
Abstract
The inertial loading thresholds for infant head injury are of profound medico-legal and safety-engineering significance. Injurious experimentation with infants is impossible, and physical and computational biomechanical modelling has been frustrated by a paucity of paediatric biomechanical data. This study describes the development of a computational infant model (MD Adams®) by combining radiological, kinematic, mechanical modelling and literature-based data. Previous studies have suggested the neck as critical in determining inertial head loading. The biomechanical effects of varying neck stiffness parameters during simulated shakes were investigated, measuring peak translational and rotational accelerations and rotational velocities at the vertex. A neck quasi-static stiffness of 0.6 Nm/deg and lowest rate-dependent stiffness predisposed the model infant head to the highest accelerations. Plotted against scaled infant injury tolerance curves, simulations produced head accelerations commensurate with those produced during simulated physical model shaking reported in the literature. The model provides a computational platform for the exploitation of improvements in head biofidelity for investigating a wider range of injurious scenarios.
Introduction
Traumatic injuries to infants can occur frequently due to infants’ lack of coordination, underdeveloped anatomy and structural vulnerability to accident and abuse. It has been approximated that each year, 19 million children worldwide experience trauma severe enough to warrant medical treatment. 1 Traumatic head injuries can be the result of large accelerations of the infant head, causing critical intracranial injuries, including cerebral haemorrhages, oedemas and diffuse axonal injuries.
Studies recording the occurrence of non-accidental head injury (NAHI) estimate the annual incidence to be 24.6 per 100,000 infants in those younger than one year old. 2 Identified NAHIs have high mortality rates of approximately 20%, with approximately 60% of cases sustaining ongoing neurological deficit; continuous medical care is required in more than 80% of cases. 3 These numbers, however, are regarded by both studies to be just the ‘tip of the iceberg’ because of both identification failures and cases not brought to medical attention.
Many age-specific developmental differences exist between infants and adults that particularly predispose an infant to injury. Burdi et al. stated that infants should ‘not just be assumed to be scaled down, miniature, adults’. 4 The infant head is both proportionally larger and heavier than that of an adult; its circumference increases by up to 25% during the first six months of life, resulting in significant demands on the infant to provide head control when the neck musculature is weak 5 and the vertebral articular facets shallow. 6
The weaker musculature of the infant neck potentially predisposes the infant head–neck complex to ‘whiplash’ effects at relatively lower torso accelerations. This may increase the likelihood of large and possibly fatal accelerations being applied to the infant head during otherwise non-injurious inertial loading scenarios. The biomechanical properties of the infant neck are defined using relationships that describe both the quasi-static and rate-dependent stiffness properties of the neck. Pintar et al. used caprine surrogate models to estimate quasi-static cervical joint stiffness in infants for lateral bending, flexion–extension and tension. 7 Nuckley and Ching investigated baboon surrogates to estimate compressive and tensile cervical joint quasi-static stiffness properties across human equivalent ages ranging from 1 to 26 years. 8 Rate-dependent stiffness properties of the cervical joints have also been investigated for compression 9 and tension 10 using baboon surrogates with average human equivalent ages of 9 and 10 years respectively.
The infant head has larger extracerebral spaces, greater laxity of the meninges and inertial differences between grey and white brain matter, potentially increasing its susceptibility to brain injury from rotational accelerations. 5 This is believed to contribute to the shearing of bridging veins between the meninges and brain, and the irreparable damage to axons. Injury criteria, therefore, focus mainly upon the levels of rotational acceleration and rotational velocity applied to the head. Injury tolerance limits, which originate from adult baboon studies, have been scaled to represent injury limits for a one-month-old infant, which establish tolerance limits for rotational accelerations and rotational velocities associated with the production of subdural haemorrhages and cerebral concussion. 11
Although there are many variables that potentially influence the biomechanics of a traumatic inertial loading scenario, this study attempts to develop a computational model of an infant, paying particular attention to the development of the neck. This is considered to be the principal and key biomechanical determinant of head kinematics.11–13
Several infant-specific mechanical and computational models have been developed in an attempt to simulate the biomechanics of human-induced shaking of an infant. A range of mechanical anthropomorphic test device (ATD) studies have been conducted, which have shown that during shaking, adults are unable to achieve the predicted injury thresholds currently attributed to the production of subdural haemorrhages (SDH).11–14 Utilising a wide range of neck, head and chest designs and shake patterns, study participants have been required to shake an ATD vigorously. Resulting thoracic shake frequencies have ranged between 2.5 and 5 Hz across all studies, producing maximum translational head accelerations, rotational head accelerations and rotational head velocities of 1737 m/s2, 10216 rad/s2 and 61 rad/s respectively.11–13 Although only Cory and Jones 11 reported rotational head accelerations in excess of predicted injury thresholds for concussion, no study has to date demonstrated that shaking alone, without an associated impact, exceeds the injury thresholds associated with SDH.
