
Abstract
Introduction
When a law enforcement officer (LEO) stops a suspect believed to be operating (a vehicle) while impaired (OWI), the suspect may resist or flee, and the LEO may respond with force. The suspect may then undergo a Standardized Field Sobriety Test (SFST) to gauge impairment. It is not known whether resistance, fleeing, or actions of force can create an inaccurate SFST result. We examined the effect of resistance, fleeing, and force on the SFST.
Materials and Methods
Human volunteers were prospectively randomized to have a SFST before and after one of five scenarios: (1) five-second conducted electrical weapon exposure; (2) 100-yard (91.4 m) sprint; (3) 45-second physical fight; (4) police dog bite with protective gear; and (5) Oleoresin Capsicum spray to the face with eyes shielded. The SFST was administered and graded by a qualified LEO. After the SFST, the volunteer entered their scenario and was then administered another SFST. Data were analyzed using descriptive statistics. SFST performance was compared before and after using chi-square tests.
Results
Fifty-seven subjects enrolled. Three received a single-point penalty during one component of the three-component SFST pre-scenario. No subject received a penalty point in any components of the SFST post-scenario (p = 0.08).
Conclusions
This is the first human study to examine the effects of physical resistance, flight, and use of force on the SFST result. We did not detect a difference in the performance of subjects taking the SFST before and after exposure to resistance, flight, or a simulated use of force.
Introduction
Operating a vehicle while impaired is a significant problem in many countries around the world.1,2 In 2012, in the United States, 10.3 million people aged 12 years or older reported operating a vehicle under the influence of illicit drugs within the previous 12 months, and an estimated 11.2% of the same population had operated a vehicle under the influence of alcohol within the previous 12 months. 3
During law enforcement stops of suspects who are believed to be operating (a vehicle) while impaired (OWI), there is the potential for the detained suspect to resist detention in some fashion. While this resistance may be minimal (e.g., verbal resistance only), in some circumstances it can escalate to fleeing from or a physical altercation with the involved law enforcement officer (LEO). If this occurs, the LEO may respond in a number of ways and with different force options. An OWI suspect may be subjected to a Standardized Field Sobriety Test (SFST). The results of the SFST may provide the LEO with a gauge of impairment. It is not known whether resistive behavior, fleeing, actions of force, or anxiety associated with these behaviors just prior to the SFST administration can create an inaccurate SFST result and mislead the LEO to investigate further for OWI, even if no impairment is present. In this study, we examine the effects that physical resistance, flight, and usage of force may have on a subsequently administered SFST on unimpaired human subjects.
Methods
Study design
This was a prospective, before and after, observational study of human subjects participating in a law-enforcement training exercise. The institutional review board at Hennepin County Medical Center (Minneapolis Medical Research Foundation, Minneapolis, MN) approved the study.
Study setting and population
The study was conducted during training courses at the Thomas A. Hontz Police and Fire Training Facility (Tempe, AZ). The volunteer subjects were a convenience sample of LEOs, LEO recruits, and corrections personnel participating in defensive-tactics training courses. Familiarity with the SFST was not a requirement, and none had specialized training in this area. The study scenarios were part of the training, and the volunteers had the expectation of participating in them as part of the course regardless of enrollment. Refusal to participate in the study did not absolve a potential volunteer from participating in the scenarios in order to complete their training successfully.
Study protocol and measurements
The volunteer subjects provided written informed consent and completed a medical screening questionnaire that was reviewed by a study physician. Participating volunteers had to be at full-duty status with their employer, and the only other specific exclusion criteria were known drug or alcohol intoxication, pregnancy, mental illness, and sleep deprivation in the preceding 24 hours. The volunteers were randomized to have data collected during one of five scenarios that were part of the training course: (1) a five-second TASER® X26™ Conducted Electrical Weapon (TASER International, Inc., Scottsdale, AZ) exposure with deployed probes to the back from an approximate seven feet (2.1 m) distance (CEW); (2) a sprint of 100 yards (91.4 m) with changes in direction and a crawl to simulate a foot chase (Sprint); (3) a 45-second fight against an opponent to simulate physical resistance (Fight); (4) a police dog search and bite exercise (with protective gear) to simulate a confrontation and induce anxiety (K-9); and (5) a spray of 10% Oleoresin Capsicum to the face and neck with the eyes shielded (OC). The Sprint and the OC spray scenarios were performed outside during full daylight in ambient temperatures of approximately 100 F (37.8℃). The remaining scenarios were performed within an air-conditioned, portable enclosure.
