
Abstract
The Maxwell Centre, a health-based place of safety (POS) adjacent to a psychiatric hospital, was opened in Gloucestershire in February 2009. It provides a POS for people detained under Sections 135 and 136 of the Mental Health Act 1983 as amended in 2007. Prior to the opening of the Maxwell Centre, police cells were the only designated POSs. To assess the impact of the opening of this new facility, we undertook a service evaluation. In the five years (February 2009 to December 2013) following the opening of the Maxwell Centre, the use of Section 136 increased by more than 60%.
Introduction
In England and Wales, Section 135 (S135) of the Mental Health Act 1983, as amended in 2007 (MHA 2007), allows a magistrate to issue a warrant authorising a police constable to enter premises, using force if necessary, for the purpose of removing a mentally disordered person to a place of safety (POS). This can be done under the following circumstances: when an Approved Mental Health Professional (AMHP) has reasonable cause to suspect that a person who is believed to be suffering from mental disorder has been, or is being, ill-treated, neglected or not kept under proper control, or that they are not able to care for themselves or are living alone in such a place.
Similarly, Section 136 (S136) of the MHA 2007 gives a police constable the power to detain an individual that they are found to be mentally disordered in a public place and in need of care and control, and then to remove that person to a POS.
Once in the POS, S135 and S136 detainees can then be assessed by a medical practitioner and an AMHP with a view to whether admission to hospital is warranted either voluntarily or compulsorily.
The Maxwell Centre, a health-based POS for people detained under S136 and S135 in Gloucestershire. was opened in February 2009. 1 Whilst located on the site of a psychiatric hospital, it is separate from the inpatient facility and staffed by nurses and other staff from the County’s Crisis Resolution and Home Treatment Teams (CRHTTs). Separating the unit from inpatient wards is consistent with Churchill et al., 2 who suggested that a police station or hospital should not be considered a POS, but rather that the POS should be clearly designated, dissociated from formal inpatient facilities, more relaxed but also able to provide security and multidisciplinary assessment, and be within easy access of medical facilities.
To assess the impact of the opening of the Maxwell Centre, we undertook a service evaluation.
Methods
We analysed anonymised data collected routinely for the purposes of inter-agency monitoring of the use of S136 in Gloucestershire, as required by the Code of Practice. 3 These anonymised data included: (1) demographic details of the detainees such as age, gender and ethnicity; (2) details of S136 detention such as time of detention, duration of detention and time in the Maxwell Centre; and (3) outcome of S136 assessment such as admission or referral on for assistance or treatment in the community.
We were able to compare the data described above with local S136 data from before the Maxwell Centre opened when police cells were the only POS available4,5 and also some data from national sources.6,7 Limited data on S136 detentions in the cells were also available from the police.
Results
Section 136 (S136) detentions in Gloucestershire February 2009–December 2013.

11 months’ data.
11 months’ data for this figure (49).
11 months’ data (missing January).
POS, place of safety.
The Maxwell Centre alone dealt with 1290 detainees, the cells alone with 253. However, a further 275 detainees spent time in both POSs, being transferred between them during their period of detention. Thus, the total number of detainees passing through the Maxwell Centre was 1565, and the total passing through the cells was 528.
Unless otherwise stated, the following results apply to the 1565 detainees passing through the Maxwell Centre. Of these, 55.3% were male ranging in age from younger than 16 years to older than 65 years. The most frequent age band was 35–44 years of age, with 21.1% of detainees falling into this category. The majority of detainees (62.2%) were aged between 25 and 54 years. Only a minority was at the extremes of age, 6.3% being younger than 18 years (with 1.3% younger than 16 years) and 3.4% being older than 65 years.
Ethnicity, when compared to census data from 2011, 8 showed marginal overrepresentation of black/African/Caribbean/black British groups (1.7% vs. 0.9%) and mixed/multiple ethic groups (1.7% vs. 1.5%). In contrast, there was some underrepresentation in white groups (91.1% vs. 95.4%) and Asian/Asian British (1% vs. 2.1%).