Infant-specific computational models have also been developed to examine parametrically the effects of neck stiffness and head-to-torso impacts on the biomechanics of a vigorous shake. Woolfson et al. 13 developed a rigid-body model of a one-year-old infant, varying the stiffness properties of a simplified infant neck, to establish the effects of these properties on the rotational head accelerations and velocities generated during simulated shaking. To simulate the kinematics of a vigorous shake, a linear acceleration of 10 g was applied to the torso of the computational model. The majority of the results was found to be clustered below all predicted infant-specific injury thresholds (rotational head accelerations of ∼1000 rad/s2 and rotational head velocities of ∼20 rad/s). However, if head-to-torso impacts (or end-stop joint stiffness characteristics) were simulated, rotational head accelerations and velocities were observed to exceed predicted injury thresholds for concussion. Bondy et al. 15 developed a rigid-body model of a newborn infant, modelling the neck and cervical spine as a seven-segment model. Vigorous shakes were simulated using a linear acceleration of 8 g applied to the torso of the computational model. By varying the joint stiffness characteristics of the model, the shake frequency and the magnitude, this study was able to simulate rotational head accelerations of 14,111–24,832 rad/s2 and rotational head velocities of 37.46–44.9 rad/s. All simulations were observed to exceed predicted concussion injury thresholds. However, no neck stiffness or shake characteristics combination exceeded the predicted injury thresholds for SDHs.
To investigate the effects of varying the quasi-static and rate-dependent neck stiffness properties on the peak translational accelerations of the vertex, a computational infant model (MD Adams®) was developed, and simulations were conducted across a range of neck stiffness combinations. Rotational accelerations and velocities recorded during these simulations were then plotted against existing injury criteria to evaluate the potential for injury.
Methods
Infant model development
This study describes the development of a computational infant model (MD Adams®; MSC Software Corp., Newport Beach, CA) by combining radiological, kinematic, mechanical modelling and literature-based data. Whilst the focus of this study was the investigation of the biomechanics of the cervical spine, head and thorax, the model was developed with a greater degree of complexity, such that further investigations of potentially injurious scenarios could be performed.
Model construction
Serial sagittal magnetic resonance images (MRIs) from two infant subjects, aged 2 weeks and four months, were obtained with Cardiff School of Engineering Research Ethics Committee approval. Detailed dimensions for the anatomical features of the head were extracted from both images and scaled to represent a nine-month-old infant male using age-specific gross head dimensions obtained from the literature.16,17 Finally, these dimensions were averaged to provide a detailed three-dimensional (3D) solid body model of the head that represented a 50th percentile nine-month-old infant male.
Normalised and scaled 3D solid body limb models for a 50th percentile nine-month-old infant male were dimensioned and rendered from the existing literature18–20 and supplemented, where necessary, by scaled measurements from an eight-month-old female subject (unpublished data obtained with Cardiff School of Engineering Research Ethics Committee approval). The limbs were constructed as lofted solids within Solidworks 2009 (Dassault Systèmes SolidWorks Corp., Waltham, MA) and imported into the MD Adams® modelling environment (see Figure 1).
