
Abstract
Students with visual impairment (VI) lack access to the same models and reinforcers as students with sight. Consequentially, behaviors that children with sight acquire through observation must be explicitly taught to children with VI. In addition, children with VI have difficulty maintaining such behaviors. Therefore, interventions that promote self-management of students’ own behavior are desirable. In this study, three adolescents used self-talk to increase chewing with a closed mouth during mealtimes. We used explicit instruction to teach students the target behavior and to use a small vibrating device as a reminder to self-talk during mealtimes. Prompts were faded as participants increased chewing with a closed mouth. Following mealtimes, performance feedback and reinforcement were provided. All students increased percentage of intervals chewing with a closed mouth immediately at the start of intervention and maintained this behavior for up to 1 month post-intervention. Implications for practice and directions for future research are discussed.
Social skills development is a critical factor affecting the success people with visual impairment (VI) experience in school and employment. Crudden (2012) found students with VI ability to positively present themselves to be associated with successful employment post-transition, and, although a causal relationship was not determined, other researchers found participation in extracurricular activities to be significantly related to better social skills in students with blindness (Zebehazy & Smith, 2011). However, students with VI may not be aware of subtle aspects of social interaction that facilitate or impede relationships, both personal and professional. In a survey administered to 68 teachers of high school students with VI, almost half of respondents believed students with VI “had a poor understanding of peer-related social skills” (Reed & Curtis, 2011, p. 555). For example, habits such as looking at the ground instead of toward a person speaking typically emerge because students with VI may not readily see the importance or reason for eye contact (Jindal-Snape, 2005a, 2005b). Similarly, the habit of chewing with a closed mouth may not be regarded as important to students with VI for the same reasons. Although, we are not aware of any studies linking these particular behaviors to quality of life or employment outcomes, these skills or lack thereof may contribute to negative perceptions some students with VI face from their peers (Reed & Curtis, 2012).
These discrepancies in social skills in students with VI are often attributed to a lack of access to visual models. That is, VI may negatively impact students’ ability to imitate the pro-social behaviors of others (Celeste, 2007; Gold, Shaw, & Wolffe, 2010). In addition, without sufficient vision to see the facial expressions of peers, like smiles or grimaces, students with VI may not understand how their peers react to inappropriate behavior (Caballo & Verdugo, 2007; Celeste, 2007). That is, students with VI lack access to the same reinforcers and consequences that impact the maintenance of some behaviors for students with sight. Because some social skills are not as easy for students with VI to acquire or maintain, it becomes essential for teachers to explicitly teach students with VI to perform these behaviors and the consequences of not performing these behaviors (Jindal-Snape, 2004, 2005a). However, it is not enough to teach students with VI the importance of and acquisition of pro-social behaviors. Instructional strategies are needed to teach students to self-monitor and maintain pro-social behaviors.
Self-management is an umbrella term for techniques used to shift behavioral control from teacher-led instruction to student-directed strategies (Briesch & Chafouleas, 2009; Fantuzzo, Rohrbeck, & Azar, 1987). For example, self-monitoring entails prompting students to self-reflect and assess their own behavior. Often in self-monitoring studies, students record whether they are on task several times during an activity and are reinforced for the level of accuracy in their self-evaluations (e.g., Blood, Johnson, Ridenour, Simmons, & Crouch, 2011). Self-management also includes such techniques as allowing students to self-select a target behavior to change, operationally define the behavior, select reinforcers, set performance goals, self-prompt, self-administer reinforcers, and chart their own performance over time (Briesch & Chafouleas, 2009).
Researchers using self-management procedures tend to target cooperative or on-task behaviors (Briesch & Chafouleas, 2009). Self-management interventions have been effectively used to increase and maintain new social behaviors as well, such as requesting teacher attention (Lo & Carthage, 2006), following instructions (Peterson, Young, Salzberg, West, & Hill, 2006), initiating and maintaining social interactions (Loftin, Odom, & Lantz, 2008), and maintaining eye contact (Gear, Bobzien, Judge, & Raver, 2011). The MotivAider®, a small vibrating timer, has been used to cue students to self-monitor time on task, talking out, tantrums, and non-compliance (Amato-Zech, Hoff, & Doepke, 2006; Legge, DeBar, & Alber-Morgan, 2010; Lo & Carthage, 2006). The MotivAider® can be used to decrease students’ reliance on teacher prompts, without the distraction inherent to auditory and visual cues. The tactile nature of this device makes it ideal for use with students with VI. However, to our knowledge, the utility of the device for learners with VI has not been empirically demonstrated.
