
Abstract
In the United Kingdom, when people die, either a doctor writes an acceptable natural cause of death medical certificate, or a coroner (fiscal in Scotland) investigates the case, usually with an autopsy. An inquest may or may not follow. The concept of ‘natural or unnatural cause’ death is not internationally standardized. This article reviews scientific evidence as to what is a natural death or unnatural death and how that relates to the international classification of deaths. Whilst there is some consensus on the definition, its application in considering whether to report to the coroner is more difficult. Depictions of deaths in terminal care, medical emergencies and post-operative care highlight these difficulties. It secondly reviews to what extent natural and unnatural are criteria for notification of deaths in England and Wales and internationally. It concludes with consideration of how medical concepts of unnatural death relate in England and Wales to coroners’ legal concepts of what is unnatural. Deaths that appear natural to clinicians and pathologists may be legally unnatural and vice versa. It is argued that the natural/unnatural dichotomy is not a good criterion for reporting deaths under medical care to coroners, but the notification of a medical cause of death, using the International Classification of Disease Codes and the medical professional view as to whether it is scientifically natural, is of great value to the coroner in deciding whether it is legally unnatural.
Introduction
The Coroners and Justice Act 2009, brought into force in July 2013, establishes a duty on coroners to open an investigation into a person’s death, if the body is lying in her or his jurisdiction, and she or he has reason to suspect that any of three conditions apply. a One is that ‘the deceased died a violent or unnatural death’ and another is ‘the cause of death is unknown’. b
Coroners can await the results of toxicology or histology tests and then discontinue the investigation, without having to proceed to an inquest. There is a duty to discontinue the investigation (only) if an autopsy reveals the cause of death and the coroner thinks it is not necessary to continue, c but this does not apply if the coroner has reason to suspect that the deceased died a violent or unnatural death or died in custody or otherwise in state detention. d
What is unnatural? No doctor or coroner will have difficulty in identifying a death from injuries in a road traffic accident, or from suspension from the rafters, as being violent and unnatural deaths. Deaths from Paracetamol overdose or an allergic reaction to a prescribed drug may not be violent, but are widely regarded as unnatural. But decisions about deaths after significant delay in providing medical treatment, deaths after surgery or where prescribed medication contributes to the death from a disease are more difficult. The bereaved often have expectations for explanations of an unexpected death of their deceased relative. What is unnatural? Does determining that the death is natural assist the doctor in determining it does not need to be reported to the coroner?
Methods
Articles were searched in Medline and Embase, up to 2017, using terms ‘natural cause of death’ or not; and ‘cause of death’, and ‘classification’. Cause of death and ‘definitions’ and ‘International Classification of Diseases (ICD)’ were searched in Medline only. Relevant articles were selected and those in a foreign language were translated (Dutch and German). Relevant statutes and leading cases in coronial law were selected. ICD guidance on certification and registration of deaths was then reviewed in aspects where there may be unnatural deaths. Articles on international reporting of deaths to coroners were reviewed to establish the use and value of the natural/unnatural death dichotomy. These were then all considered in the light of the contemporary experience of death reporting to coroners in England and Wales.
Review of what are natural and unnatural deaths in medicine
The definition of ‘natural death’ in medicine has been variously considered. It has been defined as Death related to an internal bodily event not influenced by external occurrences; 1 Death caused by disease, completely independent of any legally significant factors; 2 and as unnatural, if caused by external event. 3 There is a consistency here in regarding causative matters external to the body as unnatural, thus embracing treatment interventions.
Few disease events that lead to death happen without significant external impacts or interventions, or potential opportunities to modify or prevent the event. We will look at a range of contexts to see how this definition is applied in certification and notification of the death to the coroner.