An Adams model of a 50th percentile nine-month-old infant male, showing the simplified computational model of the cervical spine.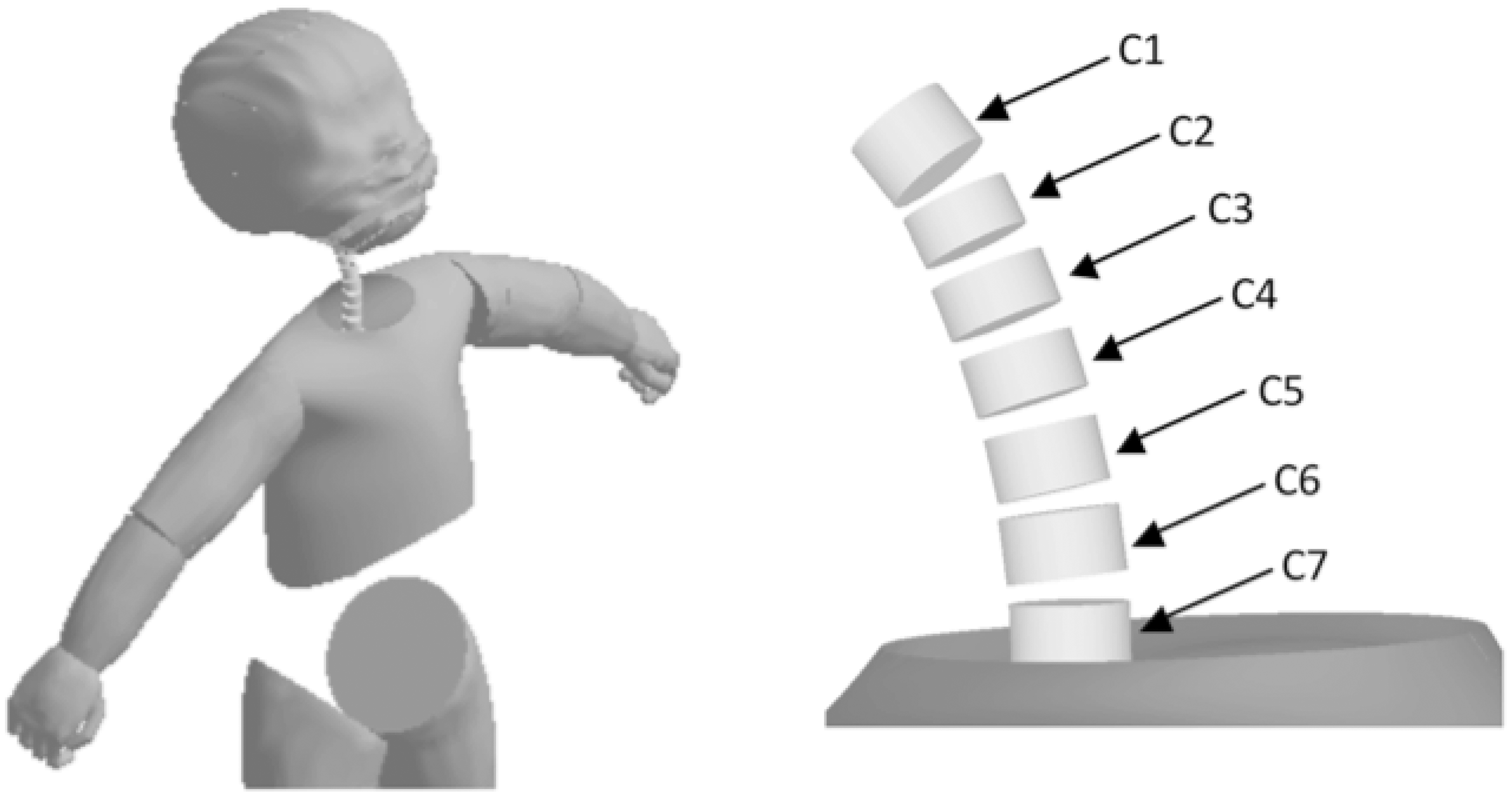
The infant spine (C0–L5) consisted of a vertically aligned collinear column of 24 cylindrical bodies and 24 joints, with vertebral centre of mass (COM) and joint centre locations. For the purpose of this study, only C0–C7 will be discussed. Vertebral body heights and intervertebral spaces were dimensioned based on scaled data obtained from the MRIs, with vertebral masses and COMs calculated by the Adams software. The head was assigned an age-appropriate mass of 2.3 kg with a COM 14.5 mm anterior and 33.5 mm superior to the C0 joint, in the sagittal plane. 17 The head, torso and spinal rigid body models were located based upon data derived from the MRI of the four month old lying in a supine position. To simplify their interaction, the head and torso were attached to the spine by fixed joints at C0 and C7 respectively.
Spherical joints attached the limbs to the body, with appropriate masses and COM locations assigned to each limb. 21 Contact between the chin and chest, during shaking, was approximated using a mass–spring–damper contact function. 10
Cervical spine joints (C0–C7) were restricted to a single rotational degree of freedom (flexion–extension), whilst the remaining joints were fixed to simplify thoracic and lumbar spinal kinematics for this study. Linear relationships were developed for the quasi-static and rate-dependent vertebral stiffness properties, in flexion–extension, across all cervical joints (T = −Kθ − Cω). Quasi-static stiffness (K) acted against the angular displacement of the joint, away from vertical (θ), whilst the rate-dependent stiffness (C) acted against the rate of angular displacement (ω).
A representative range of linear approximations for the quasi-static (0.1–1.0 Nm/deg) and rate-dependent (5–15 Nmm/s/deg) flexion–extension stiffness properties were selected for investigation. The range of quasi-static flexion–extension stiffness properties approximated neck stiffness up to the age of six years, with a quasi-static stiffness of 0.242 Nm/deg representing that of a nine-month-old infant. 22 Rate-dependent flexion–extension stiffness properties of the cervical vertebrae, however, have not been assessed by human or animal surrogate studies. Therefore, to define an appropriate rate-dependent stiffness range, a preliminary study identified that a rate-dependent stiffness range of 5–15 Nmm/s/deg resulted in model simulations that conformed to a physiological range of motion. 23
Chin-to-chest contact function
Percentage errors between experimental and simulated head drop tests using the optimised stiffness and damping constants.