Few studies have been published in which self-management strategies were taught to students with VI. Jindal-Snape (2004, 2005a, 2005b) and colleagues (Jindal-Snape, Kato, & Maekawa, 1998) conducted a series of studies using self-evaluation and feedback to teach students with VI to improve a variety of social skills. Adults intermittently prompted students to self-evaluate direction of eye gaze, participation in conversations, and on-task behavior. Subsequently, students were taught to recruit feedback from their sighted peers. Pro-social behavior increased with or without feedback but reached higher levels when feedback procedures were included. Teacher cues have also been used to prompt students to use self-talk to decrease body rocking (Estevis & Koenig, 1994) and improve study skills (Van Reusen & Head, 1994). Students were taught to first self-talk out loud. Over time, students transitioned to using internalized self-talk. Van Reusen and Head (1994) paired self-talk with teacher feedback and had students plot their accuracy. In both studies, students were successful at changing their behavior. This body of research suggests self-management may be a promising practice to teach social skills to students with VI; however, insufficient baseline data were collected or replications planned to draw strong conclusions from the data.
The purpose of this study was to test the effectiveness of a simple self-management procedure to increase and maintain pro-social behaviors of students with VI. Specifically, we are interested in the utility of the MotivAider® to prompt self-talk in students with VI to change their behavior. Therefore, the following research questions guided this study:
Method
A university institutional review board approved all procedures, and written consent was obtained from the participants and their guardians prior to the start of the study.
Three male residential students at a specialized residential school for students with VI participated in this study. To be included, dormitory staff identified students who lived on-campus during the school week and might benefit from instruction to increase appropriate chewing behavior. Subsequently, research personnel observed students to confirm that prospective participants chewed with an open mouth greater than 50% of the time during meals served at school. None of the participants had experience with self-monitoring, self-talk strategies, or the Motivaider® previous to participation in this study. Pseudonyms are used to respect confidentiality.
Participants
Bruce is an African American male who was 11 years 10 months old at the start of the study with VI due to optic nerve hypoplasia and nystagmus. Although Bruce is a braille reader, we found no specific acuity information in his records. He also had documented language impairments and a mild intellectual disability. Bruce passed a hearing screening and showed no evidence of hearing impairments.
Alfred is a Caucasian male who was 12 years 5 months old at the start of the study with VI due to optic nerve hypoplasia and nystagmus. His distance visual acuity with correction was approximately 20/320 in each eye. Alfred’s records indicated additional diagnoses of mild hydrocephalus and possible diabetes insipidus. Alfred was classified as a child with multiple disabilities, legal blindness, learning disability (unspecified), language impairment, and speech impairment. His teachers had no concerns regarding Alfred’s hearing abilities.
Karl is an African American male who was 14 years 4 months old at the start of the study. Karl qualified for services as a child with deafblindness. His visual diagnoses included optic atrophy and congenital myopia. He was a print reader who wore glasses. With correction, Karl’s distance acuity was 20/150 in the right eye and 20/200 in the left eye. Karl had a severe binaural sensorineural hearing loss. He used a total communication approach for expressive and receptive language that included speech, sign, and a Vantage Lite augmentative and alternative communication device. Additional diagnoses included hydrocephalus, which required shunting, and mild intellectual disability.
Setting
Observations were conducted in the school cafeteria during breakfast and dinner, seven to nine sessions per week, over the course of 9 weeks. The school cafeteria was arranged with both rectangular and circular tables seating three to eight students each. Participants sat at assigned seats with their dormitory roommates and staff. The participants in the study sat at three separate tables. Students usually served themselves family-style at their table. Approximately 70 to 80 students were present in the cafeteria. Instructional sessions were held individually for each participant in a vacant classroom with other key study personnel present. Feedback and reinforcement procedures were carried out in the participant’s dormitory or in the cafeteria.
Materials
MotivAider® (2000) devices, called “reminders” for this study, were used during intervention to promote self-reflection. Students received a device during mealtime to place in their pocket. The MotivAider® devices (2-3/8 × 2-1/2 × 3/4 inches) provided vibratory tactile input to students at preset intervals. Two independent observers used personal data assistant (PDA) devices with Multi-Option Observation System for Experimental Studies (MOOSES) software (Tapp, 2004) to collect data. The software was configured to provide an audio cue, a number corresponding to each participant, every 10 s to indicate when and for which participant observers should code behavior. The observers tapped the screen of the PDA with a stylus to code the behaviors. The MOOSES program automatically stopped the data collection session after 20 min.
We used a commercially available star-shaped hole punch to tally sessions during which the students showed improvement by punching holes in index cards labeled with their names. Each time a participant received five star-shaped punches, he earned a prize. Participants were allowed to choose from a selection of items including small toy cars, a piece of hard candy, rubber bouncy balls, various miniature sports balls, and snack-size packs of M&Ms. The prizes were chosen based on suggestions from participants during informal questioning before the study began. These reinforcers were not otherwise available to participants during the study. During instructional and booster sessions, participants were given access to small amounts of snack food to practice chewing with their mouths closed. Snacks included Goldfish cheese snack crackers, chocolate chip cookies, and bananas, and were based on preferences of participants.
