
Abstract
Background
Transkei is regarded as a rural part of South Africa. It was one of the black homelands where rigorous apartheid was practised. The incidence of firearm-related deaths used to be very high, but after the implementation of the Firearm Control Act in 2002, the trend changed. However, the murder rate is still a major public-health problem in this region of South Africa.
Objective
The aim of this study was to investigate 23 years (1993–2015) of homicide trends in the Transkei region of South Africa.
Method
A review of records of medico-legal autopsies performed at Mthatha Forensic Pathology Laboratory from 1993 to 2015 was undertaken.
Results
Between 1993 and 2015, the number of autopsies performed on people who had died unnatural deaths was 24,693. The records of 12,618 (51%) autopsies on victims of homicide between 1993 and 2015 were available for study. The average rate of murder was 85/100,000 of the population in this region. Of these deaths, on average 34/100,000 were caused by sharp-edged instruments, 30/100,000 by gunshot wounds and 21/100,000 by blunt trauma. The rate of murder of males was significantly higher than that of females, with a ratio of 5.7:1, and over the period of 23 years covered by this study, the incidence was highest (30.5/100,000) in the young age group between 21 and 30 years.
Conclusion
The rate of homicide is very high in the Transkei region of South Africa. It needs urgent intervention to curb unnecessary deaths.
Introduction
In 2013, an estimated 475,000 deaths in the world resulted from homicide. 1 In low- and middle-income countries, the highest estimated rates of homicide occur in the region of the Americas, with a homicide rate of 28.5/100,000 of the population, followed by the African region, with a homicide rate of 10.9/100,000 of the population. 1 The lowest estimated rate of homicide is found in the low- and middle-income countries of the Western Pacific region, where 2.1 homicides occur per 100,000 of the population. 1
Homicide is an extreme form of violence, contributing to loss of years of expected life. More than 20 years after the end of apartheid, South Africa continues to experience excessive levels of violence. 2 In 2007–2008, the South African Police Service recorded 18,487 homicides at a rate of 38.6/100,000 of the population – a decrease of 42% since 1994, when the rate was 66.9/100,000 of the population. 3 The criminal use of firearms in South Africa is widespread and a major factor in the country, which has the third-highest homicide rate in the world. 4 South Africa’s homicide rate is 31.1/100,000 of the population, which is about three times higher than that in the region of Africa. 1 The high rates of homicide in a rural South African population (2002–2008) – particularly among men – underscore the need for urgent interventions to reduce this tragic and theoretically preventable loss of life. 5
Although the female homicide rate has declined from 24.7/100,000 in 1999 to 12.9/100,000 in 2009, 6 the current figure remains considerably higher than the estimated global rate of 4/100,000 of the female population. 7 The highest rate of homicide is among men aged 15–29 years (184/100,000). The homicide rate for boys younger than five years of age is 14/100,000, while for girls younger than five years of age, the homicide rate is 11.7/100,000. These rates are more than twice the corresponding rates for other low- and middle-income countries. 8 The number of illegal firearms has been reduced by at least 24% since the implementation of the Firearm Control Act 2004. There is some evidence of the impact of the legislation on female gun-related homicide, with 1147 such cases in 1999 compared to 461 in 2009. 9
South Africa’s unique political history and resulting social and economic inequalities have been identified as some of the factors possibly contributing to the high rate of interpersonal violence. 10 Several other factors reported to be associated with violent death include poverty, lack of education, unemployment, alcohol abuse, substance abuse and power (male dominance). 2 The purpose of this study is to highlight and understand the problem of homicide in the Transkei region of South Africa.
Method
Mthatha Forensic Pathology Laboratory is the only laboratory in this region, catering for a population of about half a million in the region of Mthatha. It is attached to the Nelson Mandela Academic Hospital, which is the only teaching hospital in this province. It is associated with the Walter Sisulu University Medical School, and all medico-legal cases in this area of South Africa are dealt with at this facility. In total, 24,693 autopsies were conducted between 1996 and 2015 and recorded in the post-mortem register at this laboratory. A complete list of unnatural deaths was not kept between 1993 and 1995, but the records of victims of homicide between 1993 and 1995 was available and was therefore included in this study. Between 1993 and 2015, the laboratory dealt with 10,945 homicide victims. The details of names, addresses, age, gender and date of autopsy, with cause of death, were recorded. Fourteen forensic officers are engaged in collecting corpses round the clock from 17 different police stations in four municipalities. These are OR Tambo, Mhlontlo, Chris Hani and the Mbashe municipal area of about 200 km2 (Figure 1). The OR Tambo municipality is the largest, and covered fully by 10 police stations. Mhlontlo municipality has four police stations. There are two in Chris Hani, and Mbashe municipality has one. The combined population was 400,000 in 1993, but this number has been increasing at an average of 3% annually. In 2005, there were five police stations to be taken into account. Therefore, the population in the area of this study has increased. Population statistics were calculated with the help of the South African Statistics Department in Mthatha. However, it is difficult to estimate the total population involved. The data were collected in hard copies designed to reflect post-mortem number, year, gender and cause of death. These data were transferred to an Excel computer program and analysed with the help of the SPSS Statistics for Windows.
