
Abstract
Cognitive impairment unattended by subjective symptoms or objective signs is an uncommon but important consequence of hypoglycaemia. It can lead to a condition in which a patient behaves as an automaton in a manner totally alien to their usual personality and of which they have no recollection when their blood glucose level is restored to normal. It can cause a wide range of criminal behaviour, although the commonest offences relate to a loss of control, for example driving offences. Determination of criminal responsibility is extremely difficult and relies very heavily upon the quality of the medical evidence and interpretation of the law, which is out of step with current medical science.
Introduction
The legal approach to hypoglycaemic automatism is confused – especially in its relation to driving1,2 – due largely to the unrealistic definition of automatism adopted by legal authorities in the UK. This has no foundation in medical fact and is currently under review by the Law Commission.
Diabetes, insulin and hypoglycaemia
The brain has an absolute requirement for a constant supply of glucose in order for it to function properly. It is provided by glucose carried in the blood at a tightly regulated concentration of about 4–10 mmol/L, regardless of whether the person has eaten or not. A fall in blood glucose level to below about 3.5 mmol/L, however caused, may cause the brain to malfunction. In practice, the most common cause of such a fall is treatment of diabetes with certain drugs, of which insulin and sulphonylureas are the most important.
Insulin was introduced for the treatment of diabetes in 1922, and rapidly gained recognition as a miracle cure, even though its propensity to produce a low blood glucose concentration (hypoglycaemia) leads to both medical and legal problems. The definition of hypoglycaemia is necessarily arbitrary, but it is generally accepted to exist when the blood glucose concentration is <3.0 mmol/L (54 mg/100 mL). Hypoglycaemia, which is a chemical definition, must be distinguished from the symptoms of neuroglycopenia. Neuroglycopenia is the shortage of glucose supply to the brain, and this may occur at blood glucose concentrations that do not necessarily meet the criteria for the definition of hypoglycaemia adopted.
Symptomatology
The neuroglycopenic syndromes.
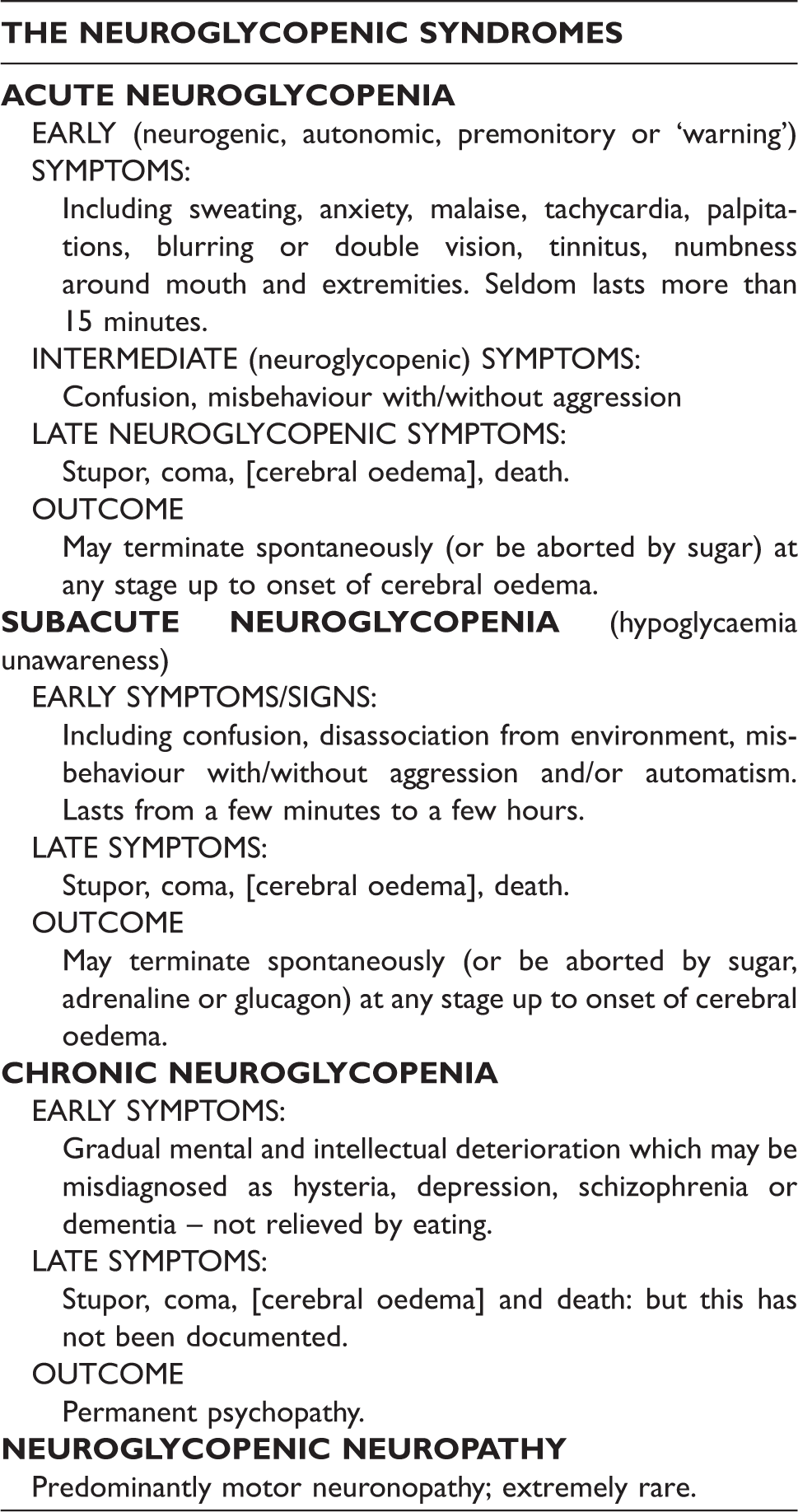
Acute neuroglycopenia
Typical symptoms produced by hypoglycaemia, including profuse sweating, rapid heartbeat, a sense of anxiety, are caused by activation of the autonomic nervous system as part of the body’s defence against the damaging effect of hypoglycaemia on the brain. They are described collectively as acute neuroglycopenia as autonomic symptoms.
