Abstract

Sudden Arrhythmic Death Syndrome (SADS)
A previously well Caucasian male in his early 50's collapsed shortly after experiencing severe chest pains at home. He developed hypoxic brain damage and survived for a further 7 days in the Intensive Therapy Unit (ITU) before expiring. In the previous 6 months, he had had 3 episodes of atypical chest pains with visits to the Accident and Emergency department, with subsequent investigations into coronary artery disease resulting in 2 unremarkable angiograms. At post mortem examination he was found to weigh 80.7 kg and measured 177.5 cm in length with a body mass index of 25.6 kgm2. The heart (374 mg) showed slight left ventricular hypertrophy and appeared to have bulging of the left ventricle near the outflow tract. The only gross pathological findings were that of moderate atheroma of the right coronary and left anterior descending coronary arteries. Both lungs (Right: 986 gm; Left: 854 gm) showed marked edema and congestion. Examination of the formalin fixed heart revealed areas of sub-endocardial infarction (Figure 1).
Areas of sub-endocardial infarction in formalin fixed heart tissue.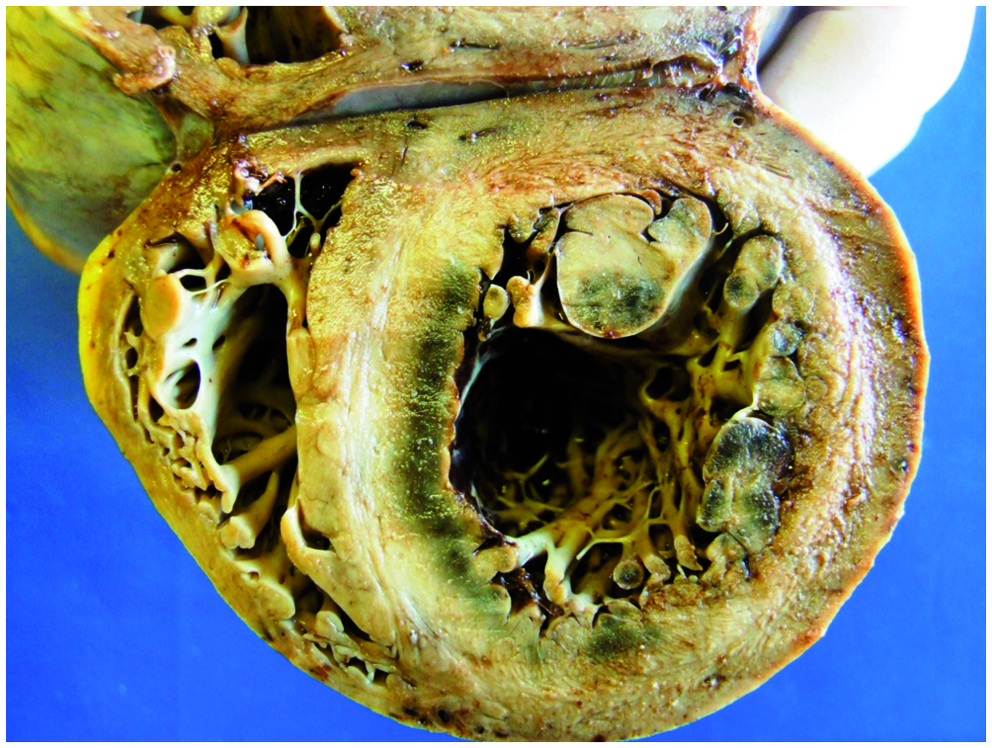
Microscopic examination of the heart shows widespread infarction (Figure 2) mainly in the subendocardium of the interventricular septum and anterior left ventricle, in keeping with survival following cardiac arrest.
