
Abstract
Eight male Dorper sheep were anesthetized with isoflurane to evaluate the effects of anesthesia on cardiopulmonary parameters, echocardiographic variables and cardiac output (CO) using echocardiography methods compared with thermodilution. Heart rate (HR), respiratory rate (f R), systolic arterial pressure (SAP), diastolic arterial pressure (DAP) and mean arterial pressure (MAP) were recorded. CO was obtained by thermodilution using a pulmonary artery catheter (COTHERMO), Teichholz method (COTeichholz) and pulmonary artery Doppler (COPA). Echocardiographic variables (interventricular septum (IVSs and IVSd), left ventricular chamber (LVIDs and LVIDd) and left ventricular free wall (LVFWs and LVFWd) in systole and diastole, respectively; ejection fraction (EF%); fractional shortening (FS%); pulmonary artery pressure gradient (PG), peak flow velocity (Vmax) and velocity-time integral of the flow (VTI) were recorded. All parameters were measured at baseline and every 15 min during the transanesthetic and recovery periods (T15, T30, T45, T60, T15REC, T30REC, T45REC, T60REC). Significant reductions in SAP, MAP, DAP and COTHERMO were observed during the transanesthetic period. Bland–Altman analysis comparing COTHERMO and COTeichholz showed mean biases of 0.49 l min–1 (limits of agreement (LOA), –2.12 to 3.12 l min–1), 0.56 l min–1 (–1.82 to 2.96 l min–1) and 0.75 l min–1 (–2.04 to 3.56 l min–1) at baseline, during anesthesia and in recovery, respectively. For COTHERMO and COPA, mean biases were −0.53 l min–1 (–2.90 to 1.90 l min–1), –0.66 l min–1 (–4.72 to 3.39 l min–1) and −0.94 l min–1 (–4.62 to 2.73 l min–1) at baseline, during anesthesia and in recovery, respectively. Isoflurane decreases blood pressure and CO without affecting echocardiographic parameters. CO values obtained by thermodilution and echocardiography methods are not interchangeable.
Introduction
Sheep are used extensively as animal models in cardiovascular research due to their anatomical and physiological similarities to humans and their adaptive responses to disease.1–3 The species has been used in the modeling of ischemic diseases, 4 cardiomyopathies, valvular diseases, 5 and general cardiovascular surgeries,3,5–7 with most of these studies conducted under anesthesia. The increasing application of sheep in translational medicine emphasizes the need to validate anesthetic protocols as well as cardiovascular monitoring and diagnostic methods appropriate for the species and specific research contexts.
Among cardiovascular monitoring methods, transthoracic Doppler echocardiography stands out due to its advantages, such as being minimally invasive, low-cost and being highly repeatable. This tool is used widely in both clinical and research settings because it enables morphological, structural, functional and hemodynamic assessments. However, echocardiography in sheep poses challenges due to anatomical peculiarities, the presence of the rumen, the heart’s position in the thorax and variations in thoracic conformations across breeds within the species.8,9 Furthermore, the reliability of the examination can be affected by species- and breed-related variations and by clinical changes such as alterations in vascular tone, myocardial kinetics and blood pressure, which arise from varying anesthetic protocols. 10
Previous studies have employed bidimensional, Doppler and M-mode echocardiography under isoflurane anesthesia to evaluate the success of surgical techniques, such as valve implantation, 5 induction of post-ischemic lesions and assessment of ventricular dysfunctions.11,12 Although specific results on the impact of anesthesia on echocardiographic measurements are lacking, De Vleeschauwer et al. highlighted the significance of sedation or mild anesthesia as an alternative to general anesthesia to mitigate stress from restraint without impact of general anesthetics on echocardiographic results. 5 In sheep, isoflurane at 2.3 V% reduces blood pressure by decreasing peripheral vascular resistance (PVR) without altering stroke volume (SV) or cardiac index (CI). 13 Similar reductions in blood pressure have been observed in horses, 14 cattle, 15 dogs and cats under anesthesia with species-specific minimum alveolar concentration (MAC) levels.11,16
The aims of this study were: to (a) assess the impact of isoflurane anesthesia on cardiopulmonary parameters, echocardiographic evaluation and cardiac output (CO), and (b) compare the agreement between different methods for determining CO by echocardiography with thermodilution method in isoflurane-anesthetized sheep. We hypothesized that isoflurane anesthesia would have a minimal impact on cardiopulmonary parameters and the echocardiographic examination, and that the CO obtained by echocardiography using both the Teichholz method and pulmonary artery Doppler would be reliable for monitoring these animals during isoflurane anesthesia.
Materials and Methods
The experimental protocol was approved by the Federal University of Goiás (UFG) Ethics Committee on the Use of Animals (approval number 052/19), and conducted in accordance with Brazilian law and the norms of the National Council of Animal Experimentation (CONCEA).
Animals
Eight clinically healthy, non-castrated male Dorper sheep (Ovis aries), aged three to five months and weighing 26.28 ± 1.24 kg, were used in this study. Male sheep were chosen before reaching the age of sexual maturity to avoid any interaction with hormonal variations related to the sexual maturity and estrous cycle of females. The study was performed in a research facility with ambient temperatures that ranged from 16 °C to 34 °C, and relative humidity varied between 47% and 65%. During the experimental stage, the animals were housed indoors at room temperature and humidity in collective pens with hay and wood shavings bedding. They had access to a forage area, water ad libitum, and were fed commercial feed for the species once a day. All animals were vaccinated and dewormed with ivermectin and levamisole before the experiment.
