
Abstract
This article examines the views of experts from a range of disciplines and how they view symptoms given to them by claimants in matters of personal injury or medical negligence assessments. The survey was carried out in 2009 and looks at current practice and attitudes from a number of different disciplines. The survey included questions looking at what percentage of cases were thought to be genuine, symptoms most likely to be elaborated, methods for assessing symptom validity, and documentary evidence required for a report. This article highlights the importance of looking at symptom validation in the legal process.
Introduction
When acting as experts in a legal context, our first responsibility is to represent genuine injuries and their consequences accurately to the Court. The aim of law is justice, and for that reason, genuine injuries are compensated. But the existence of false claims disadvantages the genuine claimant. The fact that false claims are sometimes not detected until after years of pleading and multiple examinations for Court reports, or that sometimes they receive compensation from the Court before deception becomes apparent makes defendant’s lawyers and insurers more sceptical of genuine claims, and makes claimants’ lawyers more prone to exaggerating what is a reasonable award. These mutual suspicions fuel an adversarial approach that Lord Woolfe tried to reform a decade ago. Therefore, as well as the explicit obligation of an expert to represent injuries and their consequences accurately, there is an implicit obligation to detect exaggerated or false claims of injury. Without accepting both responsibilities, experts unwittingly disadvantage the genuine claimant.
The complement of deceit is credulity. We are trained as clinicians to examine, listen to, and question our patients. But we are not trained to ask how our examination, attentiveness, and enquiries influence what we observe and what we are told. We are taught to credit the patient’s complaints. We are not alert to reasons patients may have to exaggerate or fabricate illness. It could be they want to be certified sick and unable to work, it could be they wish to be retired on medical grounds, and it could be the sick role has a particular fascination for them. Illness has many secondary gains, some obvious, some obscure, and the feigning of illness has many primary gains, none more obvious in the context of personal injury litigation than money.
This article examines the views of experts and how they view symptoms given to them by claimants in matters of personal injury or medical negligence assessments. A survey carried out in 2009 looks at current practice and attitudes from a number of different disciplines.
Symptom validity assessment
Research into the rates of malingering has burgeoned over the past 10 years. 1 There are various definitions of malingering. According to the APA, 2 malingering refers to the intentional production of false or greatly exaggerated symptoms for some external gain. Resnick 3 describes three types of malingering: pure malingering (complete fabrication of symptoms), partial malingering (exaggerating symptoms or reporting past symptoms as they if are ongoing), and false imputation (deliberate misattribution of actual symptoms to the compensatable event). As Iverson 4 points out, appreciating these different types of malingering is important as it illustrates that malingering can have a varied and complex presentation.
The base rate of malingering in personal injury claims is an important issue, i.e. how common is malingering in personal injury claims? Mittenberg et al.’s 5 survey of 388 members of the American Board of Clinical Neuropsychologists is one of the most commonly cited surveys. The survey revealed that 29% of personal injury claims (n = 6371) were thought to involve probable malingering. Malingering in mild traumatic brain injury (TBI) was estimated to be 39%, chronic pain 31%, fibromyalgia/chronic fatigue 35%, moderate-severe TBI 26%, neurotoxic exposure 26%, and electrical injury 22%. Larrabee 6 looked at the base rate of malingering in 11 published studies of mild TBI. An average of 40% (range 15–64%) was reported to be malingering.
Sullivan 7 surveyed neuropsychologists about the base rate of malingering in personal injury claims in Australia. Thirteen percent of personal injury cases were thought to be malingering. The highest rates of symptom exaggeration included cases referred for mild head injury (23%), pain or somatoform disorders (15%), moderate to severe head injury (15%), and fibromyalgia or chronic fatigue (15%). Overall, Australian symptom exaggeration base rates reported in this study were lower compared with base rates previously reported in North America. One explanation might lie in differing detection methods. Another could be the different legal system in Australia compared to the USA where the loser of litigation pays the costs in Australia whereas in the USA the plaintiff does not pay costs even if no settlement is awarded. 7 However, a base rate of malingering of 23% in mild TBI cases is still not a small number.
