
Abstract
Gastrointestinal conditions are a less common cause of sudden unexpected death when compared to other conditions such as cardiovascular conditions, but they are equally important. Various congenital and acquired gastrointestinal conditions that have resulted in sudden unexpected death are discussed. The possible lethal mechanisms behind each condition, along with any associated risk factors or secondary diseases, have been described. Through this article, we aim to highlight the need for physicians to prevent death in such conditions by ensuring that subclinical cases are diagnosed correctly before it is too late and by providing timely and efficacious treatment to the patient concerned. In addition, this review would certainly benefit the forensic pathologist while dealing with cases of sudden unexpected death due to gastrointestinal causes. This article is a review of the major gastrointestinal causes of sudden unexpected death. In addition, related fatal cases encountered occasionally in forensic autopsy practice are also included. There are several unusual and rare causes of life-threatening gastrointestinal bleeding that may lead to sudden unexpected death to cover all the entities in detail. Nevertheless, this article is a general guide to the topic of gastrointestinal causes of sudden unexpected death.
Introduction
Sudden unexpected death comprises one of the most important and worthy investigation case profiles in emergency medicine and forensic pathology.
The principal causes of sudden unexpected death vary in different age groups. 1 The predominant causes of sudden unexpected death in adults and the elderly are atherosclerotic coronary artery disease and hypertension. 2 Sudden unexpected death in infancy is usually caused by infections or sudden infant death syndrome. 3
Gastrointestinal conditions1,2,4–63 are a less common cause of sudden unexpected death compared to various other conditions. This is because gastrointestinal pathologies frequently present with symptoms which immediately attract medical attention. On rare occasions, they do present with less observable signs and symptoms which might go unnoticed by the physician. Sometimes, gastrointestinal pathologies may also remain untreated if the individual was living all alone and did not get a chance to call for help or if the individual refused medical help.
In the present review, we define ‘gastrointestinal’ causes as those either directly or indirectly related to the stomach and intestines only, and we exclude all other abdominal pathologies and oesophageal conditions. Conditions related to the accessory organs of digestion, the liver, gall bladder and pancreas are excluded. Direct causes relate to the organs, the stomach and intestines per se. Indirect causes relate predominantly to the vasculature of the stomach and intestines.
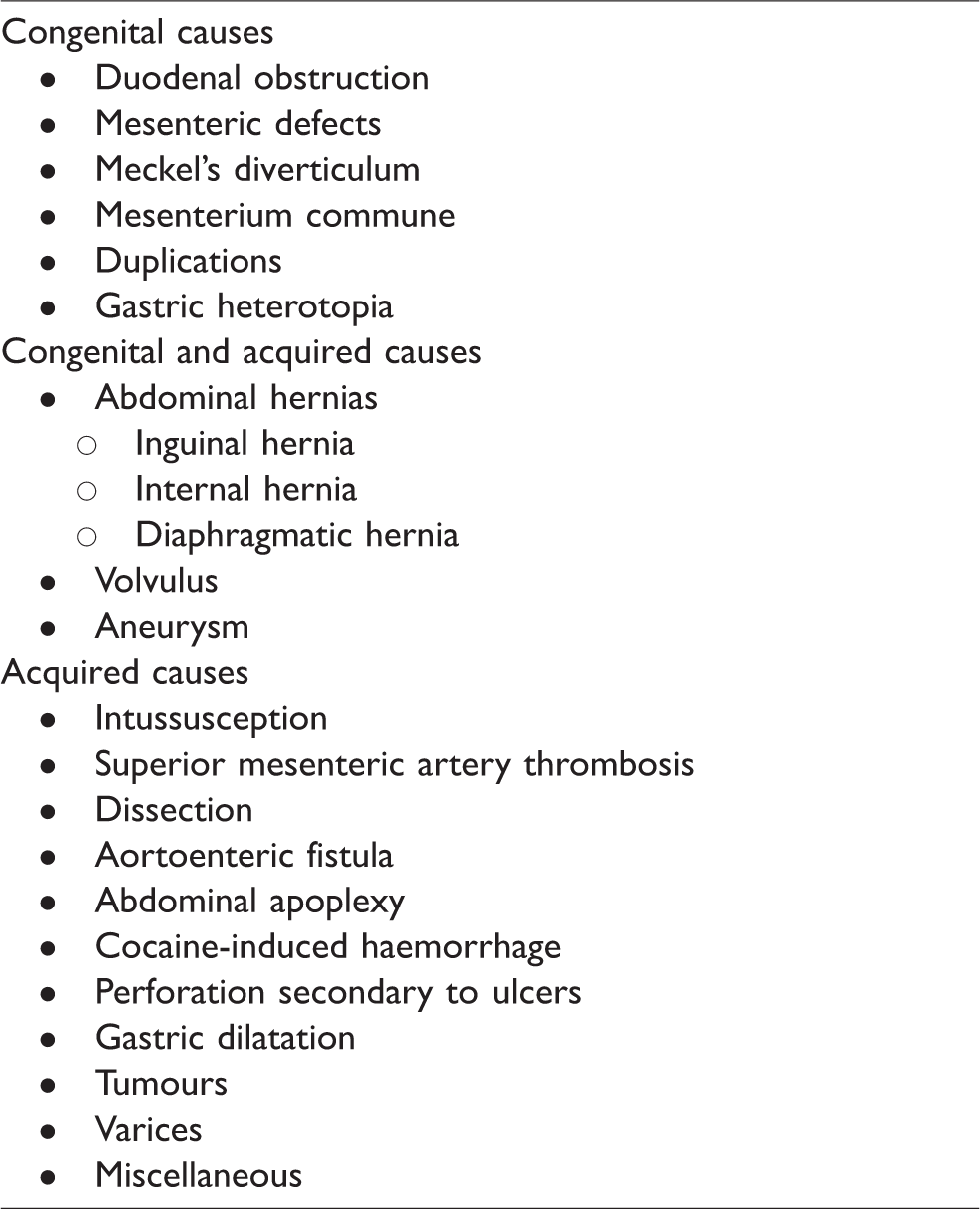
Gastrointestinal causes of sudden unexpected death include various congenital abnormalities and acquired conditions (Table 1). To our knowledge, currently, only case reports and audit articles are available on the topic, and no comprehensive review article describing the relevant pathologies has been previously published.
