
Abstract
Objective
The aim of this study was to review demographic and clinical characteristics of patients with complex regional pain syndrome type 1 (CRPS) seen in a UK medico-legal setting – particularly the relationship between CRPS and somatoform disorders.
Methods
Fifty consecutive cases of CRPS (interviewed 2005–2016) undergoing psychiatric assessment were reviewed. A systematic assessment of mental states was conducted via interview and examination of medical/psychiatric records. Thirty patients also completed the Brief Illness Perception Questionnaire (BIPQ).
Results
Sixty per cent of patients (n = 30) were female, and the mean age was 43 years. Twenty-two per cent (n = 11) were employed, and 60% (n = 30) received disability benefits. Symptoms were reported in the upper limb (62%; n = 31), lower limb (30%; n = 15), both (6%; n = 3) or elsewhere (2%; n = 1). Eighty-four per cent (n = 42) satisfied DSM-5 criteria for current somatoform disorder. A history of more than two pain-related functional somatic syndromes (e.g. non-cardiac chest pain) was found in 42% (n = 21) and functional neurological symptoms (e.g. ‘claw-hand’) in 42% (n = 21). BIPQ scores resembled those associated with somatoform disorders and disorders mediated by psychological factors (e.g. irritable bowel syndrome). In 38% (n = 19), the CRPS diagnosis was disputed among experts. A history of depression was noted in 60% (n = 30), panic attacks in 20% (n = 10) and alcohol/substance misuse in 18% (n = 9). Opiates were prescribed to 64% (n = 32).
Conclusions
Patients diagnosed with CRPS involved in litigation have high rates of prior psychopathology (mainly somatoform disorders) and pain-related disability for which opiate use is common. They risk an adverse reaction to limb pain ‘shaped’ by maladaptive illness beliefs. The CRPS diagnosis lacks reliability in medico-legal settings and may cause iatrogenic harm
Introduction
Complex regional pain syndrome type 1 (CRPS) is a condition involving limb pain associated with sensory, autonomic, skin and bone abnormalities. 1 CRPS commonly occurs after an injury and can spread to other limbs. 2 The European incidence rate of CRPS is 26/100,000 person years, and the majority of patients with the diagnosis are female. 3
A CRPS diagnosis is typically established using the Budapest criteria, 4 which are shown in Appendix 1. There is evidence that it is being diagnosed more frequently – predominantly in medico-legal settings. 5 However, CRPS remains a controversial diagnosis, and as such, it has attracted considerable recent interest and debate. 6 It has been suggested, for example, that CRPS represents an aberrant protective response to perceived threat of tissue injury7,8 and/or a disuse syndrome. 9 Limb immobilisation may induce symptoms and signs that are characteristic of CRPS.10,11 Some have even questioned whether CRPS is an authentic medical disorder. 6 There are strong reasons to be sceptical of the diagnosis, including: (1) the subjectivity of the Budapest criteria, (2) observed similarities between patients with CRPS and functional neurological disorders (conversion disorder) and (3) the existence of numerous reports of factitious CRPS in the professional literature. 12
Because patients often develop CRPS after an injury or accident, it is not uncommon for litigation to occur. 5 Previous studies have demonstrated that psychiatrists can provide information on an individual’s psychological vulnerability within the legal setting, as well as assess any co-morbid psychiatric disorder. 13 This study set out to review the demographic and clinical characteristics of a consecutive series of patients with CRPS who were involved in litigation and referred for psychiatric assessment. Recent reviews of the disorder have appeared in legal journals.14,15 We were particularly interested in determining the prevalence of previous and current somatoform disorders in these patients, as it has been suggested that ‘CRPS is not associated with a history of pain-preceding psychological problems, or with somatization’. 16
Method
Setting and participants
Fifty patients were referred to a consultant psychiatrist (C.B.) as part of a medico-legal assessment, all of whom were interviewed between 2005 and 2016. The purpose of this referral was to provide information to the court to assist in forming legal decisions.
Data collection
The assessment consisted of a comprehensive review of four sources of information: (1) a detailed medical history, (2) primary-care and medical notes, (3) supplementary witness statements from the patient and any informants and (4) medico-legal reports written by clinicians from a variety of disciplines – typically pain medicine, rheumatology and orthopaedics. Data from each patient were recorded systematically and entered into an IBM SPSS Statistics for Windows v24.0 database (IBM Corp., Armonk, NY) in anonymised form at a later date.
First, demographic information was collected from each patient, including age, sex, history of childhood adversity, employment status, use of assistive technology and receipt of long-term disability benefits.
