
Abstract
Developmental disability rates may vary by the season or month in which children are born. However, the seasonal mechanisms, such as climate, underlying these variations are unclear. Previous studies focused on high-latitude regions, leaving this climate hypothesis only partially tested. We analyzed rates of developmental disabilities in 3- to 5-year-old children from a tropical climate—South Florida—from 2004 to 2015 (N = 79,047) using a time-series analysis to identify peaks in diagnoses based on birth months. Children with speech impairments were more likely to be born in March, April, and September, a novel finding. Children with developmental delays were more likely to be born in September and October, consistent with studies in colder regions. In contrast to prior studies, there were no effects of birth month for language impairment or autism spectrum disorder. We highlight potential prenatal mechanisms that may contribute to the seasonal variations in some developmental disabilities.
Keywords
A variety of genetic and environmental factors can contribute to disabilities diagnosed in childhood (Esposito et al., 2018). Growing evidence suggests that disabilities may be associated with the month or season in which an individual is born (Gadow & DeVincent, 2012; Hebert et al., 2010; L. C. Lee et al., 2008). It has been theorized that infants born in the late winter or early spring may be at greater risk for some disabilities due, at least in part, to lower rates of prenatal vitamin D and sunlight exposure during gestation (Fernell et al., 2015). However, most of these studies were in cold climates with high seasonal variability in temperature and sunlight. Thus, it remains unknown whether these effects also occur in lower latitude climates with less seasonal variability.
Developmental Disabilities
Developmental disabilities—a group of conditions due to an impairment in physical, learning, language, or behavior areas (Centers for Disease Control [CDC], 2021a)—are typically identified and diagnosed during childhood (Butler et al., 2005). There are several disability eligibility categories legislated by the Individuals with Disabilities Education Act (IDEA; United States Department of Education, 2022), including speech and language impairments, specific learning disabilities, intellectual disabilities, autism spectrum disorders, and developmental delays. Although the general name for the grouping of disability categories varies based on specific institutions’ definitions (i.e., CDC: developmental disability; IDEA: disability eligibility categories; International Classification of Diseases, ICD-11: developmental disorder), for the sake of clarity, we hereafter refer to developmental disabilities when describing combined disability categories.
Developmental disabilities affect approximately 18% of children ages 3 to 17 years in the United States (Zablotsky et al., 2019) and can have negative life-long consequences. Children with developmental disabilities may experience language impairment (Clegg et al., 2005; Goldfeld et al., 2016), literacy difficulty (Nathan et al., 2004), lower academic achievement (Beal et al., 2010; Young et al., 2002), and social difficulties such as fewer social interactions with peers and greater difficulty maintaining friendships (Kasari et al., 2011). In adulthood, these developmental disruptions often lead to continued social difficulties with friendships and romantic relationships (Clegg et al., 2005; Magiati et al., 2014), poorer occupational outcomes, fewer job opportunities (Howlin & Magiati, 2017), and lower incomes (Murray, 2003). Moreover, these adults are at higher risk of developing mental health disorders (Howlin & Magiati, 2017). As such, understanding the mechanisms of seasonal birth effects are important to uncover possible factors contributing to the risk for developmental disabilities.
Developmental Disabilities in this Study
Although there are many developmental disabilities, we focused on the four most commonly diagnosed categories for children ages 3 to 5 years: (a) speech impairments, (b) language impairments, (c) autism spectrum disorder, and (d) developmental delay. Speech impairments are a communication disorder such as stuttering or impaired articulation (United States Department of Education, 2022). Speech impairments can cause children to have difficulties producing spoken language due to impairments in speech sounds, fluency, or voice that interfere with the child’s development (Gillon, 2005). In contrast, language impairments are voice impairments that adversely affects a child’s educational performance (United States Department of Education, 2022). Language impairments can cause difficulties in understanding and using language, along with impairments in written communication, due to difficulty in one or more of the basic learning processes involved in understanding and using language (Conti-Ramsden & Durkin, 2012).
Autism spectrum disorder is a developmental disability significantly affecting verbal and nonverbal communication and social interaction that adversely affects a child’s educational performance (United States Department of Education, 2022). It is a pervasive neurodevelopmental disorder commonly characterized by disruptions in social communication, difficulties with social interaction, and the presence of restricted and/or repetitive behaviors, interests, or activities (American Psychological Association, 2013).
Finally, developmental delay, a unique category of developmental disabilities, is a broad classification for children through 9 years of age who demonstrate significant delays in one or more of the following areas: physical development, cognitive development, communication, social or emotional development, or behavioral development (United States Department of Education, 2022). In Florida, children diagnosed with developmental delay often go on to be diagnosed with a specific learning or intellectual disability (Delgado, 2009).