A commercial body composition monitor and scale (Omron Full Body Sensor, Model HBF-516B, Omron Healthcare, Inc., Bannockburn, IL) was used to determine weight and body fat percentage for descriptive purposes. The volunteers were asked to provide their height to the investigators, and body mass index (BMI) was calculated from this information. Vital signs were measured prior to the scenarios (Nonin 2120, Plymouth, MN) and included pulse, blood pressure, and oxygen saturation on room air.
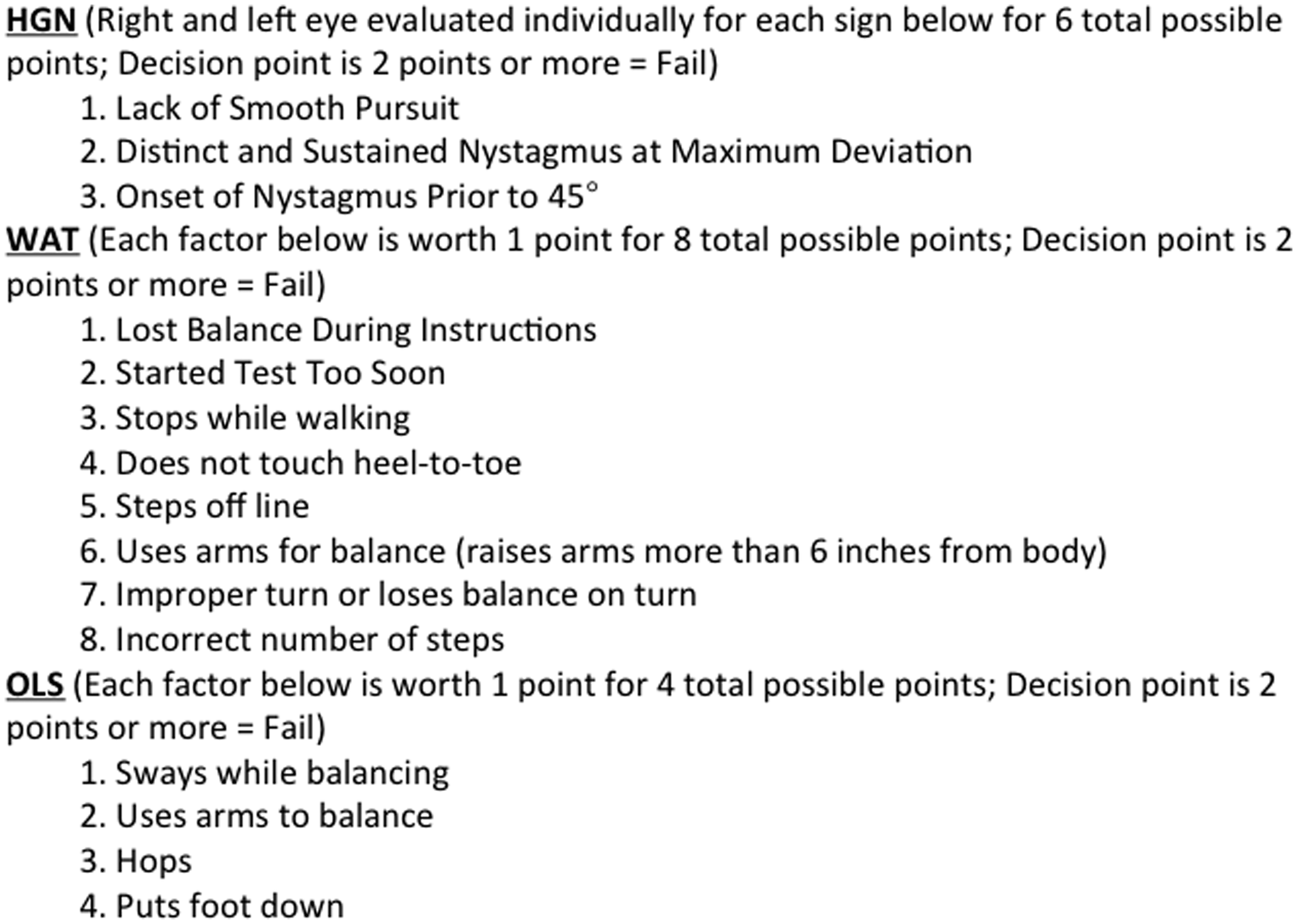
Prior to their study scenario, the volunteers were administered the following SFST battery in this order: horizontal gaze nystagmus (HGN), walk and turn (WAT), and one-legged stand (OLS). HGN measures involuntary jerking of the eyes as they follow a slowly moving target at eye level. HGN is the most reliable component of the SFST and measures six factors for scoring. WAT is a test of divided attention (divided between balance and information processing) and has two stages: the instructional stage and the walking stage. The subject maintains a heel-to-toe standing position with arms at their side while receiving instructions for the walking stage and is told to take nine heel-to-toe steps forward on command, turn around in a prescribed manner using a planted foot and small steps with the nonplanted foot, and take nine heel-to-toe steps back to the starting point. They are instructed to count their steps out loud as they take them. WAT measures eight factors for scoring. OLS is also a test of divided attention (divided between balance and information processing) and has two stages: the instructional stage and the balance and counting stage. The subject maintains a standing position with arms at their side while receiving instructions for the balance and counting stage. On command, they raise either foot approximately six inches (15.2 cm) off the ground and keep both legs straight. They look at the raised foot and count out loud “1001, 1002, etc.” until told to stop. They are timed for 30 seconds. OLS measures four factors for scoring. See Figure 1 for the factors measured in the SFST and an interpretation of the scoring process.
Standardized Field Sobriety Test (SFST) component scoring criteria. A failing score indicates an individual component sensitivity to detect a blood alcohol concentration of 0.08% or greater with these accuracies: horizontal gaze nystagmus (HGN) 77%, walk and turn (WAT) 68%, and one-legged stand (OLS) 65%. A failure of all three components yields a sensitivity of 80% accuracy.