Time of S136 detention and outcomes after assessment at the Maxwell Centre February 2009–December 2013 (59 months).
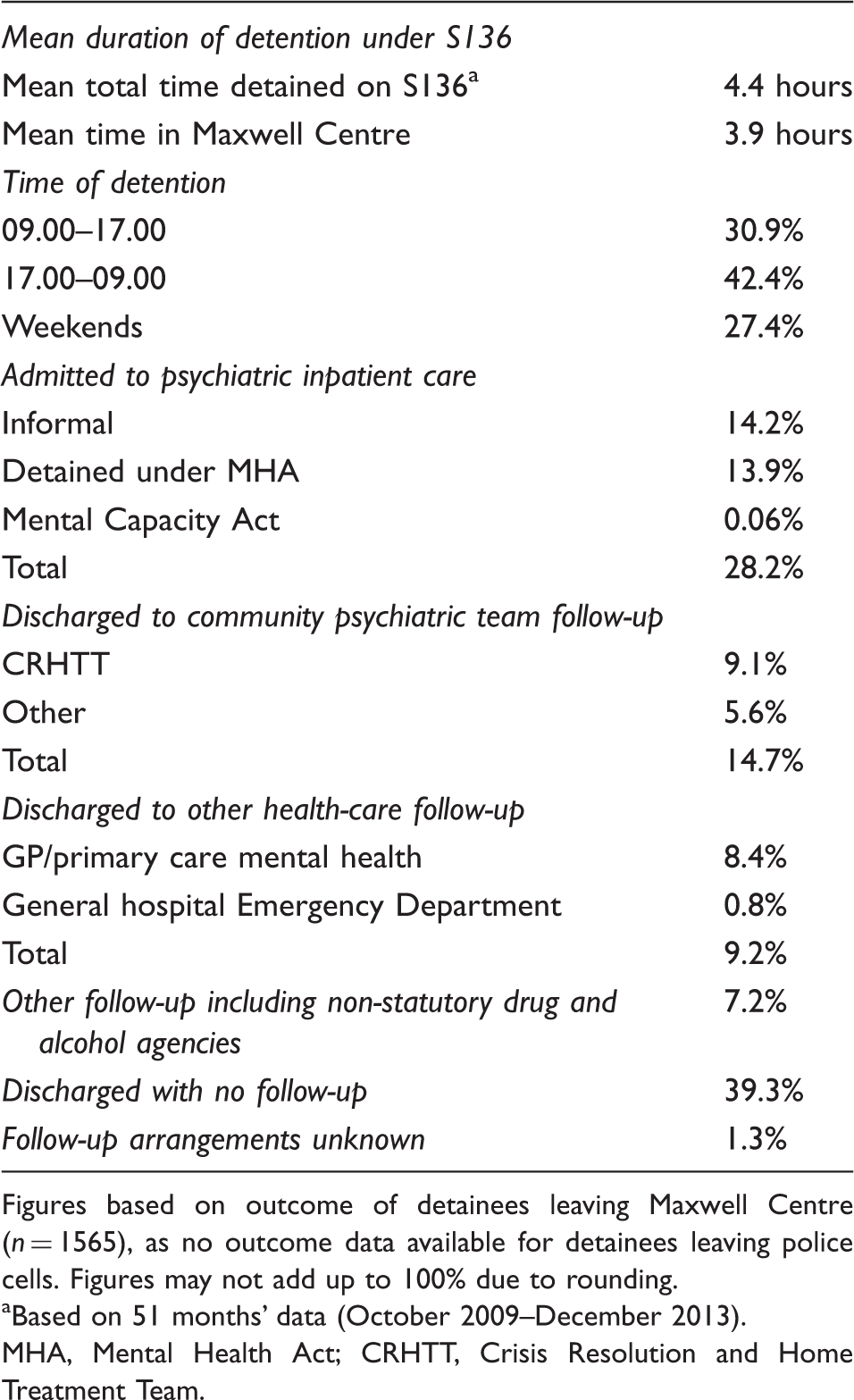
Figures based on outcome of detainees leaving Maxwell Centre (n = 1565), as no outcome data available for detainees leaving police cells. Figures may not add up to 100% due to rounding.