Participants were provided the same meals as non-participating students, which were prepared by the school cafeteria. Naturally, food items varied by mealtime. Researchers did not attempt to control the variety, pace, or quantity of food intake in anyway throughout the course of the study. In this way, opportunities to chew or speak with an open or closed mouth were presumably as frequent in baseline as during intervention and maintenance.
Measurement System
Behaviors were recorded using a momentary time sampling procedure using 10-s intervals. Observers rotated their position in the cafeteria to record the behavior of a different participant at the end of each 10-s interval. The order of the participants was randomized and changed each session. Each session lasted 20 min. Sessions began when all students were seated and had been served food or when the first student to be served was approximately half finished with his meal, whichever came first. Each participant’s behavior was recorded 29 to 30 times each session.
Behaviors were coded as chewing with an open mouth (CO), chewing with a closed mouth (CC), talking with food in the mouth (T+), talking without food in the mouth (T−), not applicable (NA), unknown (U), or absent (A). CC was defined as chewing with lips together with no food or teeth visible to observers. CO was defined as chewing with food or teeth visible to observers. NA was used to indicate the participant had food in his mouth, but was engaged in some behavior other than chewing such as swallowing, licking fingers, or drinking. T+ and T− were defined as talking with or without food in the mouth. Observers coded U if a participant’s behavior was obstructed from view. If a participant was absent from the cafeteria during data collection, an A was coded for each interval the participant was absent. The percentage of time participants chewed with a closed mouth was calculated by dividing the number of intervals coded CC by the number of intervals coded CO plus T+ plus CC.
Study Design
A multiple baseline across participants design was used to detect threats of internal validity due to history and maturation by staggering the introduction of the intervention to participants over time. Instrumentation threats were also monitored through the use of daily graphing of data to ensure that interobserver agreement (IOA) was at acceptable levels across the course of the study (Gast & Ledford, 2010).
Baseline
During baseline, the participants were observed and their behaviors recorded without any exposure to the self-management procedure or the reminder. Prior to baseline, each student gave verbal assent to participate in the study. Assent procedures included reading a script, which explained the purpose of the study was to help students chew with a closed mouth, and students were told they would be watched during mealtimes to see whether they chewed with a closed mouth. Researchers did not prompt students in any manner upon entering the cafeteria during baseline.
Once baseline data were stable for the first participant, intervention began for that participant. The other participants continued in baseline. Once the first participant achieved mastery in the first intervention phase and the second participant’s baseline data were stable, the second participant began intervention. This same pattern was repeated for the third participant. Mastery was defined as chewing with a closed mouth at least 80% of intervals in a session, for three consecutive sessions.
Instructional session
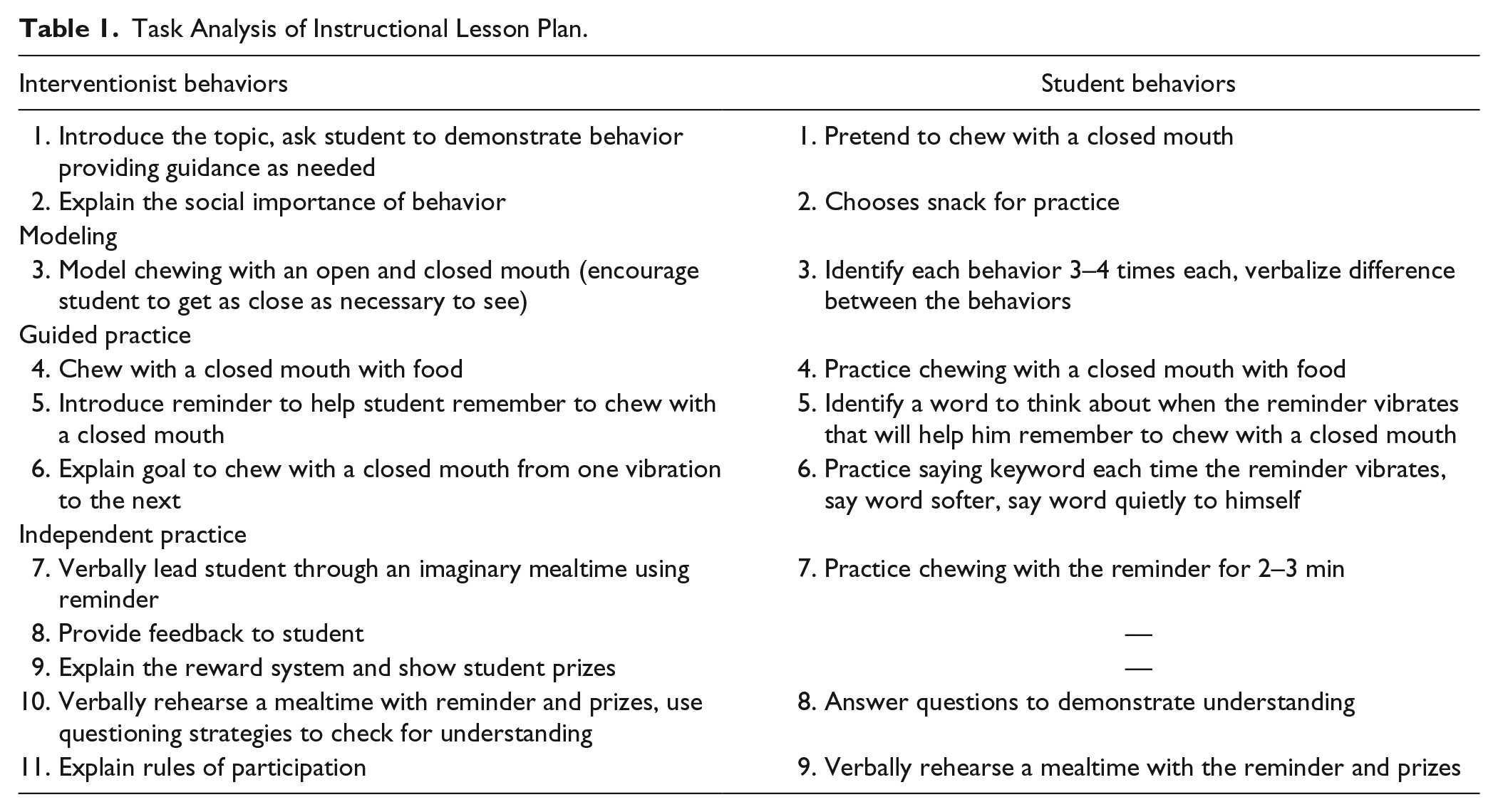
An instructional session to teach self-management of chewing behavior occurred at the start of the intervention phase for each participant immediately prior to dinner. The interventionist was a graduate student in the program for visual disabilities and the second author. She had not worked with these students prior to this study. An explicit instruction lesson plan was designed for this study (Archer & Hughes, 2010). See Table 1 for an outline of the instructional session. During this session, the interventionist explained four rules to students for participation in the project: (a) do not talk to his roommates about the project, (b) leave the reminder alone once in his pocket, (c) keep the prizes earned to himself, and (d) ignore any questions from peers about the reminder or the project. These rules were implemented to decrease the likelihood of treatment contamination from one student to the next, although student compliance was not monitored.