Second, a detailed history of CRPS symptoms was taken, covering: episode of CRPS (i.e. first or repeat episode), location of symptoms, duration of symptoms and precipitants to CRPS in the form of psychosocial stressors or traumatic events. Because the Budapest criteria for CRPS are not always easy to interpret, 4 an attempt was also made to establish whether there were any major discrepancies between the diagnoses established by the patients’ treating doctors and clinicians who had supplied reports for the court.
Third, a review of psychopathology was undertaken, noting any history of alcohol or substance abuse, depression, panic attacks or functional neurological symptoms. An attempt was made where possible to establish a diagnosis of somatic symptom disorder (SSD) via interview, using the DSM-5 criteria (see Appendix 2). A diagnosis of a SSD was established when the interviewer considered that ‘criterion B’ was satisfied – that is, that thoughts, feelings and behaviours were disproportionate and excessive. 17 For example, the criterion was considered satisfied if a patient remained convinced that nerve and/or muscle damage was responsible for the symptoms after having been reassured that this was not the case. Alternatively, ‘criterion B’ was considered to be satisfied if there was evidence of catastrophic thinking, exaggerated fear avoidance behaviour (e.g. avoiding use of a limb) or evidence of anxious introspection and excessive concern.
Patient notes were also examined to identify functional somatic syndromes (FSS). Previous studies have suggested similarities between CRPS and FSS such as fibromyalgia, repetitive strain injury and irritable bowel syndrome (IBS).18,19 Recent evidence has also emerged to suggest that FSS form part of a poly-syndromic phenotype, and that the finding of one of these syndromes predicts the appearance of others in the future. 20 Seven FSS were therefore considered: chronic fatigue syndrome, non-cardiac chest pain, IBS, migraine and/or tension headaches, chronic pelvic pain, fibromyalgia and temporomandibular joint dysfunction.
Finally, the history of treatment was taken for each patient, covering medication, pain-relieving procedures (e.g. epidural anaesthesia), cognitive–behavioural therapy and attendance at a pain clinic. Requests for procedures were also noted.
Thirty patients completed the Brief Illness Perception Questionnaire (BIPQ), which is a measure of illness perceptions.
21
Illness perceptions may be understood as ‘mental representations and personal ideas that people have about an illness’ which may ‘provide motivation … to take specific behaviours to regulate their emotions and improve the outcome of their illness’.
21
The BIPQ assesses perceptions on a 0-10 scale of:
Consequences – ‘How much does illness affect your life?’ Timeline – ‘How long do you think your illness will continue?’ Personal control – ‘How much control do you feel you have over your illness?’ Treatment control – ‘How much do you think your treatment can help your illness?’ Identity – ‘How much do you experience symptoms from your illness?’ Concern – ‘How concerned are you about your illness?’ Coherence – ‘How well do you feel you understand your illness?’ Emotional representation – ‘How much do you feel your illness affects you emotionally?’
A meta-analysis conducted recently by Broadbent et al. 21 demonstrated that the BIPQ has excellent psychometric properties, and that higher concern, identity and emotional representation scores were associated with poorer quality of life and higher rates of psychopathology, as were worse perceived consequences.
DVD surveillance
In 22 cases, DVD surveillance was made available. This was always viewed at least three months after the initial assessment. In some cases (n = 10), a conference with counsel was held to discuss the management of the case.
Data analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows v24.0. Descriptive statistics were used to summarise the baseline characteristics of our sample. Where applicable, one variable chi-squared (‘goodness of fit’) tests were used to determine the statistical significance of findings. We also examined demographic and psychopathological differences between two subgroups: (1) male/female participants and (2) participants with only upper- or lower-limb CRPS symptoms, who are generally managed by different surgical sub-specialties. The chi-square test for independence was used to compare categorical variables between these subgroups. Age was recorded in our assessment as a continuous variable and, accordingly, compared between subgroups using the independent samples t-test. The independent samples t-test was also used to compare total and individual BIPQ scores between subgroups.
Data storage
Following analysis, the anonymised data were stored on a secure hard drive at a location remote to the paper notes. Paper notes have been stored in a secure, locked facility in a general hospital.
Results
Demographic information and history of CRPS symptoms.