Based on 51 months’ data (October 2009–December 2013).
MHA, Mental Health Act; CRHTT, Crisis Resolution and Home Treatment Team.
Following assessment, 28.2% of detainees were admitted. Of the rest, 14.7% are discharged to follow-up from specialist community psychiatric teams, with 9.2% referred on to other health services – mainly primary care. Follow-up from non-statutory services was offered to 7.2%, and 39.3% were offered no specific follow-up.
Discussion
For an up-to-date review of the literature on S136 and national data, the reader is directed to articles by Borschmann 9 and Keown. 10 The Royal College of Psychiatrists has also recently published guidance for commissioners. 11
Rate of detention and POS
Comparing the mean number of S136 detentions for 2004–2008 (15.9 per month) against the mean for 2009–2013 (30.8 per month) shows that the use of S136 in Gloucestershire has increased by more than 60% following the opening of the Maxwell Centre in February 2009, and more than 100% in the period from 2008 to 2011 (Figure 1).
Section 136 (S136) detentions per year in Gloucestershire 2004–2013.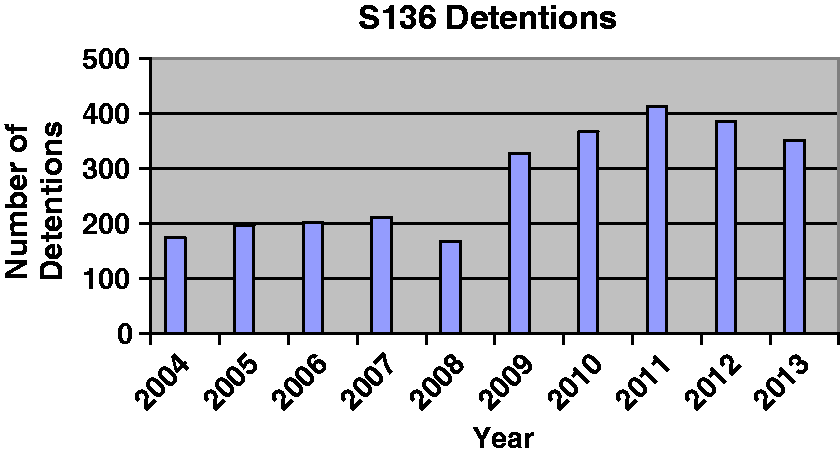
This increased use of S136 locally is in keeping with national trends in England, where hospital based POSs have been used more frequently in recent years.7,10 However, our data show a dip in 2008, rather than the year-on-year increase found in the national data which shows that POS Orders (S135 and S136) have more than doubled from 2007–2008 to 2011–2012. Nationally, the total number of such orders in 2011–2012 was 15,240, representing a 6% increase on the previous year.
A number of factors may be associated with the increased use of S136 in Gloucestershire. It may be that the local increase is simply a reflection of national trends of increased use of the MHA 2007 generally and S136 in particular. The reasons behind these national trends may include the broader definition of mental disorder within the revised MHA 2007 which, arguably, makes more people liable to detention. However, this would explain only recent increases, as the revisions to the Act were only introduced fully in 2009.
Social and political factors may also be relevant in that tolerance of odd or risky behaviour in public may be lower. Increased concerns about risk management amongst the police may also be relevant by way of an increased concern about risk and an increased willingness to use formal measures to manage situations that are perceived as worrying or unsafe. Generally, the CRHTT are unable to respond quickly enough to provide an alternative to a S136 solution.
