
Abstract
We describe a case of attempted homicide by instilling elemental mercury through an endotracheal tube into the respiratory tract. Radiographs revealed the presence of metallic mercury in both lungs. During a 2-year follow-up, mercury droplets disappeared from the lungs and only mild clinical symptoms were identified, without evidence of wider toxicity or organ damage.
Introduction
Poisoning by metallic mercury is very rare. It is usually by suicidal intravenous injection,1,2 ingestion3–6 or to improve sexual or athletic performance. 2 Metallic mercury may enter through the respiratory tract by aspiration, either due to rupture of the mercury filled bag of an intestinal tube,7–9 thermometer breakage 10 or in the procedure of gastric lavage to remove ingested metallic mercury. 11 A case of mercury poisoning by application of cosmetic cream containing mercury is noted by Tang et al. 12 This is the first case of attempted homicide by instilling mercury in the endotracheal tube of a patient admitted to intensive care unit for the treatment of suicidal organo-phosphorus poisoning.
Case report
A 33-year-old married female was brought to the casualty department at around 10.30am, following a suicidal attempt in which she had consumed approximately 40mL of organo-phosphorus insecticide – Monocrotophos - at around 9am, after a quarrel with her husband. She had previous history of attempted suicide by consuming sleeping pills ten years ago. On examination, the general condition of the patient was poor: she was unconscious, pale, frothing from the mouth and smelling of organo-phosphorus compound, and her pupils were constricted to a pin-point