Birth Month and Developmental Disabilities
The potential causes and underlying mechanisms of developmental disabilities are not well understood. Reports of birth month differences in rates of intellectual disabilities and learning difficulties may offer some clues about the mechanisms that underlie developmental disabilities (W. Liu et al., 2020; Mackay et al., 2016). Each seasonal peak in developmental disability rates is theorized to be associated with a different prenatal etiology, such as higher pesticide exposure in the summer, viral infections in fall, and seasonal affective disorder in the winter (L. C. Lee et al., 2008). Differences in climate are one of many potential explanations for inconsistent seasonality effects across locations. For example, studies of children in two countries with different climates but similar narrow ranges of temperature fluctuations—Central Italy and Scotland—both found higher rates of developmental disabilities, such as learning and intellectual disabilities, and developmental dyslexia, among children born between September and December (Donfrancesco et al., 2010; Mackay et al., 2016). However, studies of children in the United States—Arkansas and Georgia—with different climates and greater seasonal variability than Central Italy and Scotland reported higher rates of dyslexia and specific language disorders among children born between May and July (Livingston et al., 1993; Martin et al., 2004).
Month of birth also appears to play a role in the rates of autism spectrum disorder. Studies in colder climates—Sweden (Göteborg), Canada (Toronto, Ontario), Denmark (Aarhus and Copenhagen), and the Northeastern United States (Boston, Massachusetts)—all found March births to be associated with peak autism spectrum disorder diagnoses (Gillberg, 1990; Konstantareas et al., 1986; Mouridsen et al., 1994; Stevens et al., 2000). A study in Bristol, United Kingdom—a warmer and less variable climate—also identified the spring (i.e., births occurring between March and May) as the period associated with the peak rates of autism spectrum disorder (Hebert et al., 2010). Yet, even among studies within the same state—California—different patterns were observed: one study reported that infants born in November had higher prevalence of autism spectrum disorder (Zerbo et al., 2011), while the other reported that infants born in August had higher autism spectrum disorder diagnoses (Mazumdar et al., 2012). In addition, the Mazumdar et al. (2012) sample was primarily from Los Angeles, a warm climate, while the Zerbo et al. (2011) sample spanned the state of California, ranging from warm to cold climates; this divergence may partially explain these dissimilar findings in California. Meanwhile, L. C. Lee and colleagues (2008) reported not one, but three, seasonal periods associated with increased risk for autism spectrum disorder in the Mid-Atlantic region of the United States (Maryland): April, June, and October.
While there is inconsistency in these findings, several of the findings from the higher latitude regions (i.e., colder with more seasonal variability in temperature and sunlight) report that children born in or around March are more likely to be diagnosed with autism spectrum disorder than children born in other months (Gillberg, 1990; Hebert et al., 2010; Mouridsen et al., 1994; Stevens et al., 2000). Few studies exclusively examined seasonality effects in lower latitude regions (i.e., warmer with less seasonal variability in temperature and sunlight). Three seasonal studies were conducted in warm climates—two in Israel and one in Western Australia. One of the studies in Israel found that children born in both March and August had a higher likelihood of being diagnosed with infantile autism (Barak et al., 1995), while the other two studies in Israel and Western Australia found no seasonal effects (Kolevzon et al., 2006; B. K. Lee et al., 2019). Therefore, it remains unclear whether climate is indeed a driving factor, given the few studies in warm climates with low seasonal variability and the lack of studies in low latitude, tropical climates.
Although the previous studies reported some consistent seasonal birth patterns, the methodology and analyses varied greatly, including the sampling techniques, the categories of disability, and the statistical methods (see online Supplemental Table S1). With few exceptions (e.g., Mackay et al., 2016), most studies focused on a single developmental disability, making it difficult to compare across different types of disability within a given climate and region. Some types of developmental disabilities have been studied more than others in relation to birth month: 14 on autism spectrum disorder, but only four on language impairments, two on intellectual/learning disabilities, and none on speech impairment, despite the latter being one of the most common developmental disabilities (Prelock et al., 2008; Roulstone et al., 2009). Given that each developmental disability likely has unique mechanisms (Walkley et al., 2019), it is important to study each independently. Finally, most reports of birth month effects on developmental disabilities have been conducted in more moderate or colder regions (see Figure 1). While these studies are useful in supporting the proposed mechanism that variation in temperature and sunlight across seasons leads to these birth month effects, there are few studies of seasonal effects in development disability diagnosis in climates with little to no change in both temperature and sunlight exposure throughout the year, and no extant research in tropical climates.