Death in terminal care
A Norwegian paper 4 has proposed that acts of abstention by doctors – withholding treatment and providing sedation to control pain that might also hasten death in terminal care – are to be considered normal medical practice and death in these cases is natural. This paper raises the question as to whether natural death encompasses normative practice. A doctor reviewing a death and considering whether to report it to a coroner may take into account that the aim of the physician was no longer to save life. If it was not saveable, it is hard to see how non-intervention can be described by scientists as unnatural. If it was saveable, even for a short time, why should whether or not it was recognized good medical practice make a difference to the doctor’s conclusion that the death was natural, as it was not related to an external occurrence? But the moment that an intervention is made, if it can be said to cause death, it would seem on the medical definition to be an unnatural death, however much the intervention is considered professionally good practice. To say otherwise is not only to fly in the face of the scientific definitions, but also to begin to elide natural death and euthanasia.
The tendency to wish to categorize terminal care deaths as natural may reflect a keenness to avoid the need to report the death to the coroner. But if that is principally to avoid the exercise of legal jurisdiction, a doctor would seem to be in an uncomfortable position, faced with the context of Dr Shipman’s patients or doubts by some about the ethical boundaries of medical practice. It may be helpful to posit that it would be unusual for such cases to be inquested, but that is not the test of whether the death should be reported.
Operative and therapeutic deaths
It must be recognized that deaths of people with diseases being treated are multifactorial; whether or not any individual death is simply ‘natural’ may be very difficult or impossible to determine. Sometimes doctors report a death in hospital from, say, pneumonia secondary to a chronic disease, not mentioning, or putting under II (contributory but not related to I) on a medical certificate of death, an operation that occurred between admission and death. It is not infrequent that a pathologist will report a medical cause of death as ‘Ia Pneumonia Ib a disease (operated on date)’. Presumably the implications of the scientific definition require doctors to make an assessment of the contribution of the operation to death. The omission of the operation or its inclusion in parenthesis would appear to indicate that the operation was incidental to death and invites the coroner to consider the medical view of the death is that it is scientifically either totally or predominantly natural. Similar considerations arise when a patient dies from sepsis secondary to neutropenia caused by chemotherapy or in ‘graft versus host disease’. The insertion of the malignant disease in I rather than II on the Medical Certificate of Cause of Death (MCCD) suggests combined direct contributions from disease and treatment to death, but the meanings are not clear without advice from the doctor.
There is now literature reporting that mortality rates are the same or fall when doctors go on strike, e and with the increasing risks and ambitions of modern medical technology, it can hardly be claimed that external influence of treatment does not cause deaths. There is authority from the scientific world for considering complications of treatment as unnatural: the US Centers for Disease Control and Prevention lists the various causes of death and under a heading if ‘unnatural deaths’ include ‘complications of medical and surgical care’. In Taiwan 5 adverse effects of medical treatment are regarded as an unnatural death, to be notified regardless of whether there was malpractice, but a hospital record linkage study showed only 57% of unnatural deaths were reported.
In Japan, 6 regarding complications of medical treatment as unnatural deaths was not resisted until it became clear it might lead to police prosecution.
Thus there is evidence that doctors do not apply the scientific definition of what is a natural disease when reporting deaths which are caused by treatment or complications of it. It appears that what is an unnatural death in public health is different from what it is in reporting deaths. The only study that could be found to provide reasons for not reporting unnatural deaths was from the Netherlands. 7 Physicians had doubts about whether the cause of death was natural, and one of the main reasons for not reporting was that physicians considered that the judgment of a death after a fall was one for doctors, as it was an incident that fitted in the ‘descending lifeline of patients’ [translated]. The view may be that deaths from complications of properly conducted medical treatment – especially if the patient was high risk – in modern medical practice should be regarded as natural as they were not unexpected. It may be that the cause of death (a fall) death was part of the disease process of ageing. But also it may be to avoid a death investigation and the associated workload and stress to doctors, family and coroner. Whilst families may have different views, it is observed that this is essentially a public interest claim that some unnatural deaths should not be investigated by the coroner.