Subacute neuroglycopenia (hypoglycaemia unawareness)
Sometimes behavioural and mental changes precede or occur without the subjective symptoms that all patients starting insulin therapy are taught to recognise as a warning of impending incapacity and to abort by eating some rapidly absorbed carbohydrate. Such cognitive and behavioural changes are described as subacute neuroglycopenia when they occur in patients with spontaneous hypoglycaemia who have no idea about their origin or significance and as hypoglycaemia unawareness when they occur in insulin-treated diabetic patients.
During an episode of subacuteneuroglycopenia, a person can undertake, with seeming normality, – habitually performed tasks, such as talking, walking, preparing a meal, doing housework or driving a car, that have become second nature to them. On recovering from such an attack, they have no, or only the vaguest and probably incorrect recollection, when prompted, of what happened during and shortly before it began.
Abnormal behaviour caused by hypoglycaemia has been accepted as a defence against criminal charges in most jurisdictions since shortly after the introduction of insulin therapy. It is, however, rare – especially when unaccompanied by typical symptoms – considering how common insulin-induced hypoglycaemia is – and was once thought, wrongly, only to occur when accompanied by signs and symptoms of acute neuroglycopenia. Diabetes UK, commenting in 2002 on a case of death by dangerous driving, stated that ‘there would have been prior symptoms of oncoming hypoglycaemia, which is caused by low blood sugar levels’. Some expert witnesses are similarly unaware of the existence of hypoglycaemia unawareness. 3 Though subacute neuroglycopenia was first observed in the early 1940s, it was not until tighter regulation of blood glucose levels became the standard of care, in order to minimise the long-term sequelae of hyperglycaemia, 4 that hypoglycaemia unawareness was rediscovered and named. 5
The manifestations of subacute neuroglycopenia vary from mild cognitive impairment up to coma in the most extreme cases. It is characterised by a reduced ability to perform complex mental tasks and an increase in the number of errors while performing them. Patients have no insight into their incapacity, even when it is pointed out to them, and are incapable of forming criminal intent. The electro-encephalogram (EEG) reveals characteristic changes in brain activity that revert to normal on relief of the hypoglycaemia.
