
Abstract
Open disclosure is a valuable process which has the potential to benefit both the patients who receive the open disclosure and the health care professionals (or organisations) who provide it. The benefits from open disclosure will most often be seen when open disclosure is performed in an ‘ideal’ manner. When open disclosure is suboptimal, it can lead to harmful consequences for patients and health care providers alike. Numerous factors may contribute to an inadequate open disclosure including: potentially inadequate legal protection for health care professionals or organisations; failing to meet patient and/or family expectations; health care professionals experiencing a lack of education, training and support from the health care organisation; or a fear of litigation. An inadequate open disclosure may result in inadvertent consequences including: patients/families who are dissatisfied; potentially preventable litigation; legal repercussions for health care professionals and organisations; and patient harm where open disclosure is not implemented. This article seeks to explore these barriers and considers how the implementation of open disclosure could be improved to overcome these barriers. Overcoming these barriers should help to reduce the risk of inadvertent consequences and lead to better outcomes for patients, health care professionals and health care organisations.
Introduction
Open disclosure in Australia is defined as ‘the open discussion of adverse events that result in harm to a patient while receiving health care with the patient, their family and carers’. 1 While the practice of open disclosure is well entrenched in the Australian health care system, it often falls short of what families and patients expect. 2 Many health care professionals (HCPs) remain apprehensive of engaging in open disclosure, because of a fear of liability. 3 In addition, almost half of the Victorian public health services board members were not familiar with the national Open Disclosure Standard, 4 and the recently investigated Djerriwarrh incident 5 reported that open disclosure did not occur despite clear evidence of preventable patient deaths. 6 (The Djerriwarrh incident involved a cluster of perinatal deaths occurring in 2013–2014. A number of these deaths were avoidable and related to common deficiencies in care. This incident led to a broader scale review into the Victorian hospital system, seeking to eliminate preventable harm.) This raises the question of whether the good intentions behind open disclosure are resulting in inadvertent adverse consequences. The principles surrounding open disclosure are sound and it should be an important component in the provision of care. Patients expect and deserve to be advised when their health care has caused them harm. This transparency and accountability should be of benefit both to the patient and HCPs. Like any other intervention, if executed poorly the benefits of open disclosure are unlikely to be seen.
The health care and legal sectors face challenges implementing and responding to open disclosure as it was intended. Some of the core unresolved issues include: open disclosure not occurring, 7 inadequate legal protection for HCPs and health care organisations (HCOs);8–10 HCOs which are understaffed and under-resourced; fear of litigation; 3 and HCPs being inadequately prepared to enact open disclosure. 2 This failure to effectively implement open disclosure has the potential to reduce patient confidence, compound harm already experienced and promote a greater level of defensive practice that increases the costs of health care.
This article explores the potential for inadvertent adverse consequences of open disclosure by first describing the historical context, the elements and stakeholders involved in open disclosure and the value of open disclosure, before beginning to address five problems surrounding open disclosure in Australia and how these may be overcome. These problems include: (a) open disclosure not occurring; (b) adequacy of legal protection; (c) failing to meet family/patient expectations; (d) lack of education, training and support; and (e) a fear of litigation. We address, in turn, the potential consequences for each of these problems and how they could be addressed.