Gastrointestinal causes of sudden unexpected death.
This article discusses the various congenital and acquired gastrointestinal conditions1,2,4–63 that have resulted in sudden unexpected death. The possible lethal mechanisms behind each condition, along with any associated risk factors or secondary diseases, are described in detail. In addition, related fatal cases encountered occasionally in forensic/medico-legal autopsy practice are also included in the present review.
Congenital causes
Duodenal obstruction
Duodenal obstruction, which includes both stenosis and atresia, has an incidence of 1 in 10,000 live births and is considered the most common intestinal obstruction in neonates. 4 Duodenal obstruction is just one example of a congenital condition of the gastrointestinal system that can cause sudden and rapid death. As suggested by Tandler, duodenal obstruction is caused by failure of vacuolisation and recanalisation after the solid stage of duodenal development. 5 However, this has been questioned many times, and the aetiology is now considered to be much more complex because of the increased association with other congenital anomalies. Associated congenital anomalies have been discovered in about 50% of the cases, and around 30% of these are associated with trisomy 21. 4 There is an increased incidence of prenatal deaths, even in the presence of a normal karyotype, indicating that duodenal obstruction is an extremely serious condition that can cause sudden death prenatally as well as postnatally. The obstructions are most commonly found in the second and third parts of the duodenum and are located in close proximity to the opening of the bile duct. 4 These obstructions may increase the level of foetal serum bile acids. Primary bile salts such as taurochlorate have been found to alter the rate and rhythm of cardiomyocytes and affect the foetal heart rate. 4 Additionally, reflex vagal cardiac inhibition due to distension of the upper gastrointestinal tract has also been described as another rapid cause of death due to duodenal obstruction. 4
Mesenteric defects
Although extremely rare, sudden death due to congenital mesenteric defects has been described in the literature. 6 These are mostly asymptomatic but may give rise to symptoms if complications such as internal hernias arise. Therefore, it is important to consider mesenteric defects as a differential diagnosis for a paediatric patient presenting with acute abdominal pain. These defects may arise in a variety of locations but are most commonly found in the mesentery near the terminal ileum. 7 These are usually round or oval in shape and can have a diameter of >10 cm. 6 The exact aetiology of these defects has not been determined. However, one theory suggests that these defects occur either due to the expansion of a region of necrosis or because of an incomplete regression of the dorsal mesentery. 8 Due to peristaltic motility, intestinal loops can at times herniate through the defect, and as a result, fluid and air can get trapped in the intestine. Death may ensue due to ischaemia of the herniated part of the intestine if the distention is severe or due to necrosis followed by septic complications.