Model assessment
The biofidelity and subsequent accuracy of the computational model was assessed against paediatric motion analysis data (Qualisys, Göteborg, Sweden). Three-dimensional data were collected from one female infant at regular three-month intervals, between 3 and 18 months, with Cardiff School of Engineering Research Ethics Committee approval.
22
Retro-reflective markers were located on the vertex, spine, hip and shoulder of the subject to enable the quantification of motion (Figure 2). The tests at nine months of age included very gentle oscillations (shakes), as approved by Cardiff University School of Engineering Research Ethics Committee, at an approximate frequency of 1 Hz and amplitude of 65 mm, recording the relative motion of the vertex to the T1 vertebrae (Figure 3).
Example motion capture image observed at age three months. Gentle oscillation of a nine-month infant at a frequency of 1 Hz and amplitude of 0.065 m.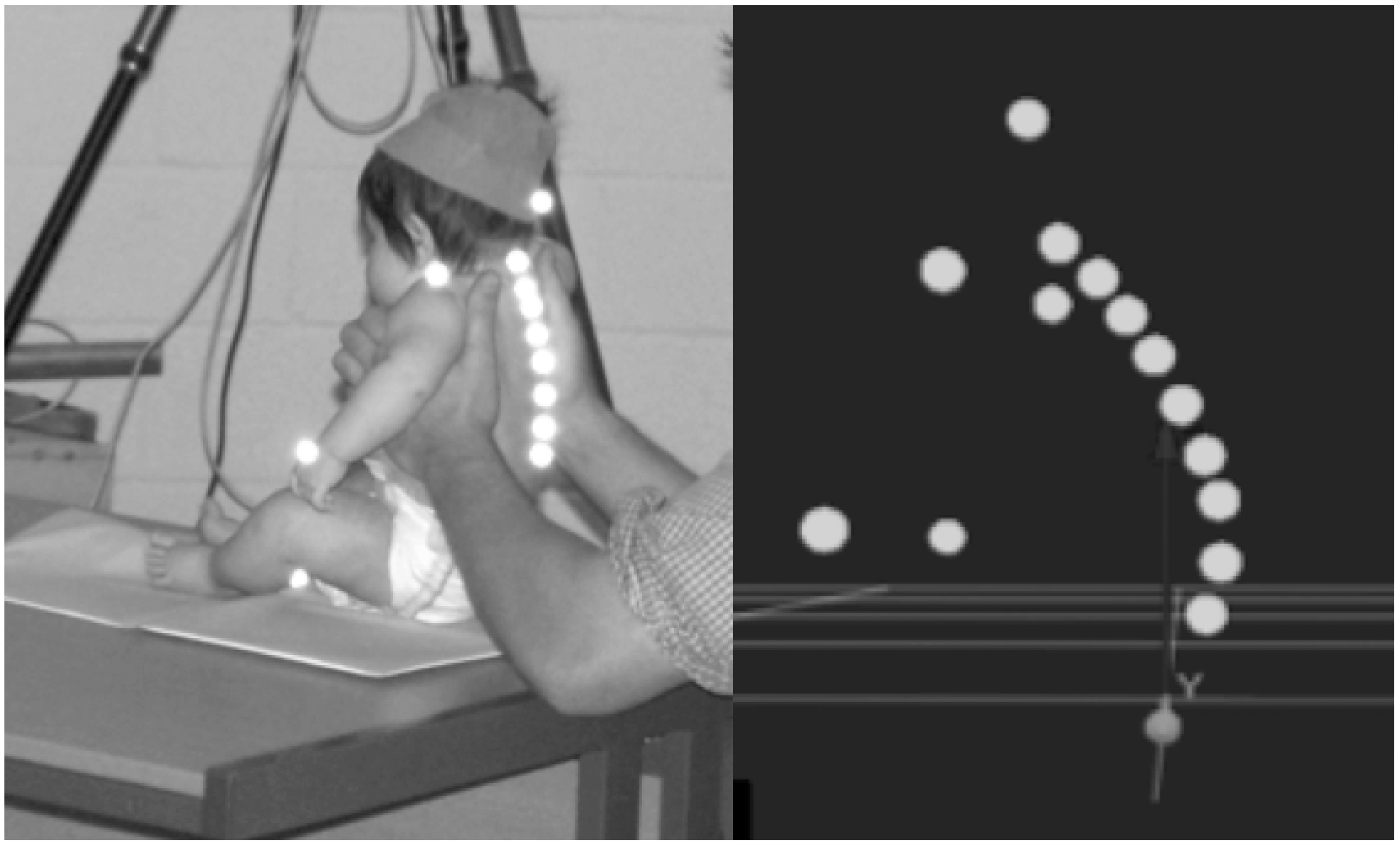

A computational simulation of the gentle oscillation was generated to assess the suitability of the biomechanical properties of the cervical spine. Torso motion for the computational simulation of this gentle oscillation was extracted from the experimental data defining the motion of the T1 marker. Quasi-static stiffness constants of 0.242 Nm/deg were assigned simultaneously across the cervical joints, whilst rate-dependent stiffness varied between 5–15 Nmm/s/deg. The global position of analogous vertex and T1 markers were recorded during these simulations to quantify the range of displacement of the head relative to the thorax. The percentage errors between simulated and experimental data, which described the range of displacement of the head relative to the thorax in the sagittal plane, were then calculated.