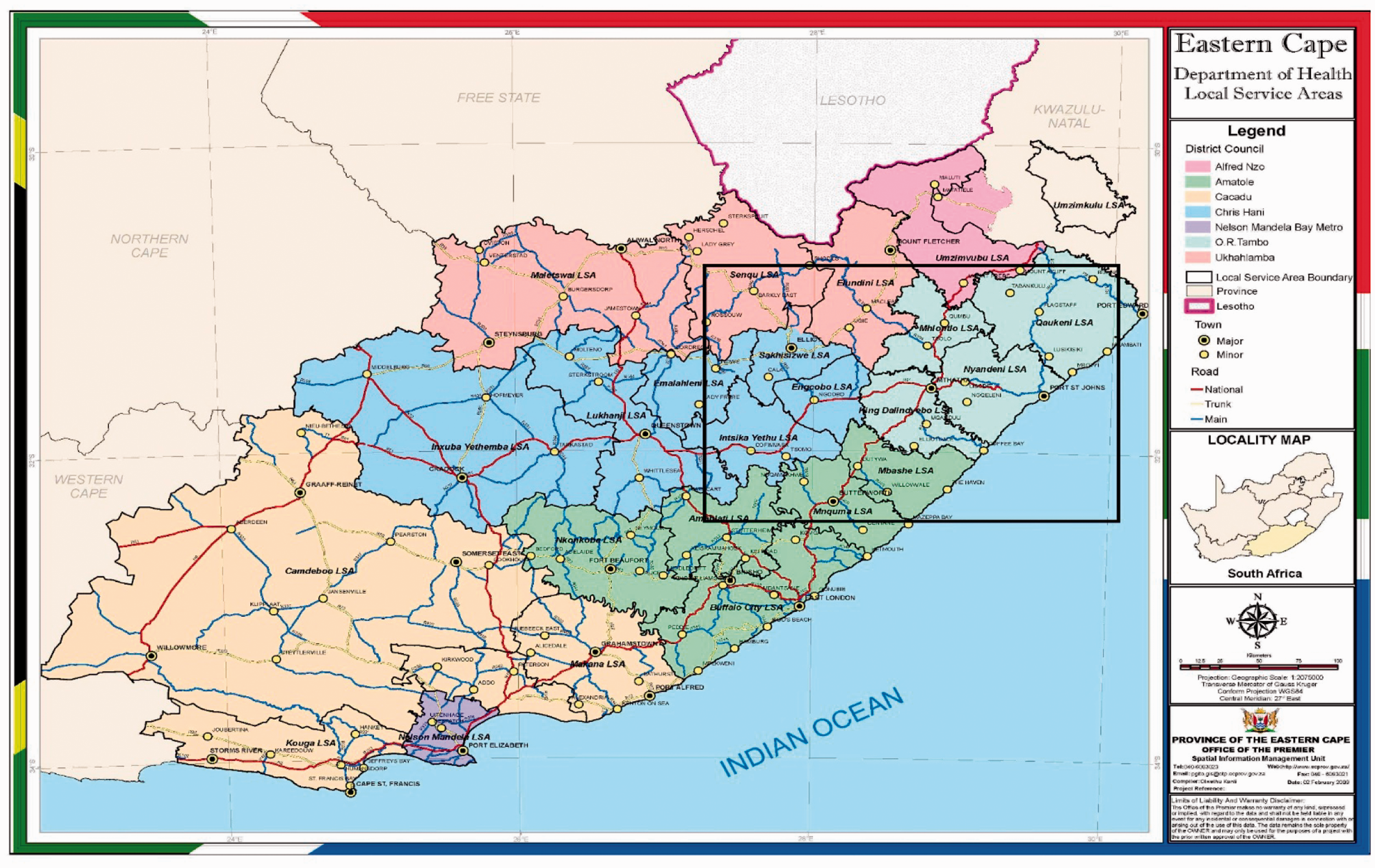
Map of Transkei subregion of South Africa – population catered for by Mthatha Forensic Pathology Laboratory indicated by a square.
Results
The post-mortem register lists 24,693 forensic autopsies carried out in Nelson Mandela Academic Hospital’s Forensic Pathology Laboratory on people who suffered unnatural death between 1993 and 2015. The records of 12,618 medico-legal autopsies on victims of homicide between 1993 and 2015 were available for study. The percentage of murder victims among those dying from unnatural causes was 45% (20% stabbing, 14% gunshot wounds and 11% blunt trauma) between 1996 and 2015 period (Figure 2).
