
Abstract
Fatal air embolism related to endoscopic retrograde cholangiopancreatography is a very rare phenomenon. The authors describe the case of a 51-year-old female patient who developed this mortal complication; a computed tomography (CT) examination was performed in articulo mortis by the physicians. Autopsy was unreliable because of bizarre post-mortem changes (reabsorption of intra-cardiac gas vs. conservation of intra-cranial gas) and a lack of strong diagnostic value of histological findings. The right diagnosis was possible thanks only to the CT examination that permitted the assumption of this possible cause of death before the autopsy and to prepare the necessary procedures to recognise and probe air embolism. This case exemplifies how early post-mortem imaging can be crucial to avoid a wrong diagnosis.
Introduction
Air embolism associated with endoscopic retrograde cholangiopancreatography (ERCP) is a known phenomenon, but fatal cases are very rare. To our knowledge, fewer than 15 cases have been described.1,2 Potential mechanisms for venous air embolism include biliary-venous fistulas/shunts, intramural dissection of insufflated air, transection of duodenal vein radicles, portocaval collaterals and air flow directly into the hepatic veins or inferior vena cava. ‘Paradoxical’ systemic embolism can be due to intra-cardiac or intrapulmonary shunts and retrograde flow into cerebral veins through the superior vena cava or vertebral veins. Inflammatory conditions (of the bile duct, its surrounding veins or bowel, hepatic abscesses and so on) and tumours represent risk factors of air embolism. 1 From data in the literature, the quantity of air necessary to cause a circulatory air embolism is unclear, varying from 10 to 480 mL,3,4 depending on the velocity of injection of the air in the circulatory system and on the extention of the embolism: only pulmonary or cerebral too. Other authors have reported that the lethal dose for humans has been estimated to be 3–5 mL/kg, and that 300–500 mL of gas injected at a rate of 100 mL/sec is fatal for humans.5,6
We describe our experience of a fatal forensic case, which exemplifies how post-mortem investigations can be unreliable for the diagnosis of a particular cause of death, and how early post-mortem imaging could help to avoid a wrong diagnosis.
Case report
A 51-year-old female was referred because of recurrent episodes of biliary colic and pancreatitis. For similar episodes, 17 years previously, she had undergone a cholecystectomy. Recently, because of the presence of calculi in the intrahepatic biliary tree, the patient had undergone extracorporeal shock wave lithotripsy and an ERCP with sphincterotomy. For the persistence of a big calculus, a further ERCP was scheduled.
During the procedure, sedation was obtained with propofol and remifentanil as needed. Spontaneous breathing was maintained with O2 therapy. Twenty minutes after the beginning of the procedure, a sudden decrease in SpO2 (83%) was observed. Soon, short runs of ventricular tachycardia (150 beats/minute) and hypotension (blood pressure 70/30 mmHg), followed by severe bradycardia, ensued. The patient was transferred to the intensive care unit. At electrocardiogram, pulseless electric activity was observed. The Glasgow Coma Score was 3. The patient died two hours later without regaining consciousness. In articulo mortis, a computed tomography (CT) scan showed massive intra-cardiac air and cerebral air embolism (Figures 1 and 2).
