
Abstract
The use of Flash-Ball® as a non-lethal weapon by several special units within the police and police forces started in France in 1995. Little literature is available concerning injuries caused by Flash-Ball® shooting. However, we report the case of a healthy 34-year-old male victim of a Flash-Ball® shooting during a riot following a sports event. This young man presented serious craniocerebral injuries with a left temporal fracture, moderate cerebral oedema, fronto-temporal haemorrhagic contusion along with an extra-dural hematoma and subarachnoid hemorrhage requiring neurological and rehabilitation care for two months leaving important sequelae. Although the risk is obviously lower than with firearms, Flash-Ball® is nonetheless potentially lethal and may cause serious physical injuries, particularly after a shot to the head.
Introduction
The Flash-Ball® is a less-lethal handgun used since 1995 by several special units of the French police Groupe d’Intervention de la Police Nationale, Brigade Anti Criminalité, Recherche Assistance Intervention Dissuasion and some police forces. 1 Developed by a French arms manufacturer, this less-lethal weapon is designed to incapacitate and neutralise dangerous individuals and to disperse riot crowds rather than to induce serious or fatal injuries.2,3 Its efficacy is based on a deterrent value, its detonation and its capacity to produce an effect equivalent to a technical knockout without skin penetration thanks to large rubber bullets with kinetic energies around 200 J. Since the first use of less-lethal weapons by British forces in Northern Ireland in 1970, reports of serious injuries and even deaths caused by hard rubber bullets have prompted the development of soft rubber bullets. 4 Descriptions of injuries caused specifically by a Flash-Ball® gun are rare. However, a case is reported here demonstrating that Flash-Ball® may induce severe craniocerebral injuries with important sequelae, which puts into question the low risk of this weapon.
Case report
A 34-year-old man was admitted in an emergency to the neurosurgery department of our University Hospital following a Flash-Ball® shot during a riot at a sports event. According to the witnesses at the scene, the shot had been fired within a 3–4 m distance of the victim. After a single impact to the left side of his head, the victim immediately lost consciousness for a few seconds.
Upon admission, the victim complained of severe headache, particularly on the left side. His medical history shows a head trauma following a road accident 14 years before his present injuries without sequelae.
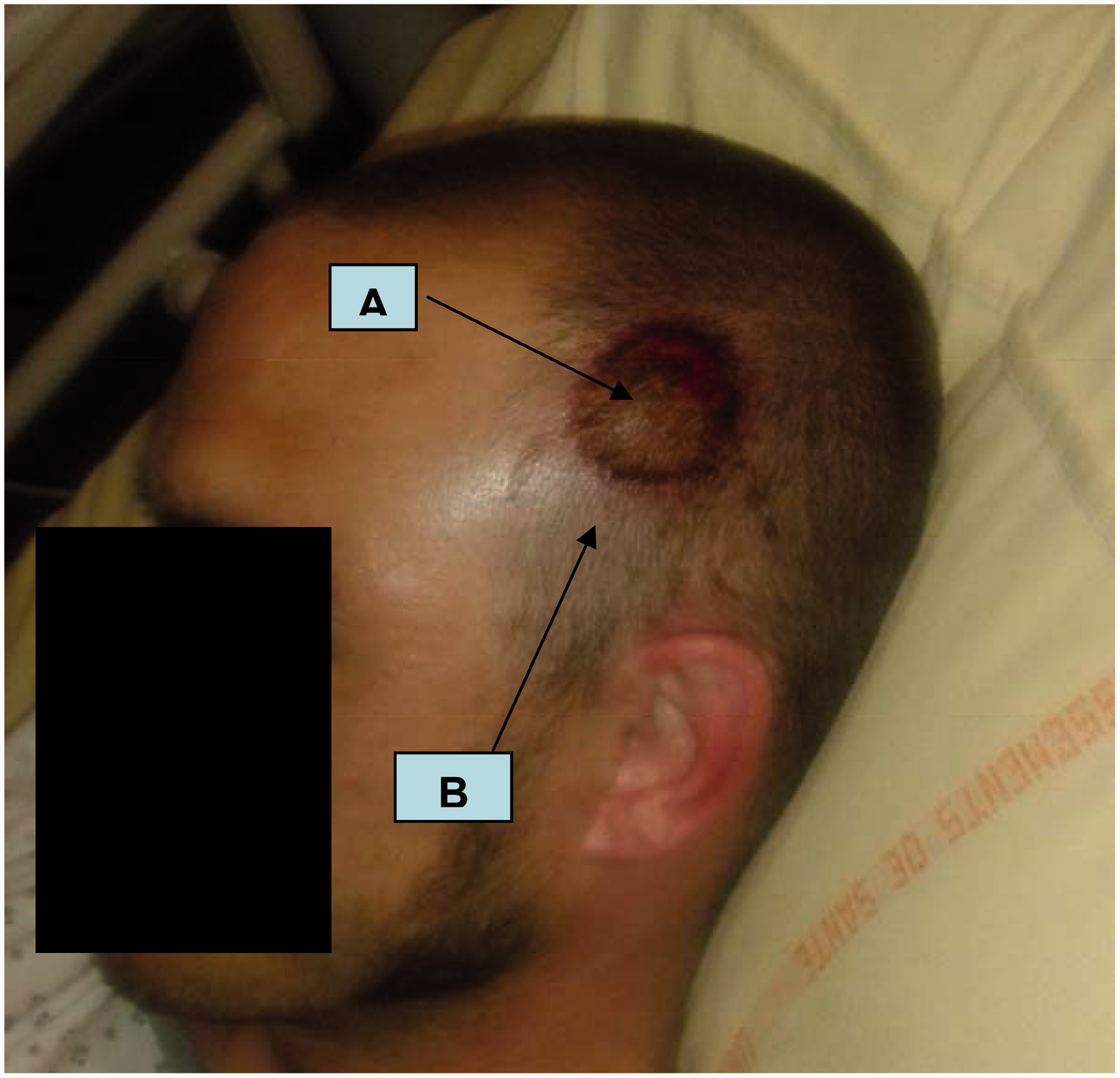
The clinical examination revealed a Glasgow coma scale score of 15/15 and a large left fronto-temporal haematoma with a severe contusion mark 60 mm in diameter with an abrased ring 10 mm wide (Figure 1). A cranial computed tomography (CT) scan showed a left fronto-temporal haematoma, a fracture of the left temporal bone extending towards the left temporo-mandibular joint, a moderate cerebral oedema, a pneumocephalus associated with a left fronto-temporal haemorrhagic contusion accompanied by extra-axial and subarachnoid haemorrhage. No bone and cerebral injuries were observed on the opposite right side (Figure 2). In the absence of surgical indication, the victim remained hospitalised in the rehabilitation department with a clinical course characterised by a generalised tonic-clonic seizure one week after admission, resulting in an initial treatment with levetiracetam. Two months later, the victim presented important sequelae:
Circular alopecia scarring in the fronto-temporal area. Neuropsychological disorders with disinhibition, extreme fatigue, attention deficiency and psychomotor delay requiring rehabilitation, which are symptoms suggestive of a subjective syndrome of brain-injured people (syndrome subjectif des traumatises crâniens). Dysarthria with shortage of words, which can be due to a right central facial paralysis and decline of muscle strength in the right hand in relation to injury of the left motor cerebral area. Left destructive vestibular syndrome, perceptive deafness for high frequencies responsible for a 35% decline of hearing on the left side requiring a hearing aid. Left destructive vestibular syndrome, perceptive deafness for high frequencies responsible for a 35% decline of hearing on the left side is a classic complication following left otic barotrauma.
Left fronto-temporal injury on admission. (A) Severe contusion mark with abrased ring. (B) Large fronto-temporal haematoma. Computed tomography (CT) scan on admission (moderate cerebral oedema, pneumocephalus, left fronto-temporal haemorrhagic contusion, extra-axial and subarachnoid haemorrhage).

In the present case, we note a link between initial injuries located on the left side of the head and, two months later, important sequelae.
Discussion
The first non-lethal weapon utilisation was reported in a civil riot in Hong Kong during the 1950s and 1960s with reports of severe facial injuries due to the use of wooden batons. 5 One decade later, plastic bullets hitting heads, faces and necks during rioting caused 14 deaths in Northern Ireland.6,7 The real lethal potential of these weapons was recognised a little later in South Africa as well as during Israeli–Arab conflicts.8–10 Non-lethal technologies are designed to incapacitate and neutralise dangerous, aggressive, violent individuals or groups in civil or war contexts rather than to induce fatal or serious injuries.1,11 Temporarily incapacitating the target makes these weapons attractive for police forces and also for self-defence in many countries where non-lethal weapons are not subject to ownership restrictions as severe as for other arms. 12 Less-lethal technology is based on the delivery of kinetic energy (Flash-Ball®, Punch®, bean bag and Flexible baton®, Fiocchi Anticrime cartridge® and rubber stinger grenade), chemical energy (pepper spray) or electromagnetic energy (electroshock weapon Taser®), and weapons are numerous according to the type of guns and projectile available.1,13
In France, two versions of Flash-Ball® are produced: one with vertically stacked barrels made from metal alloys with large rubber balls, rubber buckshot and balls with colouring or irritating chemicals designed to burst on impact; and one made from lighter composite materials with the two barrels side by side with non-metallic ammunitions. While this type of weapon delivers a blunt impact without causing penetrating injuries, the increasing use of rubber bullets has led to an increase of cases described in the literature. Rubber-bullet injuries by firearms are well described, with authors reporting cases of penetrating chest injury, 14 severe eye and facial trauma15–17 or paediatric head trauma. 18 Due to these potentially severe injuries, their use is considered the ultimate step, before the use of deadly force, within the police use-of-force continuum guidelines.2–3 To our knowledge, only four cases of injuries by Flash-Ball® have been reported. One fatal case of Commotio Cordis in a healthy 43-year-old man due to a chest impact. 19 Pinaud et al. describe an orbital and ocular trauma with loss of the internal half of the inferior eyelid, a rupture of the canthal tendon and inferior lachrymal duct, a conjunctival wound of the superior eyelid with loss of tissue exposing the levator muscle, a fracture of the upper jaw bone, a fracture with loss of bone of the orbital floor, a lesion of the infra orbital nerve and a ruptured ocular globe with burst contents. 1 Wahl et al. report a case of a vaso-vagal syncope following multiple contusions of the abdominal wall and the thighs on a healthy 22-year-old man, and a case of severe contusion of the anterior chest wall associated with cardiac and pulmonary contusion on a healthy 25-year-old man. 3 These observations show that impacts from the Flash-Ball® can cause significant injury to internal organs, even without penetration.