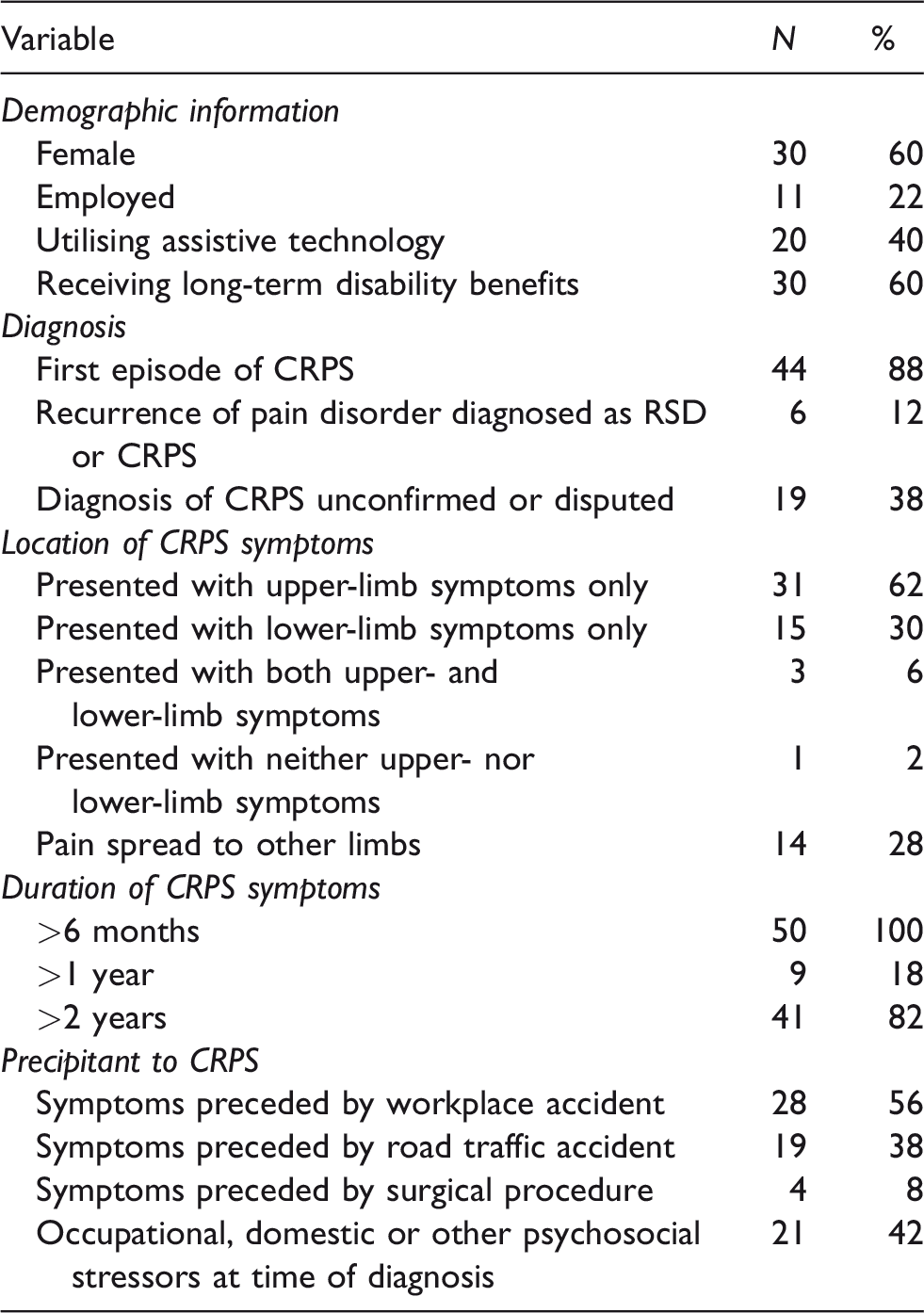
CRPS: complex regional pain syndrome type 1; RSD: reflex sympathetic dystrophy.
Psychopathology and treatment history.