Meckel’s diverticulum
Meckel’s diverticulum is an uncommon cause of intestinal obstruction. However, it is the most common congenital anomaly of the small bowel and occurs when the vitelline duct does not become completely atretic during the fifth week of embryonic life. Meckel’s diverticulum can be difficult to diagnose, as many of the symptoms, such as abdominal tenderness, abdominal pain and vomiting, can occur in several different conditions. Most Meckel’s diverticulae are clinically silent, and only about 4% of patients develop symptoms. 9 They are mostly either discovered incidentally during barium studies, laparotomies or at autopsy or when complications such as perforation, bleeding or haemorrhage arise from the diverticulum.
The vitelline duct is supplied by two vitelline arteries. Rarely, fibrous derivatives of these vitelline arteries become connected from the tip of a Meckel’s diverticulum to the mesenterium, resulting in the formation of a mesodiverticular band. Mesodiverticular bands are associated with an increased risk of mortality and can cause sudden death. Small bowel loops are highly susceptible to incarceration and subsequent infarction if they herniate below the mesodiverticular band. Additionally, severe dehydration is very likely to occur due to intestinal obstruction, and this may lead to circulatory collapse.
Littre hernia is the protrusion of a Meckel’s diverticulum through any hernial orifice. These hernias are uncommon, with <50 cases reported in the 20th century. 10 Littre hernias are usually harmless and have minimal clinical manifestations, as there is no obstruction to intestinal contents because of a patent ileal lumen. Therefore, the only clinical findings may be a mass and tenderness if the hernia is incarcerated. The usual sites are inguinal (50%), femoral (20%), umbilical (20%) and elsewhere (10%). 10 Unexpected death occurs rarely in cases of infarction and small bowel obstruction. 10
Mesenterium commune
Mesenterium commune is caused by the interruption of intestinal rotation during foetal development. 11 The malpositioned intestines cannot develop a normal mesentery and are susceptible to volvulus. This is a serious complication and, when diagnosed late, can lead to sudden death as a result of haemorrhagic infarction of the intestinal wall.
Duplications
Duplications are congenital cystic or tubular structures lined by an inner mucosal membrane present in the intestinal tract that have a common muscular wall with the bowel segment. 12 These can be located in any part of the intestinal tract but are most frequently found at the ileum and ileocaecal portion of the caecum. 12 Duplications can become symptomatic in infants when they compress the surrounding intestinal lumen causing obstruction, or they may act as a nidus for an intussusception or a site for volvulus. Duplications should always be considered in the list of differentials for an infant presenting with gastrointestinal complaints. Patients may present with non-specific signs and symptoms such as abdominal pain, vomiting, palpable abdominal mass and bloody stool. 12 An abdominal ultrasound can be helpful in diagnosing this condition before complications arise. Sudden death as a consequence of duplication cysts is very rare. Deaths have been thought to occur as a result of acute dehydration secondary to accumulation of fluid in the intestine and numerous episodes of vomiting and diarrhoea. 12
Gastric heterotopia
Gastric heterotopia is a rare occurrence, with the majority of lesions located in the duodenum. Gastric heterotopia has been associated with duplication cysts and may lead to ulceration, perforation and gastrointestinal bleeding, all of which can be life-threatening situations and can lead to sudden death.12,13
Congenital and acquired causes
Abdominal hernias, volvulus and aneurysms may be either congenital or acquired. A case of sudden unexpected death due to clinically undiagnosed neoplastic disease in a 11-year-old child is described under the section on "tumours". 46 In this case, a gastric tumour of adult-type was diagnosed at autopsy. 46
Abdominal hernias
Inguinal hernia
An inguinal hernia is the protrusion of an organ or part of an organ through the inguinal canal. It can be either reducible or irreducible. In an irreducible hernia, the contents of the hernia sac cannot be replaced into the abdomen. An irreducible hernia is associated with complications such as obstruction and strangulation. In a strangulated hernia, the blood supply to the contents of the sac is compromised, which then become ischaemic or infarcted. The loop of the gut may also become strangulated in the inguinal hernial sac. Therefore, a strangulated inguinal hernia is considered to be a surgical emergency. Mortality increases in the absence of timely surgical intervention. Incidences of sudden death can be decreased if proper timely treatment is provided.