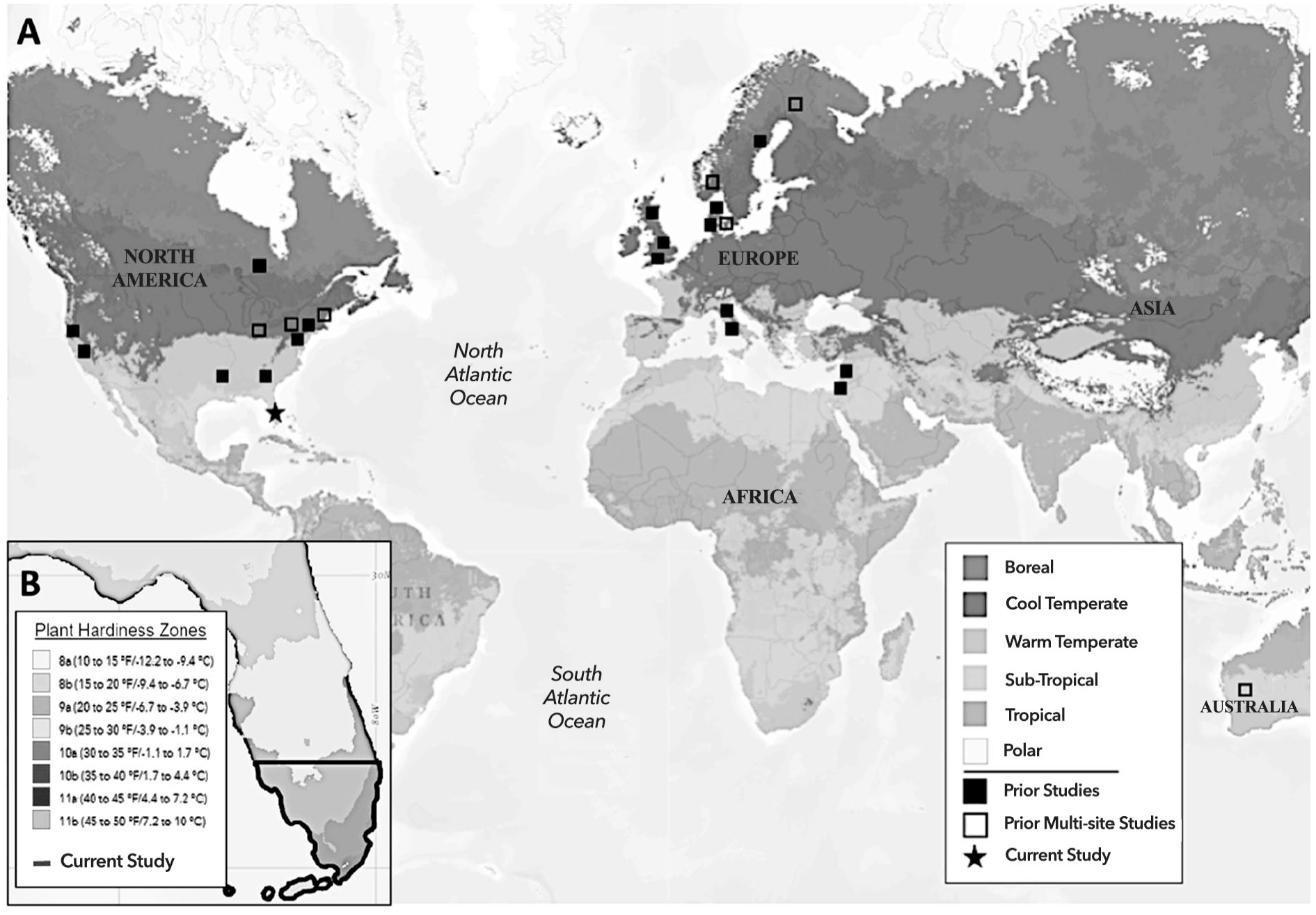
(A) Geographic Distribution of Birth Season Effect Studies by Temperature Domains, and (B) Plant Hardiness Zones of Florida and Current Study Region.
Current Study
This study examined whether the diagnosis rates of developmental disabilities—having one or more physical, mental, emotional, social, or learning exceptionality (Florida Department of Education, 2022)—in preschool age children (3–5 years old) varied across birth months in South Florida, a tropical climate. South Florida is a low latitude region (25.46°N) that has a narrow and warm average temperature range of 66 to 83°F (National Centers for Environmental Information (NCEI), National Oceanic and Atmospheric Association (NOAA), 2020] and an average of approximately 3,154 hours of sunlight per year (sunlight range of 12,823–26,184 KJ/m2; NLDAS, 2013), making it an ideal region to contrast with previous reports in colder regions with more variable seasons. We hypothesized that children’s birth month would be either unrelated to rates of diagnosis of developmental disabilities in preschool age children or would show different peak seasons than previously studied regions, due to South Florida having little seasonal variability and warmer temperatures. In other words, if climate is driving seasonal effects of developmental disabilities, we hypothesize that South Florida children will have fewer or different peak months of developmental disabilities rates than climates with greater seasonal variability.