Task Analysis of Instructional Lesson Plan.
Intervention
Participants entered the cafeteria with peers from their dormitory and once seated were greeted by the interventionist. The reminder device was presented to the participants, and they were reminded to chew with their mouths closed, to talk only when they had an empty mouth, and to try to chew with their mouths closed for the whole meal. Each participant started out with the reminder set to vibrate every 30 s. The length of the interval was doubled once a student met mastery criterion; however, in situations where IOA was low, intervention in a given phase was continued to increase confidence that the true scores were consistently above 80%. Intervals were doubled up to 8 min and then participants were given the reminder turned to the off position.
After 20 min, the interventionist collected the reminder. Participants were given one of three types of feedback: (a) the amount of time chewing with a closed mouth increased, (b) the amount of time chewing with a closed mouth did not increase, or (c) the participant chewed with a closed mouth the entire mealtime. After breakfast sessions, the interventionist gave feedback to students in the cafeteria. After dinner sessions, feedback was given to students in their dormitory. The interventionist reinforced all students in their dormitory after dinner. Individually with each participant in his dormitory, the interventionist punched students’ index cards when appropriate and asked the participants to count the number of hole punches. If students had five punches, they could choose a prize. Finally, the interventionist told students how many more punches they needed to earn a prize.
Booster session
If a participant was struggling to chew with a closed mouth, a booster session of instruction was provided. Booster sessions took place in the same classroom used for the original instructional session. First, the interventionist reminded the student of the goal to chew with a closed mouth and asked the student to demonstrate the behavior. The intention of the booster session was to elicit the behavior causing a problem for the student, to point out to the student what was incorrect, help the student correct the behavior, and reinforce the correct behavior. Booster sessions lasted 10 to 15 min.
Maintenance
Maintenance data were collected for each participant on average every 15 sessions after completion of the intervention. Participants did not have access to the reminder device during this phase nor were they told when they were being observed. No feedback or reinforcement was provided during this phase of the study.
IOA
The first and second observers trained extensively before the beginning of the study using mock videos. In mock videos, graduate students played the role of participants exhibiting a variety of anticipated and observed mealtime behaviors including difficult-to-code behaviors. First, observers reviewed the measurement system and response definitions with an expert coder using examples from mock videos. These practice data were collected using paper and pencil. After familiarity with each code was achieved, observers practiced beginning sessions simultaneously using the electronic data collection devices, which were used during experimental sessions. Two observers independently coded multiple video segments of 20-min duration each using the electronic data collection devices. Discrepancy discussions were held after coding each video, mediated by an expert coder. Reliability was calculated between the two observers using the point-by-point method, and percentage agreement was calculated for each individual code. Training continued until 90% agreement was reached on all codes. During the study, when IOA dropped below 80%, measures were taken to discern the cause of the disagreement, address the problem for the following sessions, and increase the amount of IOA data collected. An expert coder was used on three different occasions to check the codes of both observers to ensure bias and drift were not occurring. Because all data were collected live during mealtimes, both observers reported their individual codes to the expert coder immediately after coding the participant’s behavior during the session. The expert coder looked for patterns in the disagreements between herself and the observers to improve IOA. There was a tendency for IOA to be lower when the behavior of the participants was more variable.