The patient may appear completely normal to someone who does not know them. Often, however, they look and act as though they are drunk and may be treated as such by observers. They behave like an automaton and lack the facial expression and responses appropriate to the situation they are in. This altered mental state persists for as long as their blood glucose concentration remains low – generally just a few minutes but sometimes for a few hours or so – depending on what caused it and how it is treated. 6
Neuroglycopenia and the law
It is acknowledged that patients may act impulsively whilst they are impaired by neuroglycopenic brain malfunction and are incapable of forming intent to commit an offence, ranging from the trivial to the most heinous. 7 More difficult, from a medico-legal point of view, are offences involving the driving of a motor vehicle that do not occur on the spur of the moment and are consequently less readily accepted by courts as exonerating the offender due to the prevailing legal view of what constitutes automatism.
Traffic offences, whether involving death of a bystander, or not, are far from rare – I have been involved in no less than 13 such cases in the past 18 years.
Brief summary of cases in which the author was involved as an expert witness between 1994 and 2012 of dangerous driving whilst driver was suspected of suffering from hypoglycaemia.

N/I, no information.
Illustrative cases of driving whilst hypoglycaemic
Below are a few cases I have been involved with as an expert witness, which illustrate some of the problems encountered in presenting a defence of hypoglycaemic automatism to a serious driving charge.
Terence Tarleton
In the civil case of Tarleton v Weetabix, a driver who suffered a hypoglycaemic episode due to a malignant insulinoma crashed into a shop. The lorry driver’s employer was sued. The Court of Appeal 9 held that ‘There was no reason in principle why a driver should not escape liability where the disabling event was not sudden but gradual, providing the driver was unaware of it’. Civil cases apply a different standard to criminal cases, however, and as the court pointed out, ‘the criminal law relating to the defence of automatism was irrelevant’.
Phillip Willey
Phillip Willey, a diabetic patient on insulin therapy, collided with two pedestrians at about 7.10 pm on 31 May 2006, killing one and seriously injuring the other.
The accident was witnessed by a driver who trailed Phillip Willey for many miles because he had already observed him driving recklessly. Several other witnesses came forward and described Mr Willey’s car engine as ‘racing’ as he drove through the village, narrowly avoiding collisions with parked cars and vehicles coming in the opposite direction.
At the scene, Mr Willey was sitting in his car seat with his engine still on. From the way he answered questions, an observer formed the impression that Mr Willey was drunk. A passenger in a car coming the other way spoke to Mr Willey who said, ‘I didn’t see them’ or something to that effect – ‘I didn’t mean to; how could this happen?’
The first paramedic on the scene measured Mr Willey’s blood glucose level. It was 1.9 mmol/L, and he was given oral glucose in the form of Hypostop®. By the time Mr Willey got to hospital, his blood glucose level was 5.8 mmol/L, and he was in fully possession of his faculties.
At his trial, Mr Willey pleaded not guilty on the basis of hypoglycaemic automatism, and explained that that he had never been advised to test his blood glucose before driving. The team looking after his diabetes were reasonably confident that they had advised him to do this, but were unable to produce confirmatory evidence to that effect.
On that basis, the Judge decided there was no case to answer and dismissed the charge. The prosecution appealed and was upheld.