22
The SFST was administered per the Minnesota State Patrol Field Sobriety Instructions that closely mimic the USA National Highway Transportation and Safety Administration (NHTSA) SFST Administration Instructions. 4 The SFST was administered by a sworn LEO who had received 16 hours of approved SFST training by the Minnesota Department of Public Safety and had undergone regular refresher training. The SFST was administered under indoor lighting conditions on a flat hard surface. Following administration of the SFST, the volunteer was sent to perform their assigned study scenario.
For the CEW scenario, the volunteers wore safety glasses and were exposed in a standing position on protective padded mats. They had a person on either side helping to support them if they fell during the exposure. The exposures were performed by a qualified TASER International, Inc., CEW Instructor. The CEW probes were deployed to the volunteer’s back from seven feet (2.1 m) with a TASER X26 CEW using standard 25-foot cartridges and XP (13 mm) darts and the CEW was allowed to run for the standard five-second duty cycle. The CEW manufacturer provided CEW product and training personnel to assist with this portion of the study.
For the Sprint scenario, subjects sprinted 100 yards (91.4 m) on an outdoor, hard-paved, level track that was set up with two obstacles. The first obstacle was a 15-yard (13.7 m) section that required the sprinter to weave in a tight “S” pattern during the middle of the course. The second obstacle was a five-yard (4.6 m) crawling section at the end of the course. The subjects were timed by stopwatch and were encouraged to give maximal efforts by voice encouragement during the sprint.
For the Fight scenario, subjects wore padded helmets, gloves, and foot protection. They were instructed to resist vigorously an instructor wearing a heavily padded fight suit on a padded protective mat for 45 seconds. The instructor’s goal was to try to maintain physical contact with the volunteer for the entire time while physically harassing, blocking, and pushing them, but he did not punch or kick the volunteer. The volunteer was instructed to do whatever was necessary to get the instructor off and away from them. The volunteer was allowed and encouraged to punch, kick, push, and use elbow and knee strikes to accomplish this task. This task was timed by stopwatch.
