
Abstract
The effects of coronavirus disease 2019 (COVID-19) have been felt globally and in all spheres of life. Developing vaccines was an important milestone in ensuring the protection of lives, but there are concerns about vaccine availability in sub-Saharan African (SSA) countries. The living conditions of persons with disabilities, in particular, in SSA societies have been described as deplorable and unsustainable, and they are at risk of discrimination. Such persons appear to be already struggling to obtain other basic services, and the extent of vaccine accessibility to this population remains unknown. This study aimed to assess the perceptions of persons with disabilities in Ghana of COVID-19 vaccines. Between July 2021 and December 2021, 336 persons with disabilities (hearing, visual, and physical) were recruited from two regions in Ghana. The attitude toward the COVID-19 vaccination scale was adapted for this study. The results showed that persons with disabilities were ambivalent toward vaccination, and differences were observed between participant groups. The background variables found to influence attitude were age, place of residence, educational qualification, gender, and COVID-19 acquisition status. The study concludes with a clarion call to policymakers to expedite public education for persons with disabilities.
Introduction
Disability is defined as the onset of impairments in persons’ physical and sensory interaction in day-to-day living experiences (WHO 2011). The coronavirus disease 2019 (COVID-19) pandemic raised fundamental questions about the health, social, and psychological needs of and services required by persons with disabilities (Armitage and Nellums 2020; Boyle et al. 2020; Cho and Kim 2021; Clegg 2020; Ebuenyi et al. 2020; Senjam 2020). Indeed, it has been suggested that policymakers should reconsider the health and support services provided to persons with disabilities (Turk and McDermott 2020) due to their susceptibility to COVID-19 and its long-term effects. Nevertheless, some studies have reported that persons with disabilities continued to encounter barriers (Rose et al. 2022) in their effort to access health services during the pandemic (El-Zraigat and Alshammari 2020; Lunsky et al. 2021; Rotas and Cahapay 2021). Socially, the pandemic exacerbated the vulnerability of persons with disabilities because enormous social and communication restrictions were imposed (Dalise et al. 2021; El-Zraigat and Alshammari 2020; Embregts et al. 2022). Persons with disabilities harbored significant fear about the pandemic (Summaka et al. 2021), but their perception and uptake of the COVID-19 vaccine remain unclear.
Public concerns about the potential side effects of COVID-19 vaccines have increased in multiple locations around the globe and may have influenced perceptions of vaccines and their administration (Aberese-Ako et al. 2023; Al-Mohaithef and Padhi 2020; Echoru et al. 2021; García and Cerda 2020; Islam et al. 2021; Lazarus et al. 2021; Lin et al. 2020; Rahman et al. 2021; Seale et al. 2021). For instance, Lin et al. (2020) conducted a nationwide survey in China to understand public demand for the COVID-19 vaccine and hesitation about uptake. The authors listed some concerns expressed about vaccines, such as perceived susceptibility and severity of side effects; however, they reported that most participants were very afraid of COVID-19 complications and perceived that the vaccine might reduce the risk of infection (Lin et al. 2020). Rahman et al. (2021) investigated adults’ perceptions of the new COVID-19 vaccine in Bangladesh and examined participants’ hesitation to receive it. The study showed that approximately 30% of participants were hesitant to take the second vaccine after having the first dose. The age group and income level of participants were found to be significant predictors of their hesitation toward having the vaccine; a majority (∼87%) had a fear of vaccine side effects, and many (∼74%) did not have adequate knowledge of and information about the vaccine and its impact.
Despite the initial concerns and confusion, people appear to be gravitating toward taking the vaccine (Islam et al. 2021; Kishore et al. 2021). In Bangladesh, Islam et al. (2021) reported that approximately 60% of study participants were vaccinated and two thirds would recommend vaccination to their friends, relatives, and families. The study also revealed that socioeconomic status, educational level, family type (nuclear), and prior vaccinations were significant predictors of knowledge of and attitudes toward coronavirus vaccines. However, only 50% of participants believed that every person should get the COVID-19 vaccine, and a large majority (90%) believed that the vaccine might have side effects. Similarly, Kishore et al. (2021) found that approximately 70% of respondents wanted to have the COVID-19 vaccine, and approximately 30% were not positive about being vaccinated in a study conducted in India. A significant number of participants (∼51%) believed that the vaccine was ineffective in protecting them from infection.
A study in the United States reported that 52% of Americans were very likely to get the COVID-19 vaccine, whereas 22% were very unlikely to do so (Khubchandani et al. 2021). Vaccine hesitation was higher among African Americans (34%) than Hispanics (29%), and sex, income level, employment status, political affiliation, and educational status were found to be significant predictors of vaccine hesitation (Khubchandani et al. 2021).
Although the perception of the general population toward the vaccine has been studied (Adane, Ademas, and Kloos 2022; Sallam, Al-Sanafi, and Sallam 2022; Wouters et al. 2021), there is little information on the uptake and attitude of persons with disabilities. Furthermore, although there are concerns regarding inequitable access to vaccine in low-income contexts (Pilkington, Keestra, and Hill 2022; WHO 2022a; Ye et al. 2022), efforts to encourage uptake of the COVID-19 vaccine among vulnerable groups such as persons with disabilities are yet to be mainstreamed in public health discourse.