The animals were deemed healthy based on clinical history, physical examinations and previous laboratory tests (blood count, albumin, creatinine, transaminases and gamma-glutamyl transpeptidase). Exclusion criteria included previous diseases, the presence of murmurs on cardiac auscultation and arrhythmias observed by electrocardiography simultaneous with the echocardiographic examination.
Study design
Before sedation, food and water were withheld from the sheep for 18 h and 6 h, respectively. Instrumentation was performed with the animals awake and standing without sedation in order to minimize the influence of other drugs on evaluation of isoflurane anesthesia. They were restrained only with a halter and always kept in pairs until anesthetic induction to minimize separation anxiety. Peripheral venous access was obtained using an 18-gauge catheter in the cephalic vein; arterial access was secured in the middle auricular artery with a 20-gauge catheter, and central access in the jugular vein was established for the passage of a pulmonary artery catheter (Swan-Ganz Catheter 831H-7.5F, Edwards Lifesciences LLC, Irvine, CA, USA).
To gain central access, a 1.5-ml block of 2% lidocaine was administered in the region of the left jugular vein. Subsequently, an introducer (Intro-Flex 8F Percutaneous Introducers and Accessories, Edwards Lifesciences LLC) was placed into the left jugular vein using the Seldinger technique. Once the introducer was positioned, the central pulmonary artery catheter was inserted, aligning its distal end in the right ventricular outflow tract and its proximal end in the right atrium, confirmed by assessing characteristic pressure waves and radiographic examination (portable X-ray Oxson ORANGE 1060HF VET).
The animals were restrained and acclimated to the use of the mask. A trained professional restrained each animal with a halter. For pre-oxygenation, the mask was positioned close to the snout, and oxygen was administered at a flow rate that was gradually increased to 1 l/min over 2 min. This flow was maintained for 5 min. After this, anesthetic induction was initiated with the administration of the inhaled anesthetic. No signs of discomfort that would prevent induction by mask were observed during the study.
After the instrumentation, a 15-min stabilization period was observed, and baseline parameter values (BASAL) were recorded. Anesthesia was then induced using a mask that delivered isoflurane at an expired fraction (EtISO) of 3.5 V%. The animal was intubated with a tracheal tube size 6.5 that was connected to a circular anesthetic circuit, providing 20 ml kg–1 min–1 of oxygen (FiO2) at 100%. The animals were positioned standing with the aid of a species-adapted trunk and ventilated mechanically in controlled pressure mode (VPC) (Fabius Plus; Drägerwerk AG & Co., Lübeck, Germany). This setup maintained a peak pressure of 18 mmHg, positive end-expiratory pressure of 5 mmHg, an inspiratory-expiratory ratio of 1:2, and a respiratory rate (fR) that kept expired carbon dioxide levels (EtCO2) between 35 and 50 mmHg.
Anesthesia was maintained for 60 min after the fraction of expired isoflurane (EtISO) stabilized at 2.2 V%, which is 1.5 times the MAC for the species (1.47–1.53 V%), 17 monitored by a calibrated sidestream anesthetic gas analyzer (Vamus, Drägerwerk AG & Co.). Monitoring occurred every 15 min (T15, T30, T45, T60) after stabilization of EtISO at 2–2.2 V% and continued for an additional 60 min during the anesthetic recovery period (T15REC, T30REC, T45REC, T60REC).
At the end of the experimental period, the venous, arterial and central catheters were removed, along with the pulmonary artery catheter and its introducer.
Data collection
Cardiorespiratory parameters were assessed using a previously calibrated multiparameter monitor (DIXTAL DX-2010, Manaus, AM, Brazil). Heartrate (HR) and heart rhythm were monitored by electrocardiogram (DII derivation, 25 mm s–1); respiratory rate (fR); invasive blood pressure measurements including systolic arterial pressure (SAP), diastolic arterial pressure (DAP) and mean arterial pressure (MAP) were taken with a transducer positioned at heart level. Arterial blood samples were collected for gasometric analysis to evaluate arterial oxygen partial pressure (PaO2), arterial carbon dioxide partial pressure (PaCO2), pH, base excess (BE) and bicarbonate (HCO3–).
The accuracy of the invasive arterial blood pressure measurement was ensured through standard calibration procedures. The pressure transducer was zeroed and leveled to the level of the animal’s olecranon, which corresponds anatomically to the level of the right atrium. Linearity and dynamic response of the pressure monitoring system were assessed by performing the square wave or fast flush test before each measurement session. This test confirmed adequate damping and fidelity of the pressure waveform, ensuring reliable acquisition of SAP, DAP and MAP.
CO was also measured via thermodilution using a multiparameter monitor (DIXTAL DX-2010, CO Module, Manaus). The setup involved a 7.5-Fr Swan-Ganz catheter and the injection of 5.0 ml of 0.9% sodium chloride solution, chilled to between 0 and 1 °C. Measurements were taken in triplicate, each with a 3-s injection of the ice-cold solution as recommended by the manufacturer, and were performed immediately following the echocardiographic examination by a single operator. The arithmetic mean of these measurements was then calculated.
The body surface area (BSA) of each animal was determined using the formula used by Berman (2003) 19 : [BS = 0.09 × weight (kg)0.67] and CIs were subsequently calculated from the BSA values.