For the K-9 scenario, subjects wore a padded bite suit and hid in a maze constructed of cardboard boxes within an enclosed space of 400 square feet (37.16 m2), and an active duty law enforcement dog and handler were used. The volunteers in this exercise were instructed to hide toward the rear of the maze. The maze was reconfigured randomly between volunteers to avoid any memorization of the maze by the dog. The dog team began the exercise at the front of the maze, and the dog knew that it was searching for a suspect to bite. The dog was also encouraged to bark at the beginning of the exercise prior to release, and the dog handler was encouraged to shout commands to increase the volunteer’s anxiety of the pending discovery. During the search, the dog was off the leash. Prior to starting this exercise, the volunteers were told that they would be discovered and bitten by a police dog. They were told to present their arm to the dog when found. The dog was allowed to stay on the bite for 20 seconds, and the volunteers were instructed to resist the dog while it was on the bite during this time.
Volunteers in the OC scenario wore swim goggles during the actual spray stream exposure to prevent them from being so blinded by this that they would be unable to open their eyes for the post-exposure SFST. They received a stream of OC spray (Sabre Red, 10% OC, Security Equipment Corp., Fenton, MO) from a factory canister to the face and neck in a “Z” pattern starting at their forehead and ending at their neck. After this exposure, they had their face and neck rinsed with clean water in front of a fan located at a decontamination station and were instructed to remove their swim goggles. The decontamination process lasted approximately 90 seconds. They were given a wet rag to take with them to apply to their face and neck as needed during the post-exposure period.
For all volunteers, vital signs were taken immediately following their scenarios, and again between 10–15 minutes post-scenario. Immediately following the second set of vital signs, the volunteer was administered the SFST as described above by the same LEO that had conducted the test earlier and in the same environmental setting. Scoring was again recorded according to established criteria (Figure 1).
Data analysis
Data were entered into an Excel spreadsheet (Microsoft Corp, Redmond, WA) and exported into STATA 10.0 (Stata Corp., College Station, TX) for analysis. Descriptive statistics were applied where appropriate. The success of the SFST was compared before and after the scenario using chi-square tests. Assuming a baseline failure rate of <0.01%, in order to find a difference of 10% between the SFST failure rate (a 10% increase), we estimated that 45 subjects were needed.
Results
Baseline volunteer data.
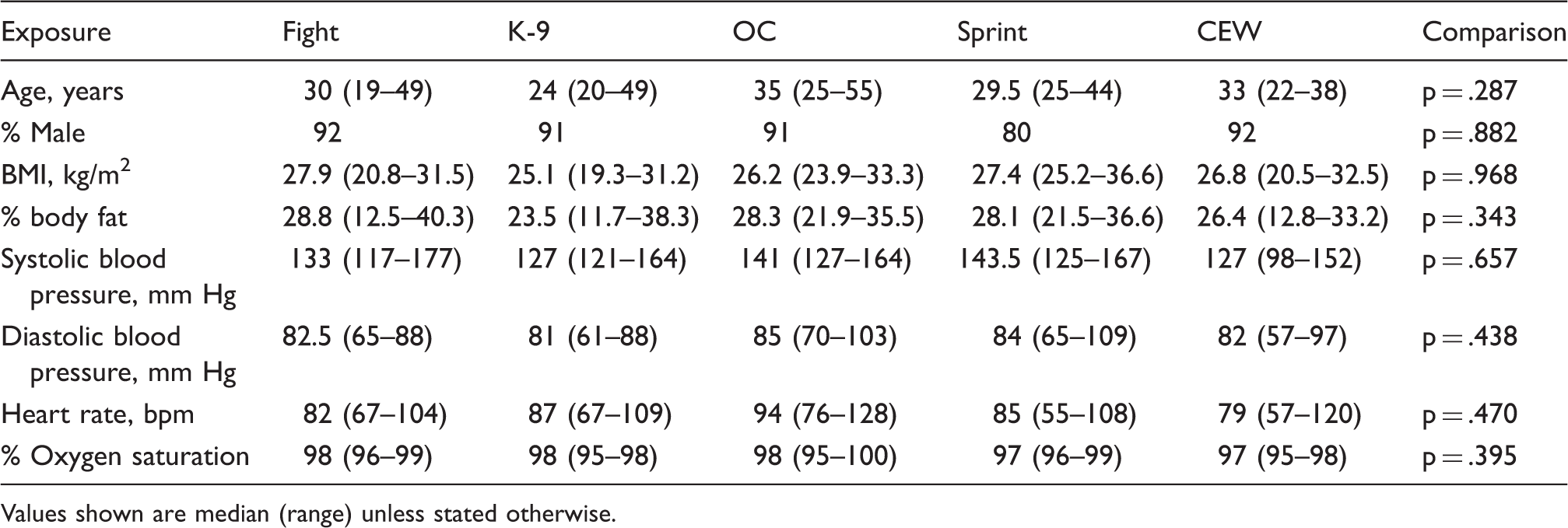
Values shown are median (range) unless stated otherwise.
