (Kazdin, 1994). Baseline measures of initiations with a peer response were done simultaneously and continuously under the same conditions to describe current level of performance. The intervention was then applied to the first dyad while baselines were extended and monitored in the remaining dyads. This pattern continued until all dyads had started the intervention condition. Causality was established by the change in one baseline (where the intervention is introduced) when there was no concurrent change in another baseline (where the intervention had not been introduced; Kazdin, 1984). Replication of the results was achieved by applying the treatment to the additional baselines. This design has been found to be especially effective in evaluating interventions targeting an increase of social behaviors (Tawney & Gast, 1984).
Procedures
Baseline
Baseline sessions were conducted two to three times per week until five sessions were completed. Children were pulled from their classrooms and taken in predetermined dyads to an empty classroom that was used for small group activities and meetings. Children were asked to play with the toys in the room. The interventionist did not prompt the children to interact with the toys or peers once the session started. The interventionist intervened only if there was a safety concern where one or both of the children would get hurt. Baseline sessions were 10 min in length and were videotaped using a digital camcorder on a tripod.
Intervention
Intervention sessions were conducted four to five times per week and were approximately 20 to 25 min in length. Each session with a particular dyad used one of the five dramatic play themes (grocery store, doctor, construction, animal doctor, and hair salon–barber) and cycled through all the other themes before repeating the themes a second time. The five dramatic play themes were chosen for two reasons: (a) pilot studies of the current intervention demonstrated that these play themes encouraged social interaction between peers and (b) the play themes incorporated toys and materials typically seen in preschool classrooms. Each intervention session had three parts: (a) the advanced play organizer, (b) the play session, and (c) the review session. We selected the format to resemble the “plan–do–review” sequence used in the High Scope Curriculum (Hohman & Weikart, 2002) and employed in many Head Start classrooms and preschool classrooms including the classroom utilized in the current study. All parts of each session were videotaped using a digital camcorder on a tripod. The intervention was used to teach the following social communication skills: (a) talk to your friend (initiations): verbally initiating a conversation or play episode with a peer (e.g., intelligible utterances, directed to peer, within speaking distance of peer—adjacency), (b) listen then respond to what your friend says (responding): verbally responding to peer verbal initiations with adequate responses (e.g., topic related, intelligible, directed to the peer, not interrupting your friend while he or she is talking, not talking at the same time as your friend), (c) use your friend’s name (use of name): stating a peer’s name to gain his or her attention before talking to him or her, and (d) take a turn and give your friend a turn (turn taking): taking an appropriate number and length of turns in conversation or play (e.g., sufficient turns, not dominating conversation, pausing for peer to talk, taking turns to maintain conversation or play, asking for clarification, providing clarification, not interrupting a peer when he or she is talking).
Advanced play organizer
The advanced play organizer component was approximately 10 min in length and had four parts: (a) instruction of target vocabulary words, (b) instruction of the roles for each theme, (c) reading the storybook and instruction of the social communication strategies, and (d) play planning. The interventionist first taught the target vocabulary words that corresponded to the day’s play theme (e.g., grocery, doctor, construction, animal doctor, barbershop–hair salon) using a direct instruction approach. Initially, the interventionist labeled each object, asked the children to imitate the word, and showed how the object could be used during the play session. In subsequent sessions, the interventionist asked the children to label the object and demonstrate how it could be used. Each theme had a list of approximately 10 words that were taught during the course of the intervention.
The children were then introduced to the roles for each theme (e.g., doctor and patient, barber and customer, grocery worker and shopper). The interventionist used pictures from the storybook to discuss the role the character played in the particular theme. After the interventionist described the roles related to the play theme, she read the storybook to the children. The social communication strategies were taught during the storybook reading. The storybooks were designed so that pages could be added or deleted. As new social communication strategies were introduced in the intervention, the interventionist added those storybook pages to the book. Based on pilot studies evaluating the intervention program described in the current study, the social communication strategies were taught in the following order: initiations (Session 1), responding (starting at Session 3), use of name (starting at Session 8), and turn taking (starting at Session 12).
When the interventionist finished reading the storybook to the children, they planned their play. First, each child selected which role he or she would like to play in the theme. Second, the interventionist reviewed these roles by using the pictures in the storybook (e.g., “The barber cuts the customer’s hair”). Third, the social communication strategies were reviewed by showing the icons and having the children think of opportunities when the strategies could be used during their play (e.g., “The doctor could use the patient’s name and say, ‘How can I help you Laura?’”). Fourth, the interventionist had the children verbally state what they were going to do in the play session (e.g., “I am going to be the animal doctor and I am going to take care of the sick dog”). Finally, the interventionist had the children practice using the social communication strategies (e.g., “Say, ‘Keith I need the hammer’”).
Play session
The children then played with the thematic materials for 10 min. The interventionist first helped the children go into their assigned roles by directing them to the specific items and/or costumes (e.g., aprons for grocery workers, lab coats for doctor) related to the roles. The interventionist sat in the play area with the children but did not get directly involved with their play. The interventionist recorded data on each child’s use of target vocabulary words and use of the social communication strategies during the play session for use in the review session. The interventionist would discreetly tally on paper each time a child used a target vocabulary word or a social communication strategy. In addition, specific examples of when the children elicited social communication behaviors or used target vocabulary words were recorded for use in the review session.