Contextualization
The 2021 Population and Housing Census Ghana Statistical Service (2021) reported that approximately 8% of the current estimated 30 million people in Ghana are living with a form of disability. There is a traditional understanding of disability (Aldersey 2012; Aldersey et al. 2018; Baffoe 2013) as the onset of disability is attributed to spirituality, the orchestration of supernatural forces (Baffoe 2013), and, specifically, sins or bad deeds committed by a family member (Avoke 2001, 2002). In this perspective, a myth or superstition is associated with a disability, making it difficult for people to associate with persons with disabilities (Baffoe 2013). In families, the birth of a child with a disability is considered a calamity and a taboo (Avoke 2001, 2002). In the past, such children used to be killed, and some rituals were carried out to pacify the gods (Baffoe 2013). However, as educational levels rise, society is opening up and gradually embracing persons with disabilities as members of society.
In the Ghanaian context, an intricate relationship has been observed between disability, poverty (WHO 2011), discrimination (Baffoe 2013; Mbamba and Ndemole 2021; Opoku et al. 2019, Opoku et al. 2022a; Oti-Boadi, Asante, and Malm 2020a; Oti-Boadi 2017), and limited access to basic services, such as education (Opoku et al. 2022a; Singal et al. 2015), healthcare (Mprah et al. 2022; WHO 2011), and employment (Kassah, Kassah and, Agbota 2012, 2014; Odame et al. 2021; Opoku et al. 2019). Persons with disabilities face limited access to healthcare because of factors such as negative attitudes of health, lack of health facilities, physical barriers, and lack of income (Mbamba and Ndemole 2021; Oti-Boadi, Dankyi, and Kwakye-Nuako 2020b). It has been reported that essential services are inaccessible to those with visual impairments (Opoku et al. 2022b), hearing impairments (Opoku et al. 2022a), and physical (Naami, Hayashi, and Liese 2012) and cognitive disabilities (Oti-Boadi, Asante, and Malm 2020a; Oti-Boadi 2017). This disadvantaged position of persons with disabilities requires a more affirmative approach so their needs will be considered in developmental policies and programs.
Ghana has committed itself to improve the lives of persons with disabilities, as seen by the Persons with Disability Act 715 (Republic of Ghana 2007) and ratification of the UN Convention on the Rights of Persons with Disabilities (United Nations 2007). Despite this evidence that some steps have been taken to advance the lives of persons with disabilities, discussions of this population's welfare during the COVID-19 outbreak and in regard to vaccination were very limited. COVID-19 remains a problem, and there is the possibility that another pandemic will occur in the future. Thus, ongoing discussion is required of the extent to which vaccines are accessible, especially to minority groups such as persons with disabilities, in specific contexts. It is against this background that this study attempts to extend the deliberation to persons with disabilities in Ghana to understand their perception of COVID-19 vaccines. This study was guided by the following questions:
What is the association between background variables and attitudes toward COVID-19 vaccination? Does disability type mediate the relationship between other variables and attitudes toward COVID-19 vaccination? Which variables predict the attitudes of youths with a disability toward COVID-19 vaccination?
Materials and Methods
Participants
The study participants were persons with disabilities recruited from 2 of the 16 regions of Ghana. Persons with hearing, visual, and physical disabilities were recruited because most of them could read, comprehend, and respond to the questions. The regions were selected because of the author's familiarity and close working relationship with the disability communities there. Disability associations were contacted and asked to extend an invitation to their members to participate in this study. The inclusion criteria were as follows: (a) diagnosed with a disability (hearing, visual, or physical), (b) aged >18 years, (c) living in the study areas, and (d) capable of consenting to participate in this study.
Instrument
A two-part survey was used for data collection. The first section collected information on the following personal profiles or demographic characteristics of the participants: disability type, gender, age, educational background, employment status, place of residence, COVID-19 acquisition, and vaccine taken.
The second section used the Attitude Toward the COVID-19 Vaccination Scale, which consists of 31 items (Mustafa et al. 2022) drawn from the literature (Tahir et al. 2021; Al-kafarna et al. 2022). While four of the items are positively worded, the remaining 27 are negatively worded and thus reverse-coded during analysis. The items are anchored on a five-point Likert scale with responses ranging from 1 (strongly disagree) to 5 (strongly agree). A mean score of at least 3 is interpreted as a negative attitude toward vaccination.
The draft instrument was given to four experts with research experience in disability and public health for review. Thereafter, the instrument was piloted before being used for this study. The comments made by experts and participants in the pilot study were incorporated in the final version of the instrument used for data collection.
Procedure
This study was part of a larger project aiming to understand global perspectives on COVID-19 vaccination. The study and its protocols were approved by the institutional ethics review committee at the United Arab Emirates University (approval number ERS_2021_7322). Contacts were then made with special schools, integrated units, and disability associations (Ghana Blind Union, Ghana National Association of Deaf, and Ghana Physical Disability Association) to recruit persons with disabilities for this study. As author four focused on data collection in schools, authors three and six worked with the recruitment of persons with disabilities for this study.