Post-task data (immediate measurement).

Values shown are median (range) unless stated otherwise.
Post-task data (10 minutes after task).
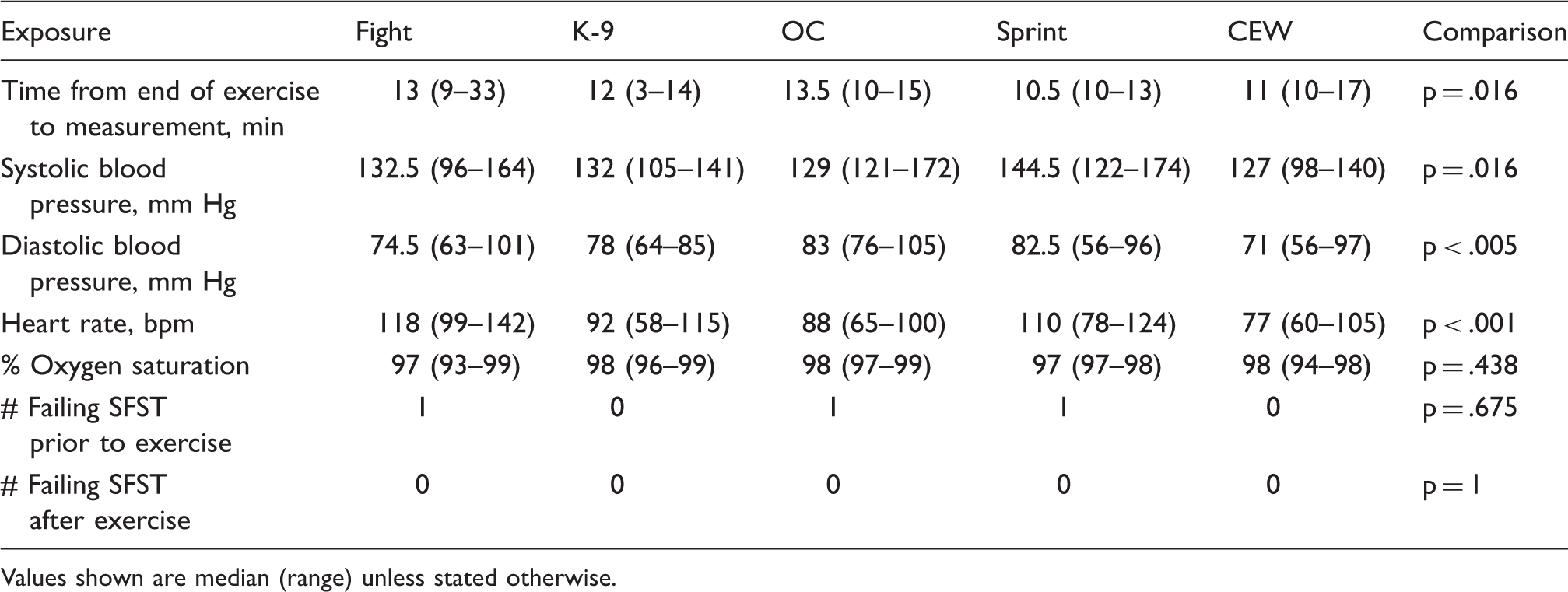
Values shown are median (range) unless stated otherwise.