Context
Historical context
Historically, the approach to patient harm caused by medical error encouraged caution and non-disclosure, including concealment. 11 Open disclosure was first implemented in the United States of America (USA) in 1987 when the Lexington Veteran Affairs Medical Centre introduced a full disclosure policy following the loss of two major malpractice cases. 12 Variations of this policy were subsequently adopted rapidly throughout the USA before Australia, among other countries, also introduced open disclosure policies. 13 In Australia the first open disclosure policy, the ‘Open Disclosure Standard’ was introduced in 2003. 1 This standard was reviewed in 2012 by the Australian Commission on Safety and Quality in Health Care to examine whether the standard reflected best practice and the latest evidence. 14 The following recommendations were made: framing open disclosure as an ongoing dialogue; encouraging timely acknowledgement; clarifying what constitutes an apology; recognising the needs of patients; and the provision of support to staff by HCOs. 14 This led to the implementation of the ‘Australian Open Disclosure Framework’ (AODF) in 2013 which adopted the recommendations from the review. 1
Elements of open disclosure
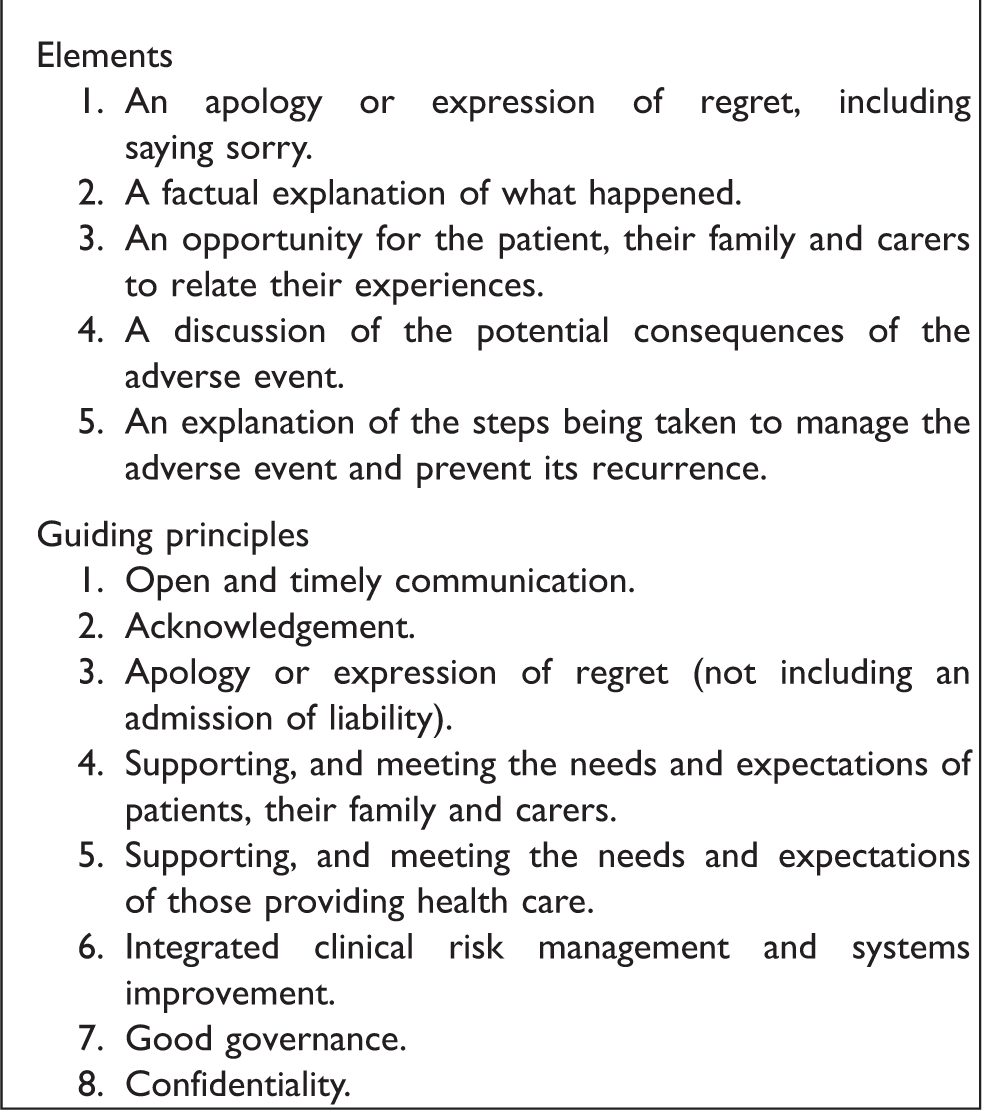
The overarching objective of open disclosure is to reduce adverse events and create a culture free from blaming individuals, focusing on creating organisational responsibility.1,15 Specifically, open disclosure aims to: improve patient safety and care through organisational learning; increase trust between patients and HCPs; assist patients to recover from harm; and support HCPs through unintended patient harm.1,15 The 2013 AODF (Box 1) also aims for open disclosure to be implemented in line with the particular HCO’s policies, risk management processes, resources and relevant laws and requirements of insurance/employment contracts. 1 Given the historical context for the development of open disclosure, it may also be suggested that a primary aim of open disclosure is to prevent litigation. 12 This is rarely explicitly stated. It is perhaps assumed that is addressing and satisfying the concerns of a patient may in turn reduce the likelihood of litigation.