10
The appeal court held that it was ‘for the defence to provide an evidential foundation for the defence and it could do so either by relying on the evidence already given or by calling Mr Willey to give evidence himself. If left to the evidence already given, there was unlikely to have been sufficient evidence of a total loss of control’. The court went on to say, ‘the blood sugar level found by the paramedics at the scene was not, of itself, evidence of total loss of control,
The case was returned to the court where, at a retrial, the defendant was sentenced to 4.5 years imprisonment for causing death by dangerous driving. HHJ Llewellyn-Jones QC told Willey that a lump of sugar could have averted the collision. He said that a gross mismanagement of Willey’s condition and failure to test his blood-sugar levels had caused the tragedy. 11 ‘If you had done that before you set off on this late afternoon, that reading undoubtedly would have shown that your blood sugar reading was low, and a lump of sugar and a short break would have prevented this tragic accident’. He went on to say, ‘Because of that gross mismanagement of your diabetic condition, in my judgment, despite the fact you had managed to drive for some years, this was in fact just an accident waiting to happen’.
Trevor Clarke
Trevor Clarke left the road as a result of a hypoglycaemic episode, colliding with two children, the younger of whom died of his injuries. Several independent accounts of his behaviour agreed that Mr Clarke had been driving erratically for at least two miles before the accident happened, narrowly missing other vehicles on the way. Several witnesses believed that Mr Clarke was drunk and one – subsequently shown to be false – believed he smelled of alcohol. The first person to speak to Mr Clarke after the accident asked him if he was OK, and he replied, ‘Yeah, I’m OK. Yeah’, the opposite to what she would have expected. She realised he was not drunk, although he sat motionless in the car seemingly ignoring what was going on around him.
Exactly what happened to Mr Clarke after the accident and got out of the car is far from clear. It appears, however, that he ended up in an ambulance and informed the paramedics that he suffered from type 1 diabetes. It appears that the ambulance crew did not measure or record his blood glucose concentration. When he reached hospital, it was 6.0 mmol/L, after he had already eaten six glucose tablets.
At around 12–12.30 pm on the day of the accident, he ate a light lunch and measured his blood glucose, which was normal at 4 mmol/L. He then gave himself three units of quick-acting insulin analogue as he had been advised. He appears to have developed subacute neuroglycopenia around 2 pm when his driving was first observed to be erratic shortly before the accident at 2.05 pm. The sugar he kept in his car was untouched.
Two experts in hypoglycaemia (the author and Prof Anthony Barnett) called by the defence testified that Mr Clarke’s management of his diabetes appeared to be exemplary and were in no doubt that he was completely unaware of his impairment. The consultant geriatrician called by the prosecution disagreed and asserted that Mr Clarke must have experienced symptoms that he ignored. The judge and jury preferred the evidence of the latter, leading the judge to remark, ‘There came a time, on the basis of the evidence that we heard and the jury’s verdict, when you should have been aware of your deteriorating condition, of the likelihood of an imminent hypoglycaemic attack’. He went on to say, ‘The jury concluded that the awareness that you had was such as it should have caused you to stop driving or indeed never start driving that two miles stretch that led up to the tragic accident that shortly afterwards took place’.
This was to misunderstand completely the pathophysiology of hypoglycaemia unawareness that has established that brain malfunction can develop from hypoglycaemia without giving rise to any subjective or warning symptoms.
Mr Clarke was convicted of dangerous driving and sentenced to three years in jail. The defendant appealed the sentence. The sentencing judge had considered Mr Clarke’s medical condition an exacerbating factor, but the Court of Appeal 12 disagreed and reduced his custodial sentence from three years to one year. They did not acknowledge that the defendant had hypoglycaemic unawareness, as this would have contradicted the basis of the jury verdict (which was not being appealed). The legal aspects of this case are discussed in greater detail by Rumbold and Wasik. 3
Herbert Aldous
Mr Herbert John Aldous, a 78-year-old man with type 2 diabetes, was involved in a fatal traffic accident in Bolton at 4.30 pm on 14 June 2004. On the morning of the accident, Mr Aldous had measured his blood glucose, and it was normal at 5.1 mmol/L. He did not measure it again before driving. He had not been advised or encouraged to do so, as he was on glibenclamide (a sulphonylurea) rather than on insulin, and therefore at lower risk of hypoglycaemia.