From a local perspective, however, the increased use of S136 in Gloucestershire is closely associated with the opening of the Maxwell Centre. This suggests an increased willingness amongst police officers to use S136 powers when an alternative POS to the cells is available. This position has been strongly reinforced by the National Police Improvement Agency (NPIA) Guidance 12 and the 2012 announcement by the Home Secretary (Theresa May) on 16 May 2014 to the Police Federation Conference that police cells should no longer be used for people with mental health needs.
An increase in the use of S136 occurred in Trafford, Manchester, following the opening of their health-based POS in 2008. They report a reduction in the rate of use of S136 following the initial surge after the opening of the unit.
13
We have also seen a slight reduction over time (see Figures 1 and 2).
S136 detentions per year in Gloucestershire 2009–2013 by place of safety (POS) and including transfers.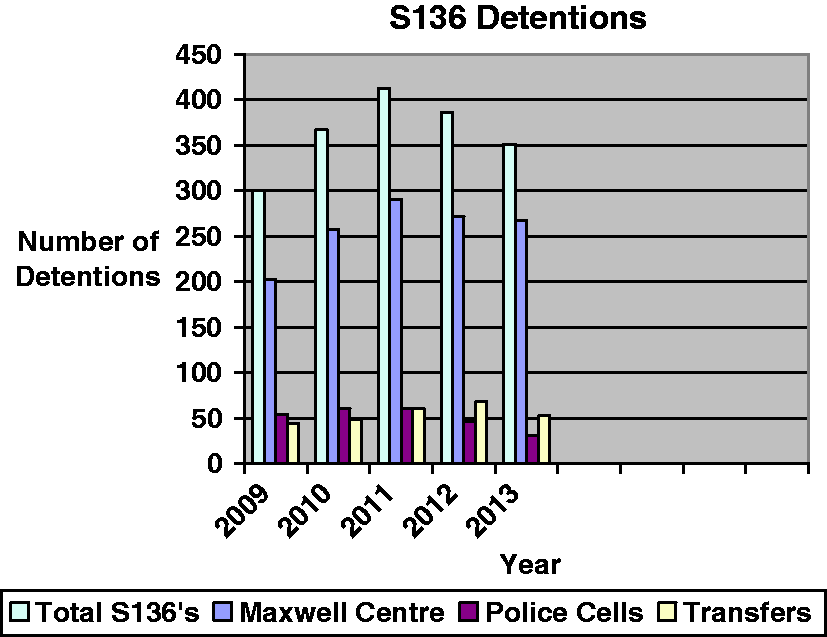
Now, for the first time, the national figures 7 have included an estimate of the use of S136 in police cells by analysing local custody suite databases. This suggests a figure of 8667 for 2011–2012, which represents 37% of all S136 detentions in that year. This percentage is slightly higher than our own figures where 30% (528 out of 1818) of S136 detentions passed through the cells. In Gloucestershire, there has been an ongoing reduction in the percentage use of police cells as the sole POS from 18% in 2009 to 9% in 2013 (note only 11 months’ data for 2013).
The Code of Practice 3 states that police cells should only be used as a POS on an ‘exceptional basis’ for S136. A previous IPCC study 7 compared police and NHS data, and showed that two thirds of S136 detainees were held in police cells, with only a third being taken to a hospital POS at that time. The national figure described above suggests that the national situation is changing and police cells are being used less frequently.
However, having two separate sources of national data (police and health) on S136 is problematic for monitoring and research purposes. This difficulty in obtaining reliable data on the use of S136 has been noted elsewhere. 14 Nevertheless, the development of combining police cell and health-based S136 POS data in national statistics is a positive one. A useful next step would be to develop a single recording system for S136 detention to overcome the difficulty of monitoring transfers between POSs, avoiding the possibility of double counting and better recording the outcomes after assessment.
The national figures 7 also show that the use of S135 is very small in comparison to S136, with only 338 detentions recorded, representing only 2% of all POS orders in 2011–2012. Only six S135s were recorded in our data, representing 0.4% of all POS orders during this period.