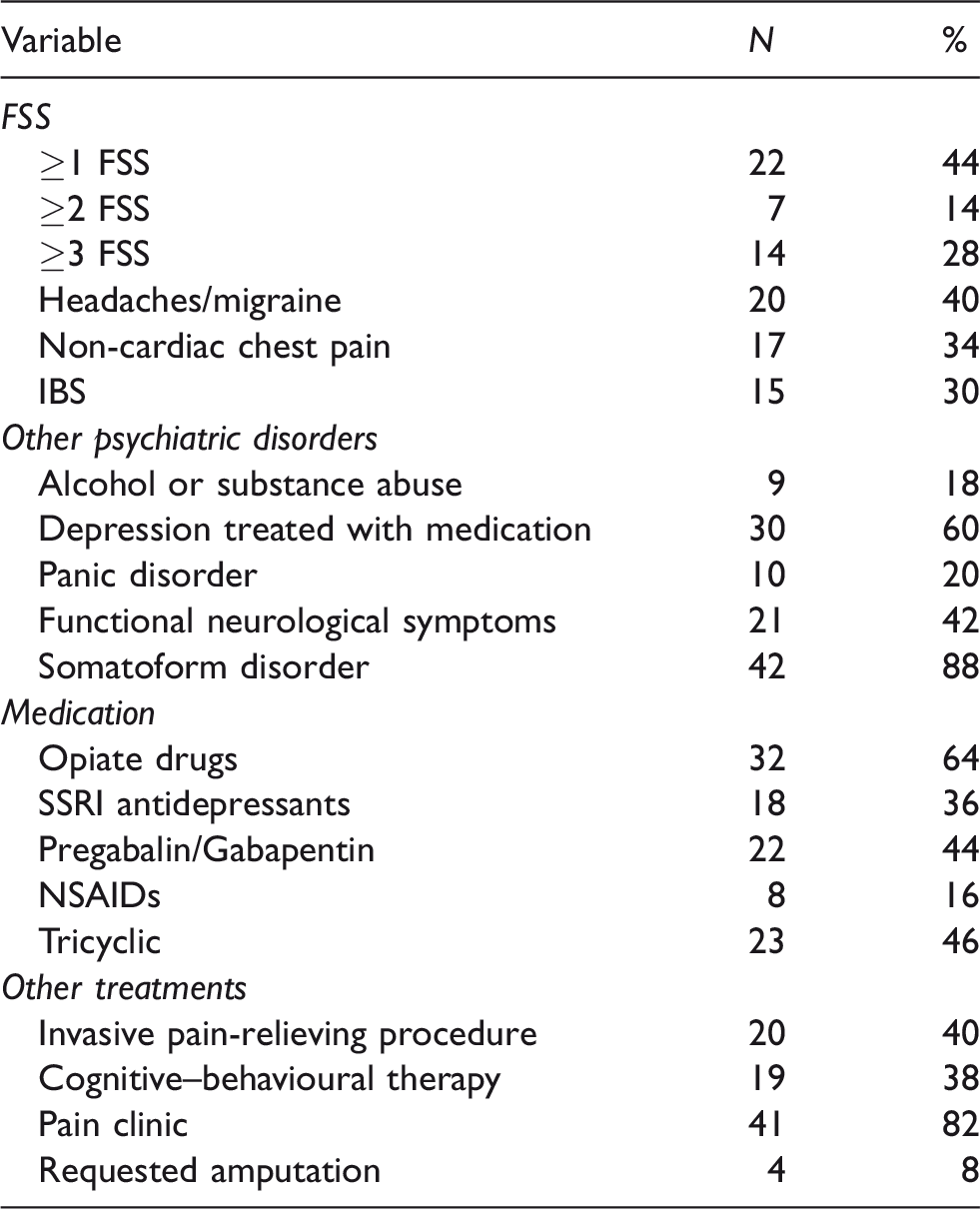
FSS: functional somatic syndrome; IBS: irritable bowel syndrome; SSRI: selective serotonin reuptake inhibitor; NSAID: non-steroidal anti-inflammatory drug.
BIPQ scores by individual item.
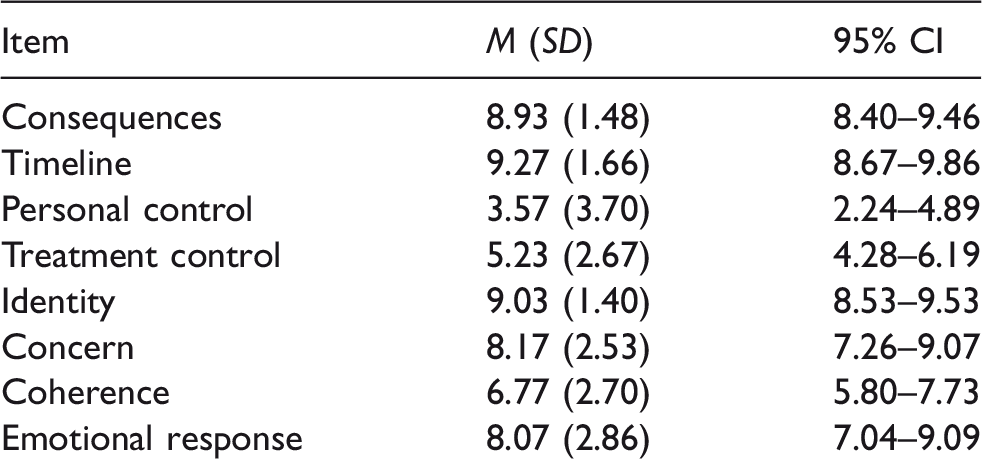
CI: confidence interval.
