
Abstract
Rats are a commonly used animal model for the study of the pathogenesis and novel treatments of glaucoma, which is induced experimentally using invasive, painful procedures. Peribulbar anaesthesia (PBA) is frequently used in people and domestic animals prior to ophthalmic surgeries to provide excellent perioperative analgesia. Our goal was to develop a PBA technique adapted to rat anatomy, improving the welfare of animals used as a model for glaucoma. Eighteen rat cadavers (n = 36 eyes) were used to establish the optimal needle insertion location. Five injection techniques using 0.1 mL/100 g lidocaine 2% and a contrast agent (1:1 volume ratio) were compared via computed tomography (CT). CT images were scored for injectate distribution at four locations: extraconal, intraconal, around the optic nerve and at the orbital fissure (scale 0–8, where 0 = none and 8 = excellent). Median scores using the dorso-medial-75° (5; range 2–6) and medial-canthus (4.5; range 2–8) injection techniques were not different from the dorso-medial-45° (4; range 3–6) technique and were higher (better distribution) compared with mid-ventral (3; range 2–5) and ventro-lateral (2; range 1–3) techniques. The two superior techniques were used in two experimental rats (n = 4 eyes) to determine the volume of bupivacaine 0.5% necessary to affect corneal touch threshold (CTT) and periocular skin sensitivity (PSS). A volume of 0.05 mL/100 g decreased CTT and PSS for several hours, while a larger volume produced excessively long effects. Dorso-medial-75° or medial-canthus PBA using 0.05 mL/100 g bupivacaine are likely to provide ocular and periocular analgesia in rats, with minor transient adverse effects.
Introduction
Glaucoma is a leading cause of blindness in humans. 1 The leading risk factor for glaucoma is elevated intraocular pressure (IOP), which results in retinal degeneration and optic nerve atrophy. 2 Rats are a commonly used animal model for the study of the pathogenesis of IOP elevation and glaucomatous damage and to assess the efficacy of new treatments.3 –5 A PubMed search (last accessed 25 September 2022) for ‘rat, glaucoma’ resulted in 1698 articles, with numerous animals used in each study. IOP elevation is induced by a variety of invasive procedures, including optic nerve crushing or ligation, laser photocoagulation, anterior chamber cannulation or injection, and episcleral vein occlusion. 3 These procedures produce moderate to severe pain due to rich innervation of the globe and orbit, 6 and the resulting ocular pain can compromise the animals’ well-being. 7 However, the most common analgesic treatment for these painful procedures in rats is general anaesthesia during the surgical procedure, 8 which is sometimes supplemented by postoperative systemic non-steroidal anti-inflammatory drugs (NSAIDs) 4 or, less commonly, systemic opioids. 9 Therefore, there is a critical and unmet need to improve pain management in this commonly used animal model.
Regional anaesthetic techniques, such as peribulbar anaesthesia (PBA), are frequently used in people10,11 and companion animals 12 prior to ophthalmic surgeries for pain alleviation. PBA is performed by injecting a local anaesthetic outside the extraocular muscle cone. The injectate spreads throughout the orbit, including the intraconal space and eyelids, and produces excellent analgesia of the globe and periocular tissues.11 –14
Recently, enucleation was reported as a salvage procedure (i.e. instead of euthanasia) in rodents with medically unresponsive corneal disease. Although both opioids and NSAIDs were used for systemic analgesia during and following enucleation, the authors reported that rats suffered pain postoperatively and suggested that regional anaesthesia techniques should be used prior to enucleation in rodents. 7 However, despite this need, to the authors’ knowledge no such technique has ever been described in rodents. The objectives of this preliminary study were to develop a PBA technique adapted to rat anatomy and to assess the volume required to decrease ocular and periocular sensitivity as indicators of analgesia in rats. Our hypotheses were that PBA will result in good periocular distribution in cadavers and that it will decrease corneal and periocular sensitivity in rats tested in an experimental setting as reported in other species.13,14
Methods
Animals
The study was approved by the Institutional Animal Care and Use Committee (MD-15714-3) of the Hebrew University of Jerusalem (HUJI). HUJI is a full-accredited institution by the Association for Assessment and Accreditation of Laboratory Animal Care (AAALAC). All animals in the study were housed in a specific pathogen free (SPF) facility.
To reduce animal numbers in experimentation, all rat cadavers used in this experiment were euthanised for reasons unrelated to the present study. Rats were not subjected to any procedure and were euthanised via CO2.15,16
To explore the effects of PBA in live rats, two Sprague Dawley male rats (n = 4 eyes) were used (Envigo, Jerusalem, Israel). Animals had ad libitum access to food (TEKLAD 2918SC) and water (acidified with HCl to pH 3.0 ± 0.5) and were housed together in environmental conditions of 22 ± 2°C and a 12-hour/12-hour light/dark cycle according to the Guide for the Care and Use of Laboratory Animals (National Research Council 2011). Animals were given three days to acclimatise to the environment and then one week of habituation to handling and procedures, including light restraint using positive reinforcement with chocolate hazelnut paste.
