
Abstract
Traumatic abdominal wall herniation, especially of the groin region, is a rare condition and typically results from a high-energy trauma to the abdominal wall. We report a fatal case of a road-traffic collision involving a young male motorcyclist who collided with a speeding lorry. The victim sustained multiple injuries over the chest and abdomen, with traumatic inguinal herniation causing gross distension of the scrotum. At autopsy, multiple lacerations of thoracic and abdominal organs were seen, along with traumatic disruption of the right inguinal canal. The contused terminal ileum was present in the scrotal sac. A literature search has revealed a limited number of reported cases of gross inguinal herniation following thoracoabdominal trauma. In cases of high-energy trauma to the thoraco-abdominal region with unilateral or bilateral distension of the scrotum, the possibility of herniation of the abdominal contents into the scrotal sac should be considered by the forensic pathologist.
Introduction
A traumatic abdominal wall hernia (TAWH) is described as a hernia produced due to trauma disrupting the muscles and fascia without penetrating the overlying skin and in the absence of a previous hernia defect at the site of the impact. 1 TAWH was first documented by Selby 2 more than a century ago. TAWH, especially of the inguinal region, is a rare condition in the clinical setting, with a high risk of associated intra-abdominal injuries. 3 The three potentially weak areas of the abdominal wall – the inguinal region, the region lateral to the rectus muscle and the region above the iliac crest in the flank region – are the common sites for TAWH. 4 The inguinal canal lies over medial half of the inguinal ligament and extends from the deep inguinal ring to the superficial inguinal ring. The literature on traumatic cases with gross disruption of the inguinal canal is limited.5,6 We present a fatal case of traumatic inguinal herniation with complete disruption of all boundaries of the inguinal canal, including deep and superficial rings, causing traumatic herniation of 90 cm of the terminal ileum into the scrotal sac. The reported case highlights an incidental finding of traumatic inguinal hernia, which at times can have serious clinical and medico-legal considerations.
Case report
A 20-year-old male motorcyclist was brought dead to the emergency room with an alleged history of a side-on collision and subsequent run over by a speeding lorry. During autopsy, on external examination, multiple impact and grazed abrasions were present over the chest and abdomen (Figures 1 and 2). Gross distention of the scrotum was evident (Figure 1). Internal examination revealed a fissure fracture of the anterior and middle cranial fossa on the left side, a complete transection of the cervical vertebrae between C5 and C6 and multiple fractures of the sternum, clavicle and ribs bilaterally. Thoracic and abdominal wall examination revealed multiple contusions. All the thoracic and abdominal organs had multiple contusions and lacerations. A significant defect was evident in the lower abdominal wall through which around 90 cm of the terminal ileum was herniating into the scrotal sac (Figures 3 and 4). The cause of death was opined as multiple injuries sustained to the head, neck and trunk. Prior history of inguinal hernia was excluded by asking relatives.

Multiple grazed abrasions over the left side of the trunk and gross distension of the scrotum.

Multiple impact abrasions over the right side of the trunk suggestive of tyre imprint abrasions caused by run over.