The interventionist also prompted children (a) to engage in the thematic play activity, (b) to use target vocabulary words, and (c) to interact using the social communication strategies. Prompts for the social communication strategies included prompts to sit next to a peer, to initiate an interaction, to listen to a peer and then respond, to take a turn, and to use a peer’s name to obtain his or her attention. Prompting to initiate, for example, was provided as needed to individual children, once the children were in proximity to one another but were not talking. If children were not adjacent to one another, they were first prompted to sit next to one another. The interventionist used a system of least prompts that first employed an opportunity to respond without prompting, followed as needed by simple verbal prompts, and finally followed as needed by verbal plus gestural prompts. Additional prompting was provided when the children were in proximity to one another but were not talking. Prompts were given following several specific rules. If a child did not engage in one of these behaviors after approximately a minute of play, the interventionist provided a simple verbal prompt (“Sit by Timmy”; “Say, ‘Keith I need the hammer”). The interventionist waited 5 s for compliance and praised the child when he or she complied with the prompt. If the child did not comply within 5 s, the interventionist repeated the verbal prompt with gestures (“Sit by Timmy” and pointed to a location closer to the peer; “Say, ‘Keith I need the hammer” and pointed to the hammer) and then praised the child when he or she complied. If the child still did not comply with the second prompt, the interventionist said the words or performed the action for the child but did not give praise.
The prompts were delivered at a rate of about one prompt per minute at times when no social interactions were occurring between the children. This translated to 8 to 15 prompting episodes during each intervention session. This rate of prompting was established based on the overall purpose of the intervention, which was to encourage child-to-child interaction using the social communication strategies and target vocabulary words during play. The goal was to have a rate of prompting that was sufficient to promote the acquisition of target behaviors but that was not disruptive to child-to-child interactions.
Review session
At the conclusion of the play session, the children moved away from the play area and reviewed their performance in the play session with the interventionist. The review session was approximately 5 min in length. First, the interventionist reviewed the thematic roles with the children. Second, the interventionist reviewed the use of target vocabulary words with the children. Finally, the interventionist reviewed the children’s use of the social communication strategies. This review questioning was based on which strategies had been taught at each point in the intervention. For example, if the children had been taught the social communication strategies of initiation, listen then respond, and use of name, then only these strategies would be reviewed in the review session.
Follow-up sessions
Follow-up sessions were conducted at the conclusion of the intervention. Two types of follow-up sessions were conducted. For the first follow-up session, the process was similar to the baseline condition. The dyads were brought to an empty classroom that was used for small group activities and meetings and were directed to play with the toys provided—the thematic toys that appeared in the baseline and intervention conditions. The session was 10 min in length, and no prompts, directions, or feedback were given. For the second follow-up session, the children were observed playing with their peers in the classroom. No prompts, directions, or feedback were given to the children.
Measurement
Measurement included language, behavioral, pragmatic, and social assessments before and after the intervention, observational measures of child performance, and treatment fidelity measures. Interobserver agreement reliability was assessed on observational and treatment fidelity measures for 20% of the sessions. Social validity was assessed at the conclusion of the study.
Data collection
Data collection procedures for baseline, intervention, and follow-up conditions followed four steps. First, videotaped sessions were downloaded from the video camera onto the computer. Second, the 10-min baseline sessions and the 10-min play sessions were transcribed word for word by research staff using Systematic Analysis of Language Transcripts software (SALT; Miller & Chapman, 1985). Research staff were trained to a criterion of 90% for five successive practice sessions—meaning their transcriptions were 90% reliable with a second transcription coder. Third, the interventionist then verified the transcripts of their baseline and intervention sessions for accuracy. Finally, the videotapes of the sessions were reviewed, and the transcribed sessions were further coded by trained research staff using the Peer Language and Behavior Code (PLBC; Stanton-Chapman, Kaiser, Vijay, & Craig-Unkefer, 2003). Similar to transcription procedures, coders were trained to a criterion of 90% for five successive practice sessions. Coders were not informed about the purpose of the study or the experimental condition of the videotapes they coded. Reliability standards were established (refer to Interobserver Agreement for more information), and a second coder was used to provide this check.
Child communication measures
The PLBC (Stanton-Chapman et al., 2003) was employed to measure verbal and nonverbal interactions between children with or without adult prompting during the play session. The PLBC has two nonverbal and four verbal categories for child behaviors. The nonverbal categories include negative physicals and physical acknowledgements. Physically negative behaviors were physically aggressive acts directed at an object or person. Physical acknowledgements were actions (e.g., head nods, giving a toy to a peer with no verbal response) performed as a result of a request given by a peer. For example, if a peer says, “Do you want this hammer?” and the target child nods his or her head indicating yes, then the target child’s response was considered a physical acknowledgement.
The four verbal categories on the PLBC were negative behaviors, descriptive behaviors, request behaviors, and miscellaneous behaviors (Table 2). Each verbal category was further subdivided into additional social communication behaviors. Negative behaviors included boasting statements, name calling, bribes, threats, negative comments to a peer, and aggressive statements directed toward the peer. Descriptive behaviors included comments, play organizing statements, acknowledgement responses, and praises. Request behaviors included requests for information, yes–no questions, and requests for nonverbal behavior (e.g., action requests, verbal signaling, stop-action requests). Miscellaneous child behaviors included repeats of a peer’s utterance, verbal others (e.g., whining, nonspeech sounds such as the sound effects of toys as interpreted by the child), play verbalizations, off-camera remarks, and unintelligible utterances. (Definitions of the target behaviors are available by request but are not provided because of space constraints.)