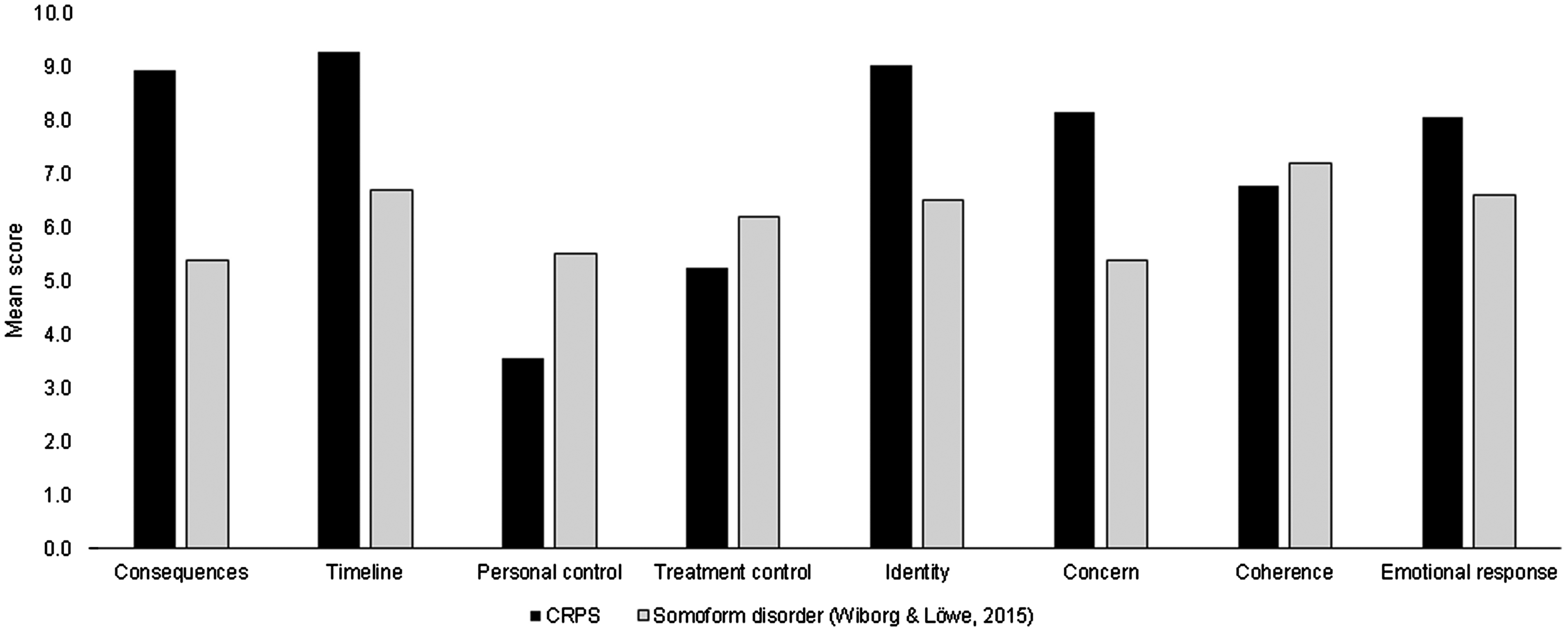
Brief Illness Perception Questionnaire scores by individual item compared with patients with somatoform disorders.
Demographic information
All but four of the 50 patients were white British, the remainder being Asian British. The mean age of patients was 43 years (range 19–67 years; SD = 10.4 years), and 60% were female (n = 30). The higher proportion of female patients in our sample was not statistically significant (60% vs. 40%; df = 1; χ2 = 2; p = 0.157). Sixteen per cent of patients (n = 8) experienced childhood adversity (physical and/or sexual abuse). Only 22% (n = 11) were employed at the time of assessment, and 60% (n = 30) were receiving long-term disability benefits. Forty per cent (n = 20) were utilising assistive technology; these patients used a wrist splint (n = 18), wheelchair (n = 5), crutch (n = 2) or walking stick (n = 1).