The evaluation of CO using echocardiography-based methods was conducted using a SonoScape S6 ultrasound device (SonoScape Medical Corp., Shenzhen, China) equipped with a multifrequency microconvex transducer (3–8 MHz). For COPA, through the right parasternal window and using this transducer, two-dimensional images of the right ventricular outflow tract were captured, where the diameter of the pulmonary valve annulus was quantified. Color Doppler and pulsed Doppler enabled the acquisition of images of pulmonary artery flow, and measurements of the pulmonary artery pressure gradient (PG), peak flow velocity (Vmax) and velocity-time integral of the flow (VTI) were taken from the flow trace. These were obtained in triplicate by a single examiner and averaged. Following the measurement of VTI (cm) and the diameter of the pulmonary valve annulus, calculations for the SV, the area of the right ventricular outflow tract (RVOT) and the CO were performed using ESV (end systolic volume) in the formulas proposed by Ihlen (1984) 18 : SV [SV (l beat1) = (ESV/2)2 × π × VTI (ml)] and CO [CO (l min–1) = SV (l beat1) × HR (ml min–1)].
In the echocardiographic COTeichholz study, the left ventricle (LV) was examined using the right parasternal window approach, with images captured in the short-axis view at the level of the papillary muscles. Quantitative assessments included the interventricular septum in systole (IVSs) and diastole (IVSd), left ventricular chamber in systole (LVIDs) and diastole (LVIDd), and left ventricular free wall in systole (LVFWs) and diastole (LVFWd). The systolic function indices, ejection fraction (EF%) and fractional shortening (FS%), were calculated. Based on these measurements, the device’s specific software used the Teichholz geometric method to calculate cardiac output.
Statistical analysis
SigmaPlot 11 software (SigmaPlot 11 for Windows, Systat Software, Inc., San Jose, CA, USA) was utilized to calculate the sample size, considering cardiac output as the main variable, a minimum detectable difference in means of 35%, an expected standard deviation of 25% and a statistical power of 0.80. The results of the cardiorespiratory, blood gasometric and Doppler echocardiographic studies are presented as means ± standard deviations (SDs). Statistical analyses were carried out using GraphPad Prism 8 software (GraphPad Prism 8.0 for Windows, GraphPad Software, La Jolla, CA, USA). The normal distribution of the data was verified using the Kolmogorov–Smirnov normality test. Comparisons between evaluation time points with normal distributions were conducted using two-way repeated measures analysis of variance (RM two-way ANOVA), followed by the Tukey test. To investigate the correlation between CO values obtained by different methods (thermodilution versus Doppler-based methods) over time, the Pearson correlation test was performed.
The agreement between the gold standard thermodilution technique (COTHERMO) and the two Doppler echocardiography techniques (COTeichholz and COPA) was assessed using the Bland–Altman test. The mean differences between the CO estimates by the different techniques were defined as bias and determined for all measurement pairs. The SD of these differences was used to calculate the limits of agreement for the pooled data, defined as bias ± SD. For all analyses, a P value of <0.05 was considered statistically significant.
Results
Tables 1 and 2 present the cardiorespiratory and blood gas parameters.
Mean [SD] values of HR, f R, T, MAP, SAP, DAP and CITHERMO in eight sheep submitted to isoflurane anesthesia for 60 min and monitored for up to 120 min.
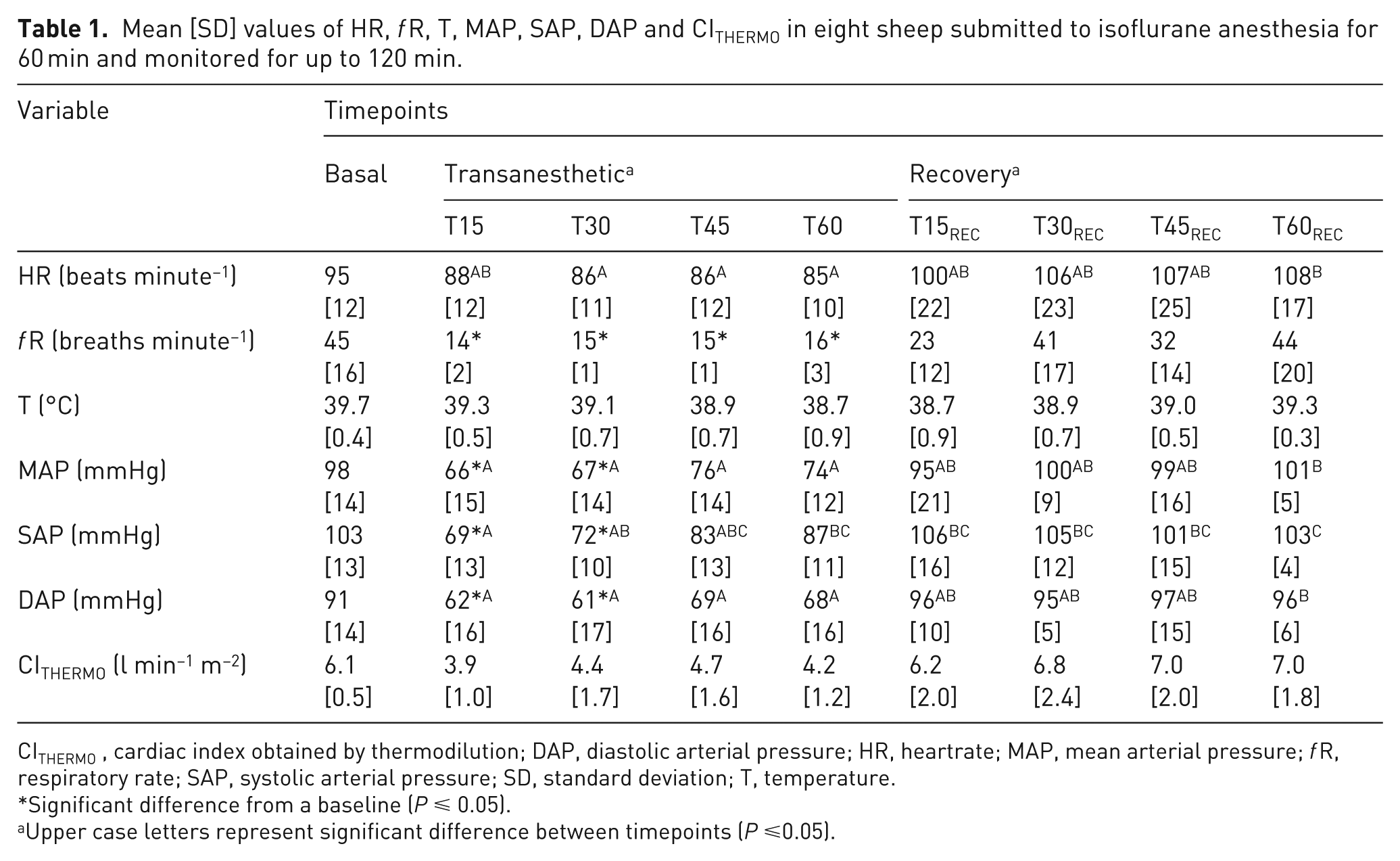
CITHERMO, cardiac index obtained by thermodilution; DAP, diastolic arterial pressure; HR, heartrate; MAP, mean arterial pressure; f R, respiratory rate; SAP, systolic arterial pressure; SD, standard deviation; T, temperature.