Peer Language and Behavior Definitions
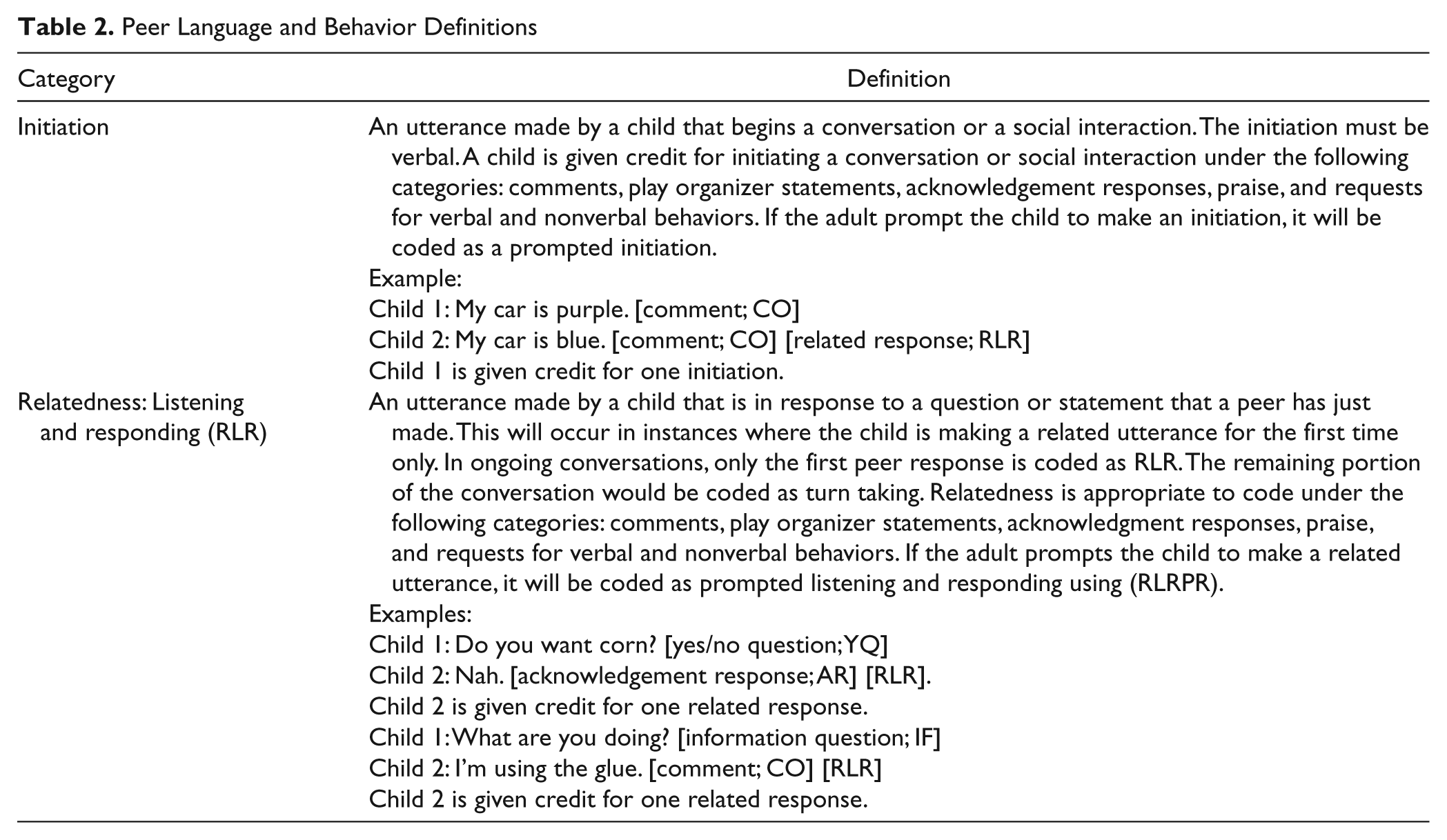
Initiating and responding
The dependent variables in the current study were initiations and responses. An initiation or response was counted if a child initiated a verbal or nonverbal social interaction with a peer and the peer responded appropriately using a verbal or nonverbal response. This is illustrated in the following example:
Can you help me? (Child 1 is counted for one initiation)
Yeah, I will. (Child 2 is counted for one response)
Unsuccessful initiations (those not resulting in a peer response) were not counted. This is illustrated in the following example:
Can you help me? (Child 1 is counted for an unsuccessful initiation)
gives no response.
Because successful initiations required a peer response, this measure is considered to be more conservative than simply tabulating the frequency of child initiations.
Procedural Fidelity Measures
Preparation of intervention materials, advanced play organizer and review session procedural fidelity
To determine if the intervention procedures were implemented as described, fidelity of treatment checklists were completed for 20% of the intervention sessions randomly selected. Videotapes of the entire session were viewed and scored by a research staff member (other than the interventionist) who was blind to the outcomes of the study. The criterion for fidelity of treatment was the correct completion of 95% of the prescribed items. Reaching the criterion level indicated that the interventionist organized, described, and demonstrated the toys used in the play theme, read the storybook, discussed and modeled the use of the social communication strategies, attended to the children’s activities during the play session, and reviewed the children’s use of the social communication strategies and target vocabulary words in the review session. Procedural fidelity for preparation of intervention materials, advanced play organizer sessions, and review sessions ranged between 96% and 100% (M = 99%).