Transfers
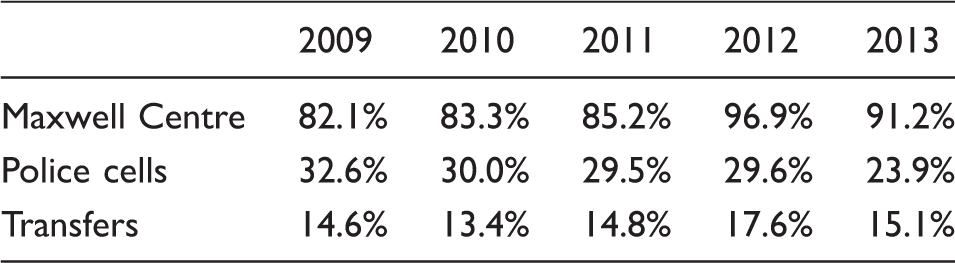
POS detentions and transfers.
Our local policy is that police cells are used as a POS for detainees who are too intoxicated to be assessed or who pose a risk of violence. The exact wording in the revised S136 policy endorsed by the local Inter-Agency Monitoring Group in July 2012 is that police cells will be used as follows:
Where the person concerned is unmanageably violent or where the arresting officer is concerned that the person may become violent. The overall consideration must always be the safety of everyone involved. No NHS POS is available (e.g. if the Maxwell Centre is full). Where the person concerned is under the influence of alcohol or drugs to the extent that they are not fit for assessment (this does not imply zero alcohol levels – see MHA Code of Practice 4.55) or detention and present a risk of harm to themselves or others that they cannot be managed safely at the Maxwell Suite.
The anecdotal evidence is that it is detainees who are no longer too intoxicated to be assessed and/or no longer pose a risk of violence who are transferred to the Maxwell Centre for assessment.
Demographics of detainees, time and duration of detention under S136
Our findings show the typical S136 detainee in Gloucestershire to be a male in the age range 35–44 years who is detained out of hours. His detention lasts a mean of 4.4 hours, 3.9 hours of which are spent in the Maxwell Centre. These findings are similar to previous data on local S136 detentions prior to the opening of the Maxwell Centre.
The vast majority of detainees are white British, in keeping with local census data. There was some slight overrepresentation of black/African/Caribbean/black British groups (1.7% vs. 0.9%) and mixed/multiple ethic groups (1.7% vs. 1.5%). This is different to other studies from large urban centres9,15 which have found more significant overrepresentation of Afro-Caribbeans.
Outcomes
As has been the practice for many years, the initial medical assessment at the Maxwell Centre is undertaken by an experienced Section 12 approved psychiatrist, either a consultant or a senior trainee. This contrasts with some other areas where much more junior doctors undertake the initial assessments.16,17
The outcomes of assessment in English hospital-based POSs in 2011–2012 were that 82% ended in an informal status (either released back to the community or admitted informally) and 18% were formally admitted to hospital. In 2007–2008, the comparable figures were 71% and 29%, showing that whilst the number of people detained under S136 continues to rise, the percentage that are then further detained is falling.7,10
Our local data show a lower use of further detention under the Act, with only 13.9% of detainees being admitted under Section into hospital. If the figures for admission, both formally and informally, are combined with detainees who were discharged to community mental health team follow-up, 42.9% of detainees were deemed to require either immediate or deferred intervention from specialist mental health services. The remainder – more than half of all detainees – did not require specialist mental health intervention.
On the one hand, therefore, S136 can be seen as an important safety net, allowing disadvantaged people to access mental health services in a time of crisis. However, local use of S136 raises important ethical issues about deprivation of liberty and appropriate use of scarce mental health resources given that only 13.9% of detainees required further detention under the Act and more than half did not require any specialist mental health follow-up.