Part 1: Developing PBA injection technique in rat cadavers
Eighteen rat cadavers (n = 36 eyes) were used to establish the optimal injection technique. The cadavers were positioned in sternal recumbency on a platform that was 5 cm high. A peribulbar injection of lidocaine 2% (Lidocaine, B. Braun 2%; B. Braun, Melsungen, Germany) and a contrast agent, iohexol (Omnipaque 300; GE Healthcare, Dublin, Ireland) at a volume ratio of 1:1 was performed. All injections were performed by a board-certified veterinary anaesthesiologist (Y.S.-B.) experienced with these techniques in other species13,14,17,18 using a 13-mm, 27-gauge needle (Shanghai KDL Co. Ltd, Shanghai, China).
Five peribulbar injection techniques were developed via trial and error. First, we used two injection techniques reported in people, 19 cats 17 and dogs, 18 where the needle is inserted at the ventro-lateral (VL) orbit (Figure 1(a)) or the dorso-medial (DM) orbit using a 75° estimated needle angle to the orbit floor (DM-75°; Figure 1(b)). As the DM seemed to result in vascular intracranial contrast, the needle angle to the orbit floor was changed to 45° (DM-45°; Figure 1(b)). Finally, two more injection sites were investigated: the medial canthus (MC; Figure 1(c)), which was reported in dogs, 18 and the mid-ventral (MV; Figure 1(d)), which was investigated in order to avoid the retro-orbital plexus of rats. 20 A volume of 0.1 mL/100 g was used based on extrapolation from cat studies, 17 which resulted in some exophthalmos, reported previously in cat and dog cadavers.17,18 A supplement of another 0.1 mL/100 g was tested in two eyes with the DM-75° technique, but this resulted in severe exophthalmos and was not assessed further.

Peribulbar injection techniques in rats. Needle insertion is shown at (a) the ventro-lateral (VL), (b) dorso-medial with 75° angle to the orbit floor (DM-75°) or 45° angle (DM-45°), (c) the medial canthus (MC) and (d) mid-ventral (MV).
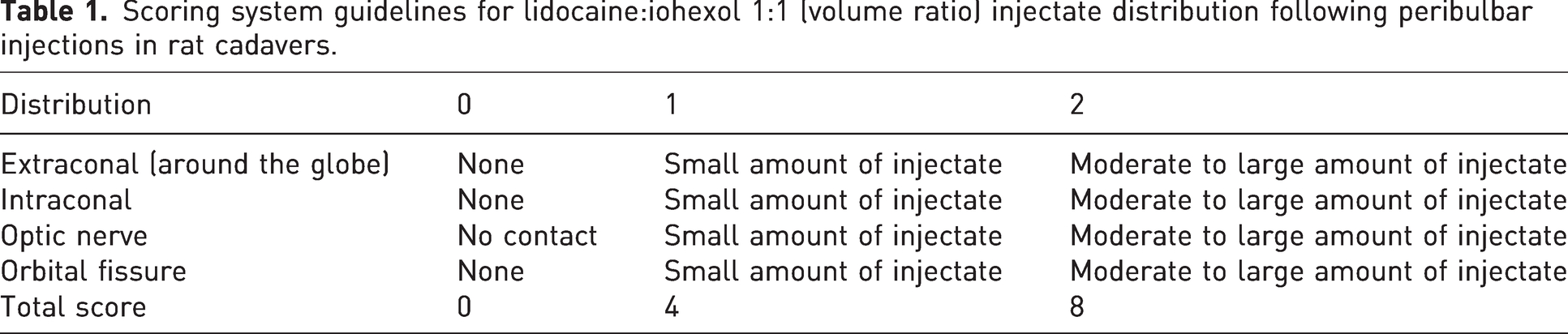
Computed tomography (CT; Philips MX8000 IDT; Philips Medical Systems Technologies Ltd, Cleveland, OH) was used to image injectate distribution and to compare the four injection techniques. CT scans were performed using an ‘EAR’ protocol with contiguous transverse slices 0.8 mm thick, a KV of 90 and a MAS of 150. A board-certified veterinary radiologist (K.B.), who was masked to the technique used, reviewed the CT images using an open-source image analysis software programme (Horos; Horos Project) in bone and soft-tissue window. Injectate distribution was scored at four locations: extraconal, intraconal, around the optic nerve and at the orbital fissure (scale 0–2 for each location; 0 = none, 1 = good, 2 = excellent), and the total scores were summarised (scale 0–8, where 0 = none and 8 = excellent; Table 1). Injectate distribution likely to produce successful anaesthesia was defined as moderate to large intraconal distribution and moderate to large optic nerve contact (Table 1). This assessment method was previously used to develop PBA techniques in cat and dog cadavers.17,18 Additionally, complications such as accidental intraocular, intravascular or intra-thecal injectate were recorded.
Scoring system guidelines for lidocaine:iohexol 1:1 (volume ratio) injectate distribution following peribulbar injections in rat cadavers.