Four schools, two for the hearing impaired and two inclusive units, agreed to participate in this study. Author four, who is proficient in using sign languages, visited the schools to explain the study purposes and rules governing participation. To assess blind participants, a Braille version of the questionnaire was administered. Moreover, authors three and six attended meetings of the disability group and explained the study to prospective participants. Those who wished to participate in this study provided oral or written informed consent. The participants were informed that there was no incentive to participate and that they had every right to withdraw from the study at any time without consequences. Participants spent 30 minutes to 1 hour completing the questionnaire, and data were collected from July 2021 to December 2021.
Data Analysis
The data collected were entered into Microsoft Excel for cleaning before being transferred to SPSS for further analysis. Due to the sample size, we presumed that the data were normally distributed (Field 2013). However, since the instrument was used in an African context, its factor structure and validity were assessed before it was used for this study. Therefore, the 31 items were subjected to factor analysis (Table 1). The initial inspection of the correlation among items showed the presence of a coefficient of at least 0.3. The Kaiser–Meyer–Olkin measure was 0.59, which is within the acceptable threshold. Bartlett's test of sphericity was significant (p = .001), which confirms the factorability.
Summary of exploratory factor analysis.

Note: COVID-19, coronavirus disease 2019.
The exploratory factor analysis identified 19 components with eigenvalues of at least 1%. However, the scree plot showed two clear breaks; thus, the two-factor model was retained. Based on this information, another model was run, and two components explained 30% of the variance. As 11 items had a loading of <0.3, 20 items had a value of >0.3. Factor I comprised 11 items referred to as an opinion toward vaccination (OVC), and Factor II comprised nine items referred to as the perceived hesitancy scale (PHS). The correlation matrix between the two measures was 0.14, confirming the scale appropriateness.
At this stage, the reliability of the scale was computed using Cronbach's alpha, which yielded the following results: OVC (0.65) and PHC (0.73). The results were at an acceptable level and thus confirmed the reliability of the scale in this study.
We computed the mean scores for the total scale and subscale. We then proceeded to answer the research questions at this stage. To answer research question 1, a t-test and analysis of variance (ANOVA) were computed to understand the difference between participants based on background variables. t-Tests (e.g., age and gender) were computed for demographic variables with two variables, whereas ANOVAs were computed for demographic variables with at least three levels (e.g., disability type). In both computations, it was ensured that homogeneity variances were not violated.
To answer research question 2, two-way factorial ANOVAs (Pallant 2016) were computed to understand whether disability type is moderately related to other demographics and perceptions toward vaccination. We then assessed to outcome to ensure that the homogeneity of variance was not violated.
To answer research question 3, a linear regression analysis was performed to enable us to understand the predictors of opinions and hesitation toward vaccination. Here, the following assumptions were assessed to ensure that they were not violated: homogeneity of variance, homoscedasticity, and multicollinearity (Pallant 2016).
Results
A total of 336 persons with disabilities participated in this study, of whom 13% had a physical disability, 24% a visual impairment, and 63% a hearing impairment. Regarding gender, 54% were females and 46% were males. Furthermore, 80% were between 18 and 25 years old, while 20% were under 26 years old (Table 2).