Iterative testing of stiffness properties was then performed at 1 Nm/deg intervals, seeking convergence of relative computational versus experimental percentage errors, to validate the model. This was achieved at cervical spine stiffness properties of 0.242 Nm/deg and 12.242 Nmm/s/deg for the quasi-static and rate-dependent flexion–extension stiffness properties respectively. This combination minimised percentage errors to <1%.
Simulation methodology
All simulations were performed using the Gear Stiff (GStiff) integrator and index 3 formulation. Relative and absolute local integration error tolerances were 1 × 10−6 mm and the maximum time step (Hmax) was 1 × 10−3 seconds. All results were sampled at a rate of 5000 Hz.
Cervical spine stiffness combinations were created from both quasi-static and rate-dependent stiffness constants and applied simultaneously to all cervical joints for all simulations. A total of 240 combinations were created from quasi-static stiffness constants that ranged between 0.1 and 1.0 Nm/deg in 0.05 Nm/deg increments. The rate-dependent stiffness constants ranged between 5 and 15 Nmm/s/deg in 1.25 Nmm/s/deg increments. A sinusoidal, uniaxial and anterior–posterior shake was applied to the infant torso at a frequency of 3 Hz and amplitude of 65 mm, corresponding to a ‘severe shake’, as categorised in the study by Cory and Jones. 11
The outcomes recorded for this simulation were peak translational accelerations, rotational accelerations and rotational velocities of the vertex for all neck stiffness combinations. This was also repeated for the approximated neck stiffness combination (K: 0.242 Nm/deg; C: 12.242 Nmm/s/deg).
Scaled cervical spine vertebral joint range of motion.

Results
The first simulation was recorded using the spinal stiffness properties successfully obtained from the experimental data (Figure 4). The peak translational accelerations, rotational accelerations and rotational velocities of the vertex recorded during this simulation were 95.73 m/s2 (9.76 g), 1133 rad/s2 and 17.17 rad/s respectively.