Large defect in the right-sided lower part of the anterior abdominal wall through which the terminal ileum is herniated into the scrotum.
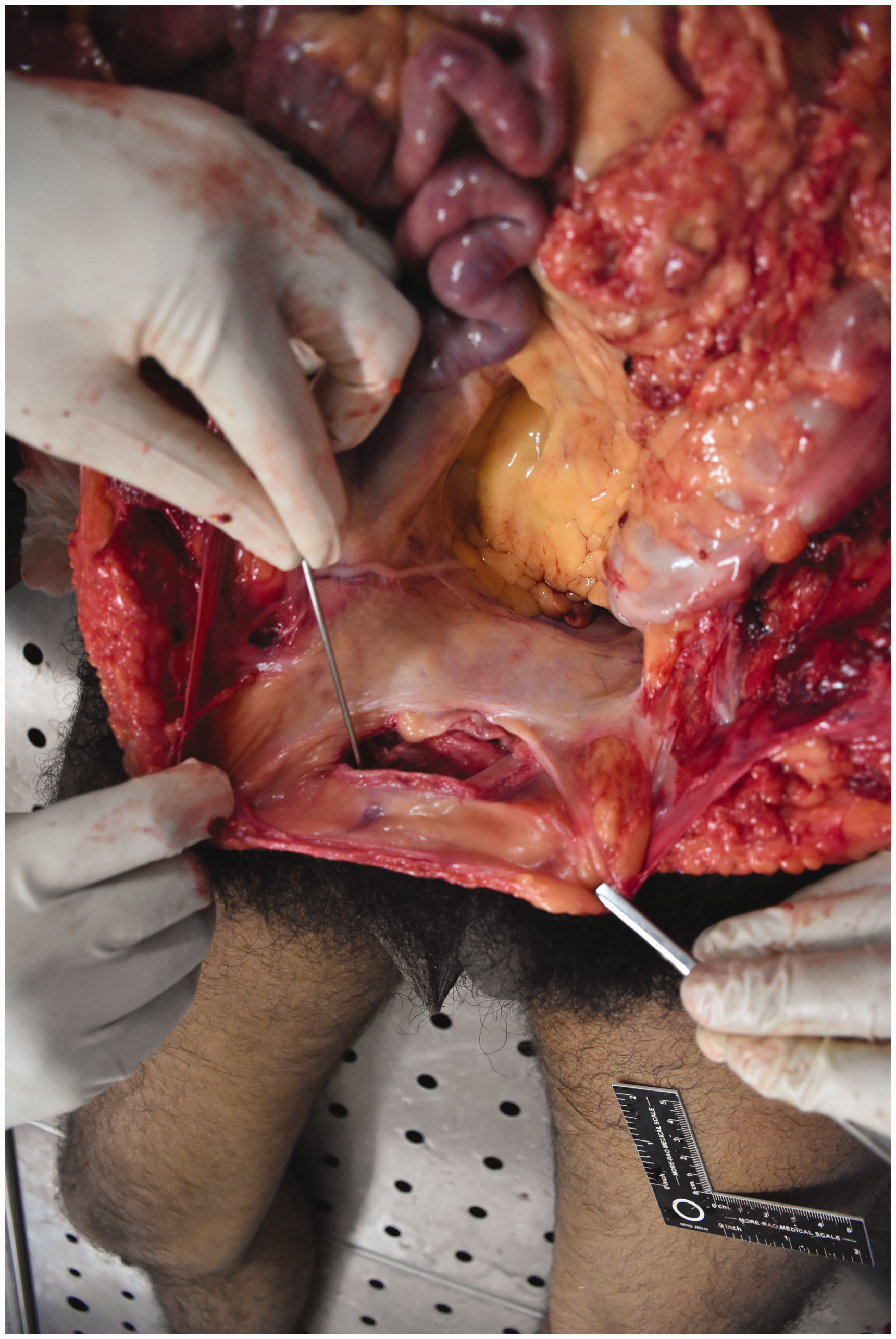
Large defect in the right-sided lower part of the anterior abdominal wall with complete disruption in the inguinal canal, as evident after removal of the terminal ileum that traversed through it into the scrotum. A probe was inserted through it into the scrotum.
Discussion
The association of blunt trauma to the abdomen and a traumatic inguinal hernia is not infrequently reported in surgical practice. However, traumatic herniation of the intestine remains a rarity in medico-legal autopsies. The most common aetiological factors for traumatic herniation include low-energy trauma such as handlebar injury, bullhorn, sports and seatbelt injuries and high-energy trauma due to road-traffic accidents. 7
Three types of TAWHs are defined according to the mechanism of injury: type 1 TAWH that describes small hernia in the anterio-inferior abdominal wall and inguinal region caused by low-energy blunt trauma (e.g. handlebar injuries); type 2 TAWH that are large hernia defects caused by high-energy trauma such as road-traffic accidents; and type 3 TAWH that are rare variants seen in acute deceleration injuries. 8
Blunt trauma to the abdomen can lead to the application of tangential and shearing forces over the abdominal wall, which causes disruption of the abdominal wall muscles and fascia that may result in herniation of the abdominal viscera. As traumatic forces on the abdomen are distributed over a broad area and the skin is more elastic than other layers, the skin usually remains intact. 9 A sudden increase in intra-abdominal pressure along with the shearing effect on the abdominal muscle and fascia is considered the primary aetiological mechanism in the development of traumatic hernias. Further, diffuse high-energy impact to the abdomen can cause a large abdominal wall defect, and its association with intra-abdominal injuries is very high. The incidence of intra-abdominal injuries in cases of TAWH is reported in 25–70% of cases. 10
Netto et al. 3 in their retrospective evaluation of 34 patients with TAWHs, highlighted the mechanism and severity of injuries and made clinical recommendations. First, the mechanism of injury should be taken into consideration in patient management, as high-energy traumas often require urgent exploration. Second, the visible hernia has a high probability of associated intra-abdominal injuries. Third, an occult hernia diagnosed only by radiological means may not require urgent surgical management. Clinically, the appearance of a bulge or tender swelling on the abdominal wall with or without associated skin lesions after an incident of blunt trauma to the abdomen helps establish its traumatic origin, and in doubtful cases, a contrast-enhanced computed tomography scan of the abdomen is considered a valuable tool for early detection of traumatic hernias.7,11 TAWH in itself can be a primary cause of death. It is recognised that delayed diagnosis of this condition can lead to bowel ischaemia/infarction, whilst it may also be associated with bowel perforation, both of which can prove fatal if untreated.
In cases of high-energy trauma, extra-abdominal injuries such as fractures of vertebrae and the ribs may accompany it. 12 Multiple fractures of the thoracic cage, skull and complete transection of cervical vertebrae were observed in our case which itself signifies the involvement of high-energy crush and shearing forces in the reported case. There is a high possibility of severe intra-abdominal injuries in the case of TAWH following high-energy trauma of the abdomen. Unilateral or bilateral distension of the scrotum following high-velocity trauma to the thoraco-abdominal region should raise a suspicion of TAWH after ruling out scrotal haematoma and emphysema.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.