Play prompting protocol procedural fidelity
To determine if the prompting protocol was followed by the interventionist, the percentage of correct prompting episodes was examined. Each element of the prompt episode was coded along with the specific behavior being prompted (which social communication strategy and the target vocabulary word). A prompting episode was considered correct if (a) the interventionist delivered a prompt, waited 5 s for compliance, and praised the child when he or she complied with the prompt; (b) the interventionist delivered a prompt, waited 5 s for compliance, repeated the prompt when the child did not comply, and then praised the child when he or she complied; or (c) the interventionist delivered a prompt, waited 5 s for compliance, repeated the prompt when the child did not comply, waited 5 s for compliance, and then said the words or did the action for the child when he or she did not comply. Procedural fidelity for the play prompting protocol ranged between 86% and 100% for the four dyads (M = 96%). The number of prompting episodes during the intervention sessions is provided in Table 3. There were no prompting episodes during the baseline condition for any of the dyads.
Total Number of Prompting Episodes Across Dyads
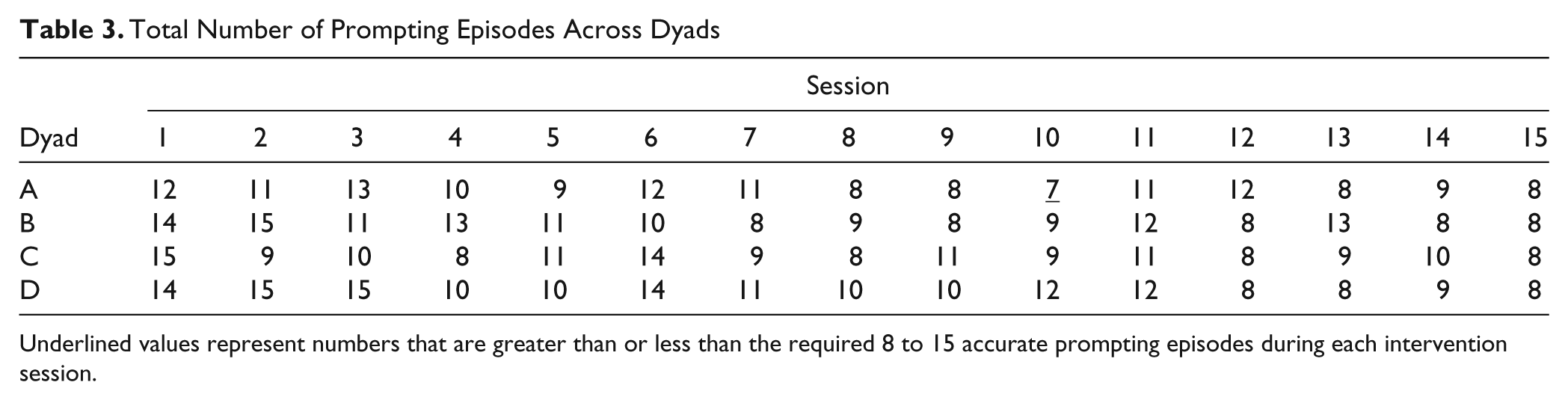
Underlined values represent numbers that are greater than or less than the required 8 to 15 accurate prompting episodes during each intervention session.
Interobserver agreement
Interobserver agreement was calculated on the PLBC (Stanton-Chapman et al., 2003) used to code behavior during baseline and intervention sessions. One research staff member, who was blind to the purpose and outcomes of the study, coded all baseline and intervention sessions. To assess reliability, a second research staff member coded a random selection of 20% of the baseline and intervention sessions. Reliability observations were equally distributed across all four dyads and experimental conditions. Using a computer-based reliability program, SALT Storybook Rely (Tapp, 2003), a sequential comparison of the coded data was made on a point-by-point basis. The program scored an agreement if both coded a behavior and scored a disagreement if they differed on an identified behavior. Reliability was assessed using an exact agreement formula in which the total number of agreements was divided by the total number of agreements plus disagreements and multiplied by 100.
Interobserver agreement was high across all dyads, measures, and experimental conditions. Interobserver agreement for initiations or responses for the baseline conditions averaged 98% (range = 85%−100%). Interobserver agreement for initiations or responses for the intervention conditions averaged 97% (range = 77%−100%). For Dyad A, interobserver agreement for initiations or responses averaged 98% (range = 95%−100%) for baseline conditions and 95% (range = 91%−100%) for intervention conditions. For Dyad B, interobserver agreement for initiations or responses averaged 92% (range = 88%−100%) for baseline conditions and 98% (range = 95%−100%) for intervention conditions. For Dyad C, interobserver agreement for initiations or responses averaged 98% (range = 94%−100%) for baseline conditions and 94% (range = 83%−100%) for intervention conditions. For Dyad D, interobserver agreement for initiations or responses averaged 96% (range = 90%−100%) for baseline conditions and 96% (range = 88%−100%) for intervention conditions.
Social Validity
Three preschool teachers with master’s degrees in ECSE who were blind to the purpose of the study and its outcomes were asked to rate the acceptability of the intervention procedures and whether they thought the intervention had produced socially important changes in behavior. To evaluate the acceptability of the intervention procedures, the teachers were asked to view two randomly selected intervention videotapes from beginning to end. After viewing the videotapes, the teachers were asked to complete a 10-item questionnaire using a 5-point Likert-type scale (4 = agree, 3 = somewhat agree, 2 = neutral, 1 = somewhat disagree, 0 = disagree). Example items include (a) “Overall the intervention procedures were acceptable to me,” (b) “The intervention requires too much time to implement,” (c) “The intervention procedures would be easy to implement in my classroom,” and (d) “The teacher prompting procedures seem reasonable.” Means and standard deviations were calculated to analyze the results.