Significant difference from a baseline (P ⩽ 0.05).
Upper case letters represent significant difference between timepoints (P ⩽0.05).
Mean [SD] values of pH, PaO2, PaCO2, HCO3– and BE in eight sheep submitted to isoflurane anesthesia for 60 min and monitored for up to 120 min.
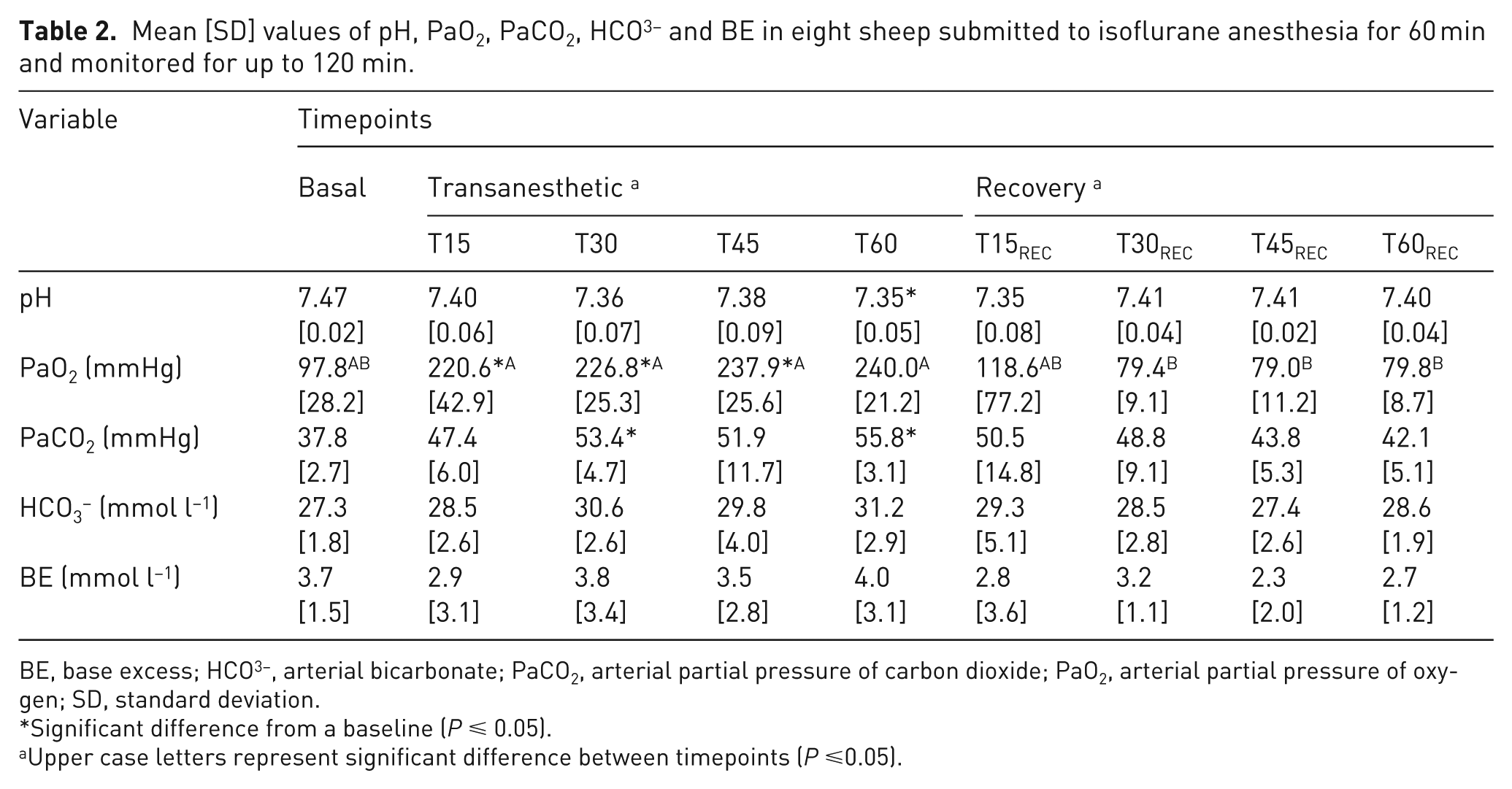
BE, base excess; HCO3–, arterial bicarbonate; PaCO2, arterial partial pressure of carbon dioxide; PaO2, arterial partial pressure of oxygen; SD, standard deviation.