IOA data were collected for at least 40% (<65.2%) of sessions for each participant in each condition. The point-by-point method (Ayres & Gast, 2010) was used to calculate the percentage agreement between two independent observers. The number of agreements was divided by the number of agreements plus disagreements and multiplied by 100. For Bruce, Alfred, and Karl, respectively, point-by-point agreement was 93%, 85%, and 84.6% for baseline; 86.8%, 91.9%, 87.6% for intervention; and 86%, 89%, and 87.5% for maintenance. Within intervention phases for varying lengths of reminder intervals, point-by-point agreement was 83.8% (30 s), 86% (1 min), 84.5% (2 min), 97% (4 min), 93% (8 min), and 93.5% (no vibration [NV]) for Bruce; 89.6% (30 s), 94% (1 min), 92% (2 min), 93% (4 min), and 100% (NV) for Alfred; and 86% (30 s) and 95.3% (1 min) for Karl. The only phase of intervention in which IOA was not collected was 8-min intervals for Alfred. In addition, the second observer’s data were graphed to detect threats to validity from observer bias or drift (Artman, Wolery, & Yoder, 2010). No threats were identified.
Procedural Fidelity
Procedural fidelity data were collected during at least 40% (<50%) of observational sessions for each participant in each condition. The occurrence or nonoccurrence of the following behaviors was measured using a checklist: (a) preparation of materials prior to the start of the session, (b) participants greeted appropriately and given the reminder with appropriate instructions, (c) correct placement of the reminder device, (d) correct feedback provided after each mealtime, and (e) correct reinforcement provided in the evenings. Procedural fidelity data were also collected during the instructional session for each participant. Because there was only one instructional session per participant, fidelity of instruction was calculated as the percentage of steps completed by the interventionist from the task analysis of the lesson plan. Procedural fidelity was above 99% for each participant within each condition and was 100% for each instructional session.
Social Validity
Social validity data were collected through surveys given to the participants, dormitory staff, and parents. The surveys were structured to assess the appropriateness and acceptability of the study’s goals, effects, and procedures. Variations of the following statements–worded appropriately for students, teachers, and parents–were rated on a 4-point Likert-type scale (1 = strongly disagree, 4 = strongly agree): (a) “It is important to chew with a closed mouth”; (b) “I observed changes in the participant’s chewing behavior”; (c) “I am confident in the participant’s ability to self-monitor eating behaviors”; (d) “I would use self-monitoring procedures to change other social behaviors”; and (e) “self-monitoring was an appropriate tool to change the participant’s chewing behavior,” or for students only, “I would like to use self-monitoring in the future.” All of the parties participating in the survey found the goals, the effects, and the procedures of the study to be adequate and acceptable to change the behavior of the participants, indicated by a response of agree or strongly agree with each statement.
Results
All three participants increased the amount of time chewing with a closed mouth during mealtime. A functional relation was demonstrated by immediate changes in level from baseline to intervention at the time of introduction to the self-management procedure. In addition, two out of three participants reached mastery criterion in the last phase of intervention with the reminder in the off position. The third participant showed improved performance, but the study ended due to time constraints before the vibratory prompts could be faded. Participant data are presented in Figure 1, and summary data for within condition and between conditions analyses are presented in Tables 2 and 3, respectively. Relative level changes within conditions were determined by comparing the median data point in the first half of each condition or phase with the median data point in the second half of the same condition or phase. Relative level changes between conditions were determined by comparing the median data point of the last half of a condition or phase with the median data point of the first half of the subsequent condition or phase. Variability or stability was determined following the 80-25 rule, where data were considered stable if 80% of data points within a condition or phase fell within a stability envelope calculated as the baseline median value multiplied by .25, which was superimposed over the trend line (Gast & Spriggs, 2014).

Percentage of intervals students chewed with a closed mouth during breakfast and dinner sessions are shown in the order students were introduced to the independent variable, the onset of which was staggered over time.
Within Condition Visual Analysis.