Menezes et al. 14 describe a case of potentially preventable sudden unexpected death due to a gastrointestinal cause wherein a 60-year-old was found lying dead near a place of worship. Following an autopsy, the cause of death was opined as that consequent to small intestinal strangulation caused by herniation of a loop of the small intestine in a right-sided inguinal hernial sac (Figures 1 to 3). 14 In such a case, the mechanisms of death may be quite complex and include fluid and electrolyte imbalance, intestinal haemorrhagic infarction and marked translocation and systemic exposure to aerobic and anaerobic bacteria with their associated toxins.

Inguinal hernia evident as scrotal swelling with the buried penis.Source: Reproduced with permission from Menezes et al. 14

Bowel loops dissected out from the inguinal hernial sac. Source: Reproduced with permission from Menezes et al. 14

A partly inflammatory and partly gangrenous segment of the herniated intestinal loop. Source: Reproduced with permission from Menezes et al. 14
Internal hernia
An internal hernia is the protrusion of an internal organ through the peritoneum or mesentery. Internal hernias are categorised according to the location of the defect and fall into six distinct groups: transmesenteric hernia, hernia through the foramen of Winslow, paraduodenal hernia, pericaecal hernia, transomental hernia and paravesical and pelvic hernia. 15 Internal hernias may cause obstruction, strangulation and gangrene of the intestine. If left untreated, the mortality rate is >50%. 8 These mostly arise as a complication of gastrointestinal surgery in case of the elderly. These elderly victims usually have an underlying disease such as diabetes mellitus, chronic renal failure or gastrointestinal cancer. 15 Transmesenteric hernia is the most common type and is difficult to distinguish from other benign conditions, especially in the presence of minimal symptoms. Open or laparoscopic examination is the only way to form a definitive diagnosis of transmesenteric hernia. Hence, a delayed or wrong diagnosis increases mortality in patients and may result in sudden death. The mechanism of death may be either hypovolaemic shock due to severe vomiting or septic shock as a postoperative complication.
Diaphragmatic hernia
Congenital diaphragmatic hernia is a rare anomaly with high morbidity and mortality. While congenital diaphragmatic hernias mostly present in neonates, a small percent of patients may present with the condition after the neonatal period during early childhood. Chhanabhai et al. 16 report a case of sudden unexpected death due to congenital diaphragmatic hernia in a previously healthy 22-month-old child. The cause of sudden death is related to the sequelae of sudden cardiopulmonary compression owing to a sudden herniation of the abdominal contents into the left thoracic cavity. 16 Sudden unexpected death due to congenital diaphragmatic hernia has also been reported in previously healthy 2-, 4- and 24-month old children. 17 The predisposing factor for the sudden herniation of abdominal contents through the diaphragmatic defect into the left thoracic cavity is the increased intraabdominal pressure from coughing, vomiting or straining during a bowel movement. Vandy et al. 18 describe an autopsy case of death due to congenital diaphragmatic herniation of the abdominal contents into the left thoracic cavity in a 30-month-old child. In this case, the child had presented to the hospital with acute abdominal pain and vomiting. 18 In addition to the diaphragmatic hernia, the autopsy revealed an associated gastric volvulus with necrosis and rupture. 18 Navarro-Crummenauer et al. 19 describe a case of death due to previously undiagnosed congenital diaphragmatic hernia in a 14-month-old child wherein the autopsy revealed herniation of the terminal ileum, caecum, colon and greater omentum into the left thoracic cavity causing significant compression of the left lung. In this case, although the child had presented to the hospital with acute abdominal pain and vomiting, the cause of death was opined as respiratory insufficiency based on the autopsy findings. 19 Navarro-Crummenauer et al. 19 stressed upon the importance of considering a late manifestation of congenital diaphragmatic hernia in children presenting with recurrent gastrointestinal and/or respiratory symptoms.