Association between demographics and attitudes.
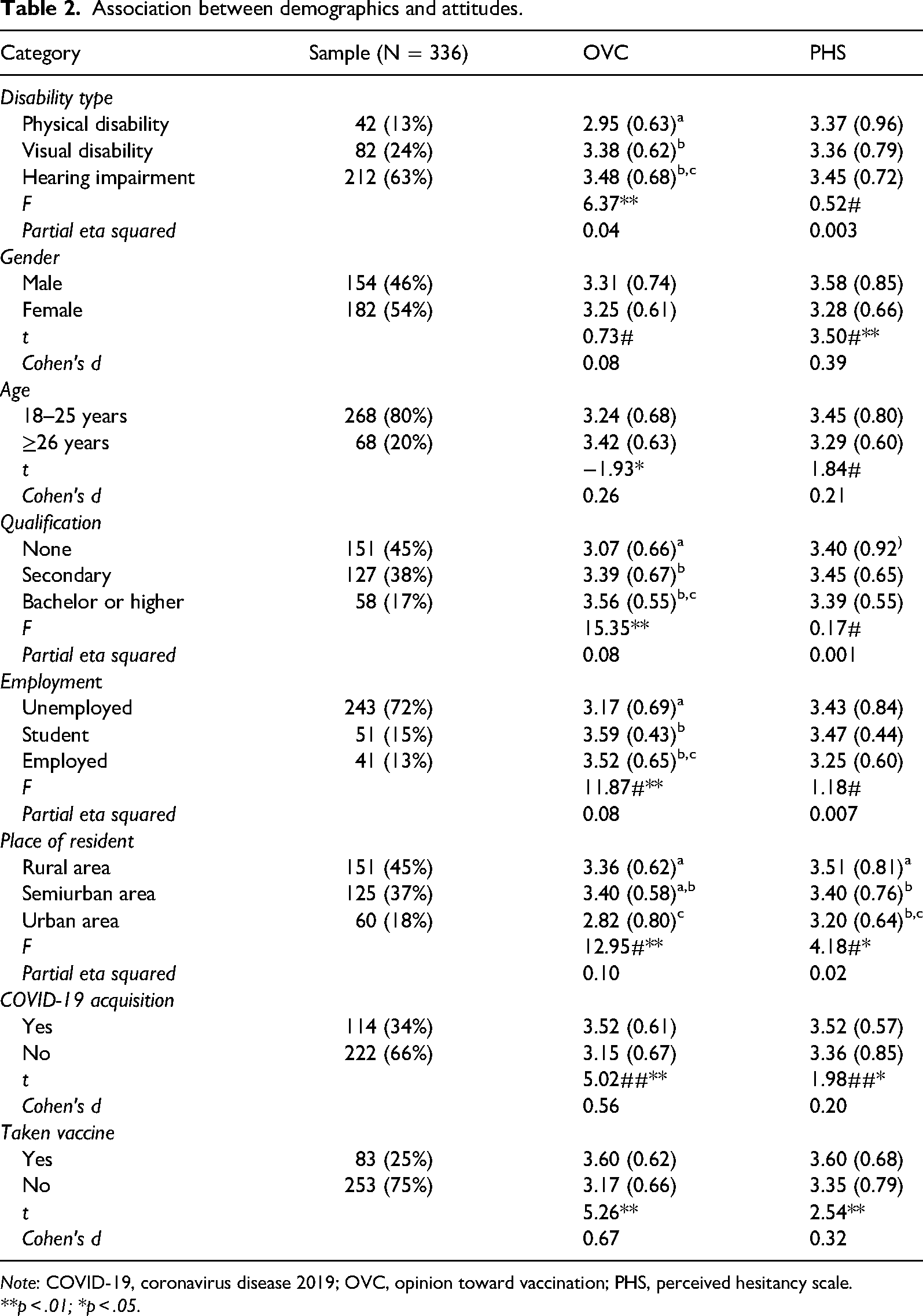
Note: COVID-19, coronavirus disease 2019; OVC, opinion toward vaccination; PHS, perceived hesitancy scale.
**p < .01; *p < .05.
The computation of the measured means yielded the following results: OVC (M = 3.28; SD = 0.67) and PHS (M = 3.42; SD = 0.77). The results showed that participants were ambivalent toward being vaccinated.
Association Between Demographics and Measures
The association between participants and measures was calculated using t-tests and ANOVAs (Table 2). For instance, t-tests were computed for demographics with two levels, namely gender and age, as well as COVID-19 diagnosis and whether participants had been vaccinated. Regarding gender, a difference was found between participants in the perceived hesitation toward vaccination, with males being more hesitant than females [t(334) = 3.50, p = .001, and a small effect size, Cohen's d = 0.39].
Moreover, regarding age, a significant difference was found between participants’ opinions about vaccination. Specifically, older participants expressed more negative OVC than younger ones. In addition, those who contracted COVID-19 and those who had taken the vaccine had more negative OVC than their counterparts who had not contracted COVID-19 or been vaccinated.
The ANOVAs demonstrated differences between participants in disability type, qualification, employment status, and place of residence. Regarding disability type, those with a hearing impairment had more negative OVC and were more hesitant toward the vaccination than those with other types of disabilities. However, regarding perceived PHS, the post hoc comparison showed no difference between participants. Regarding OVC, those with a hearing impairment were different from those with a physical disability.
Regarding educational background, those who held bachelor's degrees had more negative OVC than others. Post hoc comparison showed that participants who held bachelor's degrees had different opinions than those who did not.
On employment, a difference was observed between study participants. Students and employed participants had more negative OVC than the unemployed. Specifically, students had different opinions than the unemployed.
Regarding place of residence, participants living in rural areas had a more negative OVC and were more hesitant to take the vaccine than other in non-rural areas. Moreover, post hoc comparison showed that the difference was more significant in those living in urban areas than in those living in semiurban and rural areas. Regarding their hesitation toward vaccination, the difference was more significant in those living in rural areas than in those living in urban and semiurban areas.
Moderation Effects
A two-way between-group ANOVA was computed to assess the impact of disability status and other demographics on attitudes toward vaccination. Other demographics were used as independent variables, whereas disability status was used as a moderator variable with effects assessed based on participants’ OVC (Table 3).
Summary of moderation between disability and demographics on opinion toward vaccination.

Note: COVID-19, coronavirus disease 2019.
**p < .01; *p < .05.
First, the effects of disability type and educational status were significant (F [3, 335] = 3.56, p = .02 with small effect size, partial eta squared = 0.03). The mean scores showed that persons with disabilities with higher educational attainment had more negative OVC than those with lower educational attainment.
Second, disability type was moderately associated with employment status and OVC (F [4, 335] = 4.22, p = .002 with very small effect size, partial eta squared = 0.05). The mean scores showed that persons with disabilities who were either students or employed had more negative OVC than those who were unemployed.