size. Fasciculation, tachycardia with blood pressure 160/100 mm of Hg, SpO2 96% and very feeble pulse were recorded. As a part of the management, endotracheal intubation was followed by gastric lavage, and secretions from the respiratory tract were cleared by suction. Intravenous injections of atropine and pralidoxime (2-PAM) were started immediately, then she was transferred to the intensive care unit.
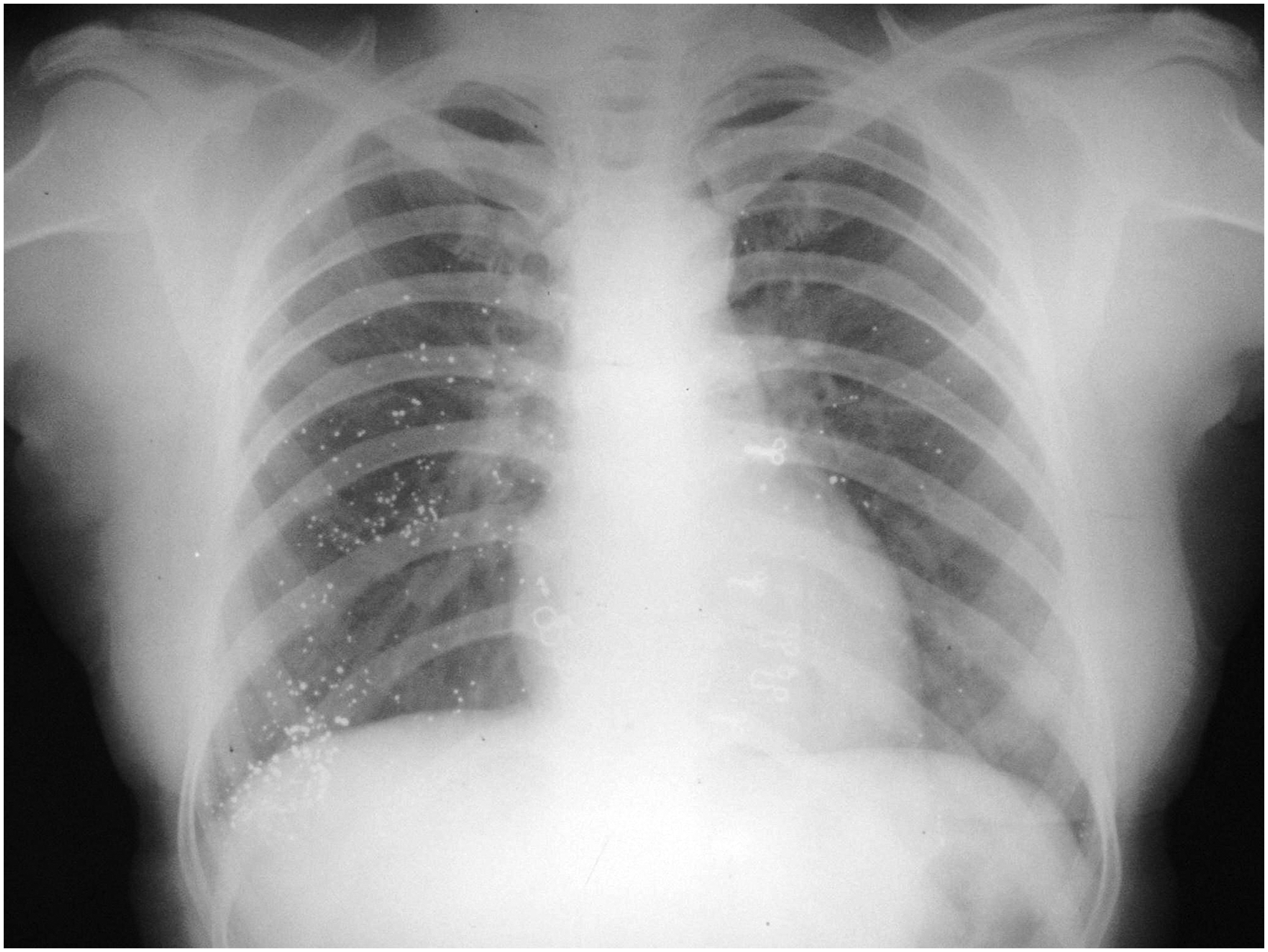
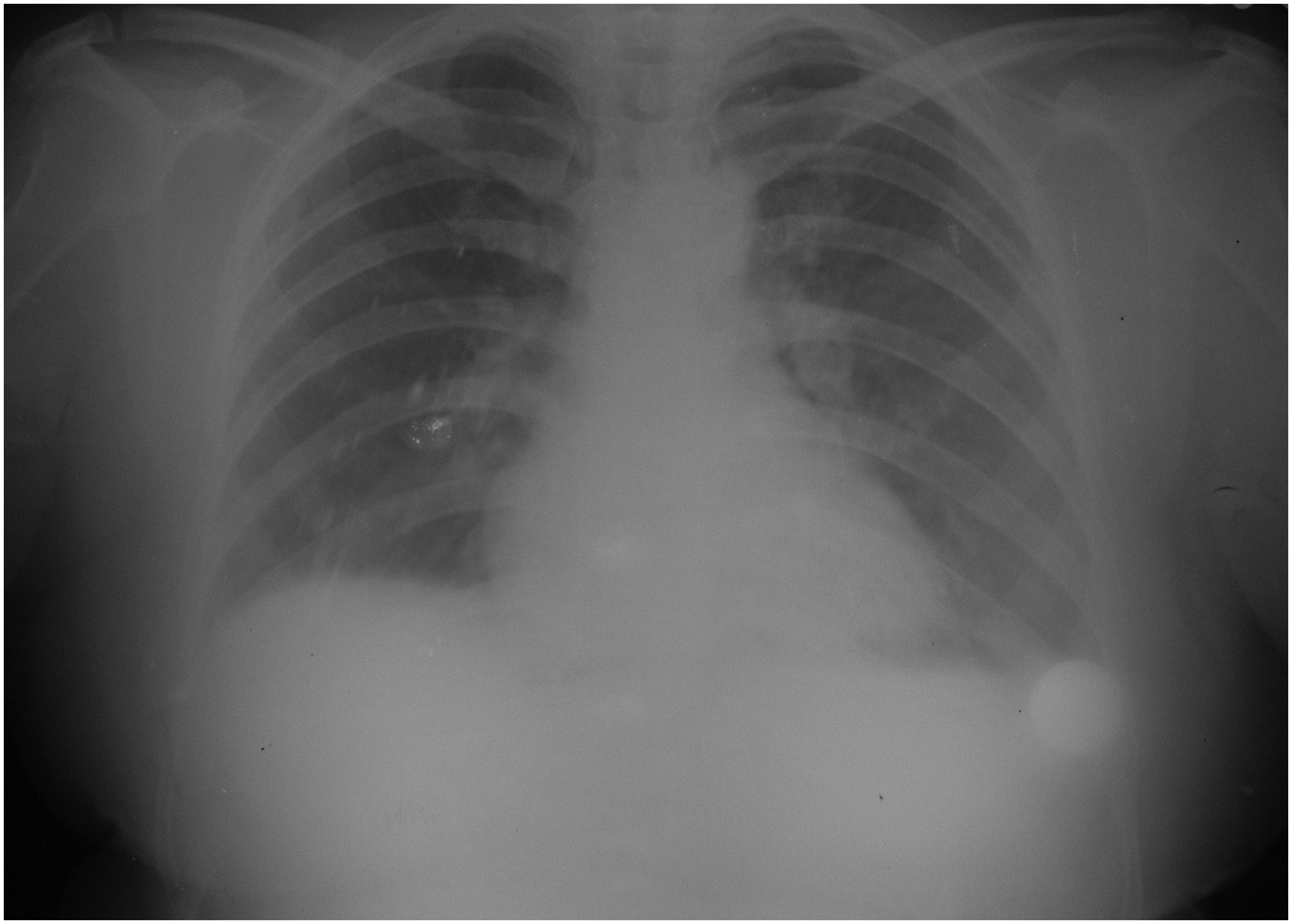
At around 3.30pm, during the visiting hour, her husband entered the unit with permission to visit his wife. After a few minutes, a visitor of the neighbouring patient saw that the husband was instilling something into the endotracheal tube. He informed the nurse and duty residents, after which medical staff rushed towards the bed of the victim, however the husband managed to escape from the unit. The endotracheal tube was immediately removed and replaced with a new one. She had tachycardia and shallow respiratory rate of 28/minute. The material that had been instilled by the husband was metallic mercury, determined by physical examination of the aspirate. It was removed from the respiratory tract by suction, frequently giving “head low” position and rotating the patient to right or left sides. Around 30mL mercury was removed using this method. Subsequent chest roentgenogram revealed that a substantial amount of mercury was still present in the lower respiratory tract (Figure 1). She gained consciousness on the third day of hospitalisation, after which around 4mL of mercury was removed by postural drainage and forced coughing. The signs and symptoms of organo-phosphorus