The Code of Practice 3 requires services to collaborate and consider any changes that might lead to a reduction in the use of S136. Recommendation 6 of the Royal College of Psychiatrists Guidance for Commissioners recommends that multi-agency groups are set up to monitor S136 and ‘should consider how the need for the use of S136 might be reduced’. 11 This is also recommended in the Department of Health’s Mental Health Crisis Care Concordat (from 18.02.2014). 18 There would appear to be scope for this locally in the light of our findings.
Operational issues and views of staff
Finance for building the Maxwell Centre was received from Department of Health allocated funds, but this funding excluded staffing costs. 1 The role of staffing the Maxwell Centre was therefore allocated to the local CRHTT. Two CRHTT staff open the Maxwell Centre prior to the arrival of the detainee and remain in attendance until the assessment is completed. By using CRHTT staff in this way, we were unable to follow guidance 19 that diluting the functions of CRHTTs can have a negative impact on delivery of their core tasks. However, a positive outcome of this model is that staff from this team can be involved at an early stage and may sometimes help arrange an alternative approach other than detention under S136.
All detainees are subject to a physical health-screening checklist. If further assessment is indicated, this is provided by a private company that provides a more detailed screening, calling in a primary care physician if necessary. There were a variety of reasons for choosing this system, including quality control and the need to protect junior doctors’ time (the hospital’s junior doctor rota is only just compliant with the European Working Time Directive [EWTD], and it was not thought that this work could be added to their jobs without breaching EWTD rules).
Prior to opening the Maxwell Centre, we anticipated three possible problems, all of which presented at the interface with the police. These were disagreement around the degree of intoxication that is acceptable for admission to the Maxwell Centre and disagreement around responsibility for very intoxicated people, what to do with very aggressive patients, and how long the police should be required to stay. These issues are difficult to legislate for precisely and involve the judgement of the police and mental health staff: for example, in respect of intoxication, we decided to allow judgement on what constitutes intoxication, and not to rely solely on an alcoholmeter reading (which could not be enforced by the police in the absence of particular offences and is not designed for this context). If a patient is too intoxicated or violent, they are taken to the custody suite at the local police station or to the Emergency Department (ED) if their physical condition indicates the need for care and treatment.
Judgements by clinicians and by the police can differ. Our strategy for dealing with the problems was threefold: first, policies for the unit were developed jointly with the police and have recently been revised after a lengthy consultation process; second, we previously ran joint training with staff from the unit and the police, particularly targeting custody sergeants and AMHPs as key decision makers in the detention process; third, we put in place a system where differences of opinion in staff on the ground are rapidly referred upwards to a senior manager in the police and local Mental Health Trust. There are regular meetings to discuss and resolve any interface issues between police and health staff.
Estate, staffing and liaison
Separating the unit from the inpatient wards has had both costs and benefits. Using CRHTT staff for the POS has facilitated community disposals from the Maxwell Centre, as CRHTT staff are more familiar with community disposals and organising support in the community than are staff on the inpatient unit. However, the additional workload on the CRHTT has been significant and has impacted on their ability to perform core functions such as home treatment: opening the unit takes two members of staff away from a shift for up to four hours. Although extra staff resources were invested in the CRHTT, the demand from the S136 suite is ‘granular’, and it is difficult to staff shifts in a way that allows for unpredictable demands.
Providing physical health checks via a private contractor also has pros and cons. There is a clear focus on the physical health needs of detainees; the care provided has been good, and there is a solid audit trail. On the downside, it is costly, and it might have been possible to structure junior doctors’ time differently to permit them to deliver this role. An option to have CRHTT staff screen and triage for physical health problems is currently being explored.
Whilst building the POS within an inpatient ward would have been at odds with the recommendations of Churchill et al. 2 it might have had advantages such as more efficient use of real estate: the Maxwell Centre has two highly specified interview rooms which are unoccupied for up to 80% of the week. Wards in the hospital are often short of such rooms, and they could have been a useful addition. Furthermore, it may have been more cost-effective to staff the unit by running it from an inpatient ward: many patients do not require two staff to be allocated to them for the duration of their stay in the POS. With the back-up of a fully staffed ward shift, it might have been possible to use fewer staff resources than are currently required.