Congenital diaphragmatic hernia presents rarely in adulthood. Moreover, sudden death secondary to a posterolateral Bochdalek hernia, a type of congenital diaphragmatic hernia, is even more rarely reported in adults.20–22 Chui and Tan report a case of sudden death resulting from a perforated gastric ulcer in an incarcerated Bochdalek hernia in an adult. 20 Salacin et al. 21 report another case of Bochdalek hernia leading to sudden death in adulthood. In this case, Bochdalek hernia was first diagnosed at autopsy. 21 Another case of sudden death due to a previously undiagnosed congenital diaphragmatic hernia in an adult is reported by De-Alwis and Mitsunaga. 22 They stress the importance of early diagnosis of such anomalies followed by prompt surgical treatment in order to avoid fatalities. 22 Kato et al. report a case of sudden death secondary to congenital diaphragmatic hernia in a 43-year-old man wherein the lethal mechanism was attributed to compromised respiration from the collapsed left lung secondary to herniation of the abdominal viscera into the left thoracic cavity. 59
Volvulus
Volvulus is the cause of 1–7% of large bowel obstructions in Western countries. 23 It most commonly occurs in the ileocaecal and sigmoid regions. It presents as a surgical emergency when there is obstruction of the intestine and compromise of blood supply due to twisting of the intestine around a mesenteric attachment. Ischaemic necrosis of the twisted part with gangrene may occur, followed by death due to sepsis and electrolytic imbalance. Patients may be predisposed to volvulus due to several factors such as a malrotation of the midgut, large redundant sigmoid colon on a long narrow-based mesentery or chronic constipation with laxative use or high-fibre diet. 23 Congenital midgut volvulus is also reported in the literature. 57 This condition can be life threatening to the newborn.
Sigmoid volvulus is primarily seen in elderly patients with pre-existing dementia and other psychiatric conditions. The mortality rate can reach up to 50% in such patients. 23 Unexpected death most commonly occurs in elderly patients because of minimal symptomatology, presence of multiple unrelated conditions, communicating disabilities and their general reluctance to see the doctor.
Omond and Byard report an autopsy case of death resulting from an acute gastric volvulus in a 55-year-old woman. 58 The lethal mechanisms in such cases of acute gastric volvulus include peritonitis resulting from gastric perforation due to gastric wall necrosis from a compromised gastric blood supply and overwhelming distension of the stomach from swallowed air and fluid, hypovolaemic shock resulting from obstruction or compromised respiration resulting from significant left lung compression due to the gastric volvulus pushing the left diaphragm upwards. 58
Aneurysm
An aneurysm is a permanent pathological localised dilatation of an artery. 24 Splanchnic aneurysms occur at numerous sites and are rather common features appearing in 0.1–2% of the population. 25
Around 60% of these aneurysms are found in the splenic arteries, which is by far the most common site, followed by 5% in the gastric arteries. 25 The pathogenic mechanisms behind the formation of splanchnic aneurysms may include inflammation, arteriosclerosis, congenital malformation and medial degeneration.
Symptoms can range from asymptomatic to non-specific gastrointestinal disorders and recurrent pain. However, their rupture can result in intraperitoneal or intragastric haemorrhages with high mortality rates and sudden death.25,26 Moawad et al. 63 report a case of life-threatening gastrointestinal haemorrhage due to the intragastric rupture of a splenic artery aneurysm with erosion into the stomach.
Aging, arteriosclerosis as a result of pre-existing hypertension, medial degeneration secondary to Marfan’s syndrome, pregnancy, congenital cardiovascular diseases and trauma are considered predisposing factors for aneurysm formation. 26 Complications of aneurysms include thrombosis, embolisation and dissection which can also be a cause of sudden death. 24
Acquired causes
Intussusception
Intussusception is a process in which a segment of the intestine invaginates into another segment of the intestine, causing bowel obstruction. It can also compromise the blood supply to the affected part of the intestine which can cause perforation, infection and necrosis of the affected tissue. Intussusception is mostly idiopathic but several pathologies have been associated with it such as Meckel’s diverticulum, omphalomesenteric duct abnormalities, mesenteric defects, enlarged mesenteric lymph nodes, polyps, neoplasms, mesenteric cysts and mural haematomas. It is a major cause of intestinal obstruction and the second most common cause of acute abdominal surgical emergency in children. 27 Signs and symptoms are usually detectable and are those of intestinal obstruction. However, they may be completely absent or quite subtle. Around 13–20% children experience ‘painless intussusception’ without any discomfort or colic, and therefore if death occurs, it will be sudden in nature and only determined at autopsy. 28 Death occurs because of a combination of factors such as intestinal obstruction causing peritonitis, electrolyte imbalance or compromised blood supply followed by intestinal infarction and shock.
Superior mesenteric artery thrombosis
Acute intestinal ischaemia precipitated by superior mesenteric artery thrombosis has a high mortality of about 60–75%. 29 It can present as a rare complication of chronic cocaine use, and the diagnosis is extremely difficult to make. The mechanisms behind cocaine-induced tissue damage are very well understood, and it is known that cocaine causes arterial vasoconstriction, activation of intravascular thrombosis cascades and accelerated atherosclerosis. Sudden death in a young patient with a history of abdominal complaints should raise suspicion for stimulant drug abuse and abdominal visceral artery thrombosis.