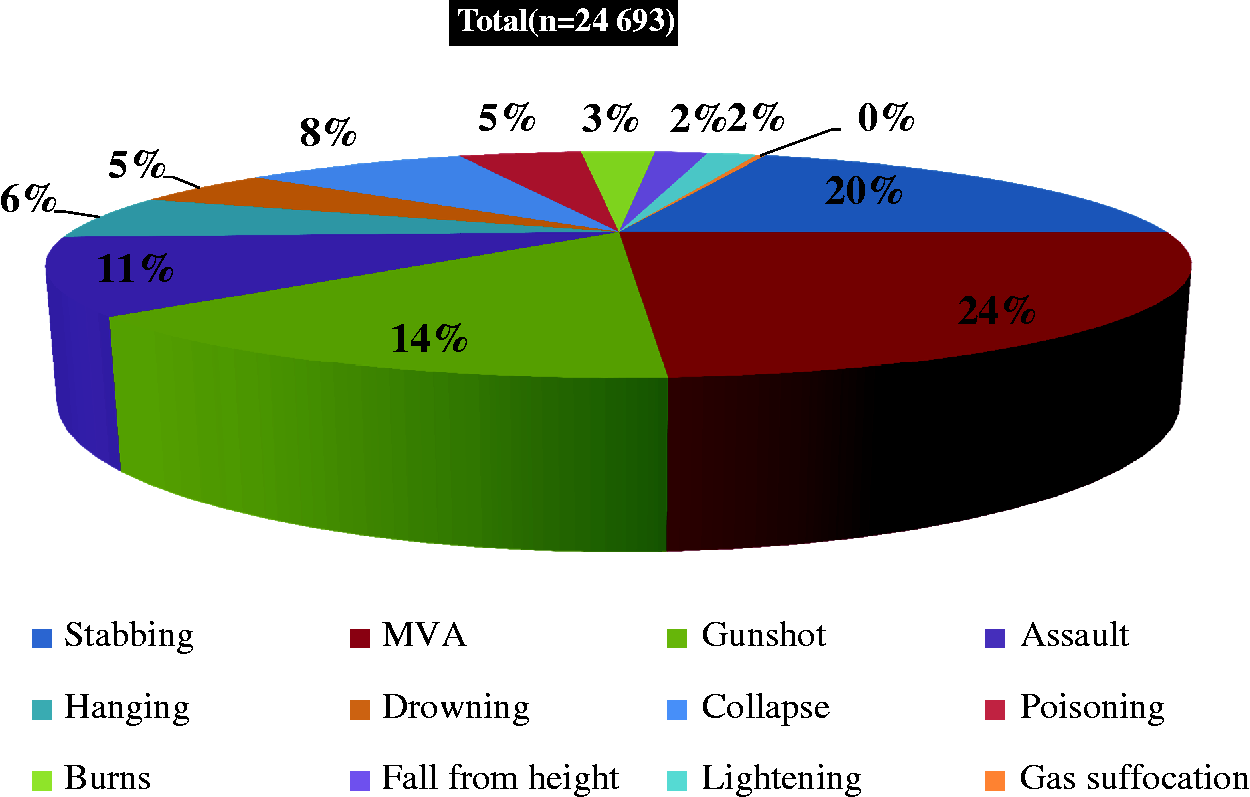
Ranks of percentage of cause of death (both sexes) in the Mthatha region of South Africa 1993–2015.
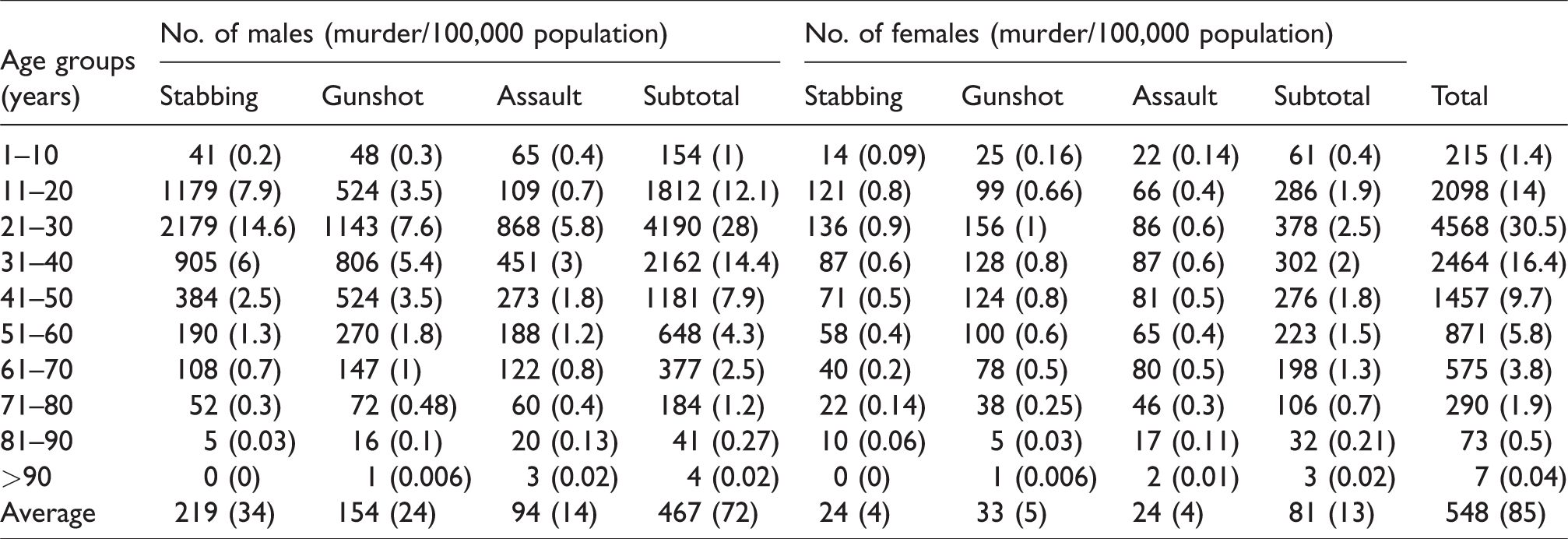
Pattern of homicide in the Transkei subregion of South Africa (n = 12,618).