Part 2: Exploring PBA techniques and the volume required in an experimental setting
Two rats (n = 4 eyes) were used in a randomised, masked, crossover study design with a two-week washout period between treatments. The two superior techniques with the highest total score from part 1 of the study were used (DM-75° and MC). Each rat was injected twice with both techniques (n = 2 per technique), each technique in a different eye. Randomisation of treatments and the eye to be treated (right or left) was performed using a computer-generated random list (https://www.random.org/lists/). Two volumes of bupivacaine hydrochloride 0.5% (Marcain heavy; Aspen Pharma Trading Ltd, Dublin, Ireland) were tested. In the first session, a volume of 0.1 mL/100 g (5 mg/kg) was used (based on the rat cadaver study), but since severe exophthalmos was observed and anaesthetic effects were excessively prolonged, the volume was reduced to 0.05 mL/100 g (2.5 mg/kg) in the second session (n = 2 per volume).
Prior to each injection session, rats underwent baseline general ophthalmic examination by a veterinarian, after which the following parameters were recorded. Corneal sensitivity was recorded as measured via corneal touch threshold (CTT) using a Cochet–Bonnet esthesiometer (Luneau Ophtalmologie, Chartres Cedex, France). Briefly, a fully extended thin nylon filament is placed in contact with the central cornea. If no blink occurs, the length of the nylon filament is decreased in 0.5-cm increments until the rat demonstrates a blink reflex in response to at least three of five stimulations. 21 Lack of corneal sensitivity was recorded when the rat did not blink in response to the shortest filament length of 0.5 cm. Periocular skin sensitivity (PSS) to mechanical stimuli was measured using von Frey filaments (North Coast Medical, Inc., San Jose, CA) applying gentle pressure that caused an observable indentation of the skin at four locations around the orbit: dorsal, ventral, medial and lateral. Six von Frey filaments equivalent to pressures of 1, 10, 26, 60, 180 and 300 g were used in ascending order. Due to the high sensitivity of the periorbita, a blink reflex will occur immediately, unless the periorbita is anaesthetised. 13 Lack of PSS was recorded when the periorbita did not responded to the 300 g filament.
Following these baseline readings, rats were anaesthetised with isoflurane in 100% oxygen in a rat induction chamber and then via a nose cone. Rats were positioned in sternal recumbency and baseline IOP was measured using a rodent rebound tonometer (TonoLab; iCare TonoVet, Vantaa, Finland). This instrument takes six readings and displays an average IOP and its statistical error. One averaged reading with a minimal statistical error was recorded per eye. Following tonometry, a PBA injection was performed. Approximately two thirds of the length of a needle (the same needle as in the cadaver part of the experiment) was inserted in close proximity to the orbital wall to avoid accidental damage to the globe. Additionally, negative pressure was applied prior to injection in order to avoid intravascular administration. IOP was measured at 1, 5 and 10 minutes post injection, and then isoflurane was discontinued. As soon as the rats regained the righting reflex, CTT and PSS were assessed on both injected and non-injected eyes as previously described every 20 minutes for up to three hours and then every 30 minutes for up to four hours and finally once an hour until six hours post injection. If CTT and PSS did not return to baseline values at six hours, measurements were repeated every 24 hours post injection until baseline values were recorded. The person (A.E.) measuring IOP, CTT and PSS was masked to the treatment but not to the volume used at each session.
Rats were monitored for two more weeks following the second injection to assess any potential side effects and were then euthanised with an isoflurane overdose followed by decapitation. The eyes and periorbital tissue (in situ) were removed gently, fixated in formaldehyde 4% and sent for histopathological analysis by a certified veterinary pathology laboratory that was unaware of the treatments. Globe and periocular tissue were evaluated histologically at three anatomical levels: (a) anterior to the globe, (b) at the middle of the globe and (c) posterior to the globe.
Statistical analysis
Normal distribution of the results was evaluated using the Shapiro–Wilk test (as well as visual assessment of plotted data). Normally distributed data are presented as the mean±standard deviation, while data with non-normal distribution are presented as median (range; minimum–maximum). Data analysis was only performed for part 1 of the study, but VL was not compared with the other techniques because of the small sample size (n = 2). The Kruskal–Wallis test or Mann–Whitney U-test with Dunn’s correction for multiple comparisons was used to compare the CT scorings between the techniques. Due to the small sample size used in part 2, statistical analysis to compare the effect of technique, volume or time was not possible. Therefore, we used descriptive statistics to evaluate our findings. Significance was set at p < 0.05. All data were analysed using GraphPad Prism v7.0 (GraphPad Software, San Diego, CA).
Results
Part 1: Developing PBA injection technique in rat cadavers
Eighteen fresh rat cadavers (11 males and 7 females; 6 Cohen Diabetic and 12 Brown Norway rat strains) aged 5.7 ± 3.0 months and weighing 353 ± 192 g (males 389 ± 217 g; females 298 ± 126 g) were used one to two hours after sacrifice. The VL injections were performed in two eyes (n = 2), and preliminary, subjective CT assessment demonstrated poor injectate distribution (injectate spreading ventral and lateral to the globe). Therefore, this technique was not assessed further and could not be compared statistically with the other techniques. The DM-75° technique was tested in the largest number of eyes (n = 14) because only later was it realised that vascular intracranial contrast spread occurred frequently with this method. A smaller number of eyes were used to evaluate the remaining techniques: DM-45°, n = 5 eyes; MC, n = 8 eyes; and MV, n = 7 eyes. Normality was observed with DM and MV techniques, but MC was not normally distributed. Therefore, non-parametric tests were chosen for comparison between the techniques.