History of CRPS symptoms
In 88% (n = 44) of patients, the CRPS represented a first episode, but in 12% (n = 6) the pain syndrome represented a recurrence of a pain disorder that had occurred during a previous episode of illness and had been diagnosed as either reflex sympathetic dystrophy or CRPS. The pain reported was generally disproportionate to the physical findings, and its duration exceeded a year in 18% of patients (n = 9) and two years in 82% (n = 41). Sixty two per cent (n = 31) of patients presented with only upper-limb symptoms, and 30% (n = 15) with only lower-limb symptoms; 6% (n = 3) presented with both, and one patient presented with neither. In 28% (n = 14), the pain had spread to another limb or body part, and one patient described ‘flitting’ CRPS.
All 50 patients had a precipitant to CRPS in the form of a traumatic event: this involved an accident at work for 56% (n = 28), a road traffic accident for 38% (n = 19) and a surgical procedure for 8% (n = 4). Forty-two per cent (n = 21) had documented occupational/domestic stressors or other psychosocial stressors at the time of the diagnosis. In most cases, the treating clinician established the diagnosis of CRPS. However, in 38% (n = 19) cases either the medico-legal expert was unable to confirm the diagnosis ‘assigned’ to the patient by the treating doctor, or there was disagreement among medico-legal experts.
Psychopathology
Only 26% (n = 13) of patients had no history of any previous treated psychiatric disorder. A history of depression treated with medication was noted in 60% (n = 30), panic attacks in 20% (n = 10) and alcohol or substance abuse in 18% (n = 9). Forty-four per cent (n = 22) had a history of at least one FSS, 14% (n = 7) had a history of two FSS and 28% (n = 14) had a history of three or more FSS. The most common FSS reported were headaches/migraine (n = 20), non-cardiac chest pain (n = 17) and IBS (n = 15). Mental-state examination of the patients who were interviewed revealed evidence sufficient to establish a diagnosis of a somatoform disorder (specifically SSD) in 84% (n = 42).
Of the eight patients who were not assigned a diagnosis of SSD, four had no current mental illness, another two had adjustment reactions, one had depression and another multiple comorbid medical disorders. Of the four found to have no mental illness, three were working. A more detailed analysis was not possible because of the small numbers involved.
Forty-two per cent (n = 21) of patients had features of motor and sensory phenomena that were characteristic of a functional neurological disorder (Table 2). In the upper limb, these phenomena included dystonic movements such as ‘claw hand’, tremors and choreoathetoid movements. In the lower limb, weakness and equinovarus ankle deformities were noted. Three patients described an ‘alien limb’, with comments such as, ‘My hand does not want to be part of my body … it’s got a mind of its own’.
Treatment history
Forty per cent (n = 20) of patients had undergone invasive pain-relieving procedures such as guanethidine blocks and/or the insertion of a spinal-cord stimulator. Forty two per cent (n = 21) had undergone treatment in pain clinics – some of which were residential units established for patients with CRPS. Thirty-eight per cent (n = 19) had received cognitive–behavioural therapy for their CRPS. Sixty-four per cent (n = 32) were in receipt of opiate drugs, which included Tramadol,Oxycontin, MST and Oramorph. Thirty-six per cent (n = 18) were prescribed selective serotonin reuptake inhibitor antidepressants, and 44% (n = 22) were prescribed Pregabalin or Gabapentin. Sixteen per cent (n = 8) were taking non-steroidal anti-inflammatory drugs, and 46% (n = 23) were prescribed a tricyclic antidepressant. Although no patient had undergone amputation of the affected limb, 8% (n = 4) had requested this procedure.
Subgroup comparisons
A significantly higher rate of a past history of substance/alcohol abuse was found in male patients with CRPS (35% vs. 6.7%; df = 1; χ2 = 6.527; p = 0.011). Patients presenting with CRPS in the upper limb only were significantly less likely to be male (29% vs. 66.7%; df = 1; χ2 = 5.906; p = 0.015), to have a history of substance/alcohol abuse (9.7% vs. 33.3%; df = 1; χ2 = 3.937; p = 0.047) or to utilise assistive technology (25.8% vs. 66.7%; df = 1; χ2 = 7.086; p = 0.008). There was a significant difference (t[25] = 2.08; p = 0.048) in the scores for BIPQ control item between patients presenting with CRPS in the upper limb only (M = 2.60; SD = 3.36) and patients presenting with CRPS in the lower limb only (M = 5.71; SD = 3.55). No other demographic or psychopathological differences between subgroups reached a conventional threshold of statistical significance (p<0.05).