Third, the disability type was moderately significantly associated with place of residence and OVC. The mean scores showed that persons with disabilities living in rural and semiurban areas held more unfavorable OVC than those living in urban areas.
Fourth, the disability type was moderately significantly associated with the acquisition of COVID-19 and OVC (F [2, 335] = 4.81, p = .01, partial eta squared = 0.03). Specifically, those who were vaccinated had more negative OVC than those who were not.
Moreover, the demographics were used as independent variables and the disability type as moderators on perceived hesitation toward the vaccine (Table 4). First, the disability type was moderately related between age and perceived hesitancy toward vaccination (F [2, 335] = 4.40, p = .01, partial eta squared = 0.03). The mean score showed that those who were younger were more hesitant toward the vaccine than those who were older.
Summary of moderation between disability and demographics on perceived hesitancy scale.
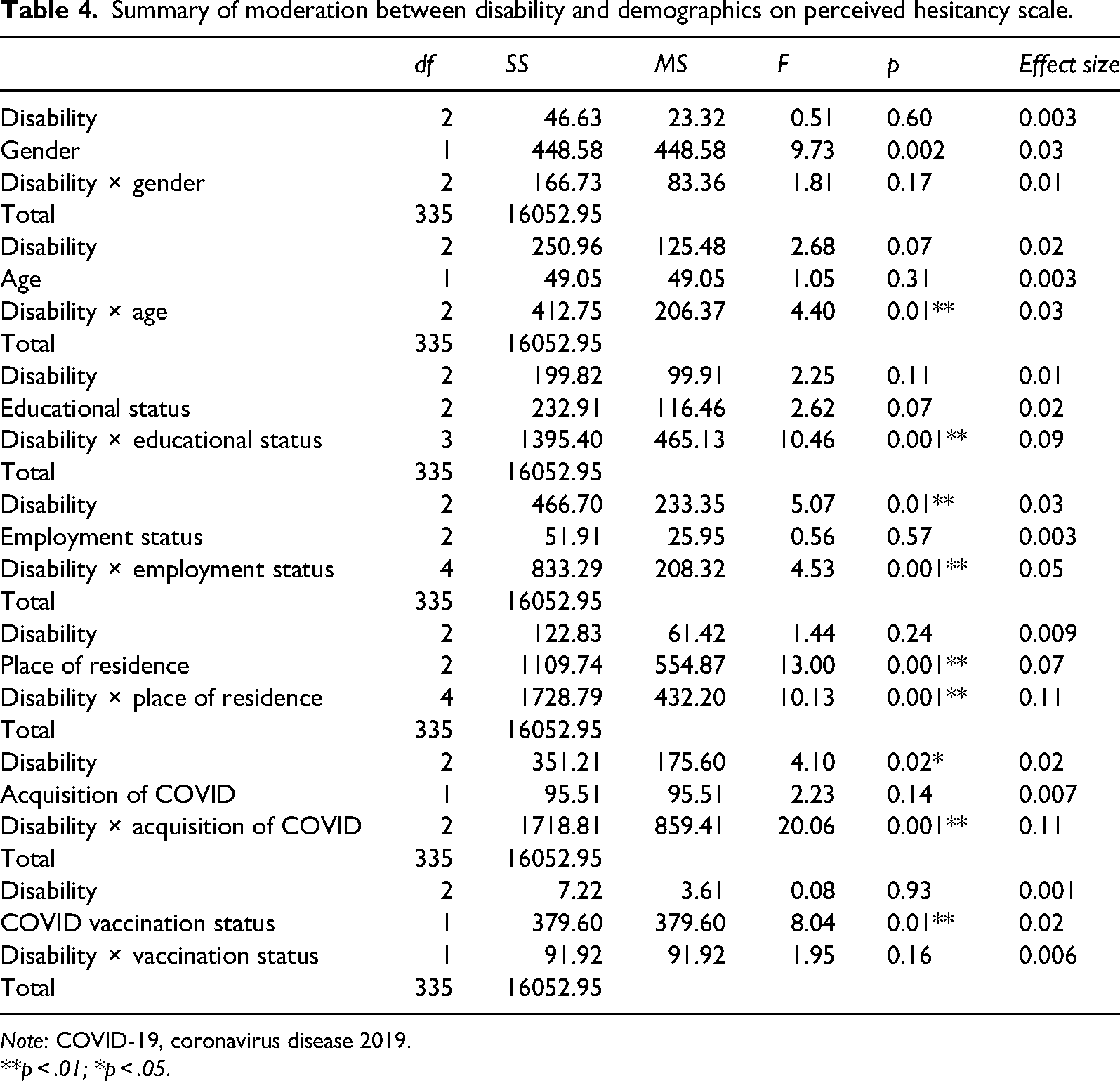
Note: COVID-19, coronavirus disease 2019.
**p < .01; *p < .05.
Second, disability type had an interaction effect on the relationship between educational attainment and hesitation toward vaccination. The mean scores showed that those who had secondary levels of education were more hesitant toward vaccination than those who held other levels.
