
Abstract
Air embolism (AE) is considered a rare event and can be either iatrogenic or traumatic. Various post-mortem methods to detect AE exist, of which radiology is preferred. The presence of air in the heart can be demonstrated using special dissection techniques where the heart is opened under water or by needle puncture from a water-filled syringe. Three cases of blunt-force head injury are presented herein, with AE being diagnosed by conventional radiography using a Lodox Statscan® full-body digital X-ray machine in all cases. This case series demonstrates that AE due to blunt-force trauma to the head and sinuses might be under-recognised in the forensic post-mortem setting. It also highlights the importance of radiology in diagnosing AE post-mortem, especially where the results of post-mortem techniques might be unsatisfactory.
Introduction
Air embolism (AE), also known as vascular air embolism, is the ingress of air into the circulation and can either be arterial or venous. 1 Various techniques exist to diagnose AE post-mortem.2–8 Radiology, especially computed tomography (CT), has proven to be superior in diagnosing AE by demonstrating the ingress of air into the circulation3,4,9 and differentiating post-mortem decomposition artefact from true pathology. 10 However, not all medico-legal mortuaries might be equipped with CT technology and must rely on plain radiography.
Currently, in South Africa, there is no medico-legal mortuary that has a CT scanner, and many facilities lack conventional plain-film radiography equipment.
Case reports
Herein, three cases are presented with suspected AE detected with radiographical imaging at the Ga-Rankuwa Forensic Pathology medico-legal mortuary in Ga-Rankuwa, South Africa, using a Lodox Statscan® full-body digital X-ray machine. An anteroposterior (AP) view was used to diagnose AE. Death occurred at the scene, with no history of medical interventions such as intravenous line placement. The cases described all occurred in the winter months in South Africa, and the bodies were refrigerated at 4℃ as soon as they arrived at the medico-legal laboratory. All bodies examined appeared to be well preserved without signs of decomposition of the external surface of the body or the organs. X-ray examination did not show any other features of decomposition artefacts of the soft tissue or organs.
Case 1
A 46-year-old male was involved as a pedestrian in a road traffic accident. Lodox Statscan® revealed the presence of air in the right heart chamber (Figure 1), as well as extensive fractures of the facial bones. On external examination, there were lacerations at the corners of the mouth. The vault and base of the skull were intact. However, multiple facial (maxillary and mandibular) fractures were present. Autopsy examination did not demonstrate intracranial pathology. At autopsy, AE was detected using a water-filled syringe. The cause of death was stated as blunt-force facial injuries.
Chest radiograph showing a large area of air in the right heart chambers.
Case 2
A 13-year-old male presented with a history of a fence-like structure falling on top of him. Lodox Statscan® showed air in the right side of the heart (Figure 2). The external examination showed a large laceration measuring 25 cm × 13 cm on the left frontal, parietal and occipital areas of the scalp. Brain matter was extruding from the cranial cavity through the scalp laceration. The entire vault and base of skull showed numerous comminuted fractures. The normal architecture of the brain was distorted and was soft and friable on handling. An AE test was performed by opening the heart under water. No air could be demonstrated. The cause of death was stated as head injury.