Significant difference from a baseline (P ⩽ 0.05).
Upper case letters represent significant difference between timepoints (P ⩽0.05).
HR showed no significant differences from baseline values during both the anesthetic and recovery periods. Arterial pressures (MAP, SAP and DAP) were lower than baseline at the onset of anesthesia, at T15 and T30 MAP T15 P = 0.03 and T30 P = 0.03; SAP T15 P = 0.02 and T30 P = 0.01; and DAP T15 P = 0.04 and T30 P = 0.04). CO assessed by thermodilution using a pulmonary artery catheter showed significant decreases at T15 (P < 0.01), T30 (P = 0.04) and T60 (P < 0.01) compared with baseline values (Table 3).
Mean [SD] values of COTHERMO, COTeichholz and COPA in eight sheep submitted to isoflurane anesthesia for 60 min and monitored for up to 120 min.
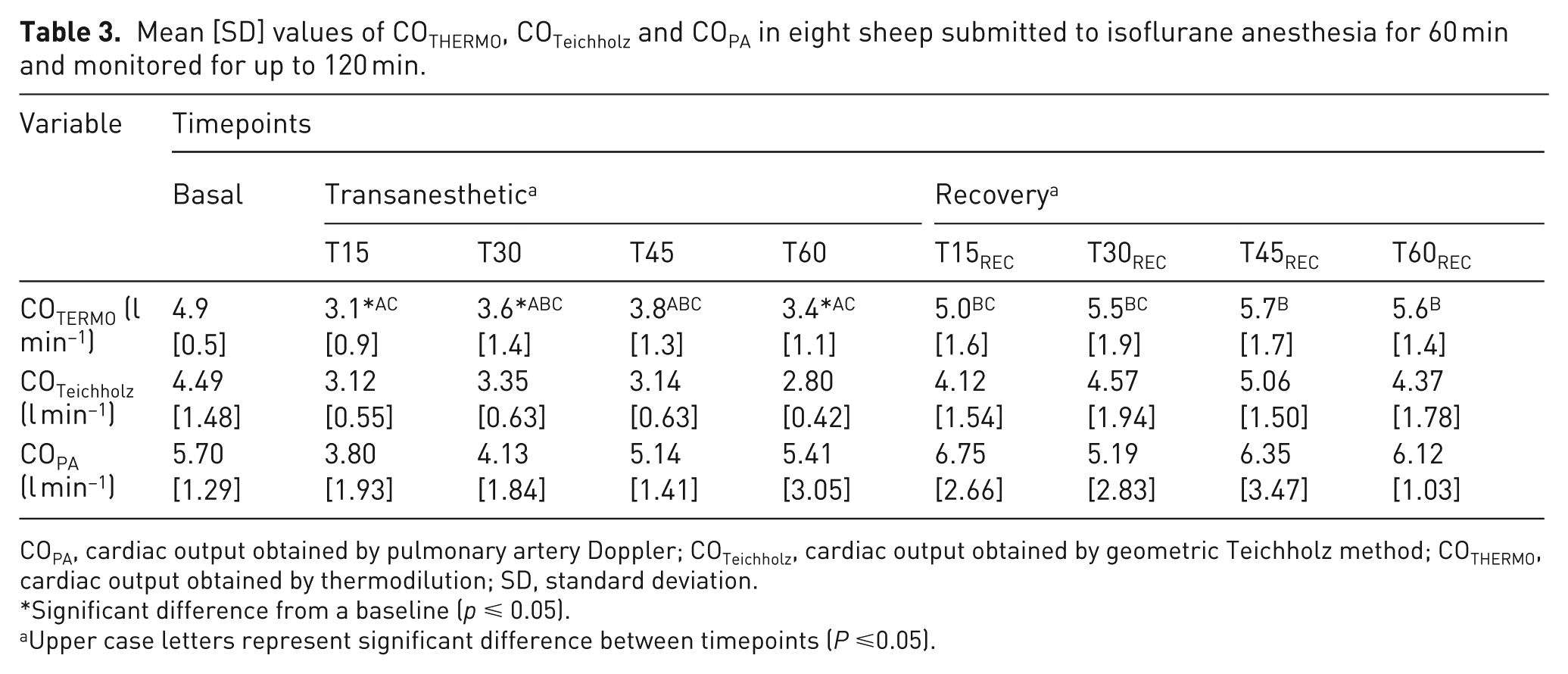
COPA, cardiac output obtained by pulmonary artery Doppler; COTeichholz, cardiac output obtained by geometric Teichholz method; COTHERMO, cardiac output obtained by thermodilution; SD, standard deviation.
Significant difference from a baseline (p ⩽ 0.05).
Upper case letters represent significant difference between timepoints (P ⩽0.05).
In the arterial blood gas analysis, the pH at T60 was significantly lower compared with baseline (P = 0.01) and PaCO2 was significantly higher during the transanesthetic period at T30 (P = 0.01) and T60 (P < 0.01) compared with baseline.
The Doppler echocardiographic parameters showed no statistically significant differences between timepoints (Table 4).
Mean [SD] values of echocardiographic values study of LV, IVSs and IVSd, LVIDs and LVIDd, LVFWs and LVFWd; SFV and DFV, SV; EF% and FS% in eight sheep submitted to isoflurane anesthesia for 60 min and monitored for up to 120 min.