To evaluate whether the intervention had produced socially important changes in behavior, teachers were again asked to view randomly selected videotapes from each dyad. The teachers viewed 1-min video clips of each dyad in a baseline session and in an intervention session. Clips were taken from the first baseline sessions and the last intervention sessions from each dyad. The order of presentation (baseline condition, intervention condition) was randomly selected, and the teachers could not determine the difference between the two conditions based on the content of the video clips. After watching each video clip, teachers were asked to rate the behavior of the children shown in the video clip using a 10-item questionnaire. Sample statements included (a) “The children in the video clip were initiating with one another,” (b) “The children in the video clip listened while their peer was talking to him or her,” (c) “The children shared toys,” and (d) “The children did not interrupt a peer when he or she was talking.” A 5-point Likert-type scale was used to assess their agreement or disagreement with each item (4 = agree, 3 = somewhat agree, 2 = neutral, 1 = somewhat disagree, 0 = disagree). Means and standard deviations were calculated to analyze the results.
Data Analysis Procedures
Observational data were collected for each session from videotapes. These data were summarized and graphed to examine patterns in the data through visual inspection. Four characteristics were examined: level, mean level, trend, and slope. Level was defined as the change from the last measurement in a phase to the first measurement in the next phase, mean level was defined as the average of the points in one phase compared to the average of the points in the next phase, trend was defined as the direction of the data points within a phase, and slope was defined as the angle of increase or decrease of the data points (Kazdin, 1982). The percentage of nonoverlapping data (PND; Scruggs & Mastropieri, 1994) was calculated to determine the intervention’s effectiveness for children’s initiations with an immediate peer response. PND was calculated by counting the number of data points in the intervention that were higher than the highest data point in baseline, dividing this number of nonoverlapping data points in the treatment series by the total number of data points in the treatment series and multiplying this number by 100 (Kazdin, 1982; Scruggs & Mastropieri, 1994). An intervention with a PND of 90% or greater is considered highly effective, 70% to 90% is considered moderately effective, 50% to 70% is considered mildly effective, and less than 50% is considered ineffective, as effects can be attributed strictly to chance (Scruggs & Mastropieri, 1994).
Results
Children’s Initiated Verbal and Nonverbal Behavior to Peers That Resulted in a Peer Response