Dissection
Dissection is defined as penetration of blood into the vessel wall through an intimal tear, normally involving the aorta, but can also involve visceral arteries. 24 The predisposing factors for a dissection are the same as those for an aneurysm and include hypertension, Marfan’s syndrome, trauma, pregnancy and congenital cardiovascular diseases.
The difficulty in diagnosing and promptly treating a ruptured artery dissection, due to its non-specific symptoms and rapid evolution into shock, is a big contributing factor to sudden death. 24
Gastric dissecting aneurysms are very rare lesions with the same risk factors as splenic artery dissections. These can arise in intramural as well as extravisceral gastric vessels. 26 Intramural dissecting aneurysm rupture results in haemorrhage into the gastric lumen leading to haematemesis, whereas extravisceral dissecting aneurysm rupture results in haemoperitoneum. 26 In extravisceral gastric dissecting aneurysm rupture, the initial haemorrhage may occur in the lesser omentum or subserosal space. This may eventually lead to a ‘free rupture’ into the omental bursa or peritoneal cavity after a tear of the serous membrane. 26
In these dissecting ruptures, the shock symptoms follow a biphasic pattern. The haemodynamic status may be stable in the initial phase, and then quickly worsens due to massive free bleeding several hours afterwards. The term ‘double rupture phenomenon’ has been coined for this phenomenon and is thought to be the mechanism of sudden death. 26 It has been observed in both splenic and gastric dissecting aneurysms ruptures.
Aortoenteric fistula
Aortoenteric fistula (AEF) occurs due to spontaneous erosion of an abdominal aortic aneurysm into the intestine and may cause sudden unexpected death. It is a rare aetiology of upper gastrointestinal bleeding and most commonly occurs at the third and fourth portion of the duodenum. 30 Early and preoperative diagnosis is extremely difficult, and the mortality rate is almost 100% if the surgery is delayed. 30
Described as ‘uniformly fatal’, AEF, an uncommon cause of upper gastrointestinal tract haemorrhage, with a reported incidence of 0.07%, most often results in sudden unexpected death. 31 As described by Sir Astley Cooper in 1829, AEF presents with a classic triad of massive gastrointestinal haemorrhage, pulsatile abdominal mass and abdominal pain. 31 A few weeks before presenting with the classic triad, patients with AEF usually experience self-resolving, small volume gastrointestinal haemorrhages also known as ‘herald bleeds’.
Causes of AEF include aortic infections (tuberculosis, syphilis, fungal and septic aortitis), peptic ulcer disease, abscess, gastrointestinal malignancies, lymphoma, penetrating/eroding foreign bodies, radiotherapy or previous aortic surgery. 31
Sudden unexpected death in the elderly as a result of aortoduodenal fistula–related haemorrhage associated with penetrating atherosclerotic ulcer or atherosclerotic aneurysm of the abdominal aorta is reported in the literature.31,32
Abdominal apoplexy
Abdominal apoplexy or idiopathic spontaneous intraperitoneal haemorrhage is a rare but important cause of sudden death. Conditions predisposing to spontaneous haemoperitoneum include liver disorders, splenic disorders, gynaecological disorders, haematological disorders, vascular disorders, inflammatory disorders and coagulation disorders. Bleeding can be retroperitoneal or intraperitoneal and is associated with hypertension in 33–50% cases and atherosclerosis in 80–87% cases. 33 Haemorrhage is usually preceded by a vessel rupture, most commonly at the site of an aneurysm. The vessels most commonly involved are the middle colic artery, pancreaticoduodenal arteries and the gastroduodenal artery.33,61 Abdominal apoplexy due to rupture of the short gastric artery is also reported in the literature. 62 In fatal cases, the source of intraperitoneal haemorrhage may remain unidentified, despite a detailed post-mortem examination of the visceral organs, peritoneal folds and major abdominopelvic vessels. 33 A thorough knowledge of the vascular anatomy and a meticulous dissection of the vasculature are certainly required to identify the definite source of bleeding at autopsy.
Cocaine-induced haemorrhage
The use of cocaine has been associated with fatal and sudden intraluminal gastrointestinal haemorrhage. 34 Cocaine use can cause intestinal infarction, ischaemia, perforation and haemorrhage. It exerts direct vasoconstrictive effects by enhancing calcium influx across endothelial membranes. Vasoconstriction is further enhanced because of direct sympathomimetic effects of cocaine. The vasoconstriction leads to hypoperfusion and ischaemic infarction of the intestine.