Prior to opening the Maxwell Centre, the joint training with the police was useful in ways that we had not anticipated. Police officers and clinicians had little real idea of what the other’s jobs involved and, in particular, of the limitations on what they could do: learning a little about each other’s roles was very valuable. However, ensuring that there is ongoing training remains an aspiration.
Cultures are also radically different between the health service and the police service, and inter-agency working needs to allow for this (e.g. allowing for the different processes of policy approval in the police and the NHS: agreeing revisions between the two bureaucracies can be time consuming).
The issue of very intoxicated detainees remains contested, with no agency seeing the issue as their remit and responsibility. The police are worried about the health and safety of prisoners in their care and do not regard cells as the best place for detainees. This position is strongly supported by Home Office guidance. Local clinical staff do not regard intoxication in the absence of evident mental illness as a mental health problem requiring specialist psychiatric intervention.
Age-appropriate environment
Since November 2008, a government commitment was made that no child under the age of 16 years can be admitted to an adult mental health ward. Section 31(3) of the MHA 2007 came into force on April 2010 amending the Mental Health Act 1983 (the Act) by inserting a new Section 131A. The new Section 131A applies to all children and young people (CYP) who are in hospital for treatment for mental disorder, whether they are detained under the Act or admitted informally. It requires managers of hospitals to ensure that ‘the patient’s environment in the hospital is suitable having regard to his age (subject to his needs)’. The wording of the Act allows for circumstances in which the adult ward may be considered the best place for a young person, although the default position for commissioners and providers is that a Child and Young Persons Services (CYPS) bed is normally preferable. Admission of a person younger than 18 years old to an adult wards will only occur if their need is either:
‘Overriding’: They need immediate admission for their safety or that of others. ‘Atypical’: The adult ward is the most appropriate clinical placement. For example, a young person who will be 18 years of age two weeks after admission may be better on the adult ward so that care does not have to be transferred within a very short time and therapeutic engagement with the adult team can take place.
There is no age limit on who may be subject to S136. Research by Laidlaw et al. 5 using health data shows that locally in 2002–2004, the age range of S136 detainees was 14–91 years. Police data for 2003–2006, a more reliable source, indicate that there were 19 (3%) people younger than 18 years of age made the subject of S136 during this period. Police data for 2012–2013 indicate there were only four people younger than 16 years of age detained in a police POS, three involving the same young person. Our most recent data for the Maxwell centre (2009–2013) show 6.3% (99) being younger than 18 years of age, with 1.3% (21) being younger than 16 years of age.
All of those younger than 18 years of age admitted to the Maxwell Centre are monitored, with key information sent to CYPS senior managers on a monthly basis. CYPS consultants were involved in the majority of the assessments, and most were confirmed to have a psychiatric presenting problem, which indicates the police are making reasonable preliminary assessments. In terms of outcomes, only a couple were admitted to an inpatient unit, with the majority discharged home, often with ongoing CYPS involvement.
In terms of care and supervision, the overwhelming majority of young people have no contact with adult patients. On the rare occasions where this is unavoidable, such contact is very carefully managed. While they are in the Maxwell Centre, their physical health is checked by primary care staff, and they are referred to the ED if necessary. Their psychiatric assessment will include contact with a consultant psychiatrist, usually a CYPS specialist, an Approved Mental Health Professional (AMHP) and a member of the CRHTT. They can ask for a friend or carer to be present and have access to the office telephone. Food and access to a television are provided. They receive a leaflet on why have been made subject to S136 which is also explained by the AMHP and a member of the CRHTT.