Classification of sudden infant deaths
Pathologists in the UK in a survey in 2010 8 agreed that Sudden Infant Death Syndrome (SIDS) should be used for unexplained sudden deaths of infants under a year in sleep. Sudden Unexpected Death in Infancy (SUDI) was used to describe deaths with a history of preceding illness, deaths with minor histological abnormalities of uncertain significance and co-sleeping-associated deaths. Most pathologists classified as ‘unascertained’ the situation where there was suspicion of non-natural cause. Consensus existed that co-sleeping should be classified as ‘unascertained’ if the parents had consumed alcohol or used drugs in the preceding 24 hours. The above definitions are not based on scientific criteria, but professional consensus, which was not always present in the study. Paediatric pathologists f usually consider that a negative autopsy, with risk factors for sudden infant death, where circumstances allow on the balance of probabilities the conclusion of a natural death, (classified as SUDI) should be reported as natural deaths. Similarly negative autopsy with no risk factors and nothing to suggest it is unnatural (SIDS) is to be reported as a natural death. If this expert advice is accepted, it would suggest that SIDS and SUDI should be regarded as natural causes of death, unless another factor unknown to the pathologist is in play, when unascertained or unnatural cause should be preferred.
The new Kennedy Guidelines 9 identify in great detail a new classification to achieve consistency, but appear to classify these deaths as Unascertained. The Chief Coroner’s Guidance 10 says that SIDS and SUDI are not medical causes of death and ‘do no more than explain why the coroner has jurisdiction, namely the death is unexplained’. Legally it is hard to see how an interpretation of ‘unascertained’ can be read other than ‘unknown’, g which requires an investigation. If SIDS and SUDI are not recognized as natural causes of death, but as unascertained, there would appear to be no discontinuation of the investigation, h as autopsy has not revealed the cause of death as it is unascertained, and an inquest must follow. This may be regarded by some as unnecessary, if the pathologist has completed all the investigations that the coroner requires. The Lullaby Trust i fears that labelling of these deaths as unascertained may lead to parental fears of a perception that a criminal cause cannot be excluded and lead to a coronial conclusion of ‘open’ rather than ‘natural’. The General Registry Office will be satisfied with a certificate of SIDs or SUDI as a natural death, certified by a coroner. j Not regarding SIDS and SUDI as legitimate natural causes of death by inference might mean that a whole range of sudden death syndromes that pathologists recognize and certify as natural causes of death should regarded as unascertained and also be inquested, as they are conclusions reached by exclusion rather than diagnostic test. What is the best classification of syndromes is clearly a matter for health professionals, and doctors will properly have views as to whether deaths are natural, but the natural/unnatural dichotomy here has not been useful in indicating what the coroner should investigate: rather, a public interest claim appears to have been made that coroners should investigate these deaths, even if they are medically considered on the balance of probability to be natural.
Falls from old age frailty
Byard has described old age frailty as a recognized syndrome, which is not usually identified in forensic situations. 11 There is increasing understanding of the frailty cycle, particularly in old age, where progressive loss of muscle mass (sarcopenia) leads to numerous complications including malnutrition, reduced immunity and increased risk of falls and osteoporosis. This explains most of the fractures in the elderly that are not associated with unusual external stress trauma. And once a disease insult, such as a fracture, has happened, the cycle is accelerated and the likelihood of death is enhanced; 12 the likelihood of dying is 3–5 times compared with pre-frail. The risk of hip fracture is 25 times greater and the mortality from it 35% in 12 months. Thus this is an important natural cause of an elderly mechanical fall. It is crucial this information is entered on the MCCD and given to the coroner, who might otherwise consider the death from a fall unnatural and open an inquest.
Dementia as a cause of dehydration
A study in the Netherlands of 890 nursing home patients with dementia 13 has shown that survival to the final phase of the illness (on a functional status scale) was an independent predictor of cachexia/dehydration as an immediate cause of death. Cardiovascular disorders and acute pulmonary disease were the other two major causes of death. But in these deaths dementia was not cited as the cause of death.
Cachexia is recognized as caused by disseminated malignant diseases, malnutrition and some chronic infections. In the absence of causation by physical disease, dehydration in a hospital or nursing home patient may be considered as a reasonable cause for concern that the death relates to inadequacy of care. This research suggests that it is often an inevitable aspect of the brain disease. So dehydration cannot per se always be an indicator of natural or unnatural death. It is suggested that the threshold of concern that the doctor should use in deciding to report the death is that there is more cachexia or dehydration than expected. A family allegation of poor care should trigger reporting. It is then for the coroner to ascertain whether dehydration is independent from dementia, and whether the death should be investigated as there is reasonable cause to believe that the death is unnatural.