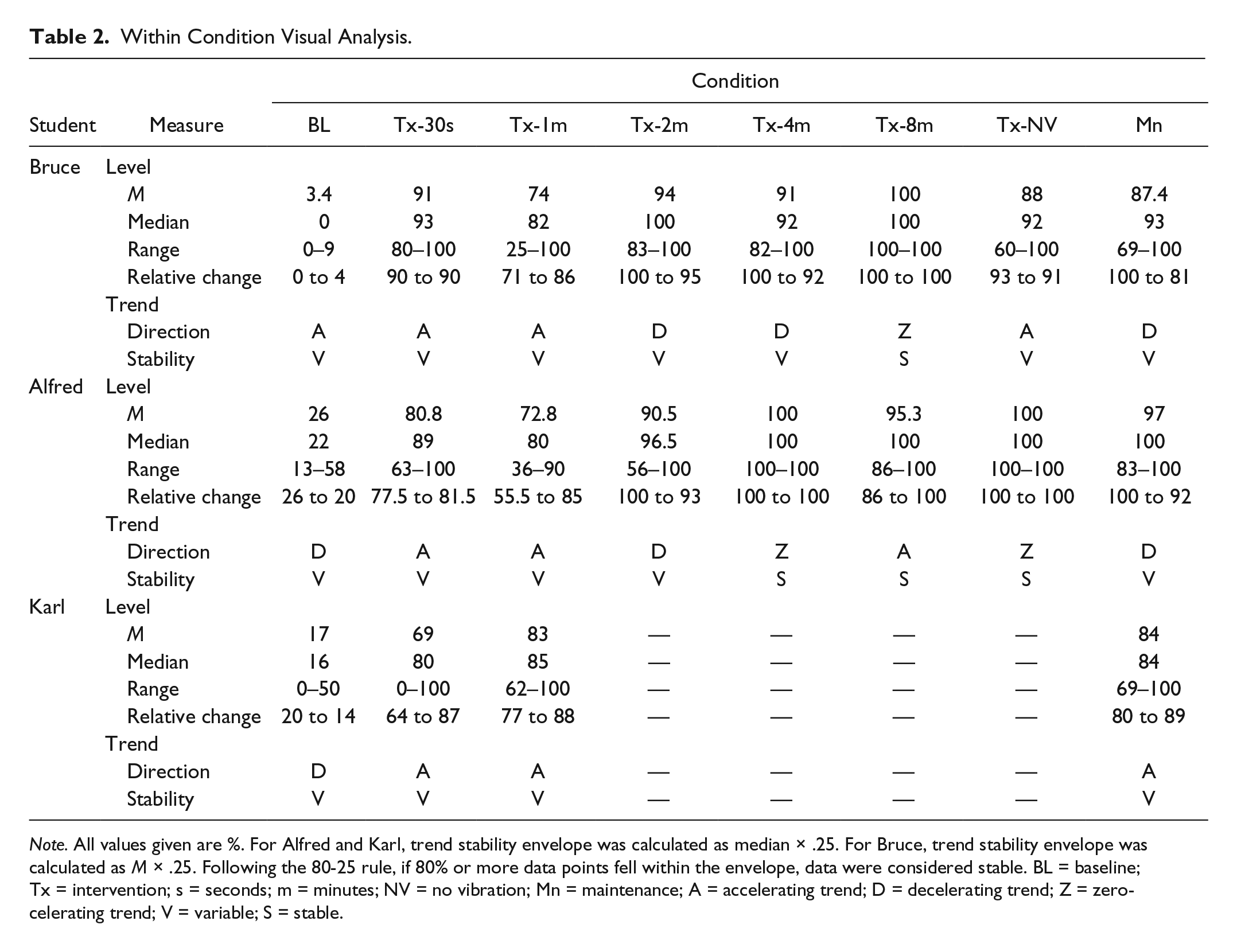
Note. All values given are %. For Alfred and Karl, trend stability envelope was calculated as median × .25. For Bruce, trend stability envelope was calculated as M × .25. Following the 80-25 rule, if 80% or more data points fell within the envelope, data were considered stable. BL = baseline; Tx = intervention; s = seconds; m = minutes; NV = no vibration; Mn = maintenance; A = accelerating trend; D = decelerating trend; Z = zero-celerating trend; V = variable; S = stable.
Between Conditions Visual Analysis Used to Determine a Functional Relation (BL to Tx-30s).