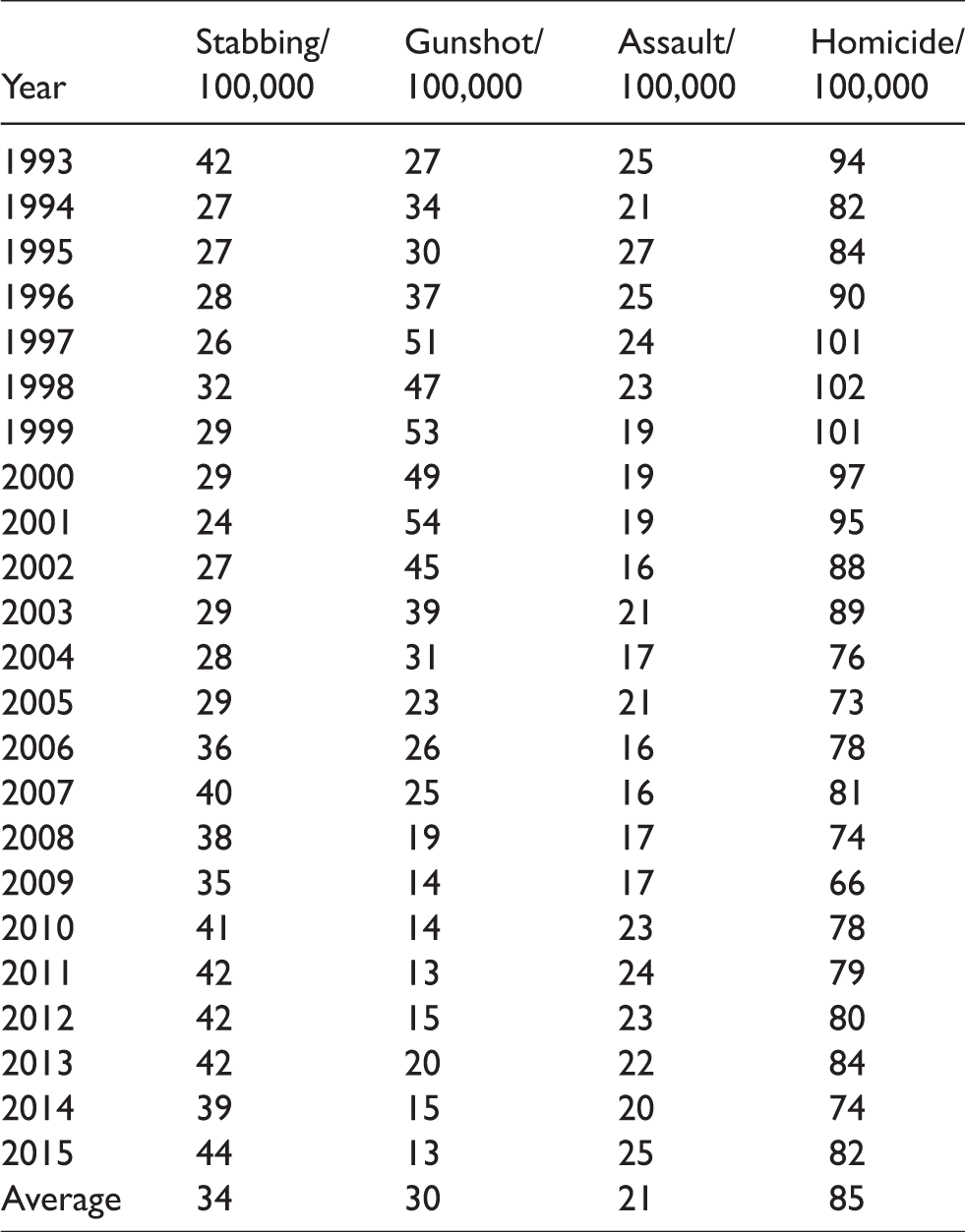

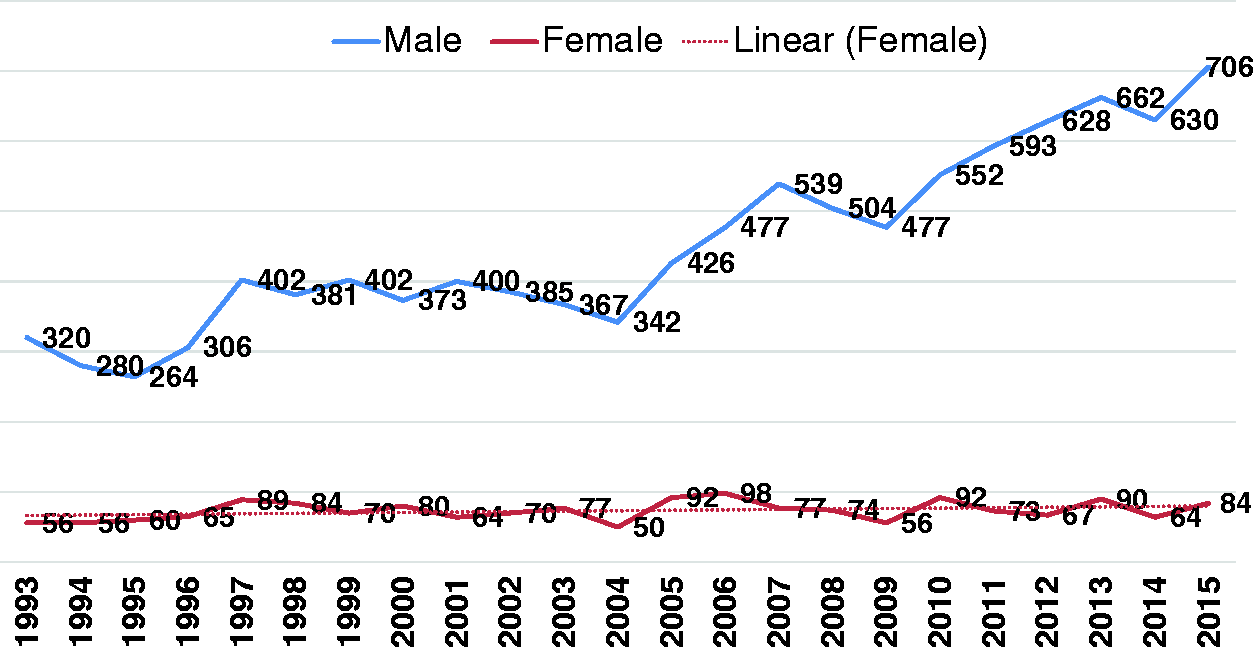
Year-wise murder rate in Transkei subregion of South Africa from 1993 to 2015 (n = 12,618).
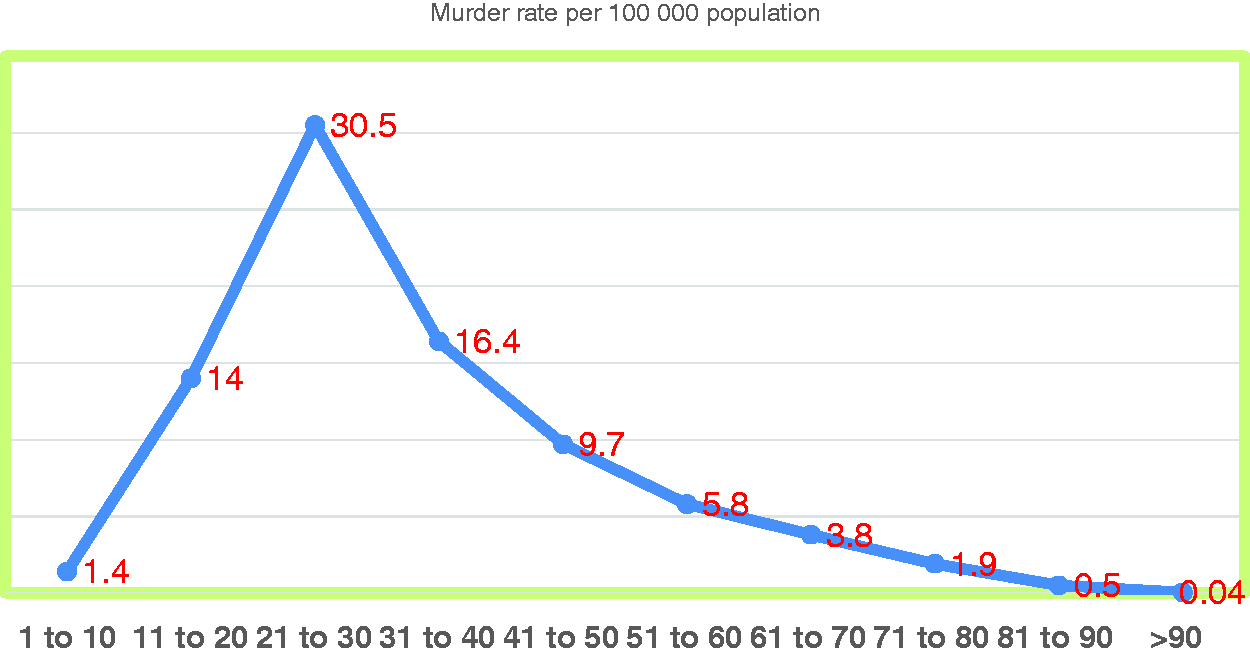
The average rate of murder involving the use of a sharp-pointed weapon was highest (34/100,000), followed by gunshot (30/100,000) and blunt trauma–related deaths (21/100,000) over a study period of 23 years (Table 1). The death rate as a result of stab injury decreased from 42/100,000 (in 1993) to 24/100,000 (in 2001), but has since climbed to its highest level of 44/100,000 (Table 1 and Figure 4). The gunshot rate increased from 27/100,000 (in 1993) to 54/100,000 (in 2001), and then it decreased from 39/100,000 (in 2002) to 13/100,000 (in 2015) during the same period (Table 1 and Figure 4). The murder rate from blunt force was 25/100,000 in 1993 and remained the same in 2015 (Table 1). Male deaths outnumbered those of females by 5.7:1 (Table 2 and Figure 5). Stab injuries were common among males, with an average of 219 (34/100,000), followed by gunshot wounds (154; 24/100,000) and blunt trauma (94; 14/100,000) over a period of 23 years (Table 2). The highest number of murders, 4568 (30.5/100,000), occurred in the 21- to 30-year age group, followed by 2464 (16.4/100 000) in the 31- to 40-year age group (Table 2 and Figure 6).