Discussion
OWI is a significant and common problem within modern society, and public safety agencies report that OWI cases result in numerous injuries and deaths each year.1–3 In 2010, the USA NHTSA reported that more than 10,000 persons died in motor vehicle crashes involving impaired vehicle operators. 5 Although ethanol is typically what comes to mind as the most prevalent intoxicant involved in OWI cases, the term “OWI” is meant to encompass impairment due to any substance (controlled, medicinal, legal, illegal, or otherwise), and there have even been OWI reports following nonalcoholic energy beverages that are commonly used on a daily basis.6,7
The SFST is a primary screening tool used by LEOs to evaluate vehicle operators for impairment in the field. Prior to our study, it was not known if certain resistive behaviors by the suspect or use of force by the LEO could cause neurocognitive or psychomotor dysfunction that might lead to a SFST evaluation that would be different from one where these factors did not exist. It was also unknown what effect, if any, the anxiety present in those situations may have on accurate SFST evaluation. There have been circumstances where force has been necessary to control an OWI suspect who later underwent SFST administration shortly after resistance, flight on foot, or the use of force. In the 2012 court trial testimony for State of New York v. Robert Collins, it was established that the defendant was operating a motor vehicle, was stopped for a speed violation, and subsequently fled on foot from the scene in an attempt to evade arrest for suspected OWI. 8 During his apprehension, the defendant also received a six-second CEW deployed probe exposure to the back (probe locations in the mid and lower back) from the pursuing LEO. A SFST was administered to him several minutes later, and he failed the HGN, WAT, and OLS components. At trial, the defense counsel attempted to blame the defendant’s total SFST failure upon lasting neurocognitive and psychomotor impairment from the CEW application, despite the presence of a significant amount of ethanol in his system. This defense was ultimately unsuccessful but did initiate the question of whether or not a suspect’s resistive actions or a LEO’s use of force upon that suspect could alter the result of the SFST.
When an investigatory stop of a suspected OWI violator by a LEO occurs, the goal of the LEO is to investigate the LEO’s suspicions expeditiously to determine if the LEO has sufficient objective probable cause to justify the suspect’s arrest for OWI legally. The stop typically occurs after the LEO has witnessed some type of suspicious vehicle operating conduct, received a complaint from a witness about abnormal vehicle operating conduct, or in response to an investigation of a vehicle crash that has already occurred. As part of the initial OWI investigation, the LEO will seek general clues from the suspect to decide whether to continue the investigation. These general clues may include factors such as open alcohol containers in plain view, suspect conduct and behavior, verbal admission of intoxicant usage, odor of intoxicant (such as alcohol or marijuana) associated with the suspect, and general appearance of the suspect. If, based on the LEO’s training, guidance, and experience, the LEO has objective and reasonable articulable suspicions of OWI, they can expand the scope of their investigatory stop and request the suspect to participate in a SFST.
Prior to 1981, there was not a standardized way to evaluate a person in the field for substance impairment. While there were laws in many countries at that time prohibiting OWI, the determination of impairment was left to physicians (usually emergency physicians) after a medical evaluation. There were many tests used at that time to evaluate impairment. These included tests such as walking, gait with turning, balance, finger-to-nose, picking up matches, counting backwards, time and place orientation, and observations of speech and general behavior. These tests were not standardized. Some of these tests depended on the subjective opinion of the physician, and some were not well suited for use in all populations. As an example, the test of counting backwards was found to be more difficult for persons of lower socioeconomic status. 9 Later, it was also found that the subjective physician opinions were inaccurate and of little value. 10
In 1981, Tharp et al. produced a report on work that was funded by the United States Department of Transportation, NHTSA. 11 This report is largely credited with solidifying the legal SFST process for OWI suspect field evaluations. The SFST battery is a combined evaluation of involuntary neurophysiologic activity (HGN) and psychomotor tasks (OLS and WAT) designed to evaluate potential impairment. The OLS and the WAT components require the ability to multitask with divided attention, a process that can be a mild challenge for a sober individual, but one that becomes increasingly difficult with increasing impairment.