The first research question addressed in the study was, what are the effects of the social communication intervention on the number of peer-directed initiations that received an immediate peer response (either verbal or nonverbal)? Changes in verbal and nonverbal initiations to the peer that received an immediate peer response were measured to address this question; the results are shown in Figure 1. Data are presented as the number of initiated verbal and nonverbal behaviors produced during each condition that resulted in a peer response, either verbal or nonverbal. Peer-directed initiations that did not result in a peer response were not included in this analysis. Both children in Dyads A, B, and D showed immediate increases in initiations receiving an immediate peer response with the introduction of the intervention. Dyad D had an increasing trend. The data for Dyads A and B were highly variable, but all data points remained above baseline levels throughout the intervention condition. For Dyad C, the number of initiations receiving an immediate peer response remained near baseline levels for the beginning intervention sessions but showed an accelerating trend throughout the remaining intervention sessions. All four dyads demonstrated a change in level. Mean performance for Dyad A in baseline was 1.00 (Child A1) and 0.80 (Child A2) and was 11.33 (Child A1) and 13.13 (Child A2) in the intervention. For Dyad B, mean performance was 3.86 (Child B1) and 2.43 (Child B2) and 13.67 (Child B1) and 12.67 (Child B2) in the intervention. Mean performance for Dyad C was 3.25 (Child C1) and 1.56 (Child C2) in baseline and 9.20 (Child C1) and 7.80 (Child C2) in the intervention. For Dyad D, mean performance was 0.92 (Child D1) and 1.75 (Child D2) in baseline and 12.54 (Child D1) and 11.87 (Child D2) in the intervention. PND calculations show that the social communication intervention was highly effective for all 10 participants.
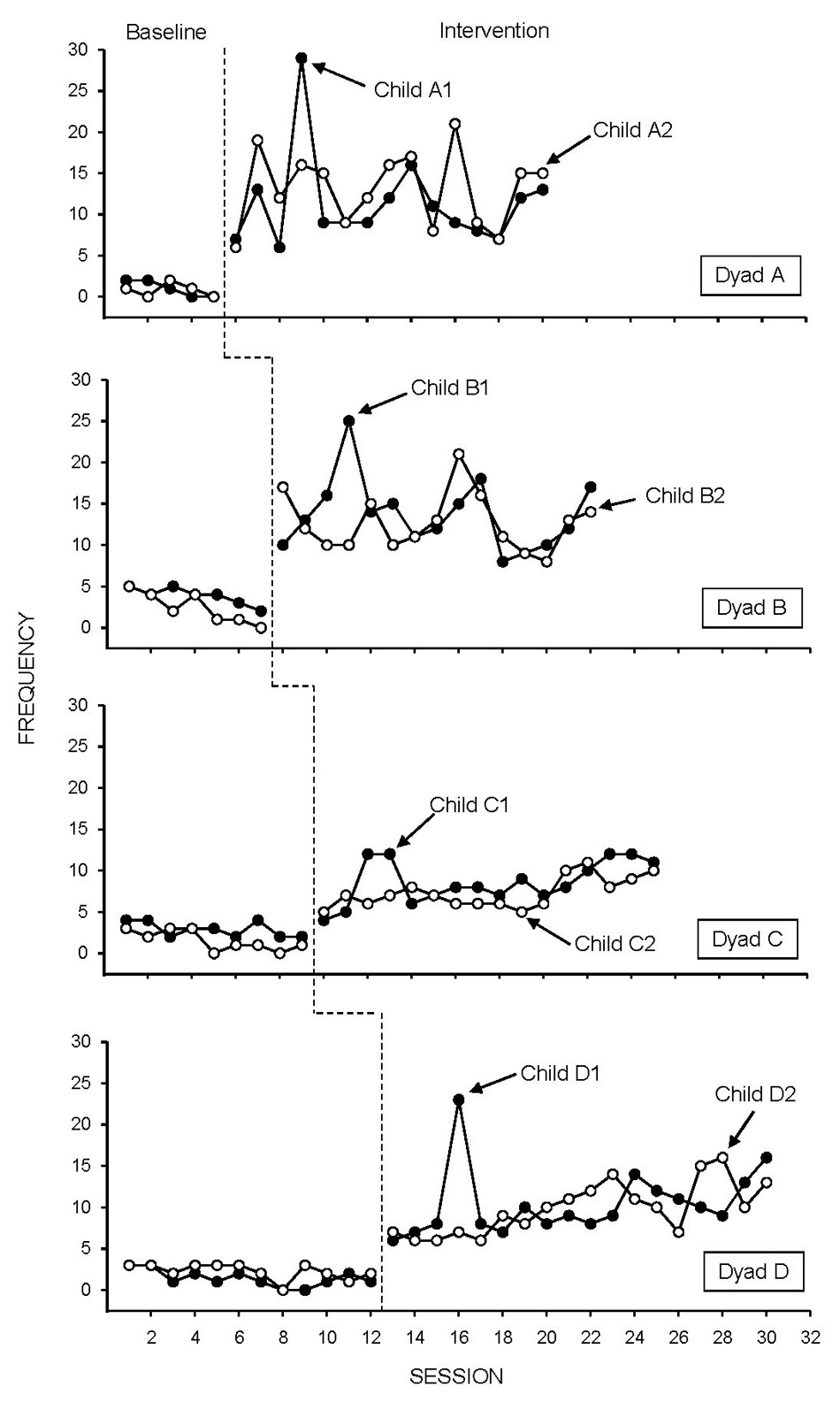
Children’s initiated verbal and nonverbal behavior to peers that resulted in a peer response.
Children’s Initiated Verbal Behavior and Nonverbal to Peers That Did Not Receive a Peer Response
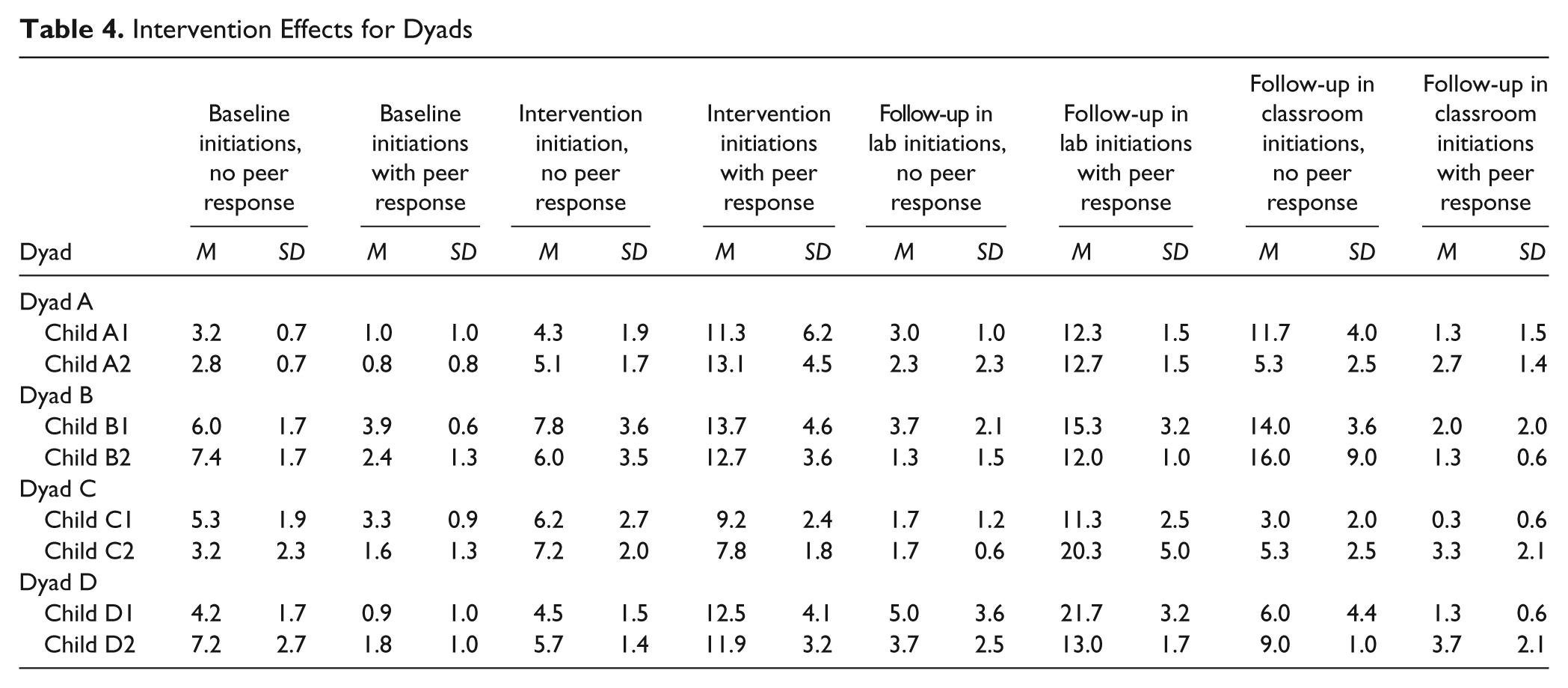
Initiations not receiving an immediate peer response are shown in Table 4. Data are presented as the mean number of initiated verbal and nonverbal behaviors produced during each condition that did or did not result in an immediate peer response (either verbal or nonverbal). Mean baseline initiation rates were similar to mean intervention initiation rates, indicating there was no change from baseline to intervention for initiations without an immediate peer response. Mean baseline rates of initiations without an immediate peer response were slightly higher than mean baseline rates of initiations with an immediate peer response for all dyads.