Causes of death associated with psychiatric illness
It is well known that those people who suffer with psychiatric illnesses have an excess mortality from both accidents and non-accidental causes. In a study of 16,871 inpatient and outpatient sufferers, 14 the excess mortality rate from accidents and suicide was low and most of the excess was from deaths referred to as ‘natural’; k the risk is related to the severity of the illness, and is highest for organic psychotic conditions. Deaths from respiratory disorders gave rise to the highest relative risks after accidental deaths, and were responsible for substantial excess mortality amongst in-patients and those with psychotic conditions, including dementia. The largest number of deaths of both sexes was due to cardiovascular conditions, with a 40% excess over expected, mainly due to deaths of in-patients and those with psychosis.
However, it is well known that schizophrenia has a high mortality rate by sudden death 15 and may relate to a cardiac arrhythmia, 16 and/or to specific antipsychotic medication. 17 Many of these deaths are reported to the coroner, who will have to inquest; as the sufferer is under section of the Mental Health Act at the time of death, this is a statutory requirement. 1 Other deaths in psychiatric patients, in the community or after voluntary admission, are notified as there is no known cause of death. Where there is a sudden cardiac death and the causation is not fully understood and probably multi-factorial, determining whether it is natural will be challenging. There is a need for pathologists to be able to advise coroners when there is no medical reason for investigating further, and accepting ‘sudden death in schizophrenia’ syndrome as a natural cause of death. That would need to include consideration of medication, dosage, toxicity and compliance (i.e. post-mortem testing for drug levels), if necessary supplemented by a clinical statement.
Sudden unexplained adult cardiac death
Sudden unexplained adult death may be natural or unnatural, being associated with epilepsy, asthma, chronic alcoholism and cardiac arrhythmias, and mainly in the young. 18 In sudden adult cardiac death (Sudden Arrhythmic Death Syndrome, SADS) there is a negative autopsy. An underlying genetic cause may sometimes be found. This happened in a recent case, m where the High Court ordered a new inquest after the coroner had given a verdict of unknown natural causes, before the genetic diagnosis was returned. n
It raises the question as to what extent a coroner should investigate a natural death with uncertain precise diagnosis. For the genetically related cardiac arrhythmias, the science is moving fast and increasing proportions of victims will be found to have an identifiable defect, and more rapidly. 19 It does appear that natural disease of unknown cause is insufficient for certification by a doctor, but the precise type of disease and whether histology is required is a matter of judgment in each case.
If there has been no intervention in a sudden adult cardiac death, the death is medically natural. But, as the leading charity CRY reports, 20 these deaths of fit young adults, such as in marathons, seem anything but natural to the bereaved. For doctors, these sudden unexpected death cases will almost always be referred to coroners as cause of death unknown, and so whether or not they are natural will not usually fall to clinicians to determine.
Principal finding of the scientific review
This brief survey is illuminating. Although there is a recognized definition of natural death in the medical literature, which is unambiguous in identifying the presence of an external agent or factor as the criteria for finding a death unnatural, when it comes to specific contexts, it is not so easy to apply. In some contexts determining whether a factor is external or what mix of external and internal factors are in play may be very difficult or not routinely possible. Secondly there appear to be differences in usage of what is an unnatural or natural death, related to the issue of what the coroner should investigate.
Review of the International Classification of Diseases
In determining how to record the cause of death, the doctor has the guidance of the International Classification of Diseases and Related Health Problems. 21 It lists all ICD codes for deaths, including many that are not diseases, such as complications of treatments, violent acts or accidents, but it does not define natural or unnatural. Chapter 4 of ICD10 describes the WHO-adopted rules and guidelines for mortality and morbidity coding. The internationally agreed form of death certificate requires entry of the underlying cause of death. The underlying cause has been defined as ‘(a) the disease or injury which initiated the train of morbid events leading directly to death or (b) the circumstances of the accident or violence which produced the fatal injury’. The MCCD allows for entry of underlying cause at Ia of the disease or condition directly leading to death due to Ib, which is due to Ic (the lowest line being the originating (antecedent) cause). o II is reserved for other significant conditions contributing to the death but not related to the disease or condition causing it.