Perforation secondary to ulcers
Peptic ulcer disease and its complications are a significant cause of sudden, unexpected mortality worldwide, particularly in the elderly and chronically ill, with atypical presentations causing a delay in diagnosis. 35 In childhood, fatal gastric rupture secondary to peptic ulcer disease is rarely reported. 36
This fatal and potentially treatable ‘abdominal catastrophe’ is clearly underreported, as only a small number of patients who die undergo autopsy.37,38 Notably in the literature, the presentation of peptic ulcer disease is silent and painless, which further makes timely diagnosis difficult in elderly patients. 35
Co-existing medical conditions such as cardiovascular disease, pulmonary disease, chronic liver disease and diabetes mellitus are strong predictors of morbidity and mortality. Perforations of longer than 48 hours and advancing age are two other important risk factors. Additionally, gastric ulcer perforation has a three times higher risk of mortality in comparison to duodenal ulcer perforation. 38
Recent epidemiologic data suggest a rise in perforations and bleeding from these ulcers. 38 Approximately 15% of peptic ulcer disease patients will have gastrointestinal haemorrhage at some point in their lives, and around 6% will develop a perforated ulcer. 38
Peritonitis and shock secondary to perforation are well-recognised sudden causes of death. A case series as well as other well-documented articles support the importance of this claim. 38 Another study places the total mortality of in-hospital perforations at 88%. 39 Vagal reflex inhibitory influences causing rapid exhaustion of the neuro-circulatory dynamics in response to the intense and sustained pain at the site of perforation of the gastric ulcer is suggested as a mechanism of sudden death when death occurs before any signs of peritonitis develop. 40
Another ulcerative cause of perforation leading to sudden death is stercoral ulcers, which are rare ulcers, primarily occurring in the sigmoid colon and rectum. 41 These occur because of pressure necrosis of the mucosa by a large, hard faecolith matter. The most important factor predisposing to stercoral ulcer is chronic constipation. Stercoral perforation is associated with a very high risk of mortality and is usually not diagnosed before an autopsy.
Gastric dilatation
Gastric dilatation is another cause of sudden death in all age groups, with mortality rates without rupture or necrosis of the gastric wall, with necrosis, and with rupture at 5.4%, 37.5% and 55.6%, respectively.42,43 Anorexia nervosa, polyphagia, volvulus, superior mesenteric artery syndrome and bulimia nervosa have all been associated with cases of gastric dilatation and rupture. 42
Ishikawa et al. 44 describe a case of sudden death due to gastric rupture suspected to have been induced by excessive eating. Regarding the rarity of this condition, they reported only 47 cases over 50 years in the Japanese literature. 44 They further reported female dominance, with a male:female ratio of 1:4, and mortality, even with surgical intervention, at 65%. 44
Gastric rupture and/or shock secondary to compression of inferior vena cava and disturbance of portal blood flow resulting from gastric dilatation have been implied as reasons for mortality. 43 Hypovolaemic shock may occur in anorexic patients because of an imbalance in circulatory minerals and fluids as a result of retention of gastric juices. Additionally, paralysis of the bowel may significantly diminish the absorptive function of the gut, and this may further exacerbate shock. 43 Another cause of sudden death may be cardiac failure caused by vaso-vagal reflex as a result of over-extension of the stomach. However, this cannot be proven in forensic autopsies.
Tumours
One noteworthy entity related to gastric adenocarcinoma is pulmonary tumour thrombotic microangiopathy (PTTM), which is a well-described complication resulting in rapidly progressive pulmonary hypertension, secondary to metastatic tumour cells occupying a large proportion of small pulmonary arterioles.