Third, disability type had an interaction effect on the relationship between employment status and hesitation toward vaccination. The mean scores showed that the difference between unemployed and employed participants was significant.
Fourth, disability type was moderately related to place of residence and hesitation toward vaccination (F [4, 335] = 10.13, p = .001, partial eta squared = 0.11). The mean scores showed that those living in rural and semirural areas were more hesitant toward vaccination than those living in urban areas.
Fifth, disability type had an interaction effect between COVID-19 acquisition and hesitation toward vaccination. Participants who had acquired COVID-19 were more hesitant toward vaccination than those who stated otherwise.
Predictors of Attitudes Toward Vaccination
A two-model linear regression analysis was performed to understand the predictors of attitude toward vaccination. In the first model, demographic variables were regressed on OVC (Table 5). The model contributed to 24% of opinion differences toward vaccination (F [8, 335] = 13.00, p = .001). However, individually three demographic variables significantly contributed to opinion differences toward vaccination: educational qualification (beta = 0.24, p = .002), place of residence (beta = -0.26, p = .001), and vaccination status (beta = -0.23, p = .001). It was evident that place of residence made more contribution to the variance in OVC.
Demographics regressed on opinion toward vaccination.
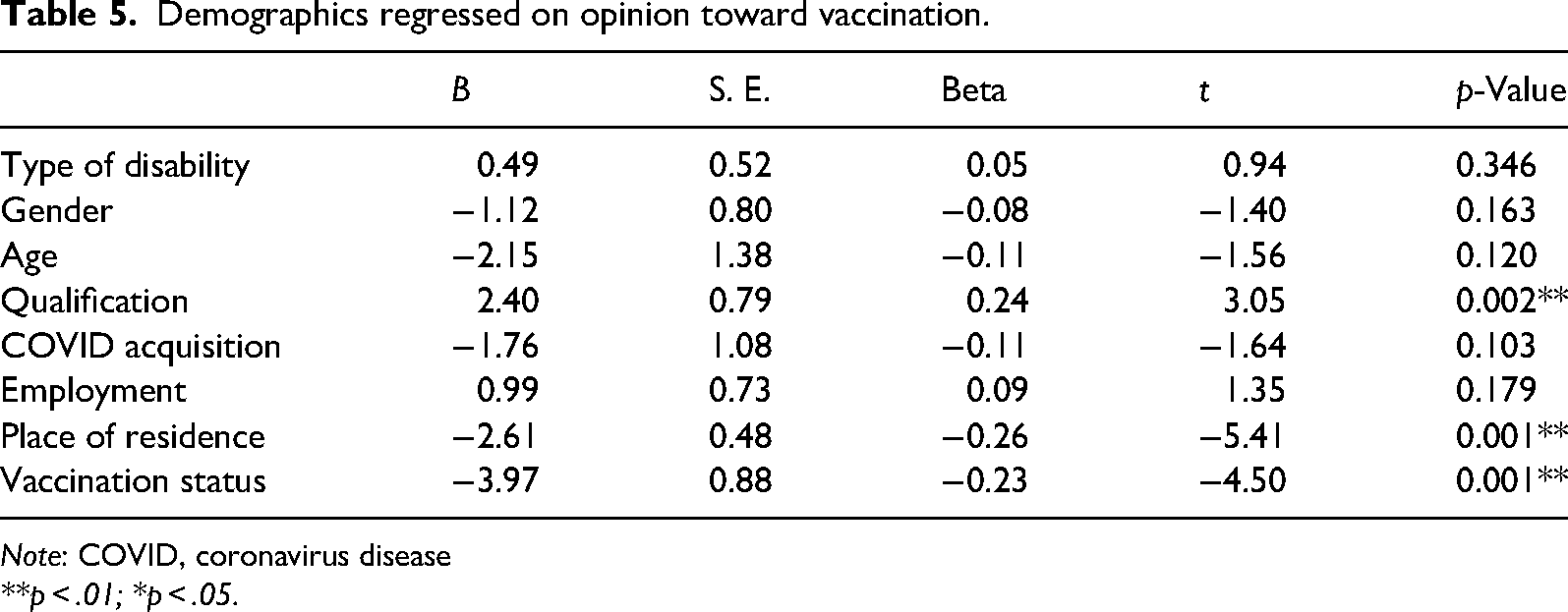
Note: COVID, coronavirus disease
**p < .01; *p < .05.
In the second model, demographic variables were regressed on the PHS. The result showed that demographics made a 10% contribution to hesitancy differences (F [8, 335] = 4.76, p = .001). Individually, four demographics significantly contributed to hesitancy differences (gender, employment status, place of residence, and vaccination status). Both gender and COVID vaccination status made significant contributed to the variance in perceived hesitancy (Table 6).
Demographic variables regressed on perceived hesitancy scale.

Note: COVID-19, coronavirus disease 2019.
**p < .01; *p < .05.
Discussion
This study aimed to assess the perception of persons with disabilities toward taking the COVID-19 vaccine. It was conducted in an environment where persons with disabilities face formidable barriers to accessing healthcare (Mprah 2013a, 2013b). This type of study is needed worldwide during the COVID-19 pandemic. Persons with disabilities have serious concerns about the effects of COVID-19 on their livelihoods (Summaka et al. 2021), and their perceptions of vaccination are an unexplored area.