In terms of the MHA 2007 age-appropriate environment (AAE) requirement, it is suggested S136 falls into the category of ‘over-riding need’, as it is a significant emergency. Strictly speaking, it is not an admission to an adult psychiatric unit. It has been suggested that a more AAE such as a local CYPS unit that is available 24/7 which could admit in an emergency would be good practice. An AAE working group considered that in the absence of such a facility, the custom-built S136 Maxwell Centre is a huge improvement on the previous sole option of a police cell POS. It is an appropriate and well-managed facility to meet the needs of young people subject to S136. This is the context where young people are generally spending a very short time in the Maxwell Centre.
Mental Capacity Act
Since the opening of the Maxwell Centre, there has been pressure from the police to use the Centre as a place to bring people who they have restrained under the Mental Capacity Act (MCA), and who they believe require a mental health assessment. It is recognised that is a challenge for the police to dispose of someone they restrain under the MCA for reasons of mental health and where the CRHTT can respond in situ in a reasonable time frame. There has been confusion over the powers available to the police under S136 and the MCA. Clearly, Sections 5 and 6 of the MCA 2005 do not confer on police officers authority to remove persons to hospital or other POS for the purposes set out in S135 and S136 (see R Sessay v South London and Maudesley NHS Foundation Trusts, 2011). The Gloucestershire multi-agency MCA policy contains a police and MCA section with a ‘Decision Tree’ appendix that clarifies police responsibilities under the MCA. 20
Conveying
Following the Royal College of Psychiatrists guidance, 21 in July 2012, the issue of how subjects of S136 are conveyed to the POS has come to prominence. The RCP document recommends that ‘An ambulance (defined simply as a vehicle provided by the ambulance service) is the preferred form of transport to and between POS in most cases’. This recommendation is consistent with Para 10.17 of the MHA C of Practice and further reinforced in NPIA guidance (2010).
Discussions have taken place between commissioners and South West Ambulance Service (SWAS) NHSFT, our local ambulance service, and this is now reflected in our local S136 policy. Para 5.5 of our local policy states that ‘Police vehicles should only be used where there is extreme urgency, risk of violence or other danger, unreasonable delay, risk or harm to the detainee due to bad weather or potential risk of harm to the public’. In the light of these exceptions, it is not anticipated that transport by ambulance will become the norm. Data are being collected to monitor this.
Conclusion
In keeping with national trends, there has been an increase in the use of S136 in Gloucestershire since 2009. It is of note, however, that this local increase is particularly associated with the opening of the Maxwell Centre, a health-based POS, in early 2009. This suggests an increased willingness amongst police officers to use S136 powers when an alternative POS to the cells is available.
Now that a health-based POS is available, police cells are used relatively infrequently, with less than a quarter of S136 detainees going to the cells, as it is our local policy that detainees who are very intoxicated and/or posing an acute risk of violence should be managed initially in the cells. Over time, this proportion has been reducing. Once in the cells, around half of this group become settled enough to be transferred to the Maxwell Centre for completion of their assessment, and over time, the proportion being transferred has been increasing.
The issue of the most appropriate venue in which to manage very intoxicated detainees remains a bone of contention between the police and health services, with neither considering themselves best placed to manage such individuals.
Whilst the cells and the Maxwell Centre are the only designated POSs in the county, the local EDs are still occasionally used, usually when a detainee has an injury that requires urgent treatment. On occasions, the S136 assessment is then, for expediency, undertaken in the ED, but such assessments are unlikely to be recorded as part of routine S136 monitoring. Anecdotally, however, this type of assessment has become less frequent since the opening of the Maxwell Centre. Section 5.6 of the revised policy includes an option for the S136 assessment to take place within the Gloucestershire Hospitals NHS Foundation Trust ‘where this is practical and would not interfere with the treatment of other patients within the ED’. However, the ED has not been designated a formal POS in order that this option is not misused.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Acknowledgements
Inspector Andy Matheson, Gloucestershire Constabulary, helped with accessing data, and staff from the CRHTT provided general assistance.