Computed tomography performed in articulo mortis showed gas in the right atrium (A), and right ventricle (B). At autopsy, the intra-cardiac gas was no longer present. Computed tomography performed in articulo mortis shows intra-cranial small gas bubble (A) and (B). At autopsy, in the same anatomical region (left occipitum), a small gas bubble was observed (C) and (D).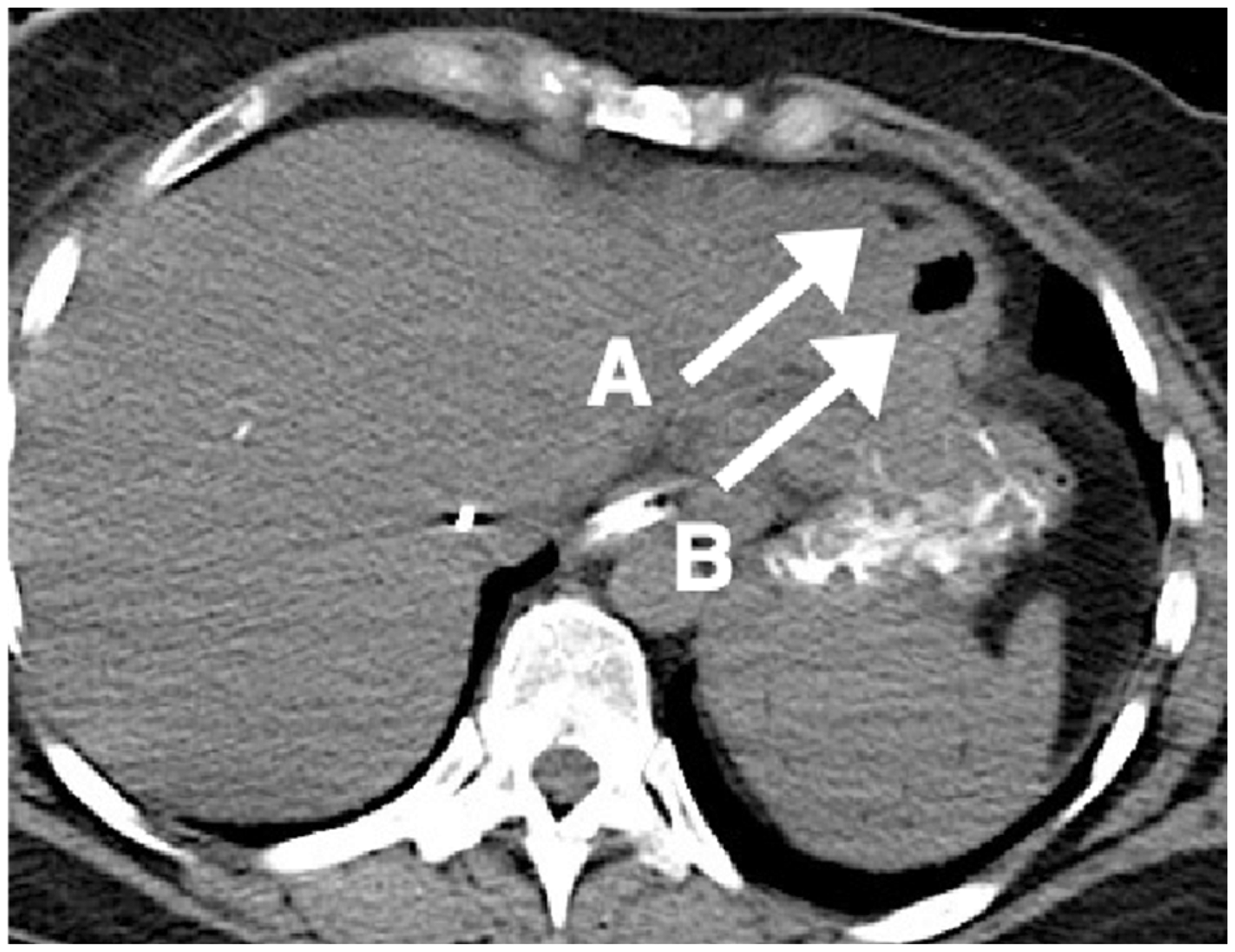

Because of decision of the public prosecutor, the autopsy could only be performed 10 days after the death. When opening the heart under water, no intra-cardiac gas was revealed. Instead, a small gas bubble was observed in a leptomeningeal vein of the left occipital region, corresponding to the TC image of the air embolism (Figure 2). Air insufflated into the common bile duct was found to exit from the supra-hepatic veins, thus revealing the existence of a biliary-vascular fistula, but this was not visible on exploration of the biliary tree. The autopsy also demonstrated a patent foramen ovale, considered responsible for the paradoxical air embolism.