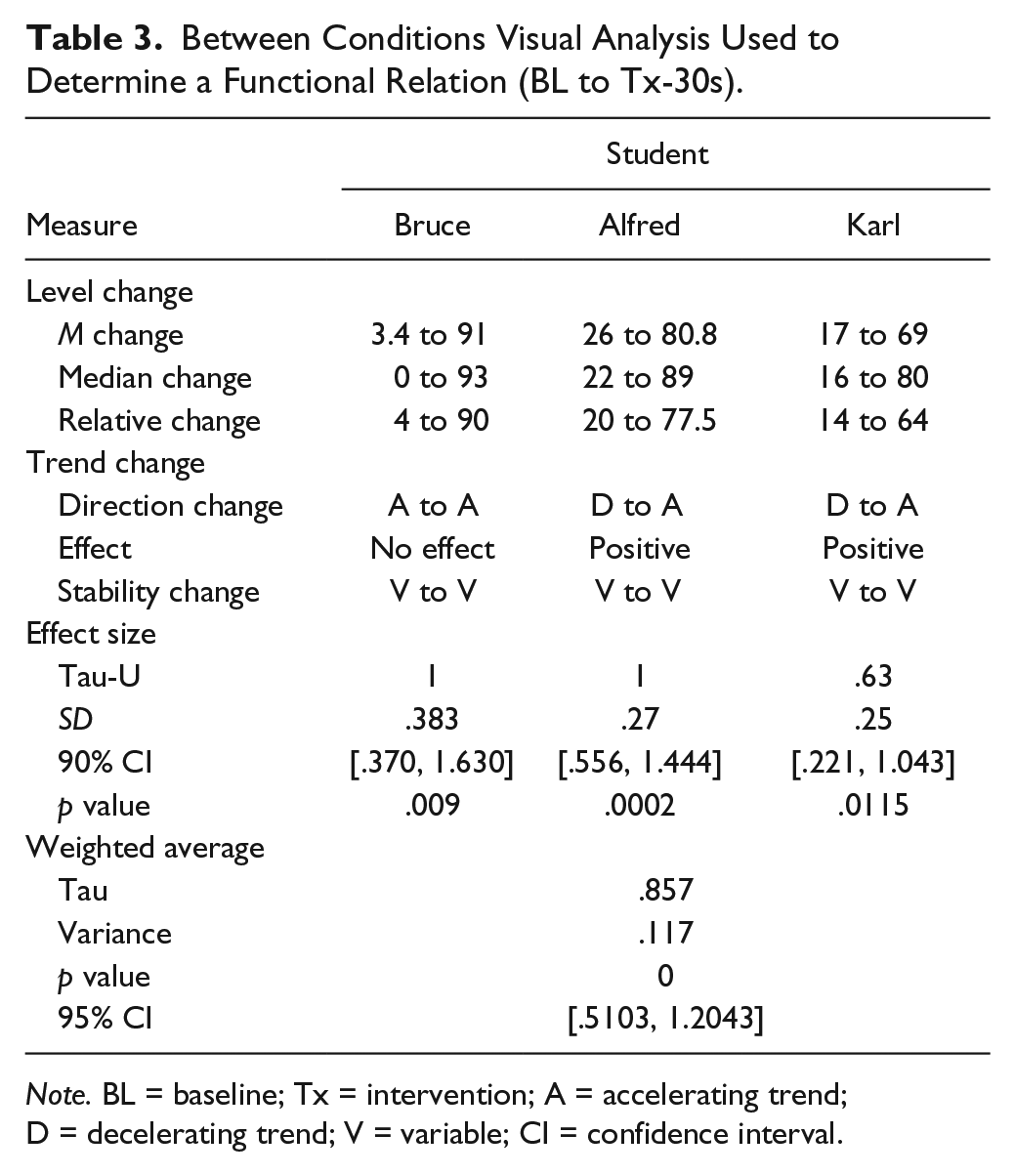
Note. BL = baseline; Tx = intervention; A = accelerating trend; D = decelerating trend; V = variable; CI = confidence interval.
Bruce
Baseline data for Bruce showed that he consistently chewed with a closed mouth during less than 10% of mealtime. Data in baseline showed variability and slight acceleration. Instruction was provided and the MotivAider® introduced between Sessions 5 and 6, and Bruce immediately increased the amount of time spent chewing with his mouth closed, with a relative level change from 4% to 90%. During the first two phases of intervention (i.e., 30 s and 1 min), data showed no effect from baseline in terms of variability and trend. Bruce spent the greatest amount of time in intervention at 1-min intervals (24 sessions). Across all phases of the intervention condition, Bruce chewed with his mouth closed on average 83% of the time (range: 25%–100%). Bruce continued to chew with a closed mouth above criterion level during the maintenance portion of the study. The last day of maintenance data collection for Bruce occurred exactly 1 month after his last day of intervention.
Alfred
Alfred’s behavior during baseline showed variability in the amount of time he chewed with a closed mouth, ranging from 13% to 58%. The intervention was introduced when Alfred’s performance showed a counter-therapeutic trend, as shown by relative changes in level from the first to the second half of baseline. The instructional session occurred between Sessions 8 and 9. Alfred immediately increased the percentage of time spent chewing with a closed mouth with a relative level change from 20% in baseline to 77.5% in intervention. In addition, data show a positive effect for trend. Data continued to show variability until the last three phases of intervention (i.e., 4 min, 8 min, and NV). On average, Alfred chewed with a closed mouth 87% of the time during intervention (range: 36%–100%). Alfred developed a serious illness during intervention, unrelated to the study, causing him to miss 2 weeks of school. Alfred maintained chewing with a closed mouth at high levels over this absence and after completion of the intervention. His longest phase of intervention was 14 days at 2-min intervals, during which time the student was also ill. The last day of maintenance data collection for Alfred occurred 1 month and 5 days after his last day of intervention.