Median injectate distribution scores were higher (demonstrating better distribution) using the DM-75° and MC techniques compared with the MV technique, although this difference was not statistically significant (DM-75°, p = 0.137; MC, p = 0.162; Figure 2), while DM-75° and MC scores were almost identical (p = 0.938; Table 2). When looking at injectate distribution into important structures that were previously correlated with successful local anesthesia,13,14 the median orbital fissure score of the DM-75° technique was significantly higher than MV (p = 0.024), and the median intraconal distribution score of the MC technique was significantly higher than DM-75° (p = 0.044; Table 2 and Figure 2). Distribution around the optic nerve did not show significant differences between injection techniques (p = 0.3294), although there was a tendency for the MC technique to produce superior distribution compared with the MV technique (p = 0.078; Figure 2).
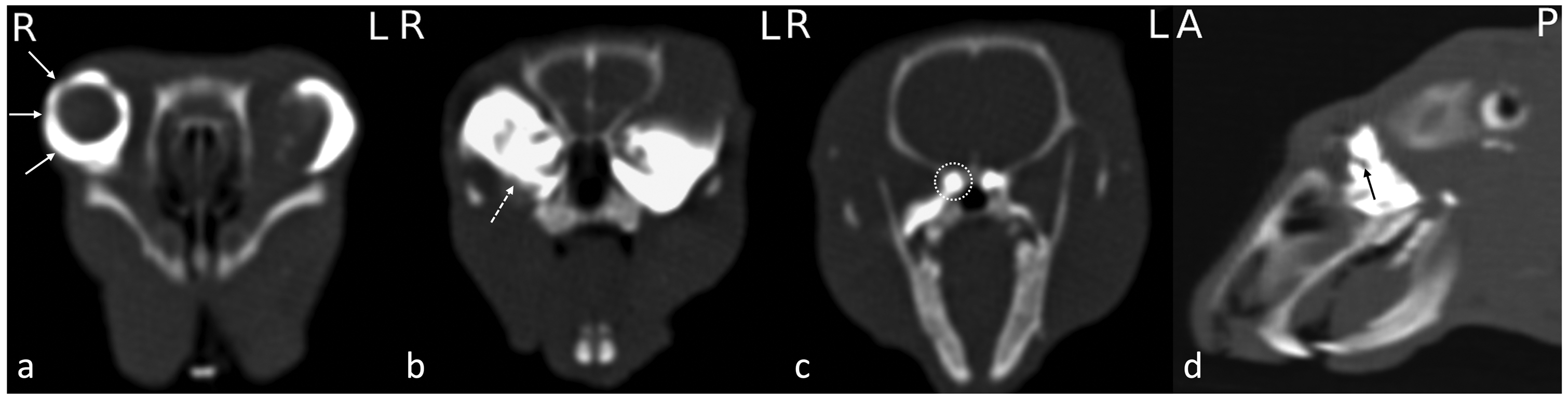
Computed tomography images of peribulbar injection techniques in a rat cadaver transverse to the level of the globe (a), intraconal space (b), and orbital fissure (c) and sagittal to the level of the optic nerve (d). Needle insertion was performed at the medial canthus (MC) on the right (R) eye and at the mid-ventral (MV) on the left (L) eye. There is excellent right sided distribution of the injectate (lidocaine:contrast agent 1:1 volume ratio) at the extraconal (solid arrow), intraconal (dashed arrow), orbital fissure (dashed circle) and around the right optic nerve (black arrow). There is comparatively less left-sided injectate in the intraconal space and around the optic nerve.
Median (minimum–maximum) distribution scores of four peribulbar injection techniques in rats: dorso-medial-angle of 75° (DM-75°), DM-angle of 45° (DM-45°), medial canthus (MC), mid-ventral (MV) and ventro-lateral (VL) using 0.1 mL/100 g of contrast agent (iohexol) with lidocaine 1:1 volume ratio in 36 rat cadaver eyes.