Elements and principles from the Australian Open Disclosure Framework. 1
Stakeholders in open disclosure
To enact an effective open disclosure process it is imperative that all parties involved receive the necessary support and are adequately equipped to engage in the process. The key stakeholders comprise: the HCO; the HCP; the patient and their family/guardian/carer. Once the patient and/or family is contacted and a meeting is organised, open disclosure should involve a discussion between all stakeholders and be an ongoing process, rather than a single meeting. 1 The discussion should begin with the relevant HCP providing an apology and explanation of the incident; what should follow is an opportunity for the patient and/or their family to present their perspectives and the impact of the adverse event. 1 An open disclosure plan should also be devised, outlining what the patient/family hopes to achieve from the process and the questions to be addressed in future meetings. 1
Role of the HCO
The 2013 AODF provides that HCOs should provide open disclosure training as part of professional development. 1 The HCO needs to be well equipped to deal with the specific needs of vulnerable patients. Specific provisions are made for some groups of patients in the AODF including: children, patients with cognitive impairment, Aboriginal and Torres Strait Islanders patients and culturally and linguistically diverse patients. 1 The HCO should be involved throughout the open disclosure process, including in discussions with patients and their families. Under the AODF, the HCO should also provide patients/families with information about support services, including patient advocates. 1 The HCO should have quality systems including root cause analysis processes that are effective in determining whether the error constitutes a systemic failure and how similar errors can be prevented in the future.
Role of the HCP who made the error
The HCP should engage in an honest discussion with the patient and their family, including offering an apology for what went wrong. They should reflect upon the adverse event and their role in it, to determine how they could prevent similar events in the future.
Role of the family/patient
An honest discussion requires active contribution by the patient and/or their family. Although they may be upset and even angered by the adverse event they will usually be seeking an explanation and apology, for similar errors to be prevented, and for the HCP or HCO to be held accountable; financial compensation may also be sought.16,17 They may have questions, and the discussion should include active listening by the HCP to reduce the risk that the discussion becomes a didactic monologue. HCPs should receive training in this aspect of the process from the HCO. 1