The collision involved a cyclist, Mr David Kerslake, who catapulted into the air and sustained injuries from which he died.
Mr Aldous was not seriously injured, but the paramedic called to the scene stated he was ‘vague. He was responding to my questions but I did notice they were delayed responses’. His blood glucose level was 2.0 mmol/L, and he was given an intramuscular injection of glucagon. His mental condition improved within a few minutes, but he had no idea what had happened to him or how he had got there. By the time he reached hospital, his blood glucose level was 6.1 mmol/L, and he was fully mentally alert.
On the basis of the evidence they had received, the CPS concluded that Mr Aldous was ‘not driving’ at the relevant time and offered no evidence at trial.
Commentary on illustrative cases
The belief, originating from the very earliest days of insulin therapy, that loss of voluntary control caused by hypoglycaemia is always preceded by a period of awareness that something is wrong – albeit sometimes very briefly – is still firmly rooted in the minds of some medical practitioners. Though known to be incorrect for at least 50 years, it persists because, until the modern era of ‘tight control’ of diabetes, hypoglycaemia unawareness was rare and beyond the experience of many general medical practitioners and diabetes specialists.
Current DVLA advice for patients on insulin is to measure their blood glucose concentration before driving and every two hours thereafter. They are advised never to start to drive if their blood glucose level is <4.0 mmol/L, and to eat some carbohydrate-containing food and retest every two hours whilst driving. If they do experience symptoms of acute neuroglycopenia whilst driving, they must stop and take some carbohydrate by mouth. The DVLA advise in a letter sent to every diabetic patient receiving insulin therapy that ‘You should not start driving until 45 minutes after blood glucose has returned to normal (confirmed by measuring blood glucose)’, as ‘it takes up to 45 minutes for the brain to recover fully’.
Unfortunately, a driver may be already so cognitively impaired that by the time they undertake their pre-driving blood glucose test, they are unable to appreciate the significance of a low reading and may consequently ignore it. Failure to follow DVLA guidelines is not evidence of negligence by the driver per se.
Automatism and culpability
Diabetic patients are, because of their propensity to develop hypoglycaemia,13,14 more likely to be involved in a driving accident, though only slightly more, than the rest of the population. 15 It has therefore been a matter of debate since the earliest days of insulin therapy whether patients on insulin therapy should be allowed to have a driving licence. Most jurisdictions have concluded that, as a matter of public policy, the risk is sufficiently small for insulin-treated diabetic patients to be permitted to hold a driving licence – providing they fulfil certain criteria. More stringent conditions apply to those driving public-service or large goods vehicles. 16
People with diabetes are no less likely, when their blood glucose level is normal or moderately raised, to drive carelessly or dangerously than non-diabetic people. Consequently, diabetes alone is not a defence against dangerous driving, whereas cognitive impairment due to hypoglycaemia resulting from its treatment may be. Not everyone who drives and causes an accident whilst in a state of neuroglycopenic (hypoglycaemic) automatism is necessarily free from blame.
The court must decide whether the defendant did suffer a genuine neuroglycopenic automatism episode. If the court is persuaded that there was neuroglycopenic automatism, it must then decide whether the driver suffered hypoglycaemic unawareness or had some warning symptoms, such that he should have recognised an impending neuroglycopenic episode and stopped driving. If the court decides that the driver suffered hypoglycaemia unawareness, it must then decide whether the driver was previously aware of the condition. If he was, then he should not have been driving at all. He would be at fault simply by getting behind the wheel.
All three decision criteria rely very heavily on medical evidence – the first almost exclusively so. Definitive diagnosis is, however, often far from easy and must usually be inferred from historical evidence rather than established by observation and measurement.