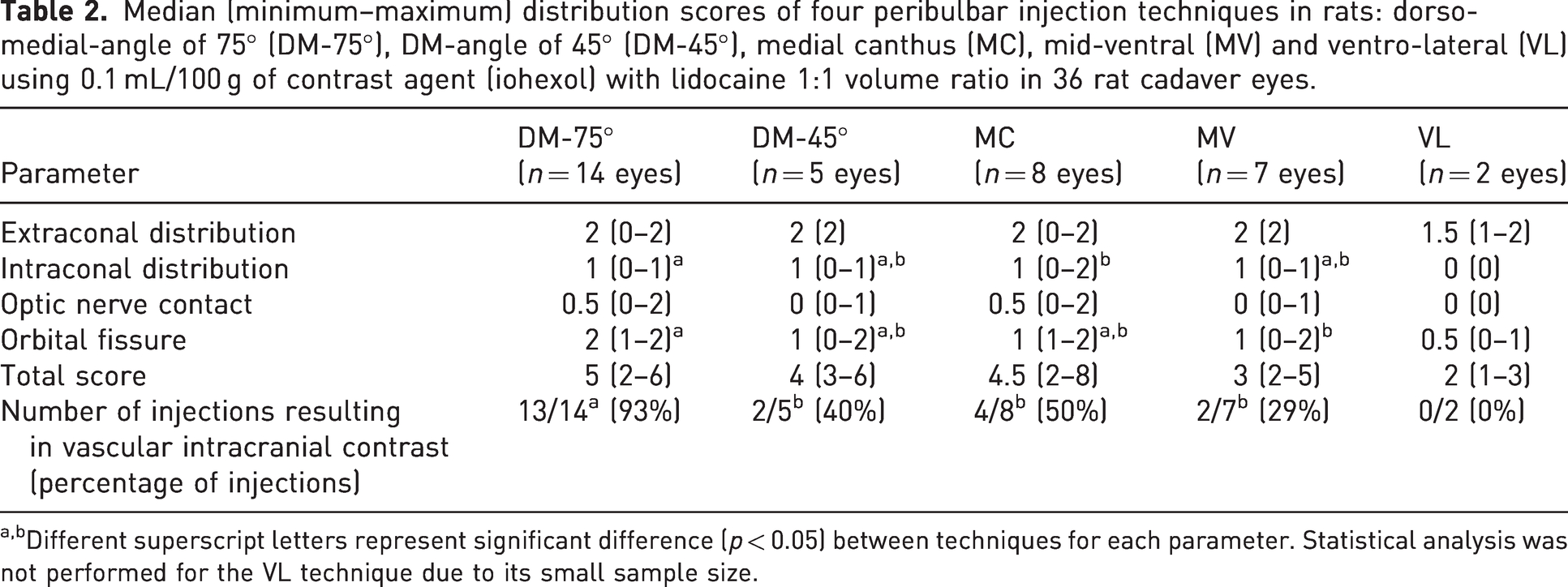
Different superscript letters represent significant difference (p < 0.05) between techniques for each parameter. Statistical analysis was not performed for the VL technique due to its small sample size.
CT images showed that none of the techniques resulted in injectate distribution into the globe or intrathecally. However, vascular intracranial contrast was observed following some of the injections in all treatment groups except the VL technique (Table 2). This observation was significantly different between treatment groups, with the DM-75° technique resulting in higher probability of vascular intracranial contrast spread in comparison to all other treatments (p = 0.015). Based on the total score trend and the better orbital fissure and intraconal distribution of the DM-75° and MC injections, respectively, these techniques were chosen to be tested in part 2 of the study.
Part 2: Exploring PBA techniques and the volume required in an experimental setting
Two Sprague Dawley male rats (n = 4 eyes) aged eight and a half weeks with a body weight of 294–303 g (first session) and 339–360 g (second session) were used. Following anaesthesia, the median baseline IOP in all four eyes was 19 (range 18–21; first session) and 17 (range 14–23; second session). Following all PBA injections, IOP tended to increase, especially when the higher volume was used, while in the non-injected eyes at each session, IOP tended to decrease (Table 3).
Individual intraocular pressure (IOP) readings (mm Hg) measured with a rebound tonometer in two rats (n = 4 eyes) anaesthetised with isoflurane in 100% oxygen before and after (time in minutes) peribulbar anaesthesia (PBA) via medial canthus (MC; n = 2) or dorso-medial at an angle of 75° to the orbit floor (DM-75°; n = 2) with 0.5% bupivacaine at a volume of 0.05 (n = 2) or 0.1 (n = 2) mL/100 g (i.e. each rat was injected twice with a two-week washout period, once with each technique, each time with a different volume).