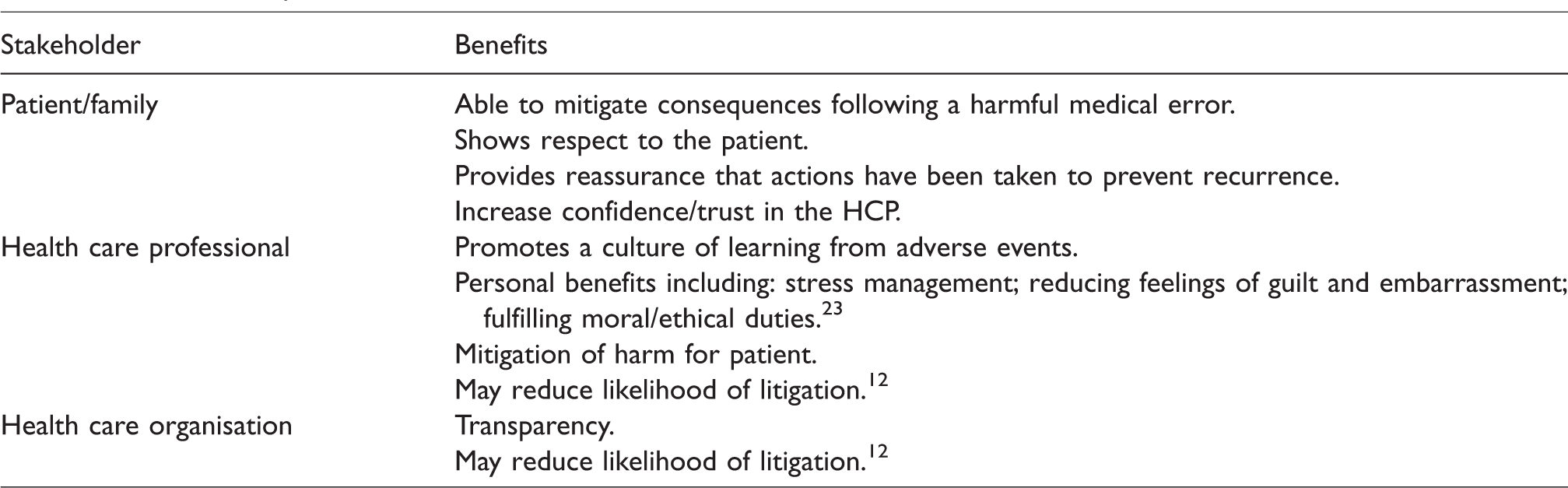
Value of open disclosure
Open disclosure is valuable to all parties affected by medical error (see Table 1). The quality of open disclosure provided impacts on the benefits to all parties involved in the open disclosure process. An example of an ideal open disclosure process, based upon the AODF, 1 is provided below.
Benefits of Open Disclosure
The ideal open disclosure
The error is recognised early by the HCP and HCO and the adverse event is adequately investigated. They enact open disclosure only after gathering sufficient information, but avoiding inordinate delay. The open disclosure process is ongoing – it is not a single meeting to be forgotten about. The HCP and HCO reflect on the adverse event and consider what steps may be taken to prevent its recurrence, and agree to provide feedback as it becomes available. Prevention opportunities will also be communicated to the wider health care community, including specialist craft groups and clinical governance agencies. This focus on wider prevention can assist patients in recognising the positive outcomes that the open disclosure process will lead to.
The HCP will be adequately prepared and well informed of the open disclosure process. They are committed to improving patient safety and communicating what went wrong to the patient. The communication should be an honest recount of what went wrong and why, including the steps the HCP and HCO are taking to prevent errors in the future. The HCP provides a sincere apology, without admitting liability. The HCP is supported by the HCO and receives ongoing training throughout the course of their employment. The patient and their family are involved in the discussion and receive answers to their questions. They are satisfied with the open disclosure process and are treated with dignity and respect.
Problems and solutions
Open disclosure offers promise to patients, families, HCPs and HCOs alike. Despite this, open disclosure may lead to a range of negative inadvertent consequences at each stage of the process (see Figure 1). HCPs and HCOs should be aware of the possible failures at each stage of the process and should look to prevent each from happening wherever possible. Many of the failures result in HCPs and HCO engaging in a less than an ideal open disclosure, potentially leading to suboptimal quality healthcare (see Box 2).

Problems at each stage of the open disclosure process.
