
Abstract
Mental health courts offer access to community-based care for defendants with psychiatric disorders, including posttraumatic stress disorder (PTSD). However, limited information is available on how judges make treatment decisions about evidence-based practices. In this qualitative study, we interviewed mental health court judges to evaluate: (1) perspectives toward the role of PTSD in criminal behavior; (2) knowledge about evidence-based practice for PTSD; (3) treatment decisions for defendants with PTSD; and (4) treatment decisions for defendants at risk for suicide, a common comorbidity with PTSD. We hypothesized that mental health court judges would report low familiarity with evidence-based practices for PTSD despite wide recognition of the impact of trauma on criminal behavior.
Keywords
Prisons and jails in the United States have become de facto mental health care institutions 1 despite recognition that these facilities are not appropriate for this role. 2 Up to one-third of individuals in jail have a serious mental illness 3 and many have been incarcerated for nonviolent or victimless crimes. 4 The Brennan Center for Justice estimated that 39% of incarcerated individuals could be released with no risk to public safety. 5
Psychiatric symptoms increase the rate of re-incarceration among individuals released from jail or prison. 6 Tragically, some life experiences, such as being exposed to a trauma and developing posttraumatic stress disorder (PTSD), also increase risk for incarceration.7,8 To reduce their psychiatric symptoms and risk of reincarceration, incarcerated individuals must receive access to evidence-based mental health practices.
Inside jails and prisons, psychotropic medications are the primary and sometimes only form of treatment;9–12 access to other evidence-based treatments are greatly reduced.13–16 At the same time, incarceration significantly elevates the risk for onset or progression of psychiatric symptoms.17,18 While some correctional mental health programs offer wrap-around services that include psychotherapy, research suggests that the cognitive behavior therapy (CBT) offered in these programs is “watered-down” to make space for other services, thereby reducing its efficacy. 19
A wide array of diversion courts have been established to both prevent incarceration of individuals with mental illness and provide supervised treatment and rehabilitation. Mental health courts represent one kind of diversion court, wherein defendants are assigned to a specialized docket with judicially supervised community-based care. A fundamental tenet of these courts is to promote access to evidence-based treatments. 20 There is some evidence to support the efficacy of mental health court outcomes;21,22 However, outcomes from the courts are idiosyncratic. 23 Limited data are available on how judges and their team make decisions on mandated treatments. This gap in the literature is especially concerning as it relates to access to evidence-based practices for PTSD given high rates of exposure to trauma and PTSD among incarcerated samples.24,25
Unfortunately, survivors of violence are more likely to become perpetrators of violence. For example, individuals with PTSD are more likely to perpetrate intimate partner violence than those without PTSD.26,27 Veterans with PTSD are also at higher risk for violent behavior in general, including physical fighting and threatening others with weapons.28,29 This is likely just one of many reasons why PTSD symptoms increase the risk of criminal justice involvement in general7,30 and involvement in more serious offenses. 31 In qualitative studies, incarcerated men and women report that maladaptive strategies for coping with trauma contributed to their incarceration, and that trauma exposure itself makes it more challenging to develop positive coping strategies to prevent incarceration.32,33 Between 15–48% of women and 27% of men incarcerated in prisons meet criteria for PTSD, reflecting a significantly elevated risk for PTSD compared to the general population (approximately 8%).24,25 Thus, the link between exposure to trauma, PTSD, and incarceration is well-established.