Toxicological analysis showed the presence of low traces of propofol and remifentanil, in agreement with the low half-life of the two administered anaesthetic substances. No other xenobiotic was revealed.
On examination of the formalin-fixed brain, no other macroscopic signs of air embolism were recognisable. Histological analysis showed only clear holes in some small cerebral arteries (Figure 3).
Histology showed clear holes in some small cerebral arteries (A), in presence of fixation artefacts: perivascular shrinkage (B).
Discussion
When death occurs during a medical procedure, often a civil and/or criminal action is brought against the physicians. Any evaluation of the death related to hypothetical medical errors must start by ascertaining the cause of death. This matter is not that straightforward. Indeed, demonstrating the exact cause of death at autopsy is often difficult, and sometimes it may even be impossible.
It is known that autoptic diagnosis of gas embolism is based on chemical analysis of gas collected from the heart and on some morphological findings, described by previous authors.7–9 However, these procedures are not part of normal practice in routine forensic autopsies and can be implemented only when such an event can be assumed before the autopsy.
Because of the rarity of fatal air embolism during ERCP, we have to acknowledge that ex ante, we would not have assumed this possible cause of death without the existence of a pre-autoptic CT, and we would not have prepared the necessary procedures to recognise and probe air embolism at autopsy.8,9
Another item of technical difficulty relates to the possibility of intra-cardiac gas reabsorption, as our case demonstrates. This could be due to a long time interval between death and autopsy (10 days in our case). Nevertheless, in the case of a criminal action against the physicians, technical waiting times are often required by the public prosecutor. In Italy, according to the Penal Procedure Code, the prosecutor appoints a forensic pathologist as his technical consultant, in order to perform the autopsy and to establish the cause of death. Whenever forensic investigations require a so-called unrepeatable act (such as the autopsy), the persons under investigation have the right to appoint a medical consultant that participates in autopsy and protects their interests. Thus, the delay depends on the need to identify the persons under investigations and to allow them to appoint their lawyers and their forensic pathologist.
In such conditions, the possible presence of air emboli could be impossible to prove, even in the presence of technically correct procedures for their collection. As already said, in our case, intra-cardiac gas was completely reabsorbed, and we would not have observed and collected it anyway.
Previous authors have reported histological findings, represented by: vesicular spaces with sharp border in the erythrocyte columns, surrounded by leukocytes, thrombocytes and fibrin; perivascular empty areas distended in a ‘bubble-like’ manner; 10 and round clear holes in the meningeal vessels. 11 In our case, we observed some intravascular clear holes, but these were not perfectly round, and fixation artefacts were present (perivascular shrinkages; Figure 3). Therefore, we do not think that these findings have strong diagnostic value, especially for the purposes of a medico-legal judgment. This is another key-point because, unfortunately, in the absence of a pre-autopsy hypothesis, histological investigations could often be the only source of evidence for a fatal air embolism diagnosis.
In conclusion, almost surely without pre-autoptic TC, we would have missed the right diagnosis.
If some rare causes of death are not suspected before the autopsy, the opportunity for the right forensic diagnosis can be completely missed. This case report illustrates how autoptic findings can be unreliable, because of bizarre post-mortem changes (reabsorption of intra-cardiac gas vs. conservation of intra-cranial gas).
So, in tune with other authors’ way of thinking,12–14 we conclude that early post-mortem imaging could be very useful to detect rare cause of death, to guide autopsy, and to avoid post-mortem wrong diagnosis, especially where autopsies are ordered several days after death, as in our experience.
Despite the case presented, as pointed out by Cole et al., CT should be carried out within one or two hours of death because post-mortem gas production can be rapid. 15 The practicality of obtaining such information for deaths occurring outside of hospital is highly questionable, but for in-hospital deaths, it is often possible and advisable, especially with the prospect of causative medical malpractice.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.