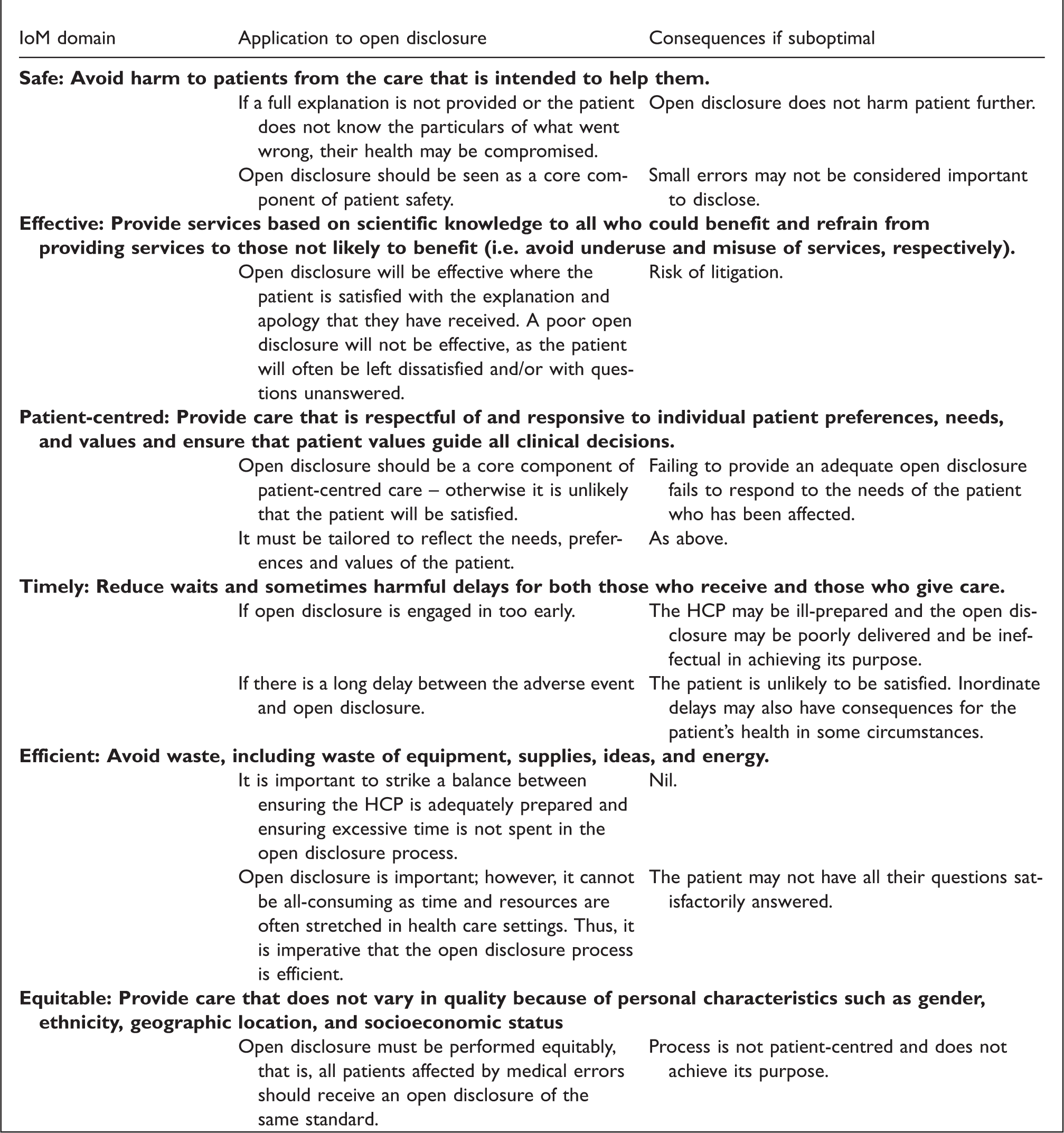
Open disclosure as a clinical intervention according to the Institute of Medicine’s domains of healthcare quality.