The purpose of the ICD is to permit systematic recording, analysis, interpretation and comparison of mortality and morbidity data collected in different countries (2.1, p.2). That is the professional standard required by all pathologists in providing certification after an autopsy. p It is clear that the Office for National Statistics (ONS) guidance intends that doctors should complete an MCCD whether or not it is an immediately registerable cause. This provides the coroner with key medical advice from analysis of the circumstances of the illness and death of the patient.
Volume 1 of ICD 1022 contains the main classification. This shows that under external causes of morbidity and mortality 23 there are codes for drugs causing adverse effects, misadventures during surgical and medical care, medical device adverse incidents, and procedures as the cause of an abnormal reaction, or later complication, without mention of misadventure at the time of procedure, the latter being Y83 and 84. There are four lists for mortality. 24
Codes V01-Y89 list external causes; q categories are provided for surgical and treatment complications. These may be recorded as the main condition, for example hypothyroidism following thyroidectomy a year ago, or as a supplemental cause, for example postoperative psychosis after plastic surgery. 25 Chapter XX was traditionally used to classify causes of injury and poisoning, but since the 9th Revision, has also provided for the circumstances in which the patient is receiving care. Chapter XXI provides for contact with health services other than disease and includes conditions such as fractured neck of femur from fall on slippery pavement, severe hypothermia – patient fell in garden in cold weather. 26
Certain postoperative complications r can be considered as direct consequences of an operation, unless surgery was carried out 4 weeks or more before death. Thus for pneumonia 10 days after a hip replacement for a fractured femur, both pneumonia and surgery should be in I. Any disease described as embolic may be assumed to be a direct consequence of certain underlying conditions. s An operation on an organ shall be considered a direct consequence of any surgical condition of the same organ, for example with pulmonary infarction due to left pneumonectomy for carcinoma of the lung 3 weeks ago (even if under II) the originating cause is carcinoma of the lung. 27 Senility or old age is usually ignored by coders if there is another condition. 28 There is a rule about linkages that requires the originating cause in Ia occipital fracture Ib fall from epileptic convulsions to be the convulsions. 29 Perinatal deaths are classified by conditions of foetus or mother and also ‘other relevant circumstances’. 30 By analogy, the fall causing a fractured neck of femur, as well as the underlying frailty of old age and osteoporosis, should be in I not II.
Principal findings of the review of ICD coding
This brief survey of coding illustrates how very useful to the coroner are ICD-compliant medical certificates of death. They indicate the medical officer’s opinion about the sequence of events that caused death, whether the cause is not simply a natural disease, but external, and whether certain complications can be considered as direct consequences of surgery.
The ICD does not require doctors to identify deaths as either natural or unnatural. This requirement originated in coronial legislation and it can be seen that scientifically it is not a significant matter to decide and record. Causes of death are often multi-factorial and doctors may not have the full knowledge of circumstances before them to determine whether it is influenced by an external event. But where doctors consider that a death needs to be notified, but is in their view probably natural, it is important that the coroner is informed.
Reporting or notifying deaths to the coroner: England and Wales
Summary of deaths that should be reported to the coroner in England and Wales from MCCD booklet and ONS Guidance for doctors.