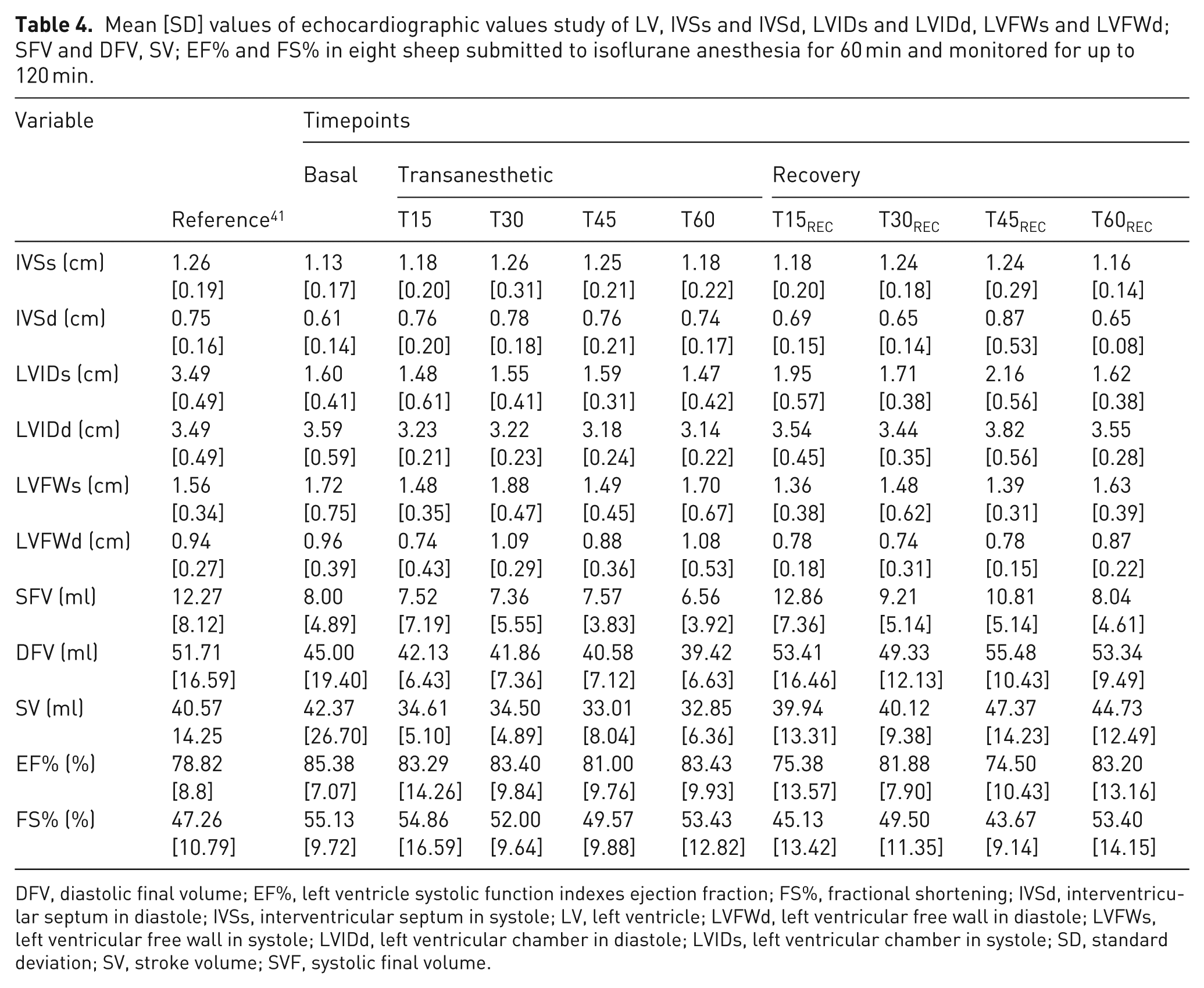
DFV, diastolic final volume; EF%, left ventricle systolic function indexes ejection fraction; FS%, fractional shortening; IVSd, interventricular septum in diastole; IVSs, interventricular septum in systole; LV, left ventricle; LVFWd, left ventricular free wall in diastole; LVFWs, left ventricular free wall in systole; LVIDd, left ventricular chamber in diastole; LVIDs, left ventricular chamber in systole; SD, standard deviation; SV, stroke volume; SVF, systolic final volume.
A comparison of the mean CO values determined by each method revealed no statistical differences between the methods (Figure 1). The agreement between methods by the Bland–Altman method is shown in Figure 2. The comparison between COTHERMO and COTeichholz at baseline showed a mean difference of 0.49 ± 0.339 l min–1 with a lower limit of agreement at −2.12 l min–1 and an upper limit at 3.12 l min–1. During anesthesia, the mean difference was 0.56 ± 1.22 l min–1 with a lower limit of −1.82 l min–1 and an upper limit of 2.96 l min–1. In the anesthetic recovery period, the mean difference was 0.75 ± 1.43 l min–1 with a lower limit of −2.04 l min–1 and an upper limit of 3.56 l min–1. The comparison between COTHERMO and COPA at baseline had a mean difference of −0.53 ± 1.24 l min–1 with a lower limit of −2.9 l min–1 and an upper limit of 1.9 l min–1. During anesthesia, the mean difference was −0.66 ± 2.07 l min–1 with a lower limit of −4.72 l min–1 and an upper limit of 3.39 l min–1. Finally, in the anesthetic recovery period, the mean difference was −0.94 ± 1.87 l min–1 with a lower limit of −4.62 l min–1 and an upper limit of 2.73 l min–1.