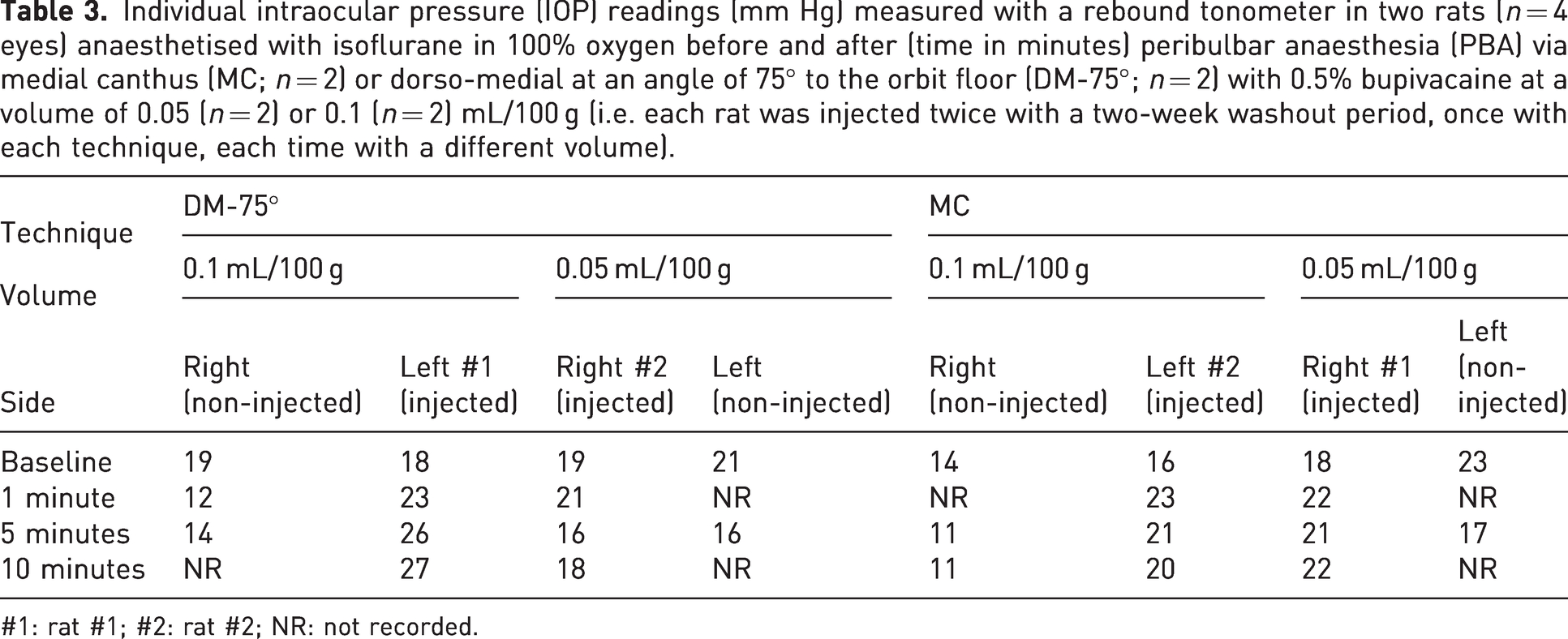
#1: rat #1; #2: rat #2; NR: not recorded.
The median total anaesthesia time for all sessions was 22 (range 21–33) minutes. Recovery from anaesthesia post all PBA injections was quick, and the righting reflex returned in all rats within a median of eight (range 6–10) minutes from isoflurane termination. Median baseline CTT in all eyes was 4.5 (range 4.0–5.0) cm. Following both PBA injection techniques and both volumes, CTT decreased to 0–0.5, demonstrating corneal insensitivity (Figure 3), while in the non-injected eyes at 20 minutes, the baseline CTT was recorded, except for one eye that had 4.5 instead of 5.0, and then at 40 minutes, it resumed the baseline value. Eyes injected with the higher volume did not regain baseline CTT (MC, 3.5 instead of 4.5 cm; DM-75°, 4.0 instead of 4.5 cm) at two weeks post injection, while eyes injected with the lower volume resumed baseline CTT at 24 hours post injection (Figure 3).
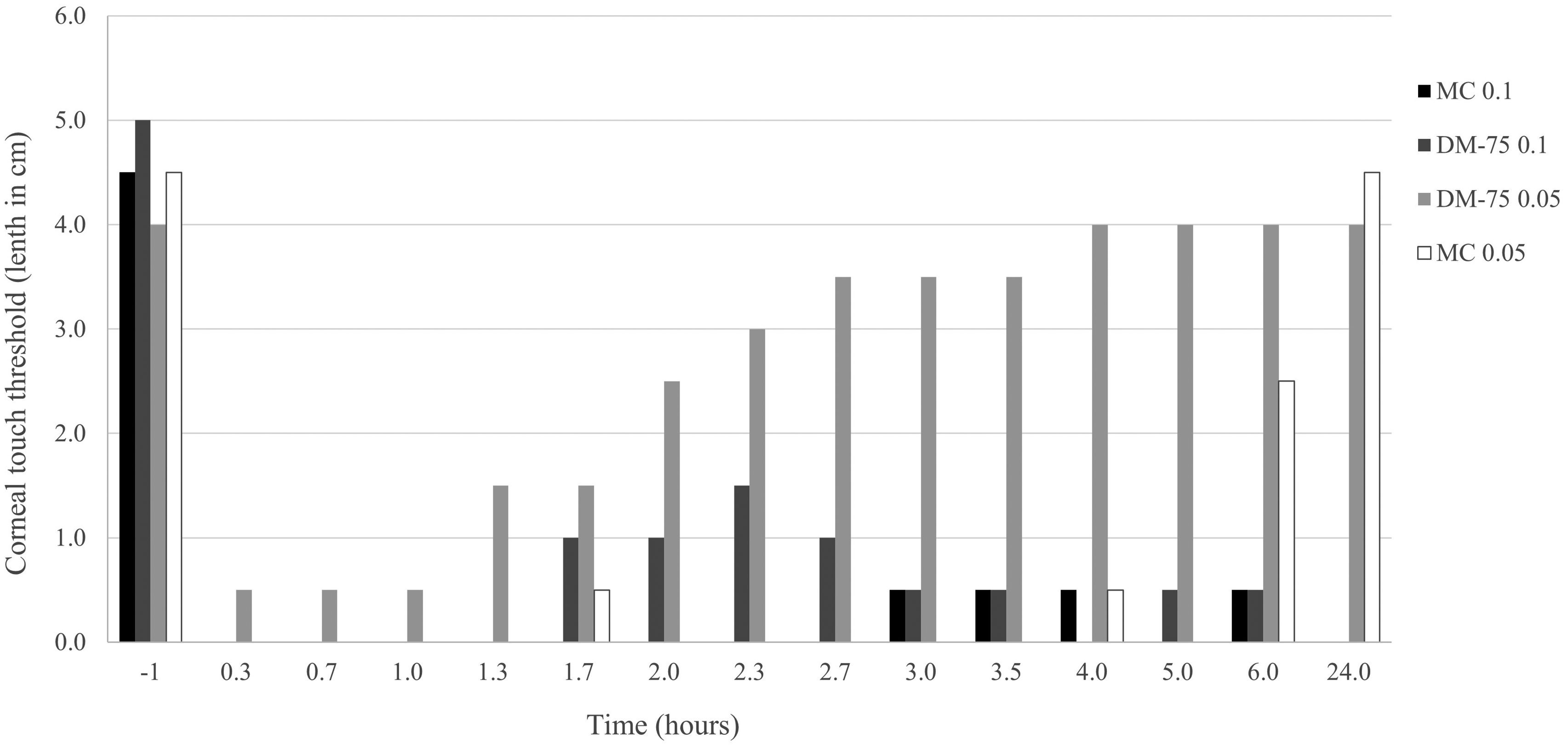
Individual corneal touch threshold (CTT) readings measured in centimetres with a Cochet–Bonnet esthesiometer in two rats (n = 4 eyes) before and after peribulbar anaesthesia via medial canthus (MC) or dorso-medial at an angle of 75° to the orbit floor (DM-75°) with 0.5% bupivacaine at a volume of 0.05 or 0.1 mL/100 g (each rat was injected once with MC and once with DM-75°, each technique with a different volume). When no response occurred at a filament length of 0.5 cm, it was recorded as 0 (i.e. complete corneal insensitivity). At two weeks from injection of the higher volume, the eyes did not regain baseline CTT (MC had 3.5 instead of 4.5 cm, and DM-75° had 4.0 instead of 4.5 cm).