The clear association between PTSD and criminality is concerning because of the robust evidence-base supporting CBT for reducing symptoms of PTSD. Meta-analyses have revealed large effect sizes of CBT on PTSD and secondary conditions, like depression, anger, substance use disorders and suicidal ideation.34,35 Clinical Practice Guidelines suggest that CBT is a first-line treatment for PTSD.36,37 Nevertheless, there are challenges to the widespread dissemination and adoption of evidence-based practices in mental health settings in general 38 which may be exacerbated in incarcerated populations due to a need for adapting protocols. 39
Several states have mandated continuing education for judges each year and have invested large sums of money toward this endeavor. 40 Without an understanding of judges’ perceptions and knowledge about treatment for PTSD and comorbid conditions (including suicide risk), these funds may not address current knowledge gaps. This study first sought to examine mental health court judges’ attitudes toward therapeutic jurisprudence and awareness of gold-standard treatment recommendations for PTSD. In light of the larger literature on challenges with dissemination,41,42 we hypothesized that judges would report low awareness of evidence-based practices for PTSD. Second, given the increased risk for suicide among patients with PTSD, we explored judges’ perception of optimal strategies for the management of suicidal thoughts in mental health court. We hypothesized that judges would similarly report low awareness of evidence-based practices for assessing and mitigating suicide risk.
Methods
Participants
Participants (N = 11) were judges on mental health court recruited from 7 states across the United States. Demographic information was collected from ten of the eleven participants. Of the ten participants, 6 identified as women and 4 as men. Six of the participants were between the ages of 50 and 59, two were between the ages of 60 and 69, and two were above the age of 70. All had obtained a Juris Doctor degree (JD) and had no other post graduate degrees. One-third of participants had between 10 and 14 years of experience as a judge, and one-third had between 20 and 24 years of experience. Participants also varied in the number of hours spent on mental health court (MHC) with the majority spending between 5 and 10 h a week, three spending less than 5 h a week, and one spending more than 10 h a week on mental health court.
Interview
Standardized interview questions are reported in Appendix I. The interview followed a semi-structured format. It was developed by an interdisciplinary research team, including an expert on correctional mental health and ethics, a sociologist, and a clinical psychologist based on the available literature on mental health court. It was designed to study judges’ broader perspectives and goals regarding mental health court, along with their experiences and attitudes working with individuals with PTSD.
Interviewers
The interviewers included a doctoral level clinical psychologist with experience and training in conducting qualitative interviews and an advanced doctoral sociology graduate student with specialized expertize in qualitative research. Interviewers were trained to deliver the interview in a semi-structured manner and to ask follow-up questions to elicit more details about a topic as needed.
Coders
Coders included an advanced doctoral sociology graduate student and a highly-trained undergraduate research assistant. Coders were trained by the first and last author, who met regularly with the coders to ensure fidelity in coding and help resolve discrepancies as needed.
Procedure
This study was approved by the Institutional Review Board at the University of Pennsylvania, and participants completed informed consent prior to their interview and completion of demographic information. Judges were recruited purposively through two avenues. First, potential participants were contacted through professional networks at the University of Pennsylvania (n = 5, of which 2 participated in the study). Secondly, potential participants were identified using the SAMHSA Adult Mental Health Treatment Court Locator and contacted by email. The interviews were conducted either in-person or over the phone and were audio-recorded for transcription. Recordings were transcribed verbatim. The codebook was developed using a combined deductive and inductive approach with predetermined codes from the interview questions and additional codes to capture emergent themes that arose during the interviews. Transcripts were independently coded by two researchers using NVivo. The reviewers reviewed two transcripts, met for consensus coding and calibration, and resolved discrepancies through deliberation and consensus. The codebook was updated to reflect this process, and a third transcript was double coded to validate the revised codebook. The third transcript was reviewed by the research team using the same method, after which both researchers independently coded the remaining nine transcripts. Once all transcripts were double-coded, members of the research team reviewed them to resolve any discrepancies through deliberation and consensus. No new themes were identified in the last 3 interviews conducted, suggesting that we reached theme saturation. Upon completion of all coding, the first-author used second coding to review all 11 transcripts and codes to identify thematic and conceptual similarities across interviews and identify the primary theme of the interviews. 43
Results
The proportion of time dedicated to each code domain averaged across all participants is reflected in Figure 1, with a break-down by participant in Table 1. The most commonly discussed topics included discussion of the treatment team; mental health treatment options; court practices, procedures and case management; challenges and