Intervention Effects for Dyads
Follow-Up Sessions
The second aim was to investigate whether intervention effects generalized to the classroom and to a condition similar to that of the baseline condition. We hypothesized that intervention participants would continue to have initiation and response rates that were similar to intervention rates. Follow-up data are shown in Table 4. The effects of the intervention appear to have generalized for the follow-up session that was similar to the baseline condition. Initiations receiving an immediate peer response remained near intervention levels for all children. The effects of the intervention do not appear to have generalized to the classroom setting. Initiations with an immediate peer response were variable and remained near baseline levels.
Social Validity
The third aim was to explore the social validity of intervention findings: (a) Did preschool teachers find the intervention procedures to socially acceptable? and (b) Did preschool teachers rate the behavior changes as socially important? In an assessment of social validity following completion of the study, three preschool teachers with master’s degrees in ECSE rated the acceptability of intervention procedures and socially important changes in behavior. Scores on the acceptability of intervention procedures could range from a minimum of 0 to a maximum of 40. Intervention procedure acceptability was rated a 38 by Teacher 1, a 36 by Teacher 2, and a 39 by Teacher 3. Scores on socially important changes in behavior could range from a minimum of 0 to a maximum score of 40. The mean ratings of baseline video clips were 13.7, 12.3, 21.0, and 18.0 for Dyad A, Dyad B, Dyad C, and Dyad D, respectively. Mean ratings of intervention clips were 37.3 (Dyad A), 39.3 (Dyad B), 32.3 (Dyad C), and 38.0 (Dyad D).
Discussion
This study extends the field’s understanding of social communication strategies teachers can use in several ways. First, little is known about the frequencies of initiations with an immediate peer response. Empirical research in this area has been directed largely toward tallying the number of peer-directed initiations and peer-directed responses separately (Beilinson & Olswang, 2003; Craig-Unkefer & Kaiser, 2002, 2003; Stanton-Chapman, Denning, et al., 2008; Stanton-Chapman et al., 2006; Thiemann & Goldstein, 2004; Timler at al., 2005), with limited exploration of the frequencies of these skills together. We found that the social communication intervention described in the current study increased the number of initiations with an immediate peer response from baseline through intervention. Indeed, all eight participants showed increases of initiations with an immediate peer response. This demonstrates a need to provide instruction of these skills concurrently rather than sequentially. These findings may also strengthen the call for directing more focused efforts toward promoting social communication skills by early childhood professionals because initiations and responses are skills needed for school success.
An interesting finding is that all eight participants demonstrated increases in initiations with an immediate peer response, including the children without IEPs. Two possible conclusions can be made from this finding. First, all participants scored below the mean on the PLS-4 (Zimmerman & Pond, 2002). This means that all eight children were technically delayed in their language development, even the children without an IEP. Children with delayed language may not have the essential language skills to make peer interactions more meaningful, may lose key opportunities to interact with peers, and cannot build on their language skills without peer interactions (Schneider & Goldstein, 2008). Therefore, it is critical that preschool teachers support the social communication skills of all children in their classrooms because more children without disabilities are demonstrating problems in social competence as they enter kindergarten (Webster-Stratton & Hammond, 1998). Second, the children selected thematic roles during the play session of the intervention, and their interactions were scaffolded by teachers. The work of Johnson and Johnson (1998) demonstrated that children who are placed in cooperative play groups with teacher support for social interactions learned more social skills and became more socially competent than children who did not receive teacher support. Clearly, role selection during play does not ensure successful peer interactions. Teachers who work with children with disabilities or who are at risk must provide support (e.g., suggestions for play, prompts to initiate or respond to a peer) for positive peer interactions to occur. In the current study, the interventionist provided support if it was needed, and the children improved their social communication skills. This suggests that teacher support and deliberate and routine teachable moments are critical for promoting social competence in the preschool classroom.
In the current study, the participants were placed in dyads. Two dyads were boy–boy, one dyad was girl–girl, and one dyad was girl–boy. Previous research has demonstrated that gender influences the nature and quality of peer interactions (Maccoby, 1988, 1990; Martin & Fabes, 2001). These studies have found that girls prefer dramatic play activities such as grocery shopping, housekeeping, and hair salon activities whereas boys prefer construction activities. Observations in preschool classrooms indicate that boys have an easier time than girls gaining entry into mixed-gender play groups (Corsaro, 1981) and boys use more physical aggression whereas girls use more relational aggression in their play (Ostrov & Keating, 2004). It does not appear that gender influenced the results obtained. All four groups had increases in initiations with an immediate peer response across all themes and activities from baseline to intervention. Such findings are not surprising, as all of the toy themes (e.g., grocery, doctor, construction, animal doctor, hair salon–barber) are classified as “social” and have previously been found to increase social interaction or higher levels of social play in typical preschoolers (Hughes & Carter, 2002). However, the paucity of information on developmental levels and functional description of social skills of participants in existing research complicates interpretation of previous findings on social toys with populations of children with disabilities.