In this study, the findings revealed the ambivalence of persons with disabilities toward vaccination, probably indicating that those who participated in this study were neither positive nor negative toward receiving the vaccination. This finding is different from studies conducted in Ghana which reported that persons without disabilities had positive attitudes toward COVID-19 vaccination (Kishore et al. 2021; Kyei-Arthur et al. 2022; Okai and Abekah-Nkrumah 2022). This finding was different from studies conducted elsewhere which reported a high likelihood that the general population would have a COVID-19 vaccination (Al-Kafarna et al. 2022; Al-Mohaithef and Padhi 2020; Edwards et al. 2021; Kalam et al. 2021; Khubchandani et al. 2021; Schwarzinger et al. 2021; Yasmin et al. 2021) or hesitancy (Ahmed Khidir 2021; Cooper, van Rooyen, and Wiysonge 2021) towards the vaccination. Persons with disabilities who participated in this study may be at high risk of contracting COVID-19 or increased risk of developing complications (Mustafa et al. 2022; Bakouny et al. 2020; Ehmsen et al. 2021; Summaka et al. 2021). As most persons with disabilities have health issues, deliberate steps should be taken to encourage them to be vaccinated. In the Ghanaian context, reasons explaining the neutrality of persons with disabilities concerning their perception of the vaccine are twofold. First, persons with disabilities are generally excluded from national development and planning (Opoku et al. 2019), which could suggest that they have not been targeted in the drive to encourage citizens to be vaccinated. Second, developing countries have struggled to access the vaccine for their citizens (WHO 2022a) and thus, making difficult for them to prioritize access to persons with disabilities. In Ghana, as at April 2024, a little under 12 million out of the estimated 33 million has received at least one dose of COVID vaccine (WHO 2023). However, persons with disabilities are least prioritized in national development (Lamptey et al. 2015), indicating that little effort has been made to extend or enhance their access to vaccines. To protect the lives of persons with disabilities, their needs should be considered in the national vaccination program.
A difference was observed between disability groups who participated in this study. Although general ambivalence was observed among persons with disabilities, those with a hearing impairment were associated with greater hesitation toward vaccination. It is useful to mention here that the influence of characteristics such as race or ethnicity on access to COVID-19 vaccine among the general population (Cooper, van Rooyen, and Wiysonge 2021; Edwards et al. 2021; Khubchandani et al. 2021; Yasmin et al. 2021). This finding is probably due to the fact that persons with a hearing impairment encounter significant problems accessing information and communicating with other members of society (WHO 2011). In particular, they are unable to listen to information disseminated on media platforms, such as the radio and television, and sign language is not a recognized language. In view of this, they might not understand what is happening around and as such, increasing their hesitancy towards the vaccine. Compounding this situation is the fact that most persons with a hearing impairment are unable to read and comprehend, denying them the ability to acquire new information (Mprah 2013a, 2013b). The call to promote equitable access to services includes the need for government to provide accessible information (WHO 2011). Unfortunately, the government seems not to have sufficiently provided accessible information to persons with disabilities, such as the hearing impaired, about vaccines, their effects, and access avenues. It is vital for the government to invest resources in the provision of educational programs in a format which is accessible to persons with disabilities.
A relationship was observed between place of residence and perception of vaccination. Both ANOVAs and linear regression analysis showed that participants living in rural areas seemed to have negative opinions and were more hesitant toward accessing the vaccine. This finding is somehow similar to previous studies which reported place of residence or geographical location of the general populace as a predictor of attitude towards COVID-19 vaccination (Ahmad Khidir 2021; Cooper, van Rooyen, and Wiysonge 2021; Khubchandani et al. 2021; Yasmin et al. 2021). This finding may not be surprising because rural communities frequently struggle to access essential services, such as education, healthcare, and transportation. (WHO 2011). Therefore, it is likely that participants living in such communities cannot access the vaccine. As advocacy for universal access to healthcare currently exists (United Nations General Assembly 2019), the situation of rural communities underscores the need for the government to ensure that, regardless of where citizens live, they receive relevant education and are vaccinated. Some lapses were observed in this regard; thus, the government should implement more personal educational programs and make vaccines available to all.
Another surprising finding in this study was the association between educational attainment and attitude toward vaccination. For instance, ANOVAs showed that those who were educated had negative OVC, while employment status showed that students had a more negative OVC than others. This finding is different from previous studies which reported a more positive attitude among those who are educated about COVID-19 vaccination than those with limited or no access to education (Cooper, van Rooyen, and Wiysonge 2021; Echoru et al. 2021; Islam et al. 2021; Khubchandani et al. 2021; Yasmin et al. 2021). Although this finding further showed that those with lower educational attainment were more hesitant to access vaccines, it remains to be elucidated why students and educated participants seem to have a negative opinion. This finding appears to be different from other studies that reported the positive influence of education on perception toward vaccination (Aberese-Ako et al. 2023). Indeed, the expectation was that educated persons may have access to information about the vaccine and be favorably disposed toward the vaccine. In the Ghanaian context, this could be related to the poor socialization of students with disabilities with the larger population (Avoke 2001, 2002). Special education remains the most viable form of education for a person with disabilities. In this study, most students received education in a special school setting where they had limited interaction with the general population (Avoke 2002), a situation which affects their access to information and essential services. Limited efforts have been made to ensure that they have access to services such as a vaccine that boosts their resistance to COVID-19. The government should take steps to ensure that all segments of society are targeted in regard to pressing issues, such as enhancing access to vaccination.