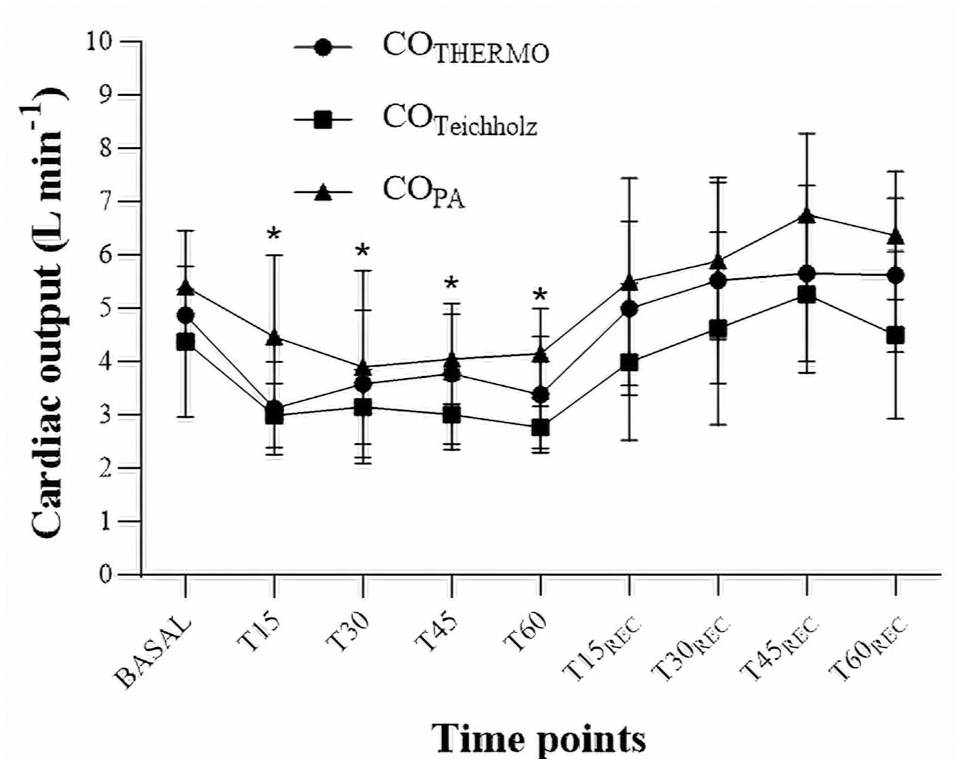
Mean ± SD values of COTHERM, COTeichholz and COPA in eight sheep submitted to isoflurane anesthesia for 60 min and monitored for up to 120 min. *Significant difference from a baseline within COTHERMO (P ⩽ 0.05). COPA, cardiac output obtained by pulmonary artery Doppler; COTeichholz, cardiac output obtained by geometric Teichholz method; COTHERMO, cardiac output obtained by thermodilution; SD, standard deviation.

Agreement between methods by the Bland–Altman method. Evaluation of the difference in COTHERMO by echocardiography with COTeichholz at basal time (a), during the transanesthetic period (b) and during anesthetic recovery (c); difference in COTHERMO with COPA at basal time (d), during the transanesthetic period (e) and during anesthetic recovery (f). The bias is indicated by the solid line and the lower and upper LOA by the dashed lines. COPA, cardiac output obtained by pulmonary artery Doppler; COTeichholz, cardiac output obtained by geometric Teichholz method; COTHERMO, cardiac output obtained by thermodilution; LOA, limits of agreement; SD, standard deviation; SDMAX, maximum SD of the differences; SDMIN, minimum SD of the differences.
The correlation coefficients between COTHERMO and COTeichholz were low at baseline and during the transanesthetic period (r = 0.3084 and r = 0.1087, respectively) and moderate during the anesthetic recovery (r = 0.6298). The correlation between COTHERMO and COPA was low at baseline, during anesthesia, and in the anesthetic recovery (r = –0.1986, r = –0.2182 and r = 0.3508, respectively).
Discussion
In this study, isoflurane anesthesia did not cause significant changes in cardiopulmonary variables HR and fR, except for a reduction in blood pressure during the transanesthetic period. This reduction was not classified as hypotension, and no treatment was administered. The lack of changes in HR between anesthetized animals and the baseline period in this study was similar to previous findings under isoflurane anesthesia at 1 MAC, where HR stability has been documented in sheep,13,20,21 cattle and goats.20,22 Although statistically significant differences were noted between anesthetic and recovery timepoints, these were not considered clinically relevant when compared with previously reported reference values for the species (81 ± 13). 40 The decrease in BP and CO associated with isoflurane can be attributed to vasodilation,16,23 direct myocardial depression and decreased sympathetic activity, 24 which collectively reduce systemic vascular resistance.14,25 These hemodynamic changes have also been reported in horses, 14 goats and dogs,25,26 and are known to be dose dependent.16,20
To our knowledge, no previous studies have investigated the impact of anesthesia on cardiac function assessments conducted with Doppler echocardiography. In this study, isoflurane had no effects on the echocardiographic variables assessed in anesthetized sheep, with preserved LV systolic function and no changes in EF% or FS%. Earlier studies have shown that volatile anesthetics induce dose-dependent changes in cardiac function assessments by echocardiography, causing primarily significant cardiac depression with inspired fractions exceeding the MAC recommended for each species.27,28 In species such as mice, 27 rats and goats,28,29 anesthesia with isoflurane did not reduce LV systolic function, and a decrease in EF% and FS% was observed only at MAC levels twice those recommended. 28 There was also a slight increase in parameters related to LV systolic function, 29 and no changes in parameters related to diastolic function,26,29 at doses up to 1 MAC. Unlike what was observed in this study, in dogs, isoflurane had a great impact on cardiac function assessed by echocardiography, 16 with a noticeable decrease in EF% and FS%, demonstrating a negative inotropic effect. This depressive effect can be attributed to the inhibition of sodium and calcium influx and efflux in cardiac myocytes, mediated by inhalational agents. 30
During CO assessment, neither the Doppler nor the Teichholz methods was sensitive to detect significant reductions when compared with the gold standard, exhibiting low correlation coefficients and poor agreement between the methods. Nonetheless, the variations in values followed similar trends in the assessment of the CO curve, with close to 45% similar percentage variations observed between values during anesthesia and in anesthetic recovery. This highlights the clinical importance of Doppler echocardiography as a noninvasive tool for monitoring changes in values and guiding therapeutic decisions in clinical scenarios.