Clinical neuropsychological practice has seen increasing use of psychometric tests and questionnaires in the detection of malingering. 5 In the UK, McCarter et al. surveyed 588 members of the British Psychological Society Division of Neuropsychology to ascertain current practices with regard to symptom validity testing. Results showed that 59% frequently used symptom validity testing in legal assessments, but a minority (15%) employed symptom validity tests in clinical assessments. 8
One of the limitations of the above surveys is that the respondents were neuropsychologists and there was no survey of psychiatrists, neurologists, orthopaedic surgeons or other therapists. One aim of the current survey is to attempt to look at malingering from the perspective of a number of different disciplines. To our knowledge, and in reviewing the literature, such a multi-disciplinary survey has not been conducted elsewhere.1,5–7 In addition, surveys that targeted individual disciplines did cover topics we have looked at including listing the documentary evidence required in preparing a court report, and whether malingering may be considered a medical diagnosis?
It is because the clinician will examine unreliable or dishonest claimants, that experts reporting to the Court on personal injuries and related matters (e.g. fitness to stand trial) need to ensure the symptoms they record are genuine. This means not accepting symptoms at face value, but where possible validating their genuineness.
When dealing with signs (i.e. directly observable conditions such as the wasting of muscles or the eliciting of reflexes), the clinician has the advantage of being able to determine if the sign conforms to its expected signature. In the medico-legal context, this has resulted in alerting clinicians to signs at physical examination that raise suspicion of non-genuine complaints, e.g. Waddell’s 9 signs which indicate a non-organic component to pain, and the typical pattern of non-organic weakness and sensory loss.
But when examining the claimant’s symptoms (i.e. subjective complaints such as pain, forgetfulness, flashbacks), the checks available are less direct and may be hard to obtain.
Method
To establish something about the attitudes and practices of colleagues at consultant level regularly undertaking medico-legal work, the authors designed and circulated a survey in the summer/autumn of 2009. The authors, based on experience and in keeping with symptoms validity literature, devised questions to deal with salient issues such as the expected prevalence of deliberate exaggeration, methods by which experts establish the likely genuineness of complaints, and which profession, including the judiciary, is most appropriate to make final decisions.
Two hundred and ninety surveys were distributed. The bulk of the surveys were sent to experts identified from the Directory of Expert Witnesses. All persons practising in the fields of psychiatry and neuropsychiatry, neurology and neurosurgery, orthopaedics, neuropsychology and clinical psychology, and experts in the field of care provision (occupational therapy, physiotherapy, care reporting) were circulated. A small additional number of surveys were distributed to persons not registered with the Directory, but identified from other sources as frequently practising medico-legal experts.
Survey results
Figure 1 shows that of the 290 surveys distributed, 73 were returned wholly or partially completed (i.e. 25%). Psychiatrists returned the highest number of surveys (37%). Orthopaedic specialists returned the lowest number of surveys (17%). The overall return rate compares favourably with some comparable surveys. For example, there was a return rate of 22% (130/588) for a survey of contemporary practice in effort testing amongst British neuropsychologists conducted recently. 8 There are no clear data as to why certain disciplines had a higher rate of return in this survey.