Another concerning finding was the negative association between the acquisition of COVID-19, vaccination status, and perception of vaccination. First, t-test findings showed that participants who had either acquired COVID-19 or received the vaccine had negative perceptions. Second, regressions showed that as participants are vaccinated, their opinions and hesitations increase. Similarly, as they acquire COVID-19, they become more negative toward the vaccine. The finding reported does not agree with previous studies which reported that members of the general population who have received vaccination are more favorably disposed to boosters (Al-kafarna et al. 2022; Islam et al. 2021). The previous literature has reported negative experiences of persons who contracted COVID-19 (Giannakoulis, Papoutsi, and Siempos 2020; Kow and Hasan 2020). Moreover, studies have reported that other persons experienced the negative effects of the vaccine. However, such conclusions cannot be confirmed until future studies have developed in-depth insights into the experiences of persons with disabilities who received the vaccine.
This study also found that the two genders have different perceptions of and attitudes toward the vaccination. Specifically, both t-test and regression analyses showed that female participants were more significantly associated with hesitation toward vaccination. While some studies show high hesitancy among females (Echoru et al. 2021; Edwards et al. 2021; Khubchandani et al. 2021; Yasmin et al. 2021), other studies have reported either the contrary (Al-kafarna et al. 2022; Islam et al. 2021) or found that gender has no impact on opinion among members of the general populace (Ahmad Khidir 2021; Al-Mohaithef and Padhi 2020). This finding is concerning in the sense that anecdotal evidence in most developing countries suggests that females are less likely to access essential services. However, being a female with disabilities presents an additional barrier to accessing services in society (Naami, Hayashi, and Liese 2012). First, females with a disability have to navigate through the disability barrier; then, they confront the gender stereotype. Thus, females may have difficulty obtaining the requisite information and accessing the vaccine, and policymakers should consider differences between persons with disabilities, including gender, when tailoring training, intervention, and vaccination programs.
Study Limitations and Strengths
The study findings should be considered in light of some limitations. First, the study was limited to persons with physical, hearing, and visual impairments. Therefore, the findings may not be applicable to persons with cognitive intellectual disabilities. However, attempts were made to ensure that participants were capable of making decisions and participating in this study. More especially, recruitment through the disability associations and special schools helped to reduce sampling bias as various groups had a fair chance to participate in this study. Second, study participants were recruited from 2 of 16 regions in Ghana; thus, it may be impossible to generalize the study findings. However, as the situation of persons with disabilities in Ghana seemed similar, for example with regard to educational barriers, access to health services, and other basic services (Kassah, Kassah, and Agbota 2012; Mamba and Ndemole 2021; Singal et al. 2015), the findings reported in this study may reflect patterns experienced by groups outside the study areas. A major strength of this study is the heterogeneity of study participants, disability groups, different qualifications, and different geographical areas.
Conclusion and Study Implications
This study was conducted due to a lack of information regarding access to the COVID-19 vaccine by persons with disabilities. The ambivalence of the study participants and findings suggest that gender, age, COVID-19 acquisition, and vaccination status seem to cause differences in their perceived hesitations toward and opinions of vaccination. Persons with different disability statuses, such as hearing, visual, and physical disabilities, had significantly different opinions of and attitudes toward vaccination. Persons with higher educational attainment and those who were students or employed seemed to have more negative OVC than those with lower educational attainment and who were unemployed. Likewise, persons with disabilities living in rural and semiurban areas had more unfavorable OVC than those living in urban areas. Furthermore, younger persons with disabilities were more hesitant toward vaccination than older ones.
The Ghana Government's effort to encourage the uptake of the vaccine by extending public education to the populace has been hampered by logistical constraints such as lack of funds and human resources (Aberese-Ako et al. 2023). Discussions of the accessibility of the COVID-19 are yet to be brought to the fore. However, COVID-19 might not be the only threat to the well-being of persons with disabilities living in especially deprived communities. Thus, the findings reported in this study have implications for public health awareness, management, and resource allocation in developing a positive attitude toward COVID-19 vaccines to reduce vaccination hesitation among persons with physical and visual disabilities and hearing impairment. For example, tailored education and sensitization programs could be organized for different disability groups. The government could also partner with disability groups and organize training programs for their members. The mass media could also consider the needs of persons with disabilities when educating the public about vaccination, avenues, and other pressing issues. Moreover, sensitization programs and vaccines could be expanded to rural communities to ensure that all persons are given equivalent access to the vaccine. Thus, everyone would have fair access to vaccines and develop immunity against the disease.