Few studies have investigated seasonality in relation to a wide range of developmental disabilities across multiple cohorts, and most were restricted by small samples of diagnosed children. This study addressed these limitations with a secondary data set that spanned 11 years and included multiple developmental disabilities in a large, representative sample of 3- to 5-year-old children. With these data, we were able to separate birth month effects based on children’s disability category, controlling for fluctuations across years. We chose to examine 3- to 5-year-old children for several reasons: (a) it is the earliest age range of accurate disability diagnosis, (b) cognitive, social, and emotional abilities are rapidly developing, and (c) identifying deviations early in development may help inform interventions and support children at increased risk for a disability diagnosis.
Method
Participants
The University of Miami Institutional Review Board (IRB) determined that this study was not considered “research involving human subjects” as defined by DHHS and FDA regulations and was therefore exempt from IRB review. We obtained preschool developmental disability data for children born between 2004 and 2015 from the Florida Department of Education, Bureau of Exceptional Education and Student Services (BEESS), Children’s Registry and Information System (CHRIS) database. The CHRIS database contains referral, screening, evaluation, and eligibility information for preschool-age children throughout Florida. The original data set included deidentified records for all children in the CHRIS database born between 2004 and 2015 (N = 440,470). We narrowed these records to the southernmost 12 counties, N = 178,212, which had the warmest average low temperatures in Florida; NCEI, NOAA, 2020: Broward, Charlotte, Collier, Glades, Hendry, Lee, Martin, Miami-Dade, Monroe, Palm Beach, St. Lucie, and Sarasota. This approach of focusing only on Southern Florida enabled us to examine the regions with the least seasonal variability within the state.
We excluded records if there was no primary exceptionality diagnosis listed (n = 92,757) or if the child did not qualify for special education services. There were 79,047 usable records of children in South Florida who were diagnosed with a developmental disability between the ages of 3 and 5 years. We chose four developmental disability categories with the most children: speech impairment (n = 16,321), language impairment (n = 13,201), autism spectrum disorder (n = 8,291), and developmental delay (n = 40,301). All other diagnoses were omitted from the analysis due to limited sample size within diagnostic groups (see Table 1), ensuring that we had sufficient power for analyses. Diagnoses were determined based on the criteria specified in the Florida Statutes and State Board of Education Rules (Florida Department of Education, 2014).
Developmental Disability Categories and Sample Size.
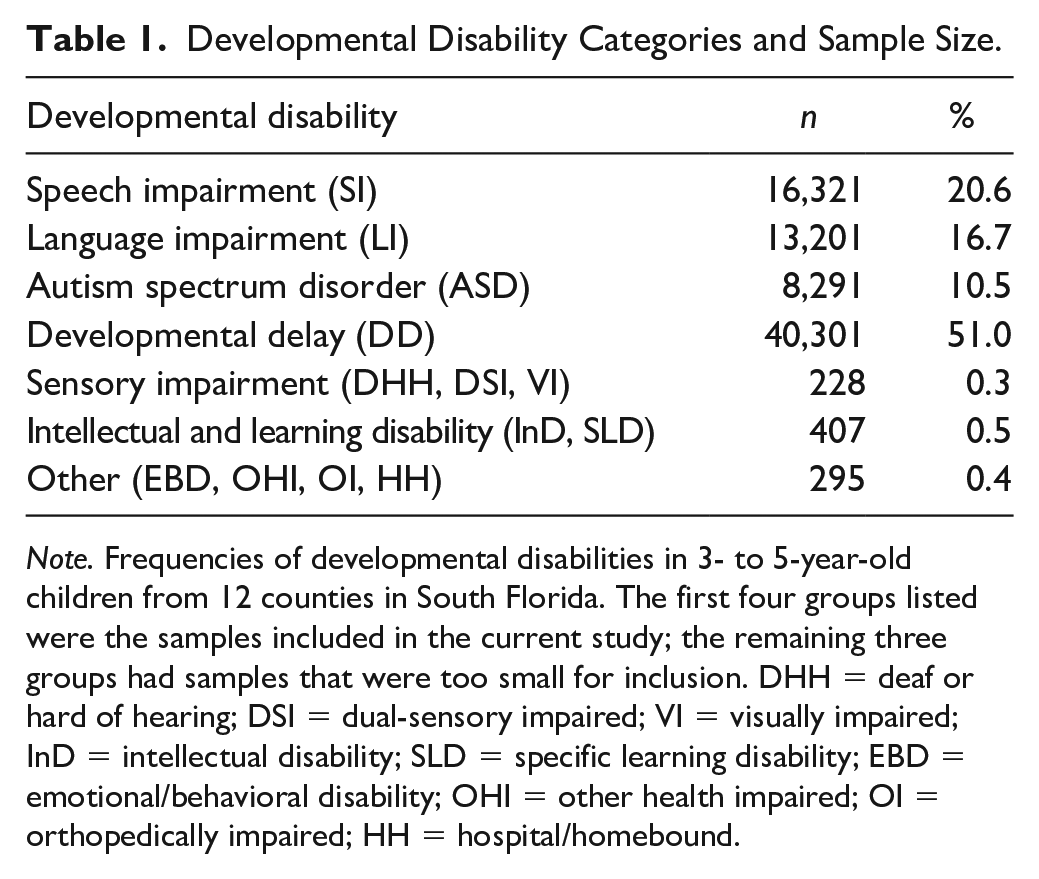
Note. Frequencies of developmental disabilities in 3- to 5-year-old children from 12 counties in South Florida. The first four groups listed were the samples included in the current study; the remaining three groups had samples that were too small for inclusion. DHH = deaf or hard of hearing; DSI = dual-sensory impaired; VI = visually impaired; InD = intellectual disability; SLD = specific learning disability; EBD = emotional/behavioral disability; OHI = other health impaired; OI = orthopedically impaired; HH = hospital/homebound.