Illness beliefs
Beliefs expressed by patients were typically negative and often catastrophic. For example: ‘This doesn’t get better and spreads to other limbs’, ‘It’s burning so much there must be an infection’, ‘I am restricted by neuro-inflammation’, ‘My brain is telling me there is a problem when there isn’t’, ‘I’ve been told if I use my hand, it will end up much worse’ and ‘The veins and arteries are all burnt up inside, I don’t know what is going on there’.
Thirty patients completed the BIPQ, and no questions on the BIPQ were returned unanswered (Table 3). Scores were highest for the items timeline, identity and consequences. Mean scores for each BIPQ item are shown in Figure 1, which compares scores with those with somatoform disorders.
Symptom exaggeration and fabrication
In 22 cases, video surveillance was carried out at the request of the insurance companies involved in the claim. In two cases, the evidence was inconclusive. However, in other cases, there was evidence of inconsistency between the level of function reported by the patient at interview and the patient’s activity when they were not aware of being observed. These discrepancies often became a focus of discussion in a joint statement. For example, one patient declined examination by an expert because of extreme sensitivity of the limb. The same patient was observed on surveillance using a cell phone, driving a motor vehicle and opening a bottle of wine with the same hand, and without any apparent discomfort, despite reporting that she could not perform these specific activities. In five cases, the discrepancies were so marked as to invite a diagnosis of marked symptom exaggeration. None of these cases went to court. However, in 10 cases, there was a conference with Counsel, which often involved debate over the nature of CRPS and how the disorder was influenced by psychosocial factors. Some of these discussions brought into question the status of CRPS as a ‘medical’ disorder or as an abnormal behavioural response to pain and injury. When surveillance evidence was available, it led to discussions about the credibility of the claimant. In one case, disclosure of surveillance led to an alleged fundamental dishonest plea in the counter schedule, and the claimant settled. In 27 cases, there were joint statements between experts: 21 with psychiatrists, four with clinical psychologists and two with pain clinicians.
Discussion
Strengths and limitations
The main methodological limitation of this study is the restriction of our sample to patients who were involved in litigation, assessed within the 10-year sampling period, and referred to a consultant psychiatrist. All of these factors may have decreased the likelihood that our sample was representative of the wider population of patients with CRPS. It must also be acknowledged that our analysis did not include a control group. Our findings are not consistent with previous studies that have failed to identify a relationship between psychological factors and CRPS Type 1,22,23 or with the outcomes of cases involving CRPS that have gone to trial under the assumption that the condition is an accepted clinical entity.24,25 How can these discrepancies be explained? All patients involved in our study were seen in a medico-legal setting with access to extensive past medical and psychiatric records that included primary-care and occupational health records. As a result, it was possible for a very comprehensive medical and psychiatric assessment to be carried out. Such detailed assessments eliminate the risk of retrospective bias, but are often not possible in clinical or research settings because of time constraints.
We were unable to establish the main characteristics of the eight patients who did not meet criteria for a current somatoform disorder, but three were at the time employed. Future studies utilising larger samples might examine whether employment rates are higher in patients with CRPS who have not also been diagnosed with a somatoform disorder.
Main findings
High levels of disability were found in our sample: few were in gainful employment, and most were involved in tertiary-care treatment services. The majority had attended a pain management programme, often with no enduring benefit, and many had received invasive treatments for pain relief (e.g. spinal-cord stimulators) or were prescribed opiate drugs, which in some patients (mostly men) had led to dependence (Table 2).
Examination of previous records revealed high rates of previous psychiatric illness (Table 2). Of particular significance was the finding that nearly half of our sample had a history of at least two previous FSS such as IBS and non-cardiac chest pains and headaches/migraine, and roughly a quarter had at least three. Their lives had been punctuated by past episodes of painful functional disorders. Within the subgroup of patients in our sample with a history of panic disorder, all but two had high rates of lifetime functional complaints, functional disability and high medical utilisation.
Importance of somatoform disorders
The evidence from this study does not support the view that ‘CRPS is not associated with a history of pain-preceding psychological problems, or with somatization’. 16 High rates of previous and current somatoform disorders were found in our sample, in addition to other psychiatric disorders (Table 2). Our findings support the view of Birklein et al. 26 that patients diagnosed with CRPS have high rates of previous pain syndromes and, if involved in litigation, are likely to suffer from multiple psychiatric vulnerabilities. The role of disability and financial incentives needs to be considered, as these could have influenced the clinical presentation. In particular, symptoms and abnormal illness behaviour can be maintained for the purposes of secondary gains, when the sick role confers sympathy, attention and potential financial and other benefits. 27
Our findings are also consistent with a recent retrospective study of 190 patients with CRPS conducted by Birley and Goebel 28 who found that one third of their sample reported pre-existing pain in the affected limb, with 11% reporting widespread pains. Significantly, 29% of patients in this latter study reported concomitant pains that had not been documented in the patient’s notes – most commonly IBS, migraine and back pain. In another recent study, fibromyalgia was recognised as a predictor of CRPS after distal radius fracture. 29 Our findings should encourage clinicians to enquire carefully about histories of previous additional pains in the assessment of patients with CRPS.