Radiograph of the chest with air in the right side of the heart.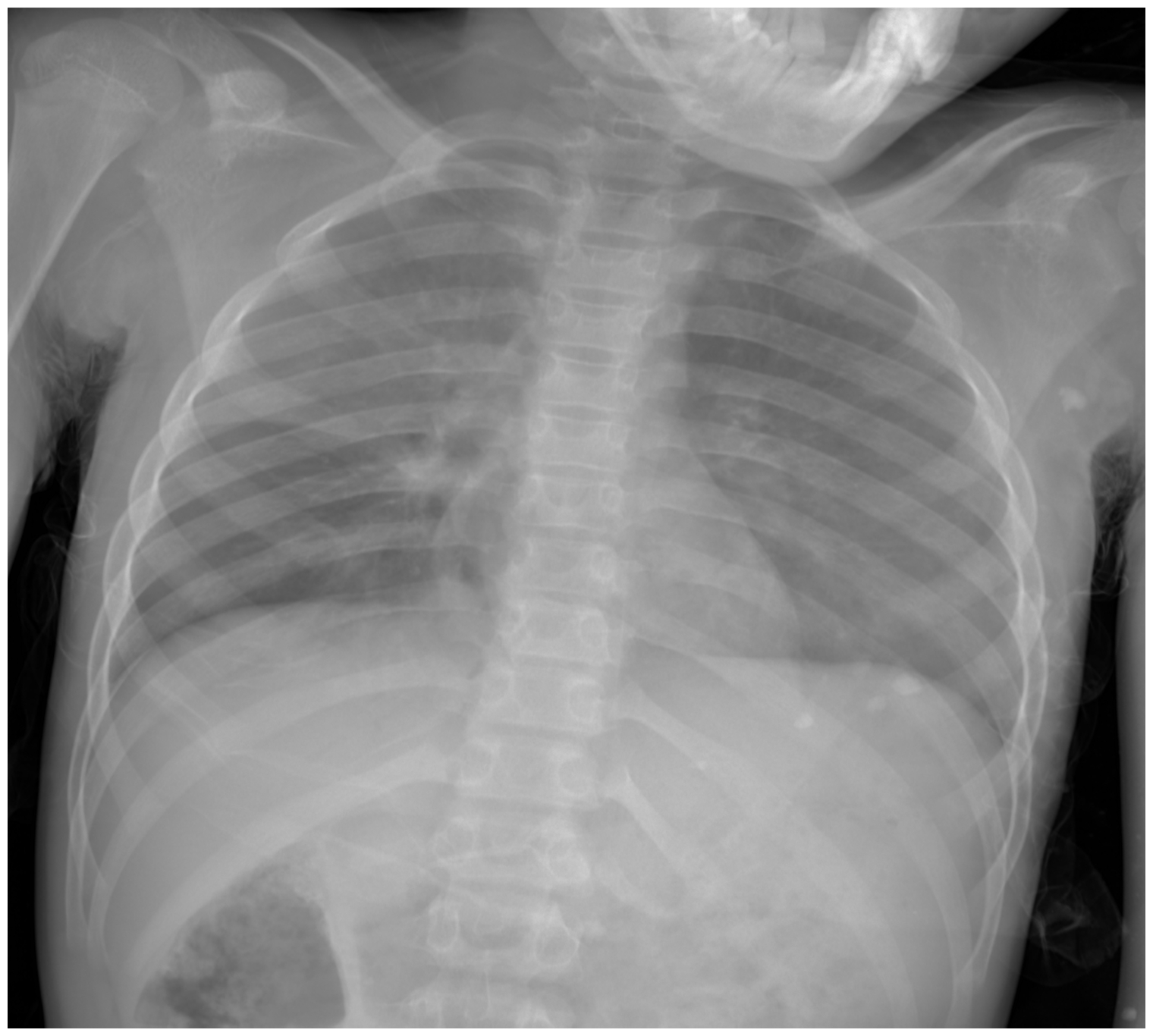
Case 3
A 23-year-old male was involved in a road traffic accident as a pedestrian. Lodox Statscan® revealed a translucency in the right heart chambers which was highly suggestive of air (Figure 3). The external examination showed multiple blunt-force injuries to the face. The vault and base of the skull were intact. A fracture of the mandible was present. Internal examination revealed multiple blunt-force injuries, including contusions of the lungs, heart and brain. The right heart chamber was opened under water, but the presence of air could not be demonstrated. The cause of death was stated as multiple injuries.
Chest radiograph showing the presence of air in the right side of the heart.