Data Analyses
We conducted all analyses in R (version 4.0.5; R Core Team, 2021) and RStudio (version 1.4.1106; RStudio Team, 2021). We computed the proportion of developmental disabilities (number of diagnosed disabilities divided by the total number of births in that county each month from 2004 to 2015) in the four categories (i.e., speech impairment, language impairment, autism spectrum disorder, and developmental delay). Total birth data for the 12 Southern Florida counties (N = 1,098,365) were extracted from Florida Health Charts and Florida Public Health databases (Florida Department of Health, 2022). This approach enabled us to account for variations in baseline birth rates across seasons and years. We computed these proportions for each month from January 2004 to December 2015. Given that the computed proportions resulted in very small numbers, we scaled each category column by 100 (e.g., speech impairment proportion × 100) to make the data more interpretable, as a rate per every 10,000 people.
Next, we used time-series analyses to examine seasonality effects and trends within each of the four categories of developmental disabilities. We conducted four regressions on the time series data, one for each developmental disability, to determine whether certain birth months within each category of disability showed higher rates of diagnosis, accounting for changes in diagnoses across the years. We obtained these data from the Florida Department of Education, BEESS, Children’s Registry and Information System (CHRIS) database and have not been previously used to examine seasonality effects of developmental disabilities. CHRIS data can be requested for research purposes through the Florida Department of Education.
Results
We found that infants born in March, b = .17, p = .010, odds ratio [OR] = 1.19, 95% confidence interval [CI: .04, .30], April, b = .17, p = .010, OR = 1.18, 95% CI [.04, .30], and September, b = .14, p = .038, OR = 1.15, 95% CI [.01, .27], had higher rates of speech impairment diagnoses compared to other months throughout the year, while controlling for the statistically significant cubic trend in the data—an indication that diagnoses of speech impairment varied in frequency over the years. These results suggest that South Florida children born in the early to mid-spring and early fall might be at higher risk for speech impairments (see Figure 2). For language impairment and autism spectrum disorder, we found no effect of season (i.e., birth month). These findings indicate that, in South Florida, children were not at higher risk for language impairment or autism spectrum disorder based on their birth month. Finally, we found that infants born in September, b = .32, p = .005, OR = 1.38, 95% CI [.10, .54], and October, b = .24, p = .037, OR = 1.27, 95% CI [.01, .46], had higher rates of developmental delay diagnoses compared to other months, while controlling for the statistically significant cubic trend in the data—suggesting that diagnoses of developmental delay varied over time (see Figure 2). These results indicate that South Florida children born in the early fall may be more likely to be diagnosed with a developmental delay. For full results see Supplemental Table S2.