Heart (H&E): Dead myocytes with haemorrhage.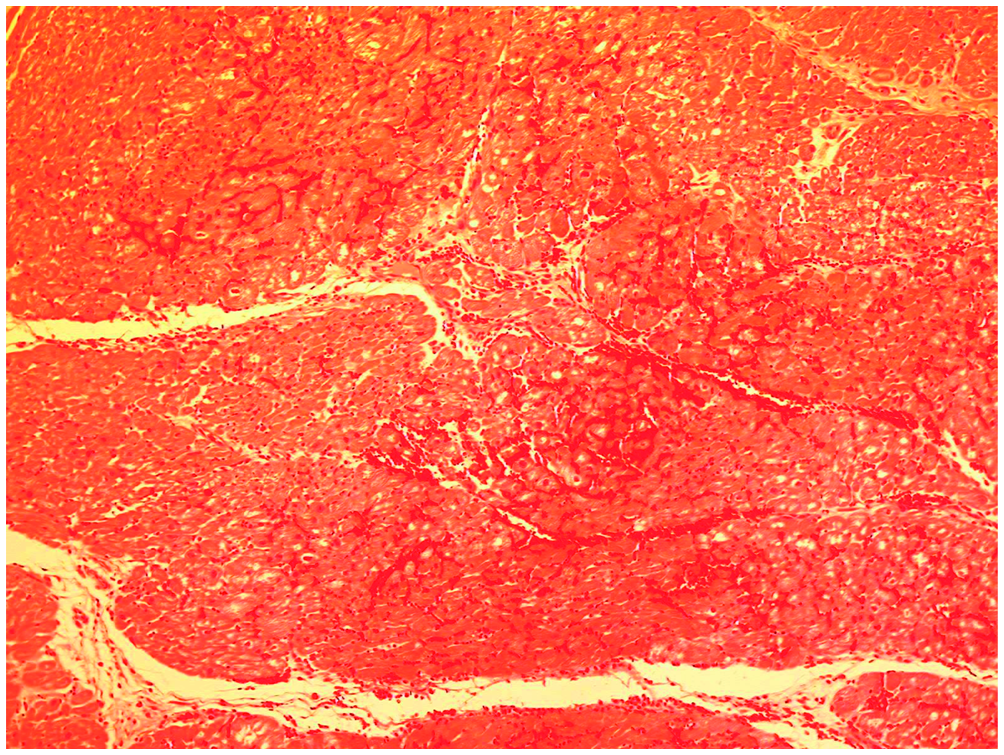
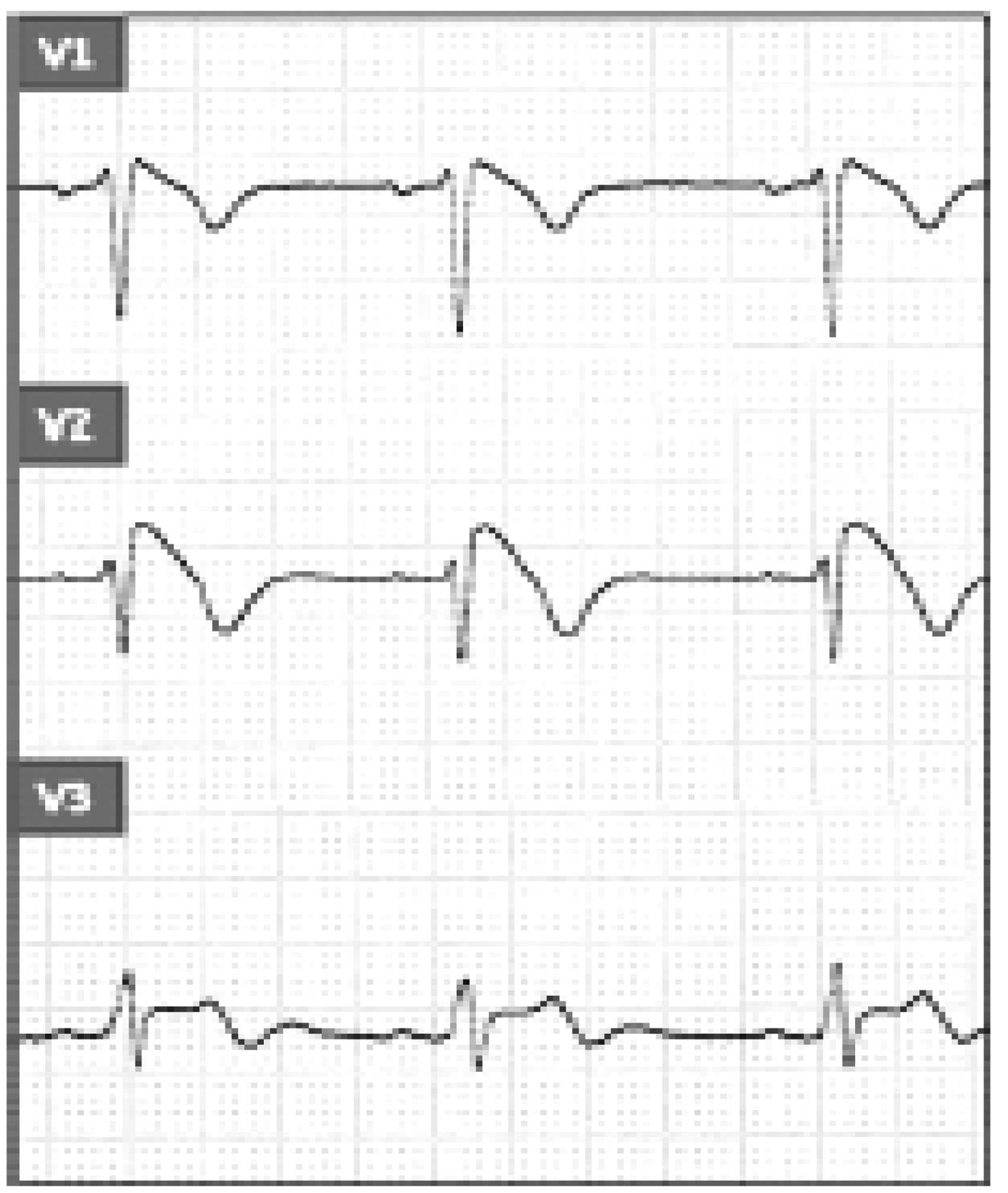
Microscopy of the remaining tissues is unremarkable. Post mortem toxicology was not carried out due to length of hospitalization. Review of his previous admission electrocardiogram (ECG) revealed the following pattern (Figure 3).
Electrocardiogram pattern of the right pre-cordial leads during previous admission for chest pain. What does the ECG show? What is the significance of the ECG changes? What is the relevance of these findings and the role of the Forensic Pathologist in such cases?