‘Crossing point’ where the most common murder weapon changed from a firearm to a sharp-edged weapon in the Transkei region of South Africa (n = 12,618). Male versus female homicide trend in the Mthatha region of South Africa (1993–2015; n = 12,618). Murder rate in different age groups from 1993 to 2015 in the Transkei subregion of South Africa (n = 12,618). Murder rate in different age groups in the Transkei subregion of South Africa from 1993 to 2015 (n = 12,618).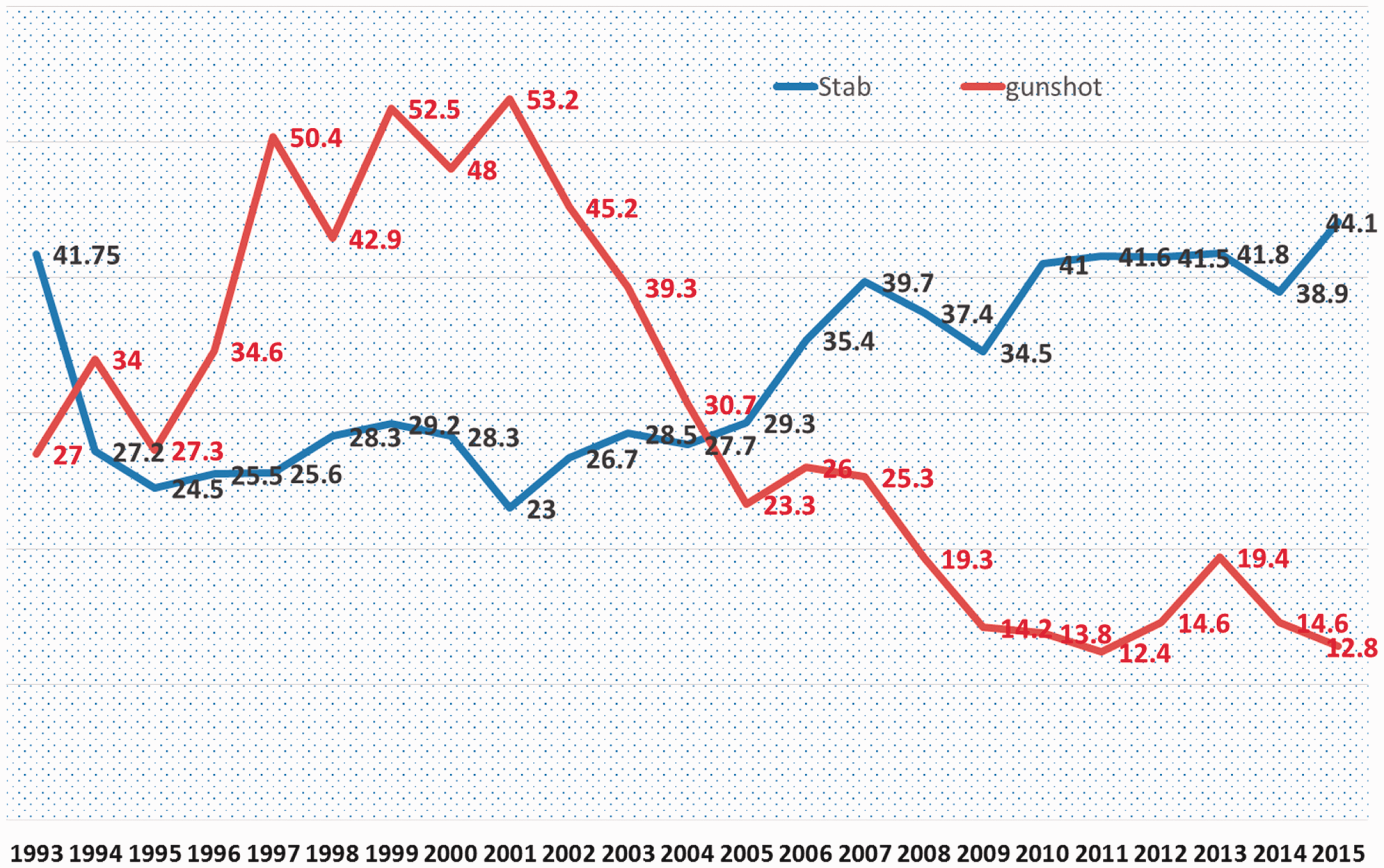
Discussion
This is the first retrospective autopsy study of a large sample size (N = 24,693) over a period of 23 years (1993–2015) showing the trends in homicide in the Transkei subregion of South Africa (Figure 1). It provides important information that justifies expanded efforts to initiate and develop a programme for the prevention of homicide in this region. The Transkei region of South Africa was a former black homeland. Most of the people live in poverty and do not have enough resources to get an education. 11 People have become free politically, but poverty in general has not declined since 1994. Poverty is severe in the former Bantustans such as the Transkei region. Seventy-three per cent of the rural people in the Eastern Cape were living on <US$23 per month in 2005/2006, and more than half of them on <US$16 per month. 12