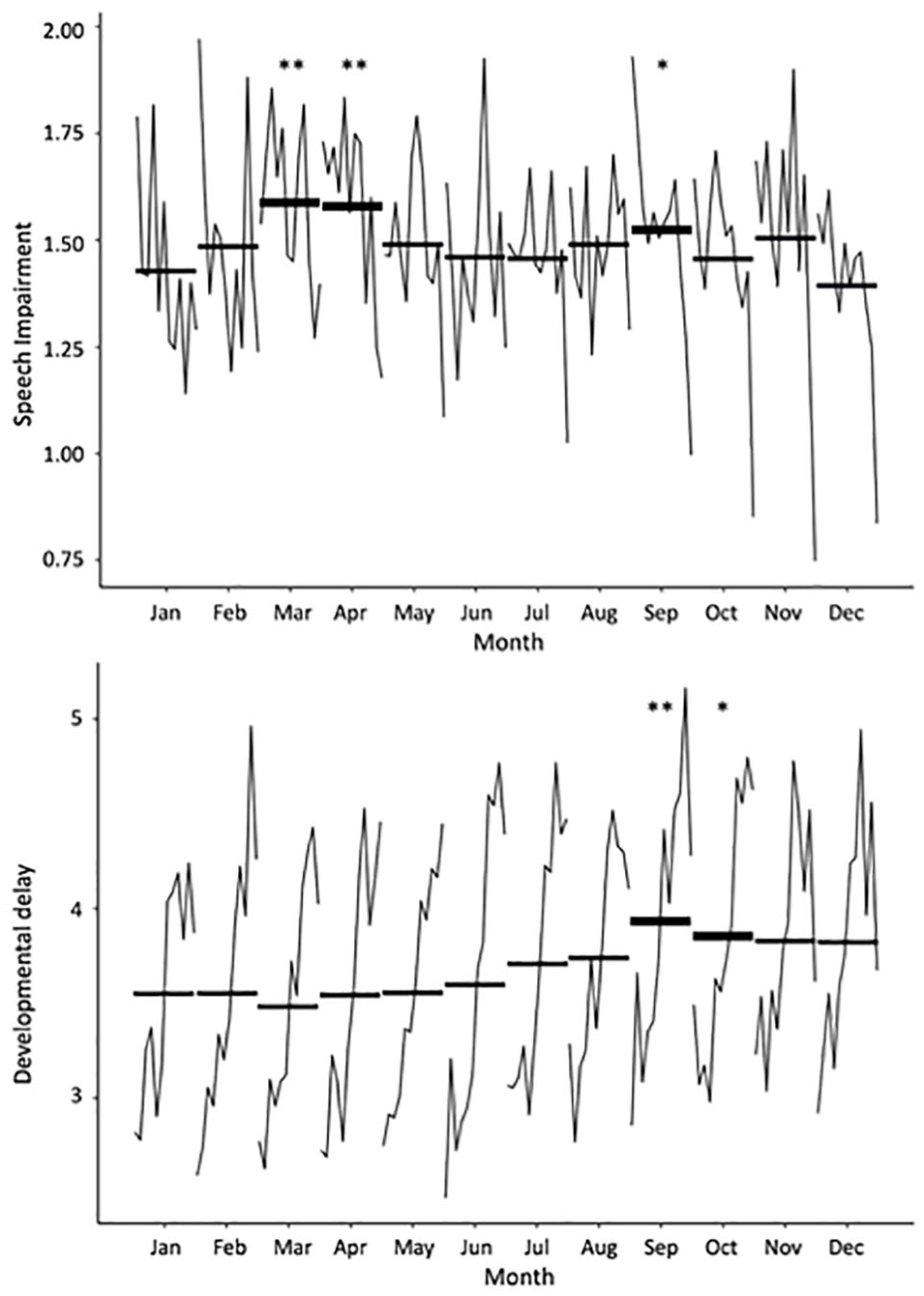
Seasonality Effect of Developmental Disabilities Out of the Total Number of Live Births From 2004 to 2015.
Discussion
In this study, we found that developmental disability diagnoses in 3- to 5-year-old children living in South Florida—a low latitude, tropical climate—may be associated with children’s month of birth. Furthermore, these associations differed from those reported in colder and more seasonally variable climates. We also found that the seasonal effects varied across different types of developmental disabilities within our South Florida sample.
Speech and Language Impairments
We found that speech impairment was diagnosed at higher rates among children born in March and April (early to mid-spring), as well as September (early fall) compared to the other months throughout the year. Yet, we found no seasonal variation in language impairment. To date, there are no published reports testing the effect of seasonality on speech impairment. One study in Surrey, England examined a variety of speech and language disorders together and reported an increase in diagnoses among children born in August (Robinson, 1991). However, the study’s limited sample size (n = 133), lack of a population control group, and combination of speech and language disorders make it difficult to determine the associations of these disabilities with children’s birth month. Two previous studies examined specific language disorders in middle childhood (Ghezzo et al., 2012; Martin et al., 2004). Researchers report higher rates of language disorders among children born in October to December in Central and Northern Italy, and in May to July in Georgia, United States. However, the study in Georgia examined data on school-age children—mainly children in fourth through ninth grade, about 9 to 14 years old—in special education, leading the researchers to theorize that maturation, or being younger than other children in the grade, may have contributed to the association of the high rate of summer births and language impairment diagnosis. In contrast, the study in Italy examined children and adolescents from 3 to 20 years, with most children below the age of 9 (n = 299; 83.5%). Furthermore, children under 5 years of age (n = 44) born between October and December, compared to older children, had the highest likelihood of having a language disorder. The study in Georgia also had a sample more than seven times the sample of the study in Italy (n = 2,768 and n = 358, respectively).