High correlation values have been observed in previous studies when comparing Doppler techniques in the pulmonary artery and aorta in dogs,31,32 yet these studies did not demonstrate high levels of agreement in Bland–Altman evaluations. 31 In both hypo- and hyperdynamic states in dogs and humans,33,34 low correlation and agreement have been observed between thermodilution and Doppler methods, and medium correlation between thermodilution and volumetric methods, without showing agreement between the methods. 33 Previous research in humans has demonstrated that, whereas techniques are not interchangeable, Doppler echocardiography evaluations are valuable and can be used to observe the behavior and trends of changes in CO in response to therapeutic interventions or variable clinical situations, both by Doppler and by M-mode echocardiography.35,36
Some factors, such as the alignment of the ultrasound beam with the direction of blood flow and accurate measurement of the vessel diameter, should be considered when assessing CO via Doppler echocardiography. Errors in these measurements can be amplified because CO calculation involves squaring the diameter. In this study, transverse linear measurements of the pulmonary artery annulus were taken from sections described previously for the species.9,12,37,38 In a recently published study with standardized echocardiography in sheep, measurements of pulmonary artery flow and diameter through the right parasternal window were possible in the quadrupedal position even in awake animals. 40
Given the variations in beam angle, volumetric methods are generally more accurate than Doppler methods in humans 34 ; however, most clinical and animal studies rely on Doppler due to the impossibility of performing volumetric methods, such as the Simpson method, in sheep due to the difficulty in obtaining views in the left parasternal window in which it is possible to observe images of a true cardiac apex. This limitation stems from anatomical challenges in identifying the cardiac apex during examination and difficulties in delineating the LV endocardial borders in ruminants. Moreover, in cases of experimentally induced myocardial infarction in animals, volumetric methods prove less effective due to myocardial akinesia, 39 causing discrepancies in CO measurements compared with other techniques. Therefore, in studies on models of changes in myocardial vascularization, the use of Doppler is recommended. Limitations of the include the absence of central venous pressure (CVP) assessment, which impeded a hemodynamic study of systemic vascular resistance values derived from CVP calculations. Additionally, there was no variation in the animals’ positioning (decubitus) to compare the Doppler echocardiographic examination with CO values obtained using volumetric methods.
We consider sample size to be a limitation of the study. Although the sample number was calculated previously, SDs above 25%, previously adopted for the sample calculation, were found in some variables, especially in the trans- and post-anesthetic periods in all evaluation methods. Therefore, it is recommended that the results of agreement between the methods be interpreted with caution depending on the sample number.
Sexual immaturity was another limitation of the study. Ecocardiographic parameters adopted to CO calculation in our study were within the range observed in a recently published studies with Dorper lamb with the same age range.40,41 There was no significant difference in echocardiographic parameters after 90 days of life, 41 although age and growth are listed as important factors of variation. In some species, cardiovascular parameters and cardiac dimensions increase as an animal grows, particularly as it approaches sexual maturity. 42 This represents a limitation when extrapolating the findings to mature individuals, highlighting the need for complementary studies adopting comparisons throughout the development of the animals and at different reproductive stages.
Additionally, our study was performed with standing position comparisons of examination, and different positions were not explored. We recognize that this positioning, even with careful trunk adaptation, may influence cardiopulmonary mechanics. The potential for the restraining trunk to limit thoracic excursion and interfere with mechanical ventilation and venous return cannot be excluded entirely. Although transthoracic echocardiography in the standing position is a preferred method over lateral recumbency in ruminants, minimizing the risk of tympanism, and a previous study demonstrated the feasibility of conducting echocardiographic assessment with minimal physical restraint, 40 additional comparisons of examination outcomes in different positions, such as lateral recumbency with anesthesia, are necessary.
Conclusions
Isoflurane anesthesia led to a decrease in blood pressure and CO, but it did not affect the echocardiographic parameters evaluated in two-dimensional, M-mode and Doppler modes in Dorper sheep. CO values obtained by thermodilution were not interchangeable with those from the Doppler and Teichholz methods. The main finding from this study was that the morphological and functional echocardiographic parameters in sheep remained unchanged under isoflurane anesthesia.
Footnotes
Acknowledgements
The authors would like to thank the Veterinary Hospital of Escola de Veterinária e Zootecnia of Universidade Federal de Goiás for facilitating the project implementation. We would like to thank Mr. Ademir Souza on behalf of the Association of Dorper and White Dorper Sheep Breeders of Goias.
Author’s contributions
Conceptualization, methodology and writing—review and editing: RSM and LGF. Formal analysis and methodology: ROAC. Visualization and writing—original draft: SMB and RSM. Methodology: BKR, DPF, JRG. Project administration, supervision and writing—review and editing: LGF.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
ORCID iDs
Data availability statement
The raw data supporting the conclusions of this article will be made available by the corresponding author email on request.