During the study period, 24,693 unnatural deaths were recorded in the forensic pathology register in the Transkei region. Of these, a little less than half (12,579; 51%) were victims of homicide between 1993 and 2015, which is equal to 218 bus accidents (50 seated), and 37 crashed airbuses carrying 300 passengers each (Figure 2 and Table 1). These are not mere accidents but wilful killing of human beings. Unfortunately, this happens in the Transkei – a black, poverty-stricken area, where people are living on a day-to-day basis. In general, the community is insensitive and intolerant and turns a blind eye to these heinous crimes. Soon after death, people start to organise the burial and funeral ceremony. This costs a lot of money, as they have to feed hundreds of the people in the community. Those who have life insurance start filling in forms for the claim soon after death, so the manner of death is a serious issue to the family or the community.
The average rate of murder was 85/100,000 of the population over a period of 23 years (1993–2015) (Table 1 and Figure 3), which is almost 13 times the global average of 6.2/100,000, and more than two-and-a-half times the average South African murder rate (33/100,000). 13 The highest murder rates in Africa today are found in Southern Africa and Central Africa. 1 The extremely high rate of murder in the Transkei region (85/100,000 of the population) could be compared to that in Central American countries such as Honduras (90/100,000). 14 The murder rate has not declined significantly in South Africa as in other middle- and low-income countries (Table 1 and Figure 3). Homicide rates are estimated to have declined (2000–2012) by just over 16% globally (from 8/100,000 to 6.7/100,000 of the population), and in high-income countries by 39% (from 6.2/100,000 to 3.8/100,000 of the population). 1 South Africa is regarded as a wealthier country than the rest of the African countries, but the murder rate is higher than in neighbouring countries such as Zimbabwe and Botswana. 15 In the list of the most homicidal countries in the world, there are only two countries in Africa: Lesotho (38/100,000) and South Africa (33/100,000). 15 There is great variation in the murder rate in South Africa. It is highest in the Eastern Cape (52/100,000) and lowest in the Northern Cape (24.5/100,000). 16 There is lack of information within the province of the Eastern Cape, but it is a known fact that it is very high in the eastern part of the Eastern Cape (i.e. the Transkei region).