Together, these results suggest that the age of diagnosis (i.e., prior 9 years of age) may influence the prevalence of a language impairment diagnosis and, along with sample size concerns, the findings call into question climate-based interpretations of prior observed seasonality patterns. In sum, considering the scarcity of previous literature examining birth month and rates of speech and language impairments, and variable findings and limited sample sizes in the existing literature, the birth month mechanisms are ambiguous. Nonetheless, our findings for speech impairment are novel and suggest that speech and language impairment are markedly different in their patterns of seasonality in South Florida.
Developmental Delay
For developmental delay—a “catch all” category of early developmental disabilities, often later re-diagnosed at school age as an intellectual disability or specific learning disability (Delgado, 2009)—we found that rates were higher among children born in September and October (early fall), consistent with previous reports. Children in Scotland diagnosed with intellectual disabilities and learning difficulties were more likely to be born in the fall or early winter between October and December (Mackay et al., 2016), and children in Central Italy diagnosed with developmental dyslexia were more likely to be born in the fall, between September and November (Donfrancesco et al., 2010). The consistency of these findings with previous reports across other countries and climates suggests that a seasonal mechanism other than climate may be driving these developmental delay birth month effects.
Maternal infection may be one possible prenatal mechanism impacting the seasonal trend in developmental delays. Common illnesses like the human influenza virus tend to follow a similar seasonal pattern—with peaks in December through March—across different climates throughout North America and Europe (Centers for Disease Control and Prevention, 2021b; World Health Organization, 2021). Indeed, animal models indicate that maternal viral infections and immune activation negatively impact offspring development (Fatemi et al., 2002; Shi et al., 2003). Research in human studies suggests that maternal fever during pregnancy (Zerbo et al., 2013) and elevated maternal cytokines—signs of an inflammatory immune response—are associated with developmental delays (Goines et al., 2011). During pregnancy, there is an increased risk for viral infections and such infections tend to result in more severe reactions, especially during the first trimester (H. Liu et al., 2020). In this study, children with a developmental delay diagnosis were estimated to be in their early gestation during the fall and winter months, when viral infections were most prevalent (Centers for Disease Control and Prevention, 2021b). Therefore, it is possible that maternal infections during pregnancy play some role in children’s developmental delays.
Autism Spectrum Disorder
We detected no evidence of birth month variation in autism spectrum disorder within our sample of South Florida children, diverging from prior reports. Several previous studies examined seasonality effects for autism spectrum disorder, and while there is some variability in the findings (Bolton et al., 1992; Kolevzon et al., 2006; Landau et al., 1999), most large-scale studies generally reported that children born in March (early spring) were at higher risk for an autism spectrum disorder diagnosis (Gillberg, 1990; Mouridsen et al., 1994; Stevens et al., 2000). These studies were mainly conducted in regions that had colder winters with markedly less sunlight and more temperature fluctuations—Sweden, Denmark, and the Northeastern United States—than South Florida. Our conflicting findings in a lower latitude region suggests a possible prenatal mechanism linked to climate, particularly for those children gestating during the winter months in these northern latitude regions. In fact, there is more seasonal variability in vitamin D levels at northern latitudes compared to South Florida (Levis et al., 2005). The lack of birth month peaks in autism spectrum disorder and language impairment found in this study may be due to lower seasonal variability in sunlight exposure across the entire year for pregnant individuals in the South Florida area. That is, the mechanisms underlying the seasonal birth peak in developmental diagnosis might be more pronounced in higher latitude regions where pregnant people have limited sunlight exposure in the winter months due to climate conditions.
The lower latitude and tropical climate of South Florida is associated with high levels of sunlight and lower seasonal variation in sunlight exposure (Levis et al., 2005; NLDAS, 2013). As the majority of vitamin D is obtained via sunlight exposure (Levis et al., 2005), pregnant people living in South Florida may be less likely to have deficiencies in vitamin D during the winter months compared to pregnant people living in colder places. Vitamin D plays a critical role in fetal brain development (Eyles et al., 2011) and has been suggested as a mechanism underlying autism spectrum disorder’s etiology (Cannell, 2008). The negative effects of prenatal vitamin D deficiency have also been experimentally examined using rodent models. One study examining the impacts of gestational vitamin D deficiency on brain structures and learning ability found that vitamin D deficient mice offspring, compared with control mice, had decreased brain volume in some regions and poorer memory (de Abreu et al., 2010). These findings support the assertion that low vitamin D levels during gestation have detrimental effects on offspring development and cognitive functioning.