Problem 1: Open disclosure does not always happen
An Australian study from 2003 examining hospital disclosure practices found that an open disclosure process did not always occur. 7 Despite the implementation of the AODF, gaps in open disclosure still exist. This is evidenced in that only 18% of persons aged above 45 years who experienced an adverse event were engaged in a formal open disclosure process. More disturbing is that some participants were not offered open disclosure. 18 This is not surprising as medical errors are often under-reported,19,20 and unless an error is reported, it is unlikely that open disclosure will occur. Despite the presence of a national open disclosure framework, there is an absence of legislation to enforce the practice of open disclosure. Public hospitals and health services in Victoria must comply with the standards under their service agreements (National Safety and Quality Health Service Standards, standard 1). 21 The absence of enforcement is most likely based on the assumption that open disclosure is the ‘right thing to do’, 22 and that it may benefit all interested parties (see Table 1).1,12,14,23 It has been found that perceiving open disclosure as a moral and professional duty is one of the greatest enablers of open disclosure. 23 The common law may also support the need for open disclosure; however, it does not mandate it, beyond the duty to disclose medical errors, 24 and inform of outcomes post-treatment. 25
Given the open disclosure framework is not mandated or enforceable, HCOs and HCPs can potentially avoid disclosing errors to patients. Doctors have been hesitant to engage in the practice of open disclosure; 26 the reasons for this will be addressed below. Smaller errors are less likely to be disclosed than ones with serious/life-threatening consequences; 7 this may be based upon the assumption that patients do not necessarily need to know, or that the error can easily be ‘covered up’. Despite this, serious errors may remain undisclosed and ultimately lead to further harm for the patient. 6 Patients have a right to know where an error (no matter how small) occurs, and the patient’s right to an honest disclosure should be considered paramount.
To combat problems of under-disclosure, the United Kingdom (UK) implemented a duty of candour in the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014(UK) 27 (reg 20; see also s 20 Health and Social Care Act 2008 (UK) and s 81 Care Act 2014 (UK)) which took effect in November 2014. There is limited empirical data on the impact of this change on the frequency of open disclosures. An analysis of the Care Quality Commission’s 59 inspections conducted in 2017 showed that duty of candour was assessed in the majority of cases, but there was limited information on the outcome of the assessment. 28 This has raised concerns about the effectiveness of the regulation’s enforcement. In Victoria, it has been recommended that a statutory duty of candour be introduced. 6 This aims to ‘embed the commitment to the principles of open disclosure across the health system’, improve the uptake of open disclosure and make the responsibilities and requirements of open disclosure clearer.
It is not clear whether mandating open disclosure will improve rates of open disclosure. It is likely to depend largely on the consequences of breaching the duty. One relevant factor to consider is if a failure to implement open disclosure would give rise to a new legal claim which could be initiated by the patient or their family. Another factor is whether failing to implement open disclosure should become an offence. In the UK it is an offence for HCOs to fail to comply with the statutory duty of candour (reg 22(3)27). If the same is proposed in Victoria, it should encourage disclosure of medical errors thereby increasing the ratio of open disclosures per adverse event. Prior to the enactment of the statutory duty of candour in the UK, it was recommended that sanctions should impact upon the organisation’s reputation to encourage compliance with the duty. 29 If there are no sanctions imposed and no fundamental changes in education on disclosure/duty of candour, it seems unlikely that the frequency of open disclosures will increase, as there is no further incentive than what already exists to comply with open disclosure.
Problem 2: Potentially inadequate legal protection
Apology laws
Under the AODF, the first element of open disclosure is an apology. 1 The protection provided by the apology laws is imperative to ensuring that HCPs can openly disclose without fear of punishment; however, the protection offered is limited, as they do not cover other elements set out in the AODF. 9 General protection is offered to HCPs by the ‘apology’ laws, implemented in all Australian states. 10 In effect, they all state that an apology is not an admission of fault or liability and cannot be used as a determination of fault or liability; however, only some states protect apologies that include a clear admission of fault. 10
This is problematic, since Iedema et al. 8 found that patients were often dissatisfied where partial apologies were provided (whereby responsibility/fault was not assumed). Allan et al. 30 found that even imperfect apologies could be considered acceptable; however, what constituted a ‘basic apology’ included an admission of fault. This illustrates that the requirements of the AODF and the protection provided by apology laws are at odds with patient expectations. An additional factor to consider is ensuring that the apology provided is sincere; patients expect a sincere apology, 31 and an apology is often only perceived as sincere where an admission of fault is made. 7
Because HCPs are concerned about not being adequately protected by the law, they are unlikely to apologise in a way that satisfies the patient’s expectations. 32 This may lead to a lack of trust/respect in the HCP as patients may perceive that HCPs are protecting themselves, rather than acting in the best interests of the patient. This has the potential to lead to the patient taking further action (perhaps even turning to litigation). 33
Given that there is a national framework, there is also a clear need for consistency in the apology laws across Australia. Reforms to the apology laws should consider the requirements of the AODF and work to provide consistently adequate protection for HCPs. They should also reflect that patients want an apology which includes an admission of fault; 8 this would also mean changing the AODF’s definition of apology to including an admission of fault.