South Africa elected its first fully democratic government in 1994, and the Republic of Transkei merged with South Africa soon afterwards. There was a very high murder rate at that time, to which conditions created by the rigorous apartheid system in the country probably contributed. In 1993, the murder rate was 94/100,000, which increased to 102/100,000 in 1998 (Table 1 and Figure 3). Firearm injuries were a major cause of death in murders at that time, and the incidence of shootings remained high until 2002 (Table 1 and Figure 3). After 2002, it started declining, but only marginally, to <90/100,000 of the population, dropping to 66/100,000 in 2009 (Table 1 and Figure 3). At present, it has stabilised at between 74/100,000 (in 2014), and 82/100,000 (in 2015; Table 1 and Figure 3). There has been a drastic decrease in the use of firearm-related deaths, but the use of sharp-edged weapons such as knives has increased, resulting in almost the same number of murders in this region (Figure 4). A ‘crossing point’ was reached where the most common murder weapon changed from a firearm to a knife in 2002 (Figure 4). There are three million registered firearm owners in South Africa. The number of illegal firearms has been reduced by at least 24% since the Firearm Control Act was implemented in 2002. 17 It conveyed the message early enough to illegal gun owners to abandon their guns, even in the year 2000 when the Firearm Control Act was legislated. The Firearm Control Act has prevented thousands of murders 17 being committed by shooting, but unfortunately this has been neutralised by the excessive use of sharp-edged weapons (Figure 4), and the net result remains the same. There has been no change in the murderous mind-set of Transkeian South Africans.
Young black males are both perpetrators and victims of violent death in this region. They consume excessive amounts of alcohol, as well as drugs, and engage in risky behaviours. Sixty per cent of murders occur among males aged 15–44 years, making homicide the third leading cause of death for males in this age group. 1 About two–thirds (9130; 60.9%) of murders were recorded in the age group 11–40 years, and a little less than half (7032; 46.9%) in the age group 21–40 years. It is agonising that one–third (4568; 30.5%) of all murders were found to have occurred among young adults in their most productive years (21–30 years) in this study (Table 2 and Figure 5). Most of the time fatal injuries among children in South Africa 18 are recorded in urban areas, but this is not the case in this study, which is rural based, as more than one–fifth of murders in this region (2313/12,579; 1:5.4) involved children younger than 20 years of age (Table 2 and Figure 5). If life is so cheap to black young people, what goes on their minds – what does the future hold for them and for the country? Moreover, they are too young to kill and be killed, but probably too old to change.
An earlier study (2004) in the Transkei region revealed an increasing incidence of traumatic deaths among women. Gun injury is the most common cause of traumatic death among females, 19 and it is still the number one cause of death by homicide in this study (Table 2). The average female homicide rate was 13/100,000, which was more than three times the global average (4/100,000 of the female population), and almost equal to the national figure of 2009 (12.9/100,000). 6 South Africa has a high female homicide rate, 20 although the incidence of male deaths was significantly higher than female ones at 5.7:1 in this study (Table 2 and Figure 5). An almost similar observation in a study carried out by Matzopoulos et al. in 2016 showed that the male-to-female ratio of homicide (six male deaths per female death) was higher than for any other apparent cause of death. This was due to the particularly high rate of three external causes of death that were attributed to homicide: sharp-force injuries/stabbing, gunshot injuries and blunt-force injuries. 21 Guns play a significant role in violence against women in South Africa, most notably in the killing of intimate partners. 3
The findings of Schneider et al. (2009) showed that murder occurred more frequently in areas with a low socio-economic status. 22 A combination of unemployment, poverty, alcohol and human immunodeficiency virus (HIV) predispose people to commit homicide. About half (49.5%) of the traumatic deaths in the Transkei region are related to alcohol. 23 In 2006–2007, only 16% of the rural population were either employed or economically active, meaning that they were permanently unemployed and living in extreme poverty. 12 A poor black man could become either a perpetrator or a victim of homicide during the search of food. They take risks every day to procure a meal. They are also at a disadvantage in getting medical treatment because they are poor. It is a vicious cycle: being poor makes one more prone to violence, and violence propagates poverty. Wealthier people are associated with a decrease in the risk of violent death. 24 Homicide has also been compounded by the high rate of HIV infection in this region, which poses an even bigger threat to the country than does violence. 19
Conclusion
There is a very high rate of homicide in the Transkei region of South Africa, which is a serious challenge to law-enforcement agencies, the judiciary and public-health delivery system. The number of firearm-related deaths has declined to less than one-third of what it was, but death inflicted by sharp-edged pointed weapon has more than doubled in the last 23 years (1993–2015). The positive effect of the implementation of the Firearm Control Act in 2002 has been nullified by the increasing use of sharp-edged weapons. This is a worrying factor. Most victims were young adults. It is not clear how this ongoing high rate of murder can be controlled. Education in the community may be an instrument to curb this crime. Strong policing and speedy court trials are always recommended, but nothing has changed in this respect in the last 23 years, and the Transkei has become the ‘mini-Honduras’ of South Africa. The government has not adopted any serious strategy to prevent these premature deaths in this region of South Africa.
Footnotes
Acknowledgements
The author would like to thank all staff of the Mthatha Forensic Pathology Laboratory for helping to collect data, and for providing information on police stations in this region. The author would also like to thank the South African Statistics Department at Mthatha for providing a population estimate of all the police stations. The author has ethical permission for collecting data and publication (approved project no. 4114/1999) from the Ethical Committee of the University of Transkei. This study is an extension of an earlier study, which was published in SAMJ 2008.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.