poisoning had disappeared and the treatment for the same was stopped on the third day. She had occasional crepitations and rhonchi on chest auscultation. To remove the remaining mercury, bronchoalveolar lavage was advised. Bronchoscopy revealed that mercury was still present (Figure 2) and ∼3mL of mercury were removed. Pulmonary function tests, performed before bronchoalveolar lavage, suggested early small airway obstruction (as forced expiratory flow was 25 to 76% and peak expiratory flow rate was less than 70%) and mild restriction (as forced expiratory volume / forced vital capacity was more than 99% and forced vital capacity was less than 80%). After bronchoalveolar lavage, the results suggested that early small airway obstructions were removed, and mild restrictions were present. She developed coughing with hoarseness of the voice on the 15th day, which was treated by decongestant, steam inhalation and saline gargles. The results of her liver and kidney function tests were within normal limits and she was discharged on the 25th day. Her chest was clear and the chest roentgenogram on day of discharge revealed the presence of a few mercury droplets in the lung parenchyma (Figure 3).

Posteroanterior X-ray film taken on the second day after instillation of the mercury showing radio-opaque mercury particles giving the bronchogram effect in the left lower lobe (oblique lines are the damages caused to the X-ray film while handling).

Multiple metallic mercury particles lining the mucosa of bronchi visualised on bronchoscopy.
Posteroanterior X-ray film taken on the 25th day showing few metallic mercury particles still present in the lungs.