The modern-day SFST battery is used in the United States by trained LEOs as a high-sensitivity screening tool for establishment of potential impairment. The development of this test battery is generally credited to the initial work by Burns and Moskowitz. 12 Their work was based on ethanol intoxication and found that the three best standardizable field evaluations to screen for a blood alcohol concentration (BAC) of 0.10% or greater were the HGN, WAT, and OLS. The HGN examines the amount of nystagmus present in each eye as the subject is asked to follow a moving target visually. The HGN test largely evaluates involuntary eye movement and is not something that a person can learn to control by practicing. The WAT and OLS examine the subject for balance and ability to follow instructions (neurocognition) as they demonstrate straight-line gait, heel-to-toe walking with a turn, and the ability to stand steady on one leg for a period of time respectively. In combination, these three components of the SFST have a validated sensitivity of approximately 80%. These three components were later revalidated to be sensitive to screen for a BAC of 0.08%. 13 This is currently the accepted per se threshold for ethanol related OWI in all 50 states of the United States. These three components continue to make up the accepted SFST battery administered in the field and were what we used in our study.
In the report by Tharp et al., SFST administration to an OWI suspect is described as a social interaction between the suspect and the LEO. 11 The report indicates that during an OWI investigation, if the suspect is going to exhibit potentially hostile or extreme behavior, it most often occurs if they are impaired. Impaired suspects are also those most likely to be selected by the LEO to undergo SFST administration. In situations such as this, LEOs are allowed to use an objectively reasonable amount of force to control the suspect and the situation. The purpose of this paper is not to discuss force options or tactics, but suffice to say that there are many options available, depending on the totality of the circumstances as objectively and reasonably perceived by the LEO. Our study suggests that significant suspect resistance, fleeing, or the application of common LEO force options does not deteriorate SFST screening accuracy when performed 10–15 minutes after the resistance, fleeing, or use of force event.
In the case of State of New York v. Robert Collins, 8 the response to the suspect’s flight and resistance was the LEO’s foot pursuit and use of a CEW. By definition, a CEW utilizes electrical charge and delivers this from a capacitor system in discrete pulses at fast rates (19 pulses per second in most models), leading to the depolarization of peripheral motor neurons within a “zone of capture.” This results in subsequent involuntary, subtetanic muscle contraction. The CEW also depolarizes afferent sensory neurons leading to pain. The theory behind how a CEW exposure might alter the outcome of an SFST evaluation was not well established in the above-referenced legal case. However, it was inferred that because a CEW affects the neuromuscular system, there might be lingering muscular, cognitive, or nervous system control issues. There is legal literature that opines that physical or emotional stressors might affect a person’s ability to drive or successfully perform tasks of divided attention such as the SFST. 14 Our study does not appear to support this opinion, although we did not test our subjects against every possible physical or emotional stressor that could have been present.
Prior to our study, there was nothing in the literature to support or refute the opinion inferred above. The CEW human study literature to date has examined primarily basic cellular, electrolyte, cardiac, and respiratory physiology.15–20 There has also been a relevant study examining the effect of extended 15-second CEW simulated probe application upon intoxicated human adults. 21 None of this CEW literature has suggested an acutely harmful or delayed physiologic compromise. Based on our current study, we also did not find any correlation with stress from resistance, fleeing, or use of force including a CEW application causing neurocognitive or psychomotor impairment that would prevent a person from participating accurately in a SFST.
Our study has important implications for LEOs in the field and legal professionals in the justice system. It should reassure LEOs to know that they can rely on their training, experience, and the validity of the SFST even in an event where resistance, fleeing, or use of force has occurred. This should also reassure legal professionals that the SFST result does not deteriorate or become altered following resistive or forceful suspected OWI events.