Admission clauses
Where apology laws provide protection for admissions of liability, HCPs may trigger a breach of the admissions clause in their insurance contract. 34 This indicates that HCPs need to be cautious to ensure that they do not make inadvertent admissions which may cause the insurance provider to refuse to assist with any legal action. 34 The same issues surrounding apology laws may arise, resulting in patient dissatisfaction. 8
The AODF does not provide that an HCP should make an admission and thus the quality of open disclosure should not be affected. Adequate preparation and support prior to open disclosure meetings may also assist in ensuring that HCPs to not inadvertently make admissions.
Problem 3: Meeting patient/family expectations
Iedema and colleagues
2
found that patients and their families expressed many concerns with the open disclosure process including:
inadequate preparation for the disclosure inappropriate disclosure of unexpected outcomes lack of follow-up support lack of appropriate disclosure insufficient integration of open disclosure with improvement of public safety
A lack of patient satisfaction may lead to litigation as patients seek more information, monetary compensation and to hold the organisation accountable.16,17 Patients may lose trust and/or confidence in the HCPs or HCOs if open disclosure is not performed in accordance with their expectations. Where patients are not provided with all necessary details, there is the potential for the incurrence of further harm.
35
These problems largely come down to the fact that HCPs are not putting in place an ‘ideal open disclosure’. They may also arise out of fears of litigation, inadequate legal protection, or lack of education. Addressing these problems may help the HCP to meet the family expectations; however, this will not be sufficient.
In addition to alleviating the fears of HCPs, there needs to be a shift in mindset surrounding the open disclosure process. HCPs need to view open disclosure as an integral component of patient-centred care and consider it part of their duty of care to the patient. Framing open disclosure as both a moral and professional obligation as well as a legal requirement may assist in encouraging HCPs to engage in open disclosure. 23 The focus should be on helping the patient by providing them with necessary information regarding the incident and answering any questions they may have. HCPs should avoid appearing overly defensive and focus not on avoiding litigation or complying with the process, but rather on supporting the patient and their family and treating them with dignity and respect. HCOs and HCPs should be aware of the concerns expressed by patients and their families in the Iedema et al. study 2 and seek to address these challenges.
The HCP should also consider the needs of the patient and tailor the open disclosure process accordingly. This client-focused requirement can be seen, for example, when considering the needs of parents of children who have suffered adverse events and rural patients who may need a specifically tailored process.
These examples illustrate the need for the open disclosure process to focus on the needs of the patient and their families, to listen to what they want and to tailor the process accordingly.
Problem 4: Education, training and support
The 2013 AODF provides that HCOs should provide open disclosure training as part of professional development. 1 The new framework is clearer about the need for education and training than the old Open Disclosure Standard; however, the impact of this is difficult to quantify. Lack of education and training has been identified by health professionals as a major barrier to the open disclosure process. 3 While education provided to HCPs in specialist craft programmes appears adequate, 38 the extent of training and instruction which occurs in the general workplace is unclear. The lack of patient satisfaction from the open disclosure process, resulting in part from a perceived lack of preparation for open disclosure,2,23 illustrates that workplace training and education may be lacking.
Inadequate training, education and support of HCPs engaging in open disclosure will most likely lead to a poorly communicated open disclosure. 3 This can have a wide range of consequences, as illustrated in Figure 1. Without adequate training and education, the HCP is unlikely to engage in open disclosure to the standard expected by the patient, and is far more likely to make errors which may ultimately lead to civil or administrative legal repercussions, including where HCPs are not reminded of the legal apology requirements.