Concerning ballistics data, the manufacturer specified on its website ‘by virtue of projectiles studied to avoid, even at extremely short distances, penetrating a normally clothed person, the Flash-Ball® provoked on impact the equivalent of a technical KO’. 20 The kinetic energy of the rubber ball and the buckshot is indicated to be 200 J, and surprisingly, the same value is given for muzzle energy at both 2.5 m and 7 m, whereas a significant decrease would be expected at a distance of 7 m. 3 The soft 44-mm rubber bullet ball weighing 28 g is the most common type, and its stopping power of 200 J at 2.5 m is equivalent to that of a 38 special and achieves the same effect as an uppercut of a champion boxer.1,20 Although there are no accurate data within literature regarding Flash-Ball®, Wahl et al. compared its characteristics to those of other non-lethal arms with a similar mechanism.
The MR 35 Punch® is a similar weapon to the Flash-Ball® with rubber balls measuring 35 mm and weighing 21 g with muzzle kinetic energy ranging from 150 to 200 J representing the best approximation of the characteristics of the Flash-Ball®.3,21 According to these data, the Flash-Ball® is more powerful than the MR 35 Punch®. The bean bag or Flexible baton® is the less-lethal weapon with the most complete description in the literature. This weapon is composed of a fabric bag containing about 40 g of lead shot pellets. It is designed to distribute the impact energy on a surface large enough to avoid skin penetration, but it has been the cause of several injuries. Even though this weapon cannot be compared to the Flash-Ball®, as almost no rubber ball munitions were included, the National Institute of Justice in North America gives a good appreciation of the incidence of severe injuries. More severe injuries were laceration (5.5%), fractures (3.5%) and penetration (1.8%). Death attributable to the impact munition occurred in 2.7% of cases. 22
Even though the Flash-Ball® is not considered lethal, its sale and use are thoroughly controlled by French law. 23 The French models are classified in the 4th category (licence for acquisition and holding of defensive fire arms with ammunition) and 7th category (arms and ammunition for shooting gallery, fair or showroom). Instructions for optimal safety use are poorly documented, and an approximation may be assessed by a study of the French MR35.1,23 This study reports that a close-range shot may result in severe wound injuries due to the potential penetration of the projectile. The low morbidity and mortality rates of these non-lethal weapons are questioned by publications reporting the field reality,4,7,10,12–20,24 and the terminology ‘less-lethal’ furthermore induces confusion, as it implies conventional weapons to be ‘lethal’. 3 For Scolan et al., the vital, functional and cosmetic prognosis of contused visceral injuries, associated or not with bone fractures, depends on the impact zone with the cephalic, cervical and thoracic regions being the most lethal ones, 13 The shooting distance also seems to be an important element to be taken into account.17,27,28 In the present case, according to the witnesses at the scene, the shot had been fired 3–4 m away from the victim, whereas in the literature, the distance was 2–7 m.1,3,19
We assume a shot, which strikes a body within 10 m, may cause several injuries, in particular to the head, thorax and abdomen. If Flash-Ball® is classified as a non-lethal weapon developed to incapacitate a violent or/and dangerous individual, the French National Commission of Business Ethic and Safety recommends it ‘should not be used during demonstrations in public places, except on rare occasions wich have yet to be defined’. 29 This report shows the potential lethality and damaging risks for this type of arms and the necessity to the precautionary measures. Even if Flash-Ball® is less lethal than lethal weapons in general, Scolan et al. suggest that the term ‘non-lethal’ should be replaced with ‘reduced lethality’ and recommend more training for police forces by providing all the information regarding the risks of injury linked to their use, followed by a practical instruction on the weapons’ use. This training often seems to be missing.7,29
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interests
The authors declare that there is no conflict of interest.