Occasionally, as in the case of Tarleton cited above, the circumstances of the case are such that there can be no doubt that the driver was suffering from neuroglycopenic automatism and that he experienced no warning symptoms. In his case, like many cases of alleged neuroglycopenic automatism, no measurement of blood glucose was made at the time of the incident, and consequently the diagnosis rested solely on the clinical evidence.
Pointers to the probability that a person’s abnormal behaviour was neuroglycopenic
These include:
Circumstances that are known to predispose to the development of hypoglycaemia and more especially of hypoglycaemia unawareness. Evidence that the suspect had taken insulin or other potential hypoglycaemia-producing drug at a time relevant to the incident. A rapid and complete change in the patient’s demeanour after being given something sugary to eat or drink. Amnesia for the events immediately preceding, during and immediately following the event. Apparently motiveless and totally uncharacteristic behaviour.
Whilst none of these pointers is diagnostic in its own right, they are collectively the best that can be done to support a diagnosis of neuroglycopenic in the absence of a blood-sugar measurement made within minutes of the event.
Abuse of hypoglycaemic automatism as a defence
Hypoglycaemia may develop spontaneously under a variety of conditions – apart from diabetes treated with insulin – and has been advanced as a defence against a large number of offences, often on extremely little evidence. 17
Nevertheless, because it is difficult to dismiss with certainty the possibility, once it has been suggested that aberrant behaviour by an insulin-treated diabetic patient or someone given a spurious diagnosis of hypoglycaemia was caused by neuroglycopenia, the defence of neuroglycopenic automatism remains open to abuse. Sometimes, for example when the accused offers the fact that they had failed to take their insulin as an explanation for their altered behaviour, 18 the claim can easily be dismissed. In most, it will depend upon the knowledge and experience of the expert consulted to advise the court as to whether hypoglycaemic automatism was likely to have been present at the relevant time.
It must be stressed that not everyone who drives whilst in an automatic state from iatrogenic insulin-induced hypoglycaemia is free from blame. Most drivers who develop hypoglycaemia whilst driving do experience warning symptoms, but some choose to ignore them. 19 Others ignore advice as to when and how often they should test their blood glucose concentration before commencing to drive and during a journey. A number fail to report a history of hypoglycaemia unawareness to the DVLA and desist from driving until awareness has been restored by adjustment of their therapeutic regime.
In the past, it was not uncommon for patients to claim – sometimes truthfully – that they had not been given adequate advice when first prescribed insulin, but this is now rare. There remains a minority of patients who develop hypoglycaemia unawareness for the first time whilst driving and who commit what would otherwise be a moving traffic offence. In these cases, the defence of neuroglycopenic automatism is fully justified.
Conclusion
Automatism due to brain malfunction consequent upon neuroglycopenia, most often caused by treatment of diabetes, with insulin is an established medical fact. In most cases, it is accompanied or preceded by intrusive symptoms that the patient has come or been taught to recognise as a prelude to more severe cognitive dysfunction, unless aborted by eating some carbohydrate. In a minority, the patient, through no fault of their own, experiences absolutely no symptoms and is totally unaware that they had become grossly impaired until they are ‘brought round’ by the ingestion or injection of glucose. Only if patients with diabetes on insulin therapy were forbidden from holding a driving license could accidents arising from hypoglycaemia unawareness be avoided completely. There have been few cases reported where the driver suffered hypoglycaemic unawareness, so there do not appear to be sufficient public-safety concerns for such a restriction.
The law should therefore take a more realistic approach to the defence of neuroglycopenic automatism and to the weight of the medical evidence than it has done in the past if injustices are to be avoided in the future. The proposed Law Commission reform would help defendants such as Clarke, who have been unable to plead automatism because they did not satisfy the requirement for ‘total loss of control’. They would lack the capacities in the first and third parts of the proposed test, namely
rationally to form a judgment about the relevant conduct or circumstances; and to control his or her physical acts in relation to the relevant conduct or circumstances.
The lack of either capacity would qualify the defendant as ‘not criminally responsible by reason of recognised medical condition’.
Footnotes
Conflict of interests
All authors declare that they have no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.