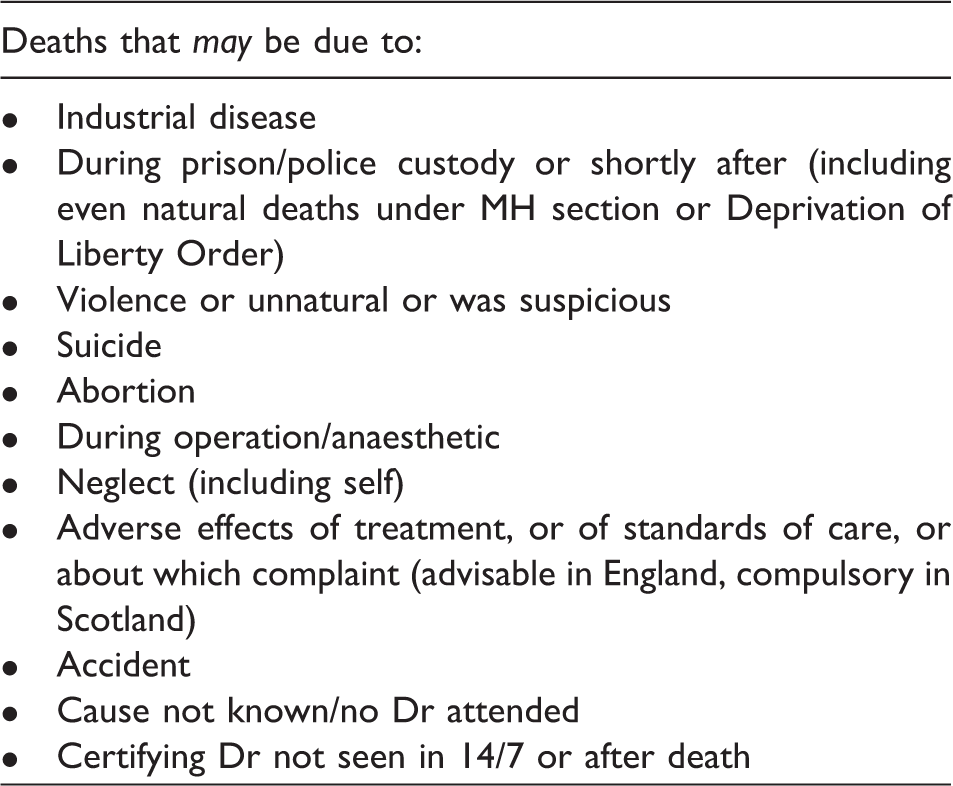
Unnatural deaths must be reported. There is no requirement to state that the death is unnatural. Reporting is expected where there death may be due to adverse effects of treatment, but there is no expectation that the doctor may also state that they view the death as natural. How doctors reach the decision to notify is clearly variable. An old Oxford record linkage study found that in 36% of patients admitted with the primary diagnosis of intracranial injury who died within 4 weeks, there was no reference to the injury on the MCCD. 32 Most UK medical schools do not teach legal aspects of medical practice, and anecdotally it would seem that doctors of all levels understand certification and notification poorly. The current guidance would appear to be insufficient.
The proposed introduction of medical examiners and statutory notification criteria is designed to improve scrutiny of death certification and notification. The suitability of the new notification criteria is considered in a separate article, which concludes that continuing to use natural/unnatural death as a dichotomous criterion for hospital deaths does not improve clarity and is to be avoided, and that the new scheme cannot be relied upon to reduce coronial investigations. 33
Review of international death reporting
An article by Das et al. 34 highlights the fact that international reporting systems do not clarify what is an unnatural death. It illustrates that a bedridden patient dying from pneumonia, weeks after a prosthetic hip replacement for a fracture from a fall at home, might be certified as a natural death by the attending physician but an accident by a coroner or the regional officer recording the death. A review of international processes in 2002 found that in the Netherlands, most states in Germany, and some in the USA, it is required for a doctor to state on the certificate whether the death is unnatural or natural or unexplained. But in only five US states is it required to report a death during a medical procedure or within 36 hours of a hospital stay; internationally, death from a medical procedure is generally classified as unnatural. In Belgium the only distinction is whether there is a medical objection to burial or cremation. The Dutch, however, do not distinguish primary cause, underlying cause and manner of death, as understood by UK physicians. A study in the Netherlands 7 has shown that 12% of nursing home physicians do not consult the “coroner” (pathologist) most of the time when they had doubts about whether the cause of death was natural, and 2% never did.