Example screen shots from a simulation run.
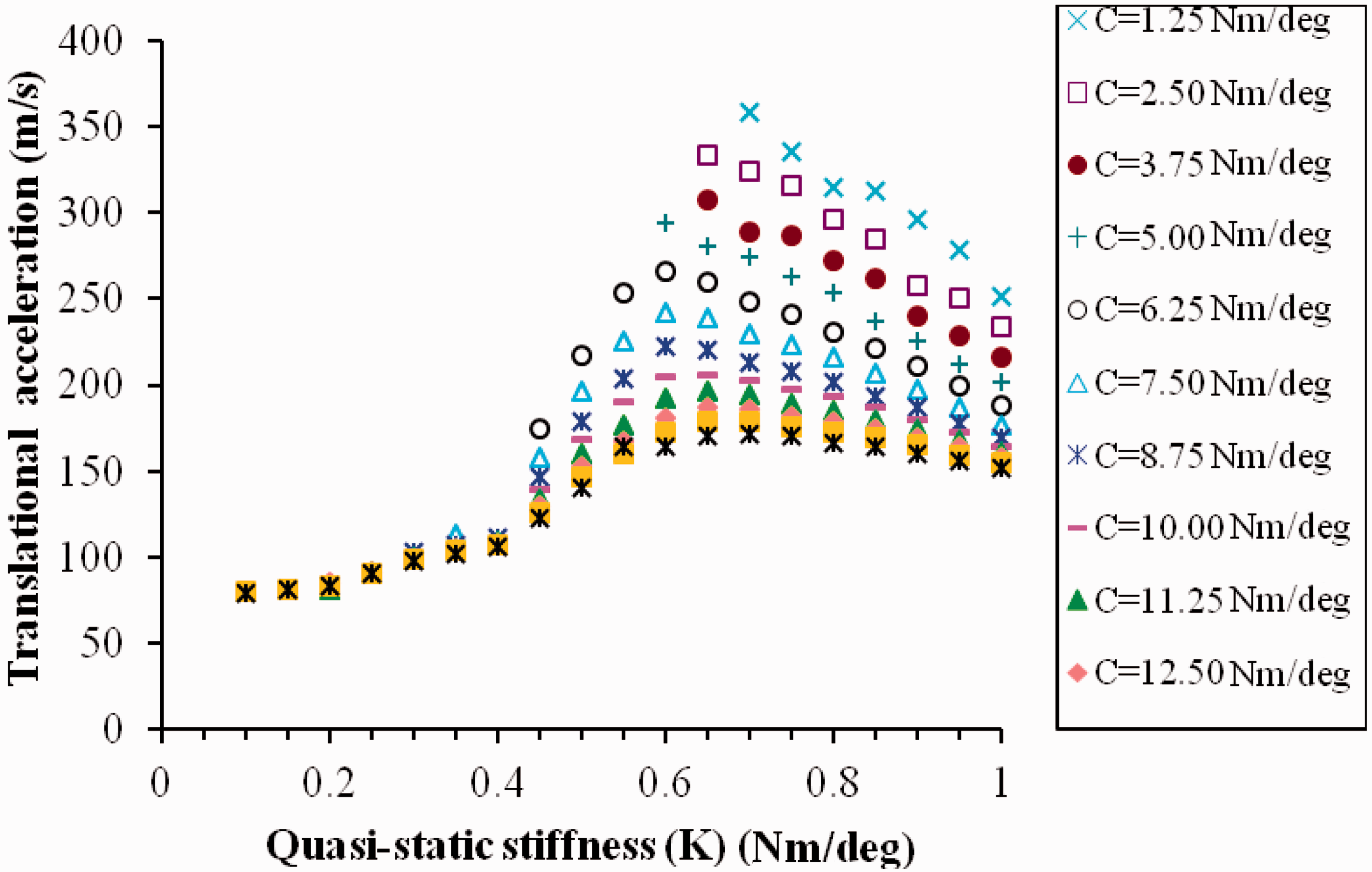
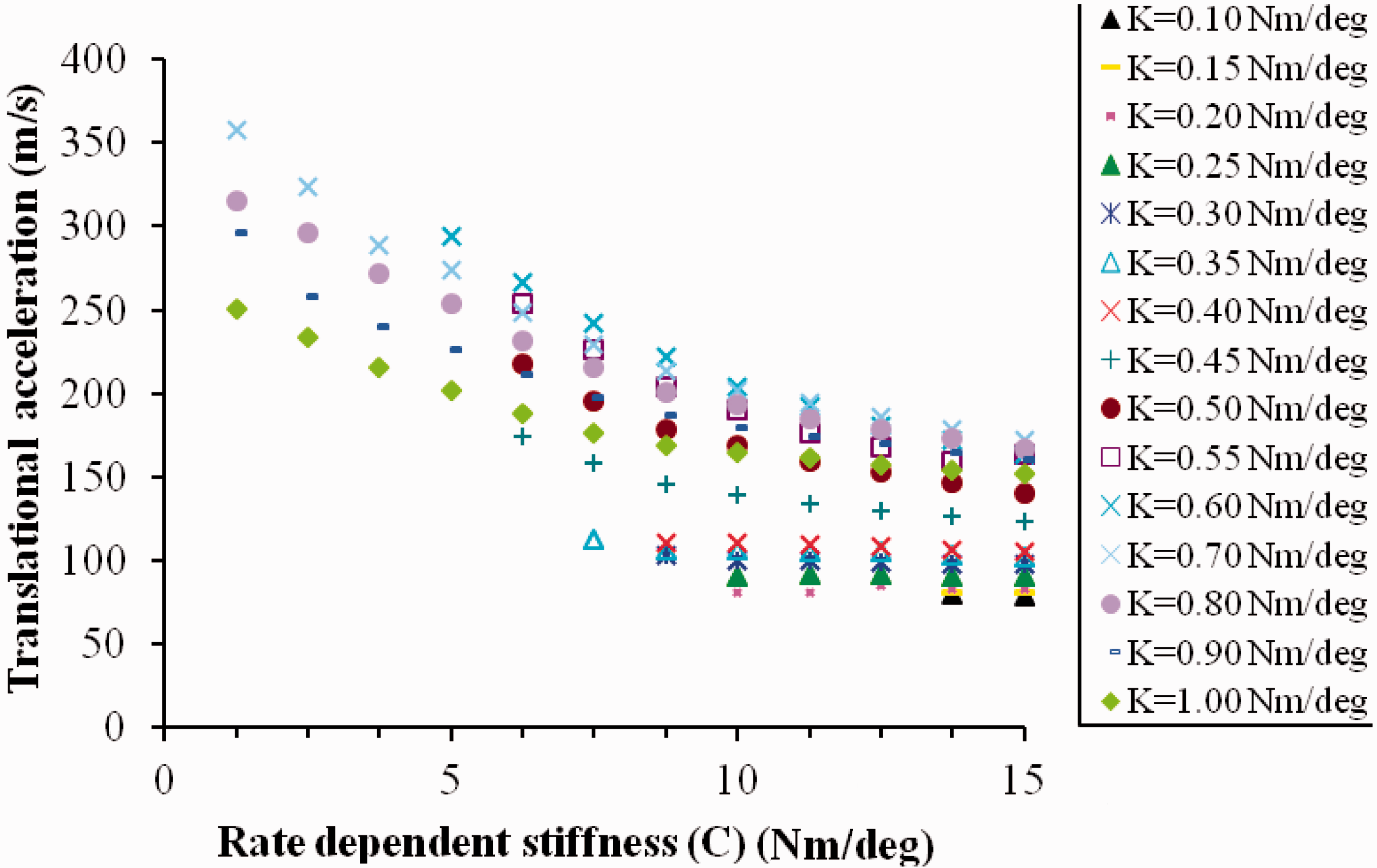
The relationship between peak vertex translational accelerations and the neck stiffness properties is shown in Figure 5(a) and (b). The neck stiffness properties can be observed to demonstrate a highly non-linear relationship with the simulated peak translational accelerations of the vertex. A decrease in the rate-dependent stiffness constant leads to an increase in peak acceleration, with peak accelerations maximised at a quasi-static stiffness value of approximately 0.6 Nm/deg. Peak rotational accelerations are plotted against peak rotational velocities (Figure 6) for all stiffness combinations. It can be observed that all simulations across all neck stiffness combinations did not exceed the scaled injury tolerance levels for a one-month-old child.
11
(a) Relationship between peak vertex translational accelerations and the quasi-static (K) vertebral flexion–extension stiffness properties, across the range of rate-dependent stiffness (C). (b) Relationship between peak vertex translational accelerations and the rate-dependent (C) vertebral flexion–extension stiffness properties, across the range of quasi-static stiffness (K). Rotational accelerations and velocities across all simulations ×, showing the scaled injury tolerance levels for a one month old
11
: ___, 50% concussion likelihood tolerance level (Ommaya
33
in Klinich et al.
33
); - - -, cerebral concussion tolerance level (Duhaime et al.
12
); - . -. -, cerebral concussion tolerance level (Thibault and Margulies
34
);………, subdural haematoma tolerance level (Duhaime et al.
12
).
Simulation failures were recorded primarily at low quasi-static and rate-dependent stiffness properties. In total, 78/240 (32.5%) neck stiffness simulation combinations produced unrepresentative joint motion and hence were classified as simulation failures.
Discussion