At baseline, all PSS periorbital test sites responded to the lowest pressure of 1 g Von Frey filament. The PSS in the non-injected eyes responded to the minimal pressure of 1 g Von Frey filament in all periorbital test sites at the 20-minute time point, while the injected eyes using both techniques and both volumes did not respond to a pressure of 300 g. Following injection of the higher volume with both techniques, the sensations in the dorsal and lateral periorbital test sites recovered at 24 hours, while at the ventral and medial sites, they recovered at 24 hours (MC) and at four to five hours (DM-75°). Following injection of the lower volume, sensation resumed at the dorsal, lateral, ventral and medial periorbital test sites at 3.5, 1.7, 3.5 and 1.7 hours (MC) and at 4, 4, 1.3 and 1.3 hours (DM-75°), respectively.
Adverse effects observed following both PBA injection techniques were considered to be minor and included exophthalmos and conjunctival oedema, which were more severe and took longer to resolve following injection of the higher volume. Exophthalmos resolved within 5 days (both techniques at 0.1 mL/100 g), 24 hours (MC, 0.05 mL/100 g) and 4 hours (DM-75°, 0.05 mL/100 g). Conjunctival oedema was not observed following injection of the lower volume and resolved within 160 (MC) and 40 (DM-75°) minutes following injection of the higher volume.
Histopathology findings were similar in all four eyes. Some haemorrhage was observed at the sections of level 1 and slight oedema at levels 2 and 3. In the left eye of rat number 2 (injected with DM-75° 0.1 mL/100 g), the iris was attached to the dorsal aspect of the lens, but no other uveitis-associated changes were observed.