It would seem that a death of a frail elder after a fall, under current guidance in England and Wales, would need to be reported as it ‘may be from an accident’, whether or not it is natural. However, it does not guide the doctor that also reporting to the coroner that the medical view is that this is a natural death, from ‘old age frailty syndrome’, is of importance.
An Australian study 35 found a coroner referral rate of only 37% of those deaths of patients with an unnatural cause of death. Many were elderly and had multiple diagnoses. Also the referral criteria were different from England and Wales.
A study linking hospital records with death registration data in Taiwan 5 found that 57% of the classified 4086 established or suspected unnatural deaths had not been notified to the coroner. The analysis showed that 71% of injury-related information was reported. For deaths related to fracture of the femur and the effects of a foreign body, many doctors did not report to the coroner (7% and 6%), compared with skull fracture (88%). Deaths related to complications of medical and surgical treatment amounted to 312 but only one was reported to the coroner. The authors speculate that ignorance of what cases should be reported may be one cause. So, clearly, would be different interpretations of what is unnatural.
Principal findings of the review of death reporting
The English and Welsh and international experience points to the lack of usefulness in determining, as a criterion for notification of a death under medical care, whether it is unnatural, but also the value in medical determination of natural death when it is possible to do so. There appears to worldwide underreporting of unnatural deaths in medical care, despite systems generally requiring deaths from complications of medical care and trauma to be reported. There is little articulation of the basis of this. Whilst in part this may relate to training issues, some doctors may view some deaths from complications of medical treatment as natural; for others, the avoidance of an investigation into the death would seem to be a key factor.
Strengths and weaknesses of the study
A weakness of the research is the paucity of relevant articles on what an unnatural death is, and that most articles originate from Northern Europe, especially Germany. Since these countries do not have the same notification regime, nor the same legal criteria for investigation of deaths as in the Coroners & Justice Act 2009, and indeed do not have a similar coroner’s service, there is a gap in academic study. The contexts in which consideration of the naturalness of the death are necessarily selective. No study could be found which identified the how deaths from complications of properly conducted medical care should be regarded scientifically, nor has any measure been made of the variety of views of doctors or patients as to what is a natural medical death. But a strength is that the study has brought together consideration of scientific literature, which is consistent, ICD guidance and coronial death notification criteria, which does not appear to have been done before. Thus a holistic view has been achieved. No other similar review could be found with which to compare this study.
Implications of the reviews
In England and Wales, doctors decide if they can certify the medical cause of death. If they or the Registrar consider that the death may be unnatural or that it is unknown or should otherwise be notified, it should be notified to the coroner.
There is great value of doctors explaining the cause of death to coroners and providing their understanding of natural death processes. In some contexts, such as elderly falls and dehydration of the elderly, the need for the coroner to be provided with antecedent medical causes may not be recognized.
Doctors should explain the underlying assumptions in syndromes that might not be understood by coroners to be recognized natural causes of death, such as SIDS, and such as ‘graft versus host disease’ where the cause of death is not a natural disease, but directly caused by the treatment.
There seems to be a striking difference between the use of the terms natural and unnatural death in the scientific literature and in public health from that apparently used by doctors in reporting deaths under medical care to coroners. In sudden infant deaths there is public interest guidance that some natural deaths require coronial investigation. In some complications of medical treatment there is, in effect, a public interest claim that scientifically unnatural deaths do not require coronial investigation.
In England and Wales there are a large number of bodies and processes investigating, regulating or monitoring the quality of medical care (NHS Trust PALS procedures, NHS England, General Medical Council, Care Quality Commission, Safeguarding Boards, the police), so care is needed in making international comparisons. But how many and what type of investigations coroners should conduct into hospital deaths are policy and legal issues; straining the medical definition of ‘natural’ and ‘unnatural’ deaths is not a preferable way to reduce or increase the number of investigations.
It is laid down in guidance that deaths that may be caused by adverse effects of medical treatment are to be reported to the coroner, but many are not. There may be a variety of opinions of doctors and others as to whether the death is unnatural, which are likely to be mindful of the knowledge that the coroner does not have the discretion not to investigate an unnatural death.