Peak head accelerations have previously been investigated using both mechanical and computational models to demonstrate the peak accelerations generated in the head by each neck stiffness combination.11–13,15,30,31 Using appropriate neck stiffness properties validated for a nine-month-old infant, this study was able to estimate the translational vertex accelerations of 9.76 g from simulating inertial loading of the head and neck by subjecting the torso to accelerations derived from abusive shaking scenarios with crude mechanical dummies. 11 This was directly comparable to the mechanical model studies performed by Duhaime et al. 12 which generated mean peak head accelerations of 9.29 g. Shaking frequencies also corresponded with the studies by Cory and Jones, 11 Woolfson et al., 13 Lloyd et al. 15 and Bondy et al. 16
The peak translational accelerations of the vertex generated during the simulated traumatic shakes were found to increase sevenfold across all neck stiffness combinations. It was established that a quasi-static stiffness value of approximately 0.6 Nm/deg, combined with a low rate-dependent stiffness, maximised the peak translational accelerations of the vertex for a nine-month-old infant. To establish the theoretical extent of trauma caused during simulation, however, rotational accelerations and velocities of the head were also recorded. These were compared to a number of existing injury tolerance levels (Figure 6), where it can be observed that all simulations did not exceed any injury tolerance level.11,12,32–34
The results from this study highlight the complexities involved in fully analysing shake biomechanics, with both stiffness properties found to be important in determining the outcomes of traumatic shakes. Once further and more complete biomechanical data are published about the immature spine and shake characteristics, the model can be used to estimate more accurately the levels of head acceleration experienced by a nine-month-old infant during an abusive shaking scenario.