Given that open disclosure is designed to be implemented in a ‘flexible’ manner, according to the HCO’s policies and resources, 1 all new HCPs at an HCO should be advised of the open disclosure policy and requirements specific to that HCO. In addition to generic support and training for all staff members, following an adverse event, extra support in preparation should be provided to the HCPs involved, before open disclosure follows, aiming to ensure the patient is satisfied with the disclosure they receive. A key to enabling support and training is ensuring that the HCO is adequately resourced to allow for this. HCOs need to consider the importance of setting aside time for education and enactment of open disclosure. While adverse events requiring open disclosure are relatively rare, HCOs are often understaffed and thus HCPs may feel as though they are required to rush through the open disclosure process, which is unlikely to result in satisfactory outcomes. Adequate time and resources need to be allocated to open disclosure to ensure patient satisfaction.
Problem 5: Fear of litigation
Many HCPs remain apprehensive of engaging in open disclosure, because of a fear of liability. 3 This is fuelled largely by a lack of education and training in open disclosure, as well as a perceived lack of protection by the law, in part because of a lack of understanding of the law. 3 This fear of litigation may lead to HCPs failing to engage in open disclosure in the first place, or practising defensive medicine whereby they fail to adequately disclose the extent of the error. 3 This fear is likely to lead to a lack of patient satisfaction, as it is unlikely the open disclosure provided will adequately meet the needs of the patient. As a result, this fear on the part of HCPs may actually increase a patient’s desire to proceed to litigation, as discussed under problem 3.
Open disclosure in some settings within the USA has reduced the likelihood of patients litigating, as well as reducing the costs of claims.12,39,40 However, broad-based empirical evidence on this issue does not exist. 41 A 2014 USA study into gastroenterology-related adverse events found a reduction in number of claims and time to claim resolution following the implementation of a medical error disclosure programme. 39 Conversely, Studdert et al. 11 have suggested that open disclosure may result in increased litigation; however, this appears to be at odds with the bulk of research on the topic.12,39,40 Given the majority of research has been conducted in the USA, it is difficult to determine whether the results will be replicated in Australia because of differing proportions of litigation (litigation rates are approximately 3.7 times higher in the USA) 42 and a lack of broad-scale evidence on the issue. 41
Given that a major motivation for initiating a medical indemnity claim is seeking explanation and apology,16,17 many patients may be satisfied if they experience an adequate open disclosure process. Even a perfect open disclosure may be insufficient to prevent litigation – some patients may be highly litigious. They may be motivated by financial considerations, a wish to blame individuals as a form of retaliation, or from altruistic attempts to ensure others do not suffer in the same way.16,17 It is important to consider that such litigation would not result from open disclosure process problems per se, but rather from the impact of the original medical error itself.
The fears surrounding litigation following from open disclosure are unlikely to be able to be substantiated as there is an absence of cases before courts on the matter of open disclosure. Overcoming this barrier again requires education (on the law surrounding open disclosure) and ensuring that adequate legal protection is provided for HCPs/HCOs enacting open disclosure. It also requires empirical evidence on the impact of open disclosure on medical negligence claims in Australia. Until empirical evidence exists, this fear of litigation is unlikely to be completely alleviated.
Conclusion
Open disclosure is a valuable process but can sometimes lead to inadvertent consequences. Patients deserve and expect an open disclosure process which may resolve their concerns and militate against future litigation, and yet if the disclosure process is impaired the result may cause further patient harm and increase the potential for civil litigation. A key aim of open disclosure is to improve patient safety and outcomes and yet, as highlighted herein, there remain numerous barriers to its successful implementation as a well-established process. Impeding factors include a continued fear of litigation by HCPs, together with a perceived lack of legal protection with the existing state-based laws; a lack of education and general support of HCPs to enable the process to be adequately implemented; and lastly, the ability for the process to meet patient and family expectations. Further exploration of such barriers would enable an evidence-based approach to reform in this area.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.