It is the unenviable duty of the coroner to determine, having received notification and advice, whether or not the death may be legally unnatural. A coroner reaches his or her decision as to whether a death is unnatural mindful of the advice, the opinions of interested persons (including the family), the legislation which gives the decision-making power, the legal rules on how to interpret the meaning of the statutory word ‘unnatural’ and the application of the judge-made case law. This process is beyond this study, but how this is applied may be briefly illustrated by considering two scenarios.
In the context of a person who has an emergency operation for a condition which is liable to kill her, and the operation goes badly wrong, even negligently wrong, and the patient dies, the death will correctly be notified to a coroner. The surgeon may well consider it an unnatural death, occurring during surgery and related to the error he made. It is thus prima facie unnatural. But at inquest (not at opening), the coroner must apply the case law of Benton. u Thus the coroner may conclude that a medically unnatural death is natural.
The second scenario is the converse. A patient dies from status asthmaticus; it is prima facie a natural death. Whether or not the corner finds it unnatural will depend on the context. In considering whether or not a prima facie natural death is unnatural, the coroner must apply the test as to whether he or she has ‘reason to suspect that’ v the death may have been due to culpable human failure or neglect. Neglect is a legal term of art, derived from Touche, w with a special meaning in coronial law x and bears no relationship to its use in common parlance or medical discourse. So a prima facie medically natural death can be found by a coroner to be unnatural.
Conclusions and further research
Scientifically it is quite clear that deaths involving external influences are unnatural. But defining what is a natural death in clinical medicine is not simple, and relates to the extent of clinical knowledge and investigation and the advance of scientific knowledge, and is subject to varying views as to whether deaths from normative practice should be regarded as natural. It is not always clearly aligned with ICD coding. Whatever the context, doctors are expected to report deaths which may be due to adverse effects of treatment. Their opinion as to whether or not they are natural will be informing to the coroner, but not determinative as to whether there is an investigation, as that is a matter for the coroner.
The legal definition of unnatural is similarly complex and involves statutory interpretation and application of case law, which cannot properly be performed by doctors. It is inevitable and not to be deprecated that doctors may consider a death unnatural and the coroner concludes otherwise and vice versa.
Thus it is submitted that, having considered the international experience, medical and legal literature, a test as to whether or not the death is prima facie unnatural is insufficient as a criterion for notification of deaths under medical care to coroners. But informing coroners of what doctors consider is medically a natural death is of great value to the coroner. Promoting the adoption of ICD codes for death certification and notifications to the coroner will be of benefit to public health, clinical practice and coroners.
Recognition is needed by policy makers that debates about whether deaths of patients whilst receiving medical treatment are natural or unnatural are often actually not about their naturalness, but about whether there should be a coronial investigation. The use of the natural/unnatural death dichotomy to determine the issue of which patient deaths should be investigated is unhelpful, and will lead to poor death certification and inconsistency. Further research is needed into the state of coronial law in deciding whether notified deaths of patients are unnatural, and into the reasons for variations in death reporting rates. At times of considerable public expenditure constraint and high expectations of bereaved families, and mindful of the evidence suggesting that many deaths related to treatment are not reported, there needs to be a public policy debate about which deaths of patients receiving medical treatment are in the public interest to be the subject of coronial investigation and inquest.
The adequacy of the current coronial system, including the possibility of further coronial law reform would then need to be reviewed.
Footnotes
Acknowledgments
I am grateful for the advice of Sebastian Lucas, Emeritus Professor of Pathology, Dept of Histopathology, Guy’s & St Thomas NHS Foundation Trust Hospital, London (GSTT), who has suggested amendments to an earlier copy. I am also grateful to Dr Andreas Marnerides, paediatric pathologist, also at GSTT, for his advice on sudden deaths in infants. The author generated the idea for the research, conducted it and remains the guarantor.
I am grateful for the translation of articles from Dutch by Ms Emma Cherim and from German by Ms Peggy Farooqi.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.