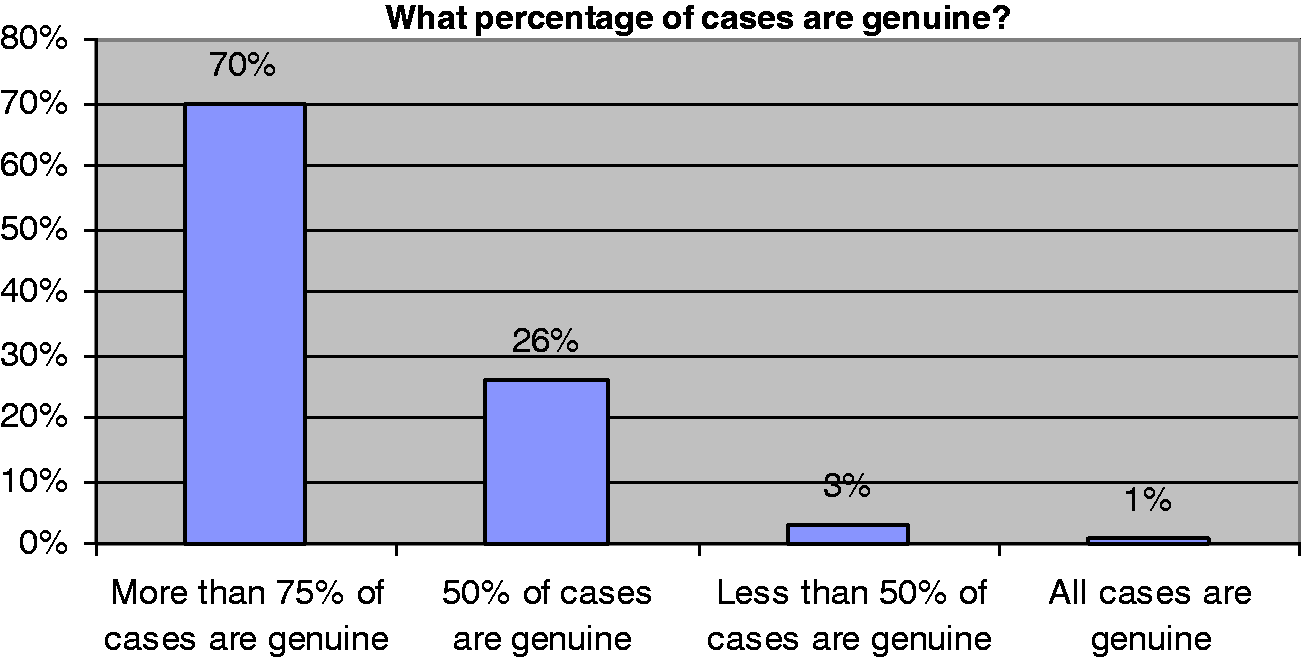
Figure 2 shows that on the contentious question of the prevalence of exaggerated or feigned complaints (Question 1), the modal response (70%) was that more than three-quarters of cases assessed were genuine. Twenty-five percent were more conservative opining that only 50% of cases were genuine. The evidence would seem to be that a small number of experts are markedly sceptical, but that the large majority think deliberate exaggeration is uncommon. Thus whilst only 11% of respondents had never expressed an opinion on possible elaboration or misrepresentation, 40% do not do so as a matter of course, implying that a significant number of experts presume complaints are genuine unless their suspicion is aroused (Questions 3 and 4).
The evidence most frequently relied on to test symptom validity was consistency between complaints and the medical history (49%), followed by complaints which were disproportionate to the severity of injury (32%). Perhaps surprisingly, behaviour at examination and interview was less frequently endorsed as likely evidence of misrepresentation.
Figure 3 shows that symptoms/conditions thought most likely to be elaborated were pain, including headache (50%) and cognitive complaints (35%).