Discussion
This is the first study assessing PBA, an ophthalmic regional anaesthesia technique in rats. Regional anaesthesia is an important part of multimodal pain management in humans 22 and in companion animals, 23 and it is likewise likely to reduce perioperative pain and improve laboratory animals’ well-being and welfare. 24
Although PBA is commonly used in other species, ophthalmic regional anaesthesia can also be provided in large animals using a different technique: retrobulbar anaesthesia (RBA), where the injection is performed directly into the extraocular muscle cone behind the globe.10 –12 Due to the small size of rats, it would be very difficult to know whether the needle is inside the cone, making this technique less suitable in this species. Additionally, even in larger companion animals, the success rate of RBA has been questioned.14,25 RBA is also thought to pose more risk to intraconal structures. 11 Therefore, it was decided not to investigate RBA in the present study. PBA was developed because it seemed to be more practical in the rat. It is administered outside the extraocular muscle cone, and hence it is easier to perform and less likely to cause injury to vessels and nerves that pass inside the cone. 11 PBA relies on local anaesthetic diffusion intraconally and also results in periorbital diffusion, which provides additional analgesia to the eyelids.13,26
The techniques that we selected to develop and which were evaluated in the current study were based on data reported in dogs and cats. 12 Because of differences in rat ophthalmic anatomy compared with carnivores (e.g. rat eyes positioned laterally, producing wide monocular visual field and narrow binocular visual field compared with carnivore eyes positioned frontally, producing narrow monocular visual field and wide binocular visual field), we used trial and error in order to adjust the PBA injection technique for use in rats. The first injection techniques evaluated were VL and DM-75°. The distribution of the injectate following VL was poor. Therefore, this technique was abandoned. Poor distribution following VL injection was also reported in cats 17 and could be explained by the lack of a complete bony shelf at the ventral aspect of the orbit in cats and rats, which results in the injectate moving ventrally and away from the desired nerves. The DM-75° technique resulted in high occurrence of intracranial vascular contrast. Therefore, we tried to optimise this method by changing the needle angle to 45° as well as assessing other techniques. Because eventually all the techniques involving medial injection in close proximity to the retro-orbital plexus resulted in some intracranial contrast distribution, we hypothesised that this could have been caused by post-mortem changes and vessel leakage via the retro-orbital plexus. 20 Recovery from anaesthesia following all PBA injections in the experimental rats was quick, suggesting that intracranial vascular leakage of bupivacaine was less likely to occur. However, this should be evaluated in further safety studies.
PBA was reported to cause significantly increased IOP for 10 minutes in cats 13 but not in dogs. 14 It is difficult to assess the effect of PBA on IOP in the present investigation, as the sample size was too small. The tendency to decrease IOP observed in the non-injected eyes most likely contributed to the use of isoflurane anaesthesia, as has been previously reported in rats. 27 The use of isoflurane anaesthesia may have masked a further increase in IOP following the PBA injections. Therefore, these injections should be used cautiously in cases where increased IOP is not desired.
Lidocaine was used in the cadavers because it is cheap. However, in live rats, bupivacaine was preferred, since it has a longer half-life compared with other local anaesthetics in rodents. 24 Both DM-75° and MC techniques were able to provide local anaesthesia as demonstrated by decreased CTT and PSS measurements for several hours following injection. The volume that resulted in good distribution in cadavers was too large for use in live rats and resulted in conjunctival oedema, severe exophthalmos and a possible high pressure on various orbital structures including nerves. The duration of effect was excessively long, and baseline CTT was not resumed, which may suggest partial ciliary nerves damage. Following death, the globes usually lose some volume and shrink. 28 Therefore, the use of cadavers probably underestimated the exophthalmos observed in live rats. Other adverse effects of bupivacaine- or mepivacaine-induced extraocular muscle damage were previously reported following ophthalmic regional anesthesia.29,30 Thus, the use of PBA should depend on the planned procedure and desired outcome; 0.1 mL/100 g bupivacaine can be used prior to enucleation, but in other ophthalmic surgeries, the use of 0.05 mL/100 g can provide ophthalmic local analgesia for several hours with fewer adverse effects.
Study limitations include the non-optimal use of a CT that was developed for use in companion animals, while a micro-CT could have produced better images. Different rat cadavers’ strains and weights were used, as these were made available for the study, whereas results may have been more reliable if one strain and similar body weight were used. Additionally, the cadaver part was not performed on an equal number of eyes, and the in vivo part was performed on a different rat strain from the cadaver part and included only four eyes, two techniques and two different volumes. Therefore, statistical analysis could not be performed. Only two experimental rats were used for technique development to accommodate the 3 Rs (reduction in experimentation) because the appropriate volume for use in rats was unknown. A follow-up study using an appropriate sample size based on the results of the present study should be performed to assess the clinical efficacy of these techniques. Following injections, several IOP measurements were missing in the non-injected eyes, and generally it would have been better to continue the IOP follow-up in awake rats. However, complete immobility is necessary for rebound tonometry and could not have been achieved in awake rats. Additionally, it would have been good to investigate injectate distribution via CT in the live rats, but this was not possible due to technical difficulty in transferring the SPF rats to the CT facility.
Conclusions
Performing PBA using DM-75° or MC injection techniques with 0.05 mL/100 g of a local anaesthetic is likely to provide ocular and periocular regional anaesthesia and analgesia in rats. One of the advantages of PBA is that it is relatively simple to perform. Therefore, most veterinary staff, whether working in laboratory setting or in exotic practice, and people performing ophthalmic microsurgery on rodents should be able to perform this regional anaesthesia technique in order to produce better analgesia. The findings of the present study provide an alternative pain management for rats that are subjected to painful ocular procedures whether for research purposes or for clinical treatment. The results of this preliminary study can be used to assess the efficacy and safety of these techniques in a larger group of rats and their application and benefit for animal welfare as a part of multimodal pain management in rat glaucoma models.
Footnotes
Acknowledgements
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by the Universities Federation for Animal Welfare (UFAW; Grant application 34-19/20).