Model and simulation limitations
The model developed in this study corresponded to a nine-month-old, 50th percentile male and provided a computational platform to perform representative simulations of applied traumatic shakes. Due to the current paucity of age-associated paediatric data, however, several assumptions and simplifications were made that currently limit model biofidelity.
Contact functions were based upon experimental data from the occipital bones of three infant cadavers aged 3, 5 and 11 days, as these were the only age-specific data that defined infant head contact parameters. 13 Contact function values were adopted and kept constant throughout, with a force exponent of 1 selected to ensure a linear stiffness and a penetration depth of 5 mm selected to represent the thickness of the skin. Obvious limitations exist, since, in a more developed nine month old, the cranial bones and mandible bones are different in shape, portion of diploe and mechanical strength. Also, the thickness of flesh tissue are different between the occipital bone and the chin. Head and torso dimensions were scaled from the MRIs of two infant subjects, with masses and centres of mass extracted from scaled adult data for the Child Restraint Air Bag Interaction (CRABI) dummy. Vertebrae, vertebral joints and vertebral centres of mass were modelled collinearly to simplify the spinal biomechanics and therefore did not characterise the natural curvature of the infant spine. Vertebral mass and COM properties were assigned Adams default values, whilst uniform growth was assumed when scaling vertebral dimensions. Cervical joints were limited to a single degree of freedom in flexion–extension, with the remaining vertebral joints fixed. The use of linear quasi-static and rate-dependent stiffness relationships simplified the use of joint-specific and non-linear relationships for both stiffness functions. Stiffness property ranges were selected to represent values found in the current literature 7 or were approximated based upon experimental data from non-traumatic oscillations of an infant subject. Perhaps the most important limiting factor was the use of uniaxial, anteroposterior and sinusoidal shake patterns, as it has been shown that the effects of coupled shake patterns can increase the levels of acceleration achieved. 11 Further development will include the shake patterns derived from the Cory and Jones study. 11
It is noteworthy that the injury tolerance curves quoted in this study may provide a limitation, since they are largely based upon the scaling of data from animal testing to the adult and further to the infant, and may not accurately represent specific infant injury tolerance curves. Further discussion can be found in Cory and Jones. 11
To develop the model further, it is important to gather a greater range of paediatric data to improve model biofidelity. Remodelling a curved spine that characterises vertebral parameters such as mass, inertia and non-linear joint stiffness properties is under way and will allow for more accurate simulation of joint motion. Accurate modelling of the infant head and torso will require age-specific anthropometry and mass distribution data, whilst further experimental data are necessary to define the chin-to-chest contact and possibly occipital to upper back properties. Development of six degrees of freedom vertebral joints in the spine will allow the investigation of applied shakes with coupled motion. Non-linear quasi-static and rate-dependent vertebral stiffness properties are also required for all six degrees of freedom of the cervical spine, whilst the differences in stiffness between each joint and for each degree of freedom must also be modelled. Further, the biomechanical effects of neck length and musculature should also be investigated.
All simulation failures occurred when joint angles extended beyond their biofidelic boundaries. The main failure mechanism was a result of unrestrained neck motion in extension. Though neck motion was limited by chin-to-chest contact in flexion, it remained unconstrained in extension. It is hypothesised that a limit is provided by the occipital-to-torso contact. 12 Yet, biofidelic neck extension boundary conditions were exceeded in all failures before occipital-to-torso contact was recorded. It may therefore be that the hard tissue of the cervical vertebrae and musculo-ligamentous structures of the neck primarily limits extension. This may result in greater head accelerations during the extension phase of the cervical spine. Simulation failures may therefore be reduced by developing the model further to include both occipital and vertebral contact functions.
Conclusions
This study has presented the developmental framework for a validated computational model of a nine-month-old infant for the simulation of inertial loading scenarios. The importance of neck stiffness properties in shaking scenarios was demonstrated, with both quasi-static and rate-dependent stiffness properties influencing peak vertex accelerations. The results from this study suggest that in uniaxial shaking alone, infant head accelerations generated during inertial loading of the computational model compare with those generated during physical model studies. The model provides a computational platform for the exploitation of improvements in head biofidelity for investigating a wider range of injurious scenarios.
Footnotes
Acknowledgements
The authors would like to acknowledge the contributions of the Cardiff University School of Engineering ‘Babysafe’ project groups 2007–2009.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.