Karl
Karl also showed variability in performance during baseline, ranging from 0% to 50%. From the first half to the second half of baseline, data also showed a counter-therapeutic trend. An instructional session was provided between Session 17 and 18. Immediately following instruction, Karl increased the amount of time chewing with a closed mouth to above 70%, with a relative level change between conditions from 14% to 64%. A positive effect for trend was also noted, although variability in the data remained. His level of performance subsequently dropped dramatically in the first phase of intervention (i.e., 30 s), and so a booster session was provided between Sessions 25 and 26. Following improvement, Karl’s shunt malfunctioned, requiring surgery. When Karl returned to school, we provided another booster session. From Session 49 until the end of the study, the percentage of intervals Karl chewed with a closed mouth did not fall below 60%. On average, he chewed with a closed mouth 74% of the time during intervention (range: 0%–100%). He spent the greatest amount of time in the first intervention phase (23 sessions). Due to time constraints, we were not able to gradually fade the vibratory prompts provided with the reminder device; however, Karl maintained high levels of chewing with a closed mouth 2½ weeks post-intervention without the reminder.
Discussion
The self-management procedures used in this study show promise as a tool to increase socially appropriate eating behaviors during mealtimes for students with VI. These include prompting self-talk and reflection, providing feedback on behavior change to students, and allowing students to self-select reinforcement delivered by the teacher. Findings from this study expand the literature on self-management in important ways. First, it is the first study that we are aware of to demonstrate a functional relation between a self-management intervention and behavior change for students with VI. The weighted average effect size across participants for this analysis was found to be large and significant (Tau = .857; p = 0) as described by Brossart, Vannest, Davis, and Patience (2014). Second, the findings suggest self-management interventions may promote maintenance of hard-to-maintain behaviors. Third, the data pattern replicated with all three participants suggests that although behavior change may occur quickly, frequent prompts, teacher feedback, and reinforcement may need to be ongoing for students to acquire lasting skills.
Three similarities in the data patterns for each participant warrant discussion about the effectiveness of the intervention. First, all three students’ behavior abruptly changed at the time of intervention, suggesting that the explicit instruction lesson plan was effective for teaching this new skill. Second, after this immediate behavior change, two of three students’ (Bruce and Karl) data patterns showed a deceleration in performance. Third, all three participants’ behavior throughout baseline and intervention was highly variable; however, visual analysis of the data showed a decrease in variability as performance improved. These last two observations suggest that students need time during which they receive frequent prompts (under the conditions of this study, at least 8 days or 16 sessions) to develop consistency with this new skill. Our results suggest that after this period of adjustment to new expectations, prompts can be faded relatively fast.
Unfortunately, time constraints only allowed data collection under maintenance conditions for approximately 1 month post-intervention. During this time, participants maintained behavior at levels similar to intervention. For two of three participants, we were able to fade prompts over time during intervention. Despite not fading prompts for Karl, he maintained high levels of behavior as well. This finding supports the idea that after students master the behavior with frequent prompts, prompts can be faded quickly. Procedures for fading teacher feedback and reinforcers over time were not included in this study, but future research should examine how maintenance is affected by these factors.
Limitation
Alfred and Karl had sufficient vision to see the observers collecting data. Although data collectors were as discreet as possible while observing, it is possible that their presence impacted these students’ behaviors. Unfortunately, there is no reliable way to determine whether the observers’ presence did in fact affect the behavior of the participants. Future researchers should strive to make data collection as inconspicuous and unobtrusive for participants as possible.
Implications for Practice
We have shown how self-management procedures, used often with students who are sighted, can be adapted for students with VI to change their own behavior. Moreover, the target behavior in this study was one that students with sight likely maintain by visual feedback, which is not available for many students with VI. Teachers of students with VI (TVIs) are responsible for providing access to the general education curriculum as well as teaching the Expanded Core Curriculum (ECC), which consists of nine skill domains for which students with VI need additional direct instruction. Two areas of the ECC are self-determination and social skills instruction (Hatlen, 1996). Chewing with a closed mouth is an important social skill that may impact acceptance by peers and future employability. In addition, students’ ability to self-manage their own behavior is an aspect of self-determination.
This study needs to be replicated, and more research is needed to define the parameters of an effective and efficient self-management intervention for students with VI. Given the lack of research to inform practice for teachers who work with students with VI, we suggest teachers draw ideas from these findings to use in their classrooms. Of note, the total instructional time to teach students the target behavior and how to use the reminder as a tool for self-reflection amounted to approximately half an hour. Data collection was time-consuming, but in practice it may not need to be collected on a daily basis. For example, students’ behavior could be monitored at a higher rate at the beginning of the intervention, and the teacher could gradually move to weekly or biweekly check-ins with the student. However, progress monitoring is necessary so that teachers can provide feedback and reinforcement to students. Finally, TVIs should consider use of the MotivAider® to provide prompts that are accessible to students who are blind and allow students to monitor their behavior independently and discreetly.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.