Patients typically present with acute pulmonary hypertension, progressing to right-sided heart failure and sudden death, often before the actual gastric adenocarcinoma is discovered. 45 PTTM is reported to be present in 25% of patients dying of such carcinomas. However, the actual mortality associated with tumour emboli remains at 8%. 45
Sudden unexpected death due to clinically undiagnosed neoplasia in infancy and childhood (SUDNIC) is another rare tumour-associated phenomenon in individuals with apparently normal activities until the onset of acute signs and symptoms. 46 The primary tumours normally involve critical structures within the heart or central nervous system. Non-central nervous system and non-cardiac causes of SUDNIC are rarer, and a 20-year (1984–2003) retrospective review of autopsy records from the Hospital for Sick Children (Toronto, Canada) include a single case of sudden death due to previously undiagnosed widely disseminated gastric adenocarcinoma in an 11-year-old girl with only symptoms of back pain. In the aforementioned patient’s case, death was attributed to pulmonary tumour microemboli with pulmonary hypertension and haemorrhage. 46 Another retrospective study of paediatric autopsies at Great Ormond Street Hospital (London, UK) over a 20-year period (1996–2015) did not reveal any clinically undiagnosed gastrointestinal neoplasms as the cause of SUDNIC. 47 Due to its rarity, SUDNIC is usually not considered in the differential diagnosis of sudden death in infancy and childhood. Nevertheless, it can be an important cause. 46
Hayashi et al. 48 describe a case of sudden unexpected death due to spontaneous perforation of an unclassified small bowel tumour with intra-tumoural haemorrhagic necrosis wherein a 62-year-old woman was found lying dead in her single prison cell. Following an autopsy, the cause of death was opined as peritonitis secondary to a jejunal malignant tumour perforation. In a 10-year retrospective study of undiagnosed fatal malignancy in adult autopsies, Parajuli et al. report a 69-year-old woman with clinically undiagnosed adenocarcinoma of the colon who died as a result of perforation of the colon and subsequent acute peritonitis. 49
Other more unusual gastrointestinal-related causes of sudden death include a case report of a 39-year-old woman with Gardner syndrome, a rare familial disorder characterised by colonic as well as gastric and small bowel polyps. The patient died from marked hyponatremia (serum Na <130 mEq/L) and hypokalaemia (serum K <3.5 mEq/L). 50 However, attributing it solely to Gardner syndrome remains questionable.
Varices
Varices can rupture and bleed, leading to sudden unexpected death. Most varices pertaining to the gastrointestinal tract are caused by portal hypertension due to cirrhosis of the liver. Various other aetiologies are implicated in the rest of the small proportion of cases of varices. For example, gastric varices can be caused by splenic vein thrombosis related to pancreatitis or malignancies of the pancreas and stomach in the region of the splenic vein. Idiopathic small bowel and colonic varices are also reported in the literature.
Gastric varices may be isolated or an extension of the oesophageal varices downward along the curvatures of the stomach. Gastric variceal bleeding following rupture tends to be more severe, with a higher mortality rate compared to oesophageal varices. Ectopic varices appear in locations other than the gastroesophageal region, and those pertaining to the gastrointestinal tract may be present in the duodenum, jejunum, ileum, colon and anorectum.
Machida et al. 51 report an autopsy case of death due to ruptured duodenal varices after endoscopic ligation of oesophageal varices in a 79-year-old woman. Another two autopsy cases of bleeding from ruptured duodenal varices in a 48-year-old man and 35-year-old man are described by Hashiguchi et al. 52 and Amin et al., 53 respectively. Waxman et al. 54 report two autopsy cases of death due to massive rectal bleeding from ruptured rectal varices. Batoon and Zoneraich 55 report a case of misdiagnosed anorectal varices that resulted in a fatal outcome in a 69-year-old woman. Olusola et al. 56 report a fatal case of intraperitoneal haemorrhage resulting from ruptured ectopic varices located in the rectovesical pouch in a 52-year-old man. Hayashi et al. 60 report an autopsy case of intra-abdominal bleeding from ruptured ectopic varices of the mesentery of the ascending colon in a 43-year-old man with a clinical history of alcoholic liver cirrhosis.
Miscellaneous
Gastroenteritis may cause sudden death from severe dehydration and electrolyte imbalance, especially in infants. Several rare and unusual conditions that may cause life-threatening gastrointestinal bleeding are not described here. Miscellaneous causes also include those that are iatrogenic, but these are not described here. This review mainly deals with sudden unexpected death from natural disease.
Conclusion
This review draws attention to the gastrointestinal causes of sudden unexpected death and the associated pathology of each cause, which may not have been covered as extensively in previous medical literature. In addition, related fatal cases encountered occasionally in forensic autopsy practice are also discussed. We aim to highlight the need for physicians to prevent death in such conditions by ensuring that subclinical cases are diagnosed correctly before it is too late and by providing timely and efficacious treatment to the patient concerned. In addition, this review would certainly benefit the forensic pathologist while dealing with cases of sudden unexpected death due to gastrointestinal causes.
Footnotes
Acknowledgements
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.