The patient was followed up for two years following discharge from the hospital. She had mercury droplets in her sputum for the first four months. During her stay in hospital, and for the subsequent two years of follow-up, she never had signs and symptoms of acute or chronic mercury poisoning. Her blood and urine mercury levels, measured at intervals of one month, were found to be between 14 to 18µg/L and 121 to 138µg/L respectively. As the blood and urine mercury levels were insignificant during treatment in hospital and subsequent follow-up, it was decided not to administer British anti-lewisite (BAL), ethylenediamine tetra-acetic acid (EDTA) or d- penicillamine. At the end of the second year from the episode of poisoning, the chest roentgenogram depicted that there were no mercury droplets in the lung (Figure 4).
Posteroanterior X-ray film taken two years after the instillation of mercury showing no traces of metallic mercury in the lungs.
Discussion
Mercury is the only metal that is liquid at room temperature. Its atomic number is 80; atomic weight 200.59 and density 13.50 at 37°C, with a melting point of −38.9°C. It is found in three forms - inorganic mercury, organic mercury and metallic mercury, which is also referred to as elemental mercury. Inorganic mercury, found mostly in mercuric salt, is highly toxic and corrosive. Organic mercury can be found in three forms, aryl, short- and long-chain alkyl compounds. Organic mercury compounds are absorbed more from the gastrointestinal tract than the inorganic salts. Metallic mercury has a high water-metal interfacial tension and will not wet surfaces of the respiratory tract and vessels. Metallic mercury may enter the body orally, through skin or by absorption through the respiratory epithelium. 13 It may also enter by accidental or deliberate deposition in subcutaneous, intramuscular, or intravascular sites. Within the body, the mercury may remain localised for an indeterminate period as a depot of elemental mercury (Hg0) or it may be oxidised to the soluble mercuric ion (Hg++) and distributed to other body tissues, principally the kidneys and liver. 14 Deposited mercury may take from a few months to years to disappear. 15 A case of mercury toxicity by ingesting a traditional Indian medicine containing elemental mercury was recorded. 16 Inorganic and organic mercury are much more toxic than elemental mercury. 17 Metallic mercury entering in the respiratory tract can cause direct tissue injury as well as obstruction of the bronchial tree. 18 Electrocardiogram abnormalities are recorded following self-administration of metallic mercury intravenously. 19
In this case, chest X-ray revealed the appearance of metallic mercury in the lung, as in the bronchogram, however the metallic opacities were in the form of clumps, predominantly in the lower lobes. They were not linear in appearance, as in the case of aspiration of barium or bronchographic contrast media. In cases of metallic mercury embolism, the metallic opacities are more widespread and diffused, corresponding to the course of pulmonary vessels in their pattern of arborisation.18,20
In previously reported cases of aspiration of metallic mercury, acute effects such as haemoptysis, tachycardia and cyanosis, along with hypotension, bloody diarrhoea and haematuria were described, followed by death, or survival.8,9 Acute pneumonitis 4 and immediate respiratory distress, followed by symptoms of chronic respiratory disease, 7 were also noted.
Metallic mercury globules surrounded by dense fibrous tissue in the lower lobe of both lungs were found in the post-mortem examination of a person who died 22-years following the aspiration of metallic mercury. On histological examination, these globules were surrounded by multi-nucleated giant cells, epithelioid cells and fibroblasts on the periphery. 7
Metallic mercury is commonly used as a medicinal constituent in traditional Indian medicinal preparation (Ayurvedic medicine), Hispanic, Arabic and Chinese non-allopathic medications, which makes it easily available to the customers without prescription.
In the management of our patient, even though she was unconscious and suffering from organo-phosphorus poisoning, changing position and suction proved to be of great importance in removing metallic mercury. On gaining consciousness, forced coughing and postural drainage were also helpful in removing the mercury. In a previously reported case of metallic mercury aspiration, bronchoscopy was seriously considered but deferred because of the nature of the foreign body and its diffused distribution. 9 We found that it is helpful, along with bronchoalveolar lavage, in removing early small airway obstruction. Systemic effects were not identified in this case, because metallic mercury is very poorly absorbed by the mucosa. However, it must be remembered that metallic mercury is quite toxic when inhaled as a vapour.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.