Discussion
AE occurs when there is an injury to a vessel, typically a vein, which serves as the point where air enters the circulation. A pressure gradient is needed for air to enter the body, and circulation is necessary to carry air to the right heart chamber and pulmonary trunk. 2 The majority of air emboli are venous and affect the right heart circulation. 11 However, arterial air emboli can occur due to pulmonary lacerations or barotrauma, with air travelling to the coronary arteries or cerebral arteries. 2 Common causes of AE in the medico-legal setting can include surgical12,13 and therapeutic procedures such as intravenous infusion, 3 or during percutaneous transthoracic needle biopsy, 14 criminal abortion, 15 dysbaric barotrauma seen in scuba divers 16 and blunt-force injury to the head.4,5,9,17 The forensic pathologist should have a high index of suspicion in the above-mentioned cases, and AE testing should be done at autopsy.4,5 It is not routine practice in most medico-legal mortuaries in South Africa to test for AE in cases of blunt-force injury to the head. It is noted in the literature that neurosurgical procedures have a propensity to cause AE, with air entering the cranial sinuses.5,18 Skull fractures can lacerate the dural sinuses, with air entering the venous circulation.9,17
The diagnosis of AE at post-mortem can be made using radiography and through special dissection techniques where the heart is opened or punctured under water.2–8 CT is now more commonly used to detect AE.3,4 This has the advantage of not only demonstrating AE clearly, but also following the route of entry of air into the circulation.3,4 The disadvantage of CT imaging is that not all medico-legal facilities/mortuaries are equipped with this technology. However, conventional plain radiography can still be used if CT is not available. 2 In the early 1950s, Taylor concluded that radiology is a useful adjunct to autopsy examinations in cases with AE. 6 Burton and Rutty suggested that an AP and lateral X-ray should be done when diagnosing AE on plain radiography. 7 In the case series by Adams and Guidi, 17 the importance of conventional radiography was demonstrated. In two cases, air could be visualised on chest radiography and at autopsy. However, in the other two cases, the pathologist did not diagnose AE. A subsequent review of the radiographical images revealed AE. 17
The interpretation of AE post-mortem is difficult, and the possibility of artefact versus true pathology should always be considered. In the interpretation of AE on CT scan, the study by Groell et al. who demonstrated the presence of small air emboli in approximately 5% of patients who underwent peripheral venous cannulation should be kept in mind. 19 The interpretation of post-mortem radiology can be more challenging, and consideration should be given to artefacts, especially in cases where the body shows features of decomposition.10,20,21 It is for this reason that the pathologist should recognise post-mortem decomposition changes when interpreting radiological images. Decomposition artefact consists of gaseous collections in the tissue and, according to Swift and Rutty, is usually diffuse on imaging modalities. 20 The state of the body will also provide evidence to differentiate decomposition gas formation from AE. 20 Another method to distinguish between artefact and true air is the analysis of the gas withdrawn from the ventricles. 10 In 2012, Egger et al. from Switzerland concluded that post-mortem gas follows a specific distribution pattern and that there is an association between intracardiac gas and gas in the hepatic parenchyma, which could differentiate between decomposition artefact and AE. 22 Jackowski et al. studied the difference in appearance between post-mortem artefacts and true cardiac pathology. 10 Gas bubbles due to bacterial putrefaction start at the endocardium and progress to form intraventricular bubbles in the non-dependent parts of the ventricles and can fill the cardiac chambers. 10 This is clearly visible on CT imaging, as demonstrated in the figures they provided. However, decomposition artefact can be seen in the rest of the tissue compared with the figure with a true cardiac AE. Saunders et al. demonstrated a case of blunt-force trauma to the head with cardiac AE using a multi-detector CT with a post-mortem interval of 12 hours, and reported that air might be present within a few hours after death. 4 All authors reporting on the presence of air in the heart also reiterate the degree of putrefaction in other organs, especially the liver, can be used as a measure to discern whether the air is indeed artefact.4,10 These studies demonstrate another advantage of CT scan technology, where decomposition artefact is more easily recognised in the heart on CT than it is on conventional X-ray imaging and probably in the early stages of decomposition. Unfortunately, CT images are not compared to conventional radiography to appreciate whether the presence of small air emboli would be visible and to what extent. No literature reports could be found regarding isolated artefacts of air in the heart in radiographs showing decomposition artefact. It is usually clear that diffuse decomposition is present when viewing X-ray images relating to decomposition artefact.
Furthermore, interpretation of radiological images in many facilities is the responsibility of the forensic pathologist. O’Donnell and Woodford stated that interpreting post-mortem radiology can be fraught with difficulty and referred to the misinterpretation of findings by clinical radiologists. 23 Most forensic pathologists are not routinely trained in interpreting radiographic findings, and forensic radiology as a specialised field is still a novel idea in South Africa and many other countries.