Limitations
Our study has potential limitations. During true OWI investigations in the field, there is typically a perceived sense of anxiety on the part of the suspects because they are aware that there may be legal consequences associated with their performance. Because this study was conducted in a field laboratory setting using consenting volunteers, the same conditions of legal consequence were not present. It is difficult to know what effect this may have had on the study results, if any. We believe, however, that by not having any true legal ramifications associated with their SFST performance during this study, the volunteers would have been more likely to underperform and less likely to demonstrate performance enhancement. Furthermore, our subjects were not intoxicated. It is possible that there are differences in the study results that may have been detected if the studied subjects were impaired at the time of testing. It is also possible that because each volunteer participated in the SFST twice, there may have been some learning that led to artificial improvement of their performance during the second SFST. Although this may explain the result of none receiving point deductions during their second SFST, this result did not reach statistical significance.
Another limitation of our study is that the same investigator performed the SFST on all subjects before and after. This lack of variation may have introduced the possibility of bias, since the investigator was not blinded to whether the test was being administered before or after the exertion/force event. It is also possible that our volunteers may have exhibited performance enhancement through behavior alteration (also known as the “Hawthorne Effect”). This can occur in persons when they know that they are being observed. The volunteers in this study were not blinded to the protocol of taking part in a SFST before and after their scenarios. Because they knew they were in a testing environment with researchers recording their behavior, this may have artificially inflated their performance during the SFST administration. However, we believe that the environment of having them know that they were being observed is quite similar to what occurs in the field when a LEO conducts a SFST on an OWI suspect. Additionally, the HGN component of the SFST battery is an evaluation of involuntary nystagmus. This is not something that the subject can control or improve upon with effort or practice.
Another possible limitation to our study was that the volunteers in the OC scenario were allowed to wear swim goggles for eye protection during their scenario, and the volunteers in the K-9 scenario were wearing a protective suit. In reality, suspects receiving OC or K-9 exposures in the field are unlikely to be wearing similar protection and may have more physical impairment during a SFST administration because of this. Field OC spray largely impairs vision and a field K-9 bite has a high probability of resulting in a significant suspect physical injury. Both of these factors would impair the true ability of a suspect to participate in a SFST. However, SFST administration guidelines advise the LEO to ask the suspect if they have any physical conditions that would prevent them from fairly participating in the test, and if they do, it is inadvisable to continue the test out of concern for their safety. Based on this, it is unlikely that a suspect would be allowed to continue in a field SFST if their vision or physical abilities were significantly limited in the field.
Finally, our SFST environment may not have been as challenging as a field situation. In our study, the volunteers were tested on a flat, level surface free of debris. There was good ambient and fluorescent lighting, and there were no distractions such as motor vehicles passing closely by or flashing emergency vehicle lights. In a field situation, the surface used for SFST administration is not always pristine, and lighting may be dim or may include flashing emergency warning lights that could lead to some disorientation. Closely passing traffic also can present a safety hazard and a distraction. However, our goal was to evaluate the result of the actual SFST and not the testing environment.
Conclusions
This is the first human subject study to examine the effects of physical resistance, fleeing, and simulated use of force on the results of a SFST. We did not detect a significant difference in the success of subjects taking the SFST before and after simulated resistance, simulated fleeing, or a simulated use of force encounter. The SFST battery appears to function the same and yield a similar result if the encounter has involved physical resistance or flight by the suspect or a LEO use of force. This study may be limited by the artificiality of the lab conditions in which it was conducted, but it can serve as a significant contribution to the literature regarding use of force and neurocognitive or psychomotor impairment.
Footnotes
Acknowledgments
The authors acknowledge the logistical and technical expertise of Ms. Jami LaChapelle and Mr. Matthew Carver during this project. They also acknowledge the study concept contributions of Captain Eric Underhill and the Troopers of the New York State Police. This project could not have been completed without their assistance. This work was supported in part by TASER International, Inc., who contributed personnel for assistance and product for use.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
Dr. Ho serves as the medical director to TASER International, Inc., and Dr. Dawes serves as a medical consultant to TASER International, Inc. Both own shares of stock in the company. No other authors have a conflict to disclose.