CRPS type 1 and functional neurological symptoms
In nearly half of our sample, CRPS symptoms were associated with functional neurological symptoms (Table 2). In the upper limb, these symptoms included ‘claw hand’, functional weakness and tremor. In the lower limb, equinovarus deformity or restless legs were frequently reported. This was perhaps not surprising, as these symptoms resemble those listed in the Budapest criteria for CRPS, 4 and other studies have documented similar findings. 26 Within our sample were three patients who expressed difficulty in knowing where the limb was positioned, which can occur in patients with both CRPS and functional neurological symptoms. 30
There are marked similarities between the dystonia thought to be associated with CRPS and psychogenic dystonia. 31 Fixed dystonic postures have been described as one of the movement disorders most frequently associated with CRPS. 32 Our findings suggest that patients assigned a diagnosis of CRPS often have co-existing functional neurological symptoms and signs. More florid motor signs such as choreathetoid movements and clenched-fist syndrome are likely to be manifestations of functional movement disorders. 33 It also seems likely that CRPS symptoms associated with functional motor symptoms such as weakness, dystonia, impaired limb function and limited range of motion are more likely to persist in the long term and worsen the prognosis. 8
Symptom exaggeration and fabrication
Mailis Gagnon et al. found a period prevalence of 15–27% of self-induced disorders among female patients referred with CRPS to their pain clinic. 12 They noted that this high prevalence could not be generalised to other populations because of selection bias: their clinic accepted cases involving treatment resistance and diagnostic difficulty. We did not detect any evidence of self-induced illness, but of the 22 patients in whom surveillance was available, inconsistencies were sufficiently marked in five cases to question the credibility of the claimant. We note that such cases are rarely referred to in published accounts of CRPS in legal reports. 34 One explanation for this is that when fundamental dishonesty is pleaded in a counter schedule following disclosure of surveillance evidence, the claimant often settles. These outcomes are rarely referenced in the legal (or medical) literature.
Lack of diagnostic consistency
Previous authors 35 have described lack of inter-rater reliability in the diagnosis of CRPS, and it is clear that a lack of a unifying explanation for the clinical presentation can account for this. In our sample, we found a large number of cases involving either disagreement between the treating clinician and the medicolegal expert, or a disagreement between medicolegal experts (Table 1). In either event, the diagnosis did not appear to be secure in a medicolegal context.
How can these findings be explained? Within a medicolegal framework, patients with limb pain(s) following an injury/accident may become involved in a complex system where iatrogenic factors and disease labelling shape their attitudes and beliefs. This results in avoidance behaviour (e.g. inactivity of the body part) and vigilant preoccupation with the affected limb, often associated with fixed posturing and high levels of anxiety. 7
It has been suggested that the pain in CRPS represents an exaggerated or protective response to an ‘injury’ that has been perceived as a threat, often mediated by catastrophic thinking. 8 This was manifest in the responses of our sample on BIPQ items including consequences, timeline, identity, concern and emotional response (Figure 1). Their scores for these items were considerably higher than those typically reported by patients seen in pain medicine, rheumatology and orthopaedics services for organic problems 22 and are closer instead to scores associated with somatoform disorders 36 and other disorders heavily mediated by psychological factors such as IBS. 37 The same was true for the lower perceived control of symptoms reported by our sample. Elevated concern, identity and emotional representation and consequences scores are associated with poorer quality of life – and indeed the co-morbid psychopathology (e.g. depression) observed in our sample. 21
Conclusions
Patients assigned a diagnosis of CRPS who become involved in litigation have high rates of both functional neurological symptoms and somatoform disorders associated with pain-related disability. Nearly half report a previous history of at least two recurrent FSS, and past histories of depression and panic disorder are common. This suggests that they have a pain vulnerability or pain sensitivity influenced by both genetic and environmental factors. 38 Our patients represent a subset of vulnerable patients who are markedly predisposed to respond to pain in an exaggerated fashion – especially if they become involved in litigation. The finding of diagnostic disagreement among clinicians suggests that in a medico-legal setting, the diagnosis of CRPS is often insecure. It is not surprising that doubt and uncertainty occurs in the mind of the patient.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.