If AE is detected in radiography, special post-mortem techniques can be used to demonstrate air during autopsy. These include opening the heart under water,2,6,24,25 using an aspirometer 24 or using a water-filled syringe with needle puncture into the right ventricle.2,7,25 Techniques to detect AE at post-mortem were first described as far back as 1924, 26 with the most recent study done by Bajanowski et al. in 1998 on using an aspirometer to diagnose AE. 24 The use of an aspirometer to diagnose AE is difficult and has many requirements. 24 Not all facilities might have aspirometers, and many pathologists might not be adequately trained in performing or interpreting this technique. Although texts2,7,25 mention the water-filled syringe technique, its origin is unclear. The challenge with diagnosing AE with special dissection techniques is that no standardised method exists, and there seems to be a paucity of more recent studies which critically review the techniques. The reason for the disparity with the radiology and autopsy demonstration is not clear. It is evident that the air visible on chest radiography was substantial. The autopsy was done immediately after X-ray examination, and so dissipation of the air would be unlikely. The techniques were performed within the prescripts described in the relevant literature. There are too many questions and uncertainties about the interpretation, artefacts, possible false negatives or positives when diagnosing AE at post-mortem. There appears to be paucity of literature critically reviewing the diagnosis of AE. It is clear from the literature reviewed that radiography or positive demonstration of air in the heart chambers can constitute a positive diagnosis of AE.4,6,27
The exact volume of venous air necessary in the human circulation to be fatal is uncertain. The mechanism of death in massive AE is due to the mechanical obstruction of the right outflow to the lungs caused by the air forming an ‘airlock’ that alters circulation and results in death.2,9 Kauczor et al. reported on a case of a gunshot wound to the head with an ingress of air from the venous sinuses and cervical veins bilaterally and subsequent air in the right heart chambers. They calculated the volume of air to be 186 mL. 9 Saunders et al. described the case of blunt-force trauma to the head where the assailant used a hammer and a desktop computer, and they illustrated the ingress of air also from the venous sinuses into the vasculature of the neck and thoracic inlet. 4 Cases 1 and 2 demonstrated an intact vault and base of skull. The authors postulate that due to the extensive facial injuries, the ingress of air resulted from tears in the facial blood vessels. This was, however, not proved at autopsy, as these structures are not routinely dissected. The use of post-mortem CT angiography could demonstrate this, but this unfortunately is not available in South Africa. In their case report, Kauczor et al. 9 did not comment on the cause of death and how the AE contributed. In all three cases described in this case series, the blunt-force injuries were severe enough to have caused death. The role of the AE in these scenarios is unclear, but could also, as in the case from Saunders et al., 4 be compounded to an already fatal head injury and could thus be the underlying mechanism of death.
Conclusion
This case series highlights the usefulness of conventional radiological investigations using the Lodox Statscan® in the diagnosis of post-mortem AE in cases with blunt-force head injury, where CT scanning is not available and where autopsy techniques might not be successful.
All three cases had histories of blunt-force trauma. Two cases showed the presence of facial fractures with an intact vault and base of skull. One case had severe comminuted fractures of the vault and base of skull. Our case series supports that blunt-force head injury is a risk factor for developing AE. It further demonstrates the probability of facial fractures as an additional risk factor. Although forensic imaging in the diagnosis of AE is leaning towards CT scan, this case series highlights that the use of imaging modalities, such as the Lodox Statscan®, should not be underestimated in diagnosing AE at post-mortem. In all three cases, radiology indicated air present in the right heart chambers in the absence of other decomposition artefact, but autopsy failed to do so in two cases, thus demonstrating the importance of radiology to demonstrate AE that might otherwise be missed. It is necessary to differentiate decomposition artefact from true pathology. As CT was unavailable, true pathology was considered in view of the circumstances of the deaths, absence of decomposition changes of the body grossly and air in the heart on X-ray without other soft-tissue decomposition artefact.
Our case series demonstrates the importance of a high index of suspicion when examining cases and that AE at autopsy might be under-recognised. Blunt-force trauma is one of the most common mechanisms of injury in the forensic setting and includes cases of assaults, abuse, traffic fatalities and falls. 2 South Africa is one of the countries with the highest homicide rates globally, with a current rate of approximately 33/100,000. This is five times higher than the global average. 28 With these statistics in mind, the question arises of how many cases of AE as an underlying mechanism of death are being missed in cases of blunt-force injury to the head due to a lack of radiography and because it is not routine practice to test for AE in these cases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.