Second, increases in initiations with an immediate peer response in the intervention and the return to baseline follow-up do not translate seamlessly within the classroom context. The children in Dyads A, B, and D did interact with their peers, but their interaction did not typically receive an immediate peer response. Children with disabilities tend to engage less in cooperative play with their typically developing peers in the classroom setting (Beckman, 1983; Hundert & Mahoney, 1993; Nabors, McGrady, Rosenzweig, & Srivorakiat, 2007; Van Hoorn, Nourot, Scales, & Alward, 2007). The role of teachers in the social interactions of children in integrated early childhood settings becomes increasingly important as researchers contemplate generalization strategies for this population of children. Negative correlations between the presence of teachers and the social interactions of preschoolers who were developing typically have been reported previously (e.g., Harper & McClusky, 2003; Kontos & Wilcox-Herzog, 1997). However, teacher-mediated intervention strategies may be needed in generalization conditions to continue to encourage interactions between preschoolers with disabilities and their typically developing peers. Strategies such as teacher arrangement of children with disabilities into groups that contain more socially skilled children (Guralnick & Groom, 1988; Odom & Strain, 1984), teacher prompting and praising (McConnell, Sisson, Cort, & Strain, 1991), and group contingencies on the social interactions of an inclusive group of children (Lefebvre & Strain, 1989) would be appropriate techniques provided that the teacher does not attempt to direct the children’s play, as this has been found to hamper peer-to-peer interaction with typically developing children (Carta, Sainato, & Greenwood, 1988). It may be unreasonable to assume that preschoolers with disabilities should be able to generalize newly learned skills to an untrained classroom context without teacher assistance.
Third, assessments of social validity by preschool teachers with master’s degrees in ECSE support the use of the social communication intervention described in the current study. Mean ratings on intervention video clips were higher than baseline video clips, demonstrating the observers’ view of peer dyadic interactions as more positive and reciprocal in the intervention. Furthermore, teachers feel the intervention approach is something they could implement easily in their classrooms. By bringing the intervention package into the classroom setting, children with disabilities would have consistent opportunities to receive social communication instruction across the school day because this population of children often requires frequent and sustained opportunities to acquire, refine, and maintain new skills.
Limitations
A major limitation of the current study is that the intervention services were provided as a “pull-out” service delivery model rather than a “pull-in” service delivery model. Pull-out service delivery models have previously been criticized in the literature for isolating the target children, for the target children having difficulty generalizing to natural settings, and for the lack of social communication interactions (Paul-Brown & Caperton, 2001). However, our conversations with lead teachers, assistant teachers, and center directors led to the selection of social pragmatic skills that were relevant to classroom needs.
The extent to which preschool teachers value and promote social interactions between peers in their classroom may have influenced social validity ratings. Teacher variables (e.g., teaching experience, special education background) and school variables (e.g., positive behavior support programs in the schools) may have contributed to positive ratings. For example, research indicates that teachers report varied degrees of exposure to preservice training and professional development opportunities in the area of social skills (Sugai, Horner, & Gresham, 2002) and that these experiences are likely to influence the value that educators place on social skills development. Future research should examine the role that prior teacher training plays in determining instructional priorities in this area as well as the extent to which programmatic efforts to promote social skills training are implemented in the schools.
Implications
Several implications for practice can be derived from the present study findings. Teaching children turn-taking strategies (e.g., initiations or responses) is likely to improve the quality of social interactions that children have with their peers. The methods used in this study to teach social communication skills would be classified as social learning intervention procedures (Elliott & Gresham, 1993) in that they included a combination of observational learning and reinforced learning. These approaches have high social congruence with methods teachers naturally use with preschoolers, perhaps differing mainly in their intensity and their systematic application. Thus, the modeling and prompting strategies used in this study could be applied by clinical practitioners and teachers to improve the sociodramatic play of the children in their classrooms. Sociodramatic play typically occurs on a daily basis in the preschool classroom and is actively encouraged by classroom teachers. The social communication intervention described in the current study offers a more systematic technique for teaching social communication and play skills than do the informal strategies commonly used by teachers, and this intervention appears to lead to improvements in initiating and responding between peers. Teacher prompting and reinforcement may be necessary to achieve desired effects though, especially at the onset of the intervention program. Improved outcomes would be reflected by children who could spontaneously combine their skills to initiate, respond, and maintain longer social interactions with their peers during center time, on the playground, during group time, and during mealtimes (Fujiki, Brinton, Isaacson, & Summers, 2001; Goldstein, Schneider, & Thiemann, 2007). This may lead to improved social status and peer acceptance.
More maintenance data are needed to determine whether participants can continue using the social communication skills without support from the interventionist. Future research might consider assessing maintenance at 1 month, 3 months, and 6 months. Follow-up assessments should also include observations of the children in various settings and during different times of the school day. If children are expected to use the learned strategies across time and in different settings, it would be important to determine whether or not they can use the strategies when presented with different stimuli.
Conclusion
The current study adds to the growing body of evidence that interventions incorporating several different domains (i.e., social, language, cognitive) are effective in promoting positive social outcomes and children’s later academic achievement (Caprara, Barbaranelli, Partorelli, Bandura, & Zimbardo, 2000; Guralnick, 1992). Following training, the majority of the children increased their initiations with an immediate peer responses. By engaging in socially identified situations via storybook reading and behavioral modeling, children begin to understand and participate in appropriate social communication behavior.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.