Consistent with animal models, vitamin D deficiency during human gestation is associated with impaired neurodevelopment (Grant & Soles, 2009). For example, in two cohorts of sibling pairs born in Sweden, children with autism spectrum disorder had lower vitamin D levels at birth than nonautism spectrum disorder siblings. Furthermore, among these children, those with autism spectrum disorder were more likely to be born in the spring (i.e., to have gestational periods during the winter months) than their nonautism spectrum disorder siblings (Fernell et al., 2015). As Sweden experiences large fluctuations in hours of sunlight and vitamin D acquisition by season (Klingberg et al., 2015), these findings align with the theory that limited winter sunlight exposure is related to lower levels of vitamin D and impaired neurodevelopment. Therefore, vitamin D deficiency could be a potential mechanism underlying birth month fluctuations in the rates of some developmental disabilities like autism spectrum disorder.
Limitations
There are several limitations in this study. Demographic information (i.e., race, ethnicity, and sex) has been linked to differences in vitamin D levels (Fernell et al., 2015; Schmidt et al., 2019) and differences in rates of developmental disabilities (e.g., higher rates of autism spectrum disorder in males and lower rates of developmental disabilities in Hispanic/Latino children; Garcia et al., 2019); however, in this study, demographic information was unavailable. Moreover, while we had diagnostic data and birthdates for the children in our sample, we cannot confirm that the pregnancies occurred in South Florida, nor do we know about prenatal factors (e.g., maternal infections and vitamin D levels) that could also affect developmental disabilities. Furthermore, we did not have the gestational age of the children, so we were unable to account for preterm births, which could confound our inferences about the timing of exposures during pregnancy. We were also unable to account for any other contextual variables that may have contributed to delays in development, including genetic risk factors and environmental factors like birthing complications, health issues, and other traumas. Our retrospective study only covered a small region of the United States; however, this was the first study examining birth month and developmental disabilities in a tropical climate. Nevertheless, prospective studies are needed spanning wider regions to better determine the effects of birth month on developmental disability diagnoses.
Conclusions
We detected variability in developmental disability rates by children’s birth month in low-latitude, tropical, South Florida. Rates of speech impairment and developmental delay differed by birth month, while language impairment and autism spectrum disorder did not. These distinct patterns of seasonality for speech impairment compared to the lack of seasonality effects for language impairment further emphasize the need for future studies to differentiate between these two distinct disorders. Our findings suggest that developmental disabilities may have diverse underlying prenatal mechanisms, such as viral infections or climate factors (e.g., warm temperature and sunlight exposure), which may influence the prevalence of a developmental disability diagnosis. Additional studies with detailed prenatal medical information are needed to retrospectively examine potential mechanisms influencing developmental disability diagnoses, such as maternal infections and vitamin D deficiency.
Supplemental Material
sj-docx-1-sed-10.1177_00224669221148726 – Supplemental material for Rates of Developmental Disabilities Vary Across Birth Months in a Tropical Climate
Supplemental material, sj-docx-1-sed-10.1177_00224669221148726 for Rates of Developmental Disabilities Vary Across Birth Months in a Tropical Climate by Sarah E. Maylott, Regina M. Fasano, Jacquelyn M. Moffitt, Cody L. Boland, Evan T. Burdette, Erica R. Nahin, Elizabeth A. Simpson and Christine Delgado in The Journal of Special Education
Footnotes
Author Contributions
C.D. conceived the study idea. J.M.M., E.R.N., R.M.F., C.L.B., and E.T.B. reviewed the literature and created Table 1. All authors wrote the introduction section. J.M.M., E.R.N., R.M.F., C.L.B., E.T.B., S.E.M., C.D., and E.A.S. planned and wrote the methods. ![]() was created by C.L.B. C.D., S.E.M., and E.A.S. requested and obtained the FDOE and CDC data sets. S.E.M. cleaned, analyzed, graphed, and interpreted the data. S.E.M. wrote the results and discussion and finalized the manuscript. All authors edited and approved the final manuscript.
was created by C.L.B. C.D., S.E.M., and E.A.S. requested and obtained the FDOE and CDC data sets. S.E.M. cleaned, analyzed, graphed, and interpreted the data. S.E.M. wrote the results and discussion and finalized the manuscript. All authors edited and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.