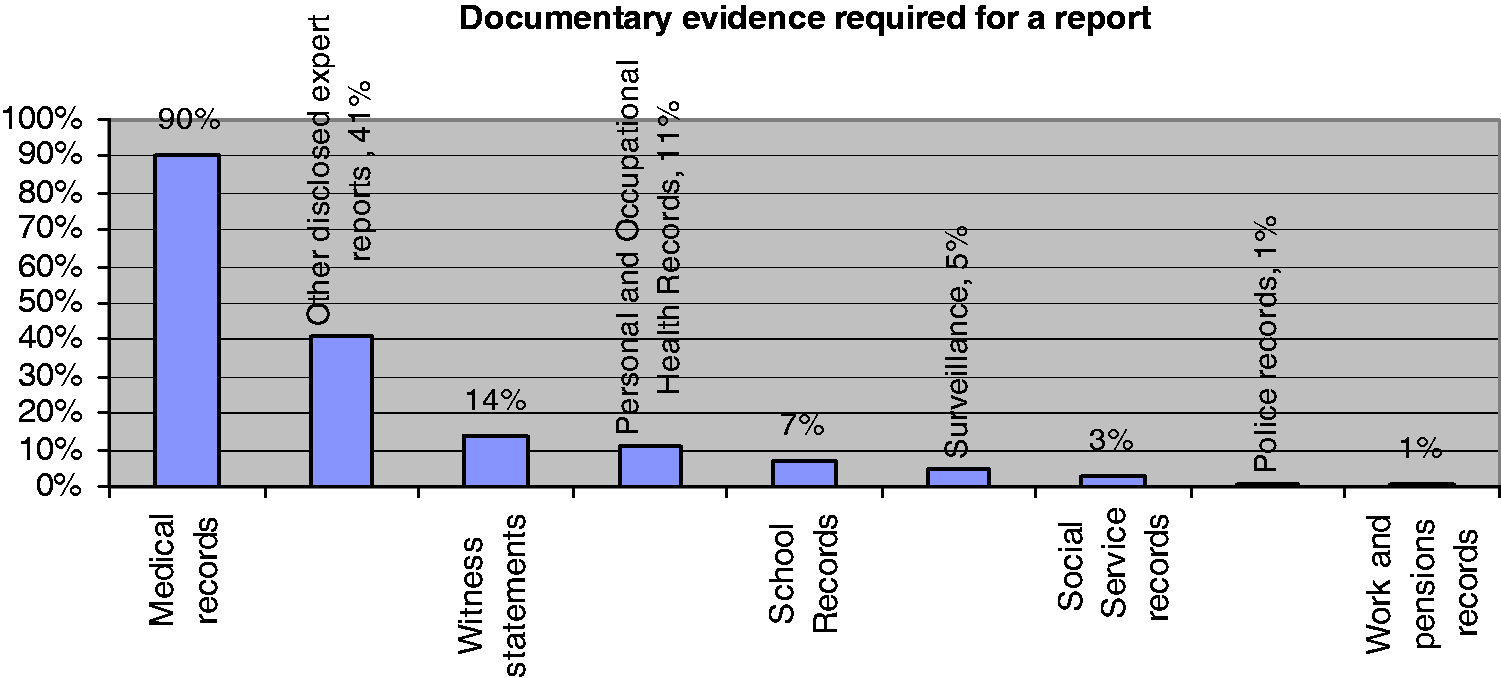
Figure 4 shows evidence that experts thought were required for a report. When asked about sources of evidence required as a matter of course when preparing a court report or regarded as desirable, lay evidence such as witness statements were given low priority (14% wanted them as a matter of course, 21% said they were desirable) and surveillance evidence (if available) was only listed as essential by 5% of respondents and as desirable by a further 5%.
Only 11% specified Pleadings as essential and 3% knowledge of quantum (quantum in this context refers to how much compensation is being claimed). However, when specifically asked about motivation to misrepresent symptoms, 46% of respondents agreed that it was desirable to know the size of award being claimed.
Forty-four percent of respondents do not routinely use any tests/procedures for symptom validation (Question 6).
On a related question, 55% of respondents did not reply when asked to specify peer reviewed articles or books that they found useful on the subject (Question 15). On examining the replies, there was little overlap between respondents to these two questions. Half of those who routinely use some form of symptom validity testing did not specify any peer reviewed sources that were useful in their practice.
Twenty-five percent of respondents thought that malingering was a medical diagnosis (Question 16). When asked to consider who might make a final decision about whether a claimant was malingering (recognising that the different possibilities offered might apply in different situations and therefore more than one professional might be appropriate), 68% preferred the Judge to be the arbiter, whilst 28% felt either any expert, or 31% an expert in psychiatry/psychology could make a final decision. The idea of an independently appointed Court assessor received little support (8%).
Return rate of respondents. Percentage of cases that are considered genuine by experts. Symptoms/conditions most likely to be elaboration. Documentary evidence that experts consider to be necessary for their opinion.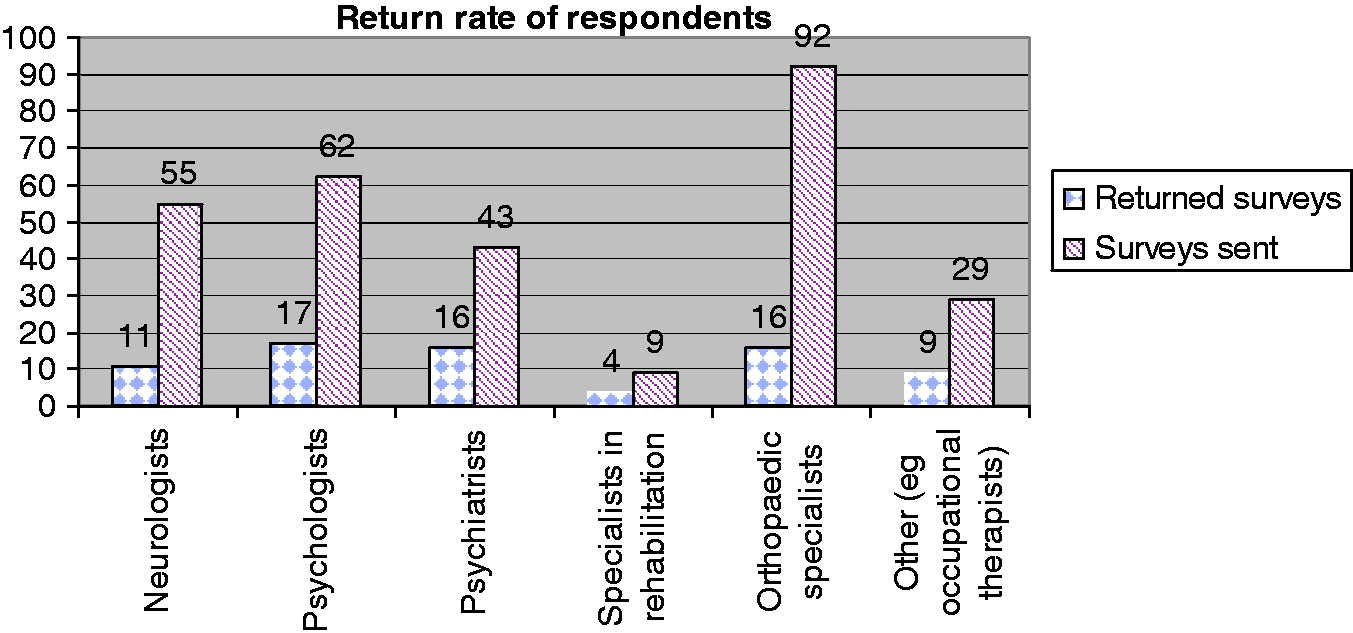

Discussion
Relying on the respondent profile, amongst the larger professional groups, responding psychiatrists are the professionals who are most concerned about validating complaints (37% of those surveyed responded) and orthopaedic specialists the least interested (only 17% response rate). There was a surprising lack of concern amongst psychologists and neurologists responding, especially as one would expect a self-selection process to have operated, with those experts more interested in the matter of validation likely to respond.
It is notable that respondents when evaluating genuineness of complaints place comparatively less emphasis on evidence gained directly from examination compared to evidence from the clinical history. This is an interesting finding, as over 50% of respondents stated that they routinely use tests/procedures to validate symptoms. One wonders whether such procedures are adopted by some experts as good form, rather than out of personal conviction of their value. This possibility is supported by the number of comments made on the matter such as: ‘history and examination are best indicators’; ‘validity of such instruments remains questionable’; ‘I am unaware of any reliable tests or procedures that are of help’; ‘I have found personal experience more useful than any of the above (peer reviewed publications)’.
Further evidence of scepticism regarding symptom validity testing is that half of those who stated they regularly use some objective assessment procedure did not list any peer reviewed publications which they had found useful. Although there is a rapidly expanding volume of publication on this subject, the overall impression is that most experts, including very seasoned experts, are yet to be convinced that methods of objective assessment reliably contribute to validating a claimant’s complaints.
The comparative reticence of experts to move away from a primarily clinical basis for making decisions on symptom validity is well illustrated by the lack of enthusiasm regarding surveillance evidence (see replies to Questions 2 and 10). There are occasions when surveillance provides irrefutable evidence that alleged complaints have been exaggerated or fabricated. But only 12% of respondents identified it as an important indicator (Question 2) and only 5% thought it either an essential or desirable source of evidence (Question 10). The claimant’s injuries are therefore being defined by what is found in medical records and at examination; an artificial and extremely selective sample of their behaviour.
A related fact is the comparative lack of emphasis given by respondents to lay evidence, other than that of the claimant. For example, only a third of those responding to Question 13 thought it Very Important to interview another informant, and a fifth thought it Not Important at all. Witness statements were only regarded as essential documentary evidence by some (Question 10). Those who listed it as desirable (21%) often specified that only the witness statement of the claimant was required (Question 10). Sworn Witness Statement’s carry significant weight in establishing facts for the Court unless disproved or called in doubt by other evidential sources. They therefore require the expert’s attention, but we suggest that experts should note that family members or friends frequently repeat the same details within the claimant’s statement. This often includes terms as multi-tasking, disinhibition and executive functioning as if these terms are in daily colloquial usage.
With regards to the question as to whether malingering (deliberate exaggeration and fabrication of complaints) is or is not a medical diagnosis, the majority of respondents answered this question (number 16) in the negative (75%). The majority view on this matter is that malingering by definition is not a feigned illness or disease and therefore there is no illness to diagnose. A less confident view would be that malingering is a diagnosis of exclusion, but insofar as the behaviour concerned is deliberate, when other diagnoses have been excluded, what we are left with is not a medical condition. But there is also an argument that because malingering is listed in diagnostic manuals (e.g. DSM-IV) ipso facto it is a medical diagnosis. Finally, it could be argued that insofar as we are able to reliably distinguish real and feigned signs and symptoms from use of objective examination and tests, then the existence of malingering is established on just the same basis as other medical conditions and therefore it is a positive diagnosis, not just a diagnosis of exclusion.
The view an expert takes on this matter is likely to influence their opinion about who should decide whether malingering is present or absent (Question 17). When asked who is appropriate to express a final opinion on the matter most experts would defer to a Judge (68% of those responding). Less than half as many experts felt that a medical expert should reach such a conclusion, and the suggestion that there might be an independent assessor to the Court advising on the matter was unpopular (only 8% agreeing).
In terms of future surveys, it would be helpful to repeat this survey at a later date to see whether medical experts have changed their views and approaches to detecting malingering as research into this area continues to grow. It would also be useful for there to be work between different disciplines as to what types of documentary evidence may be considered essential in conducting court reports.
Lawyers, the Courts and society as a whole need to recognise that from our results many experts even those with extensive medico-legal experience do not feel comfortable in questioning the integrity of claimants. This must favour the elaborating claimant and in turn generate greater difficulty for the genuinely injured individual. The Courts have begun addressing this with recent contempt hearings finding claimants and their families guilty of deliberate falsification of functional handicap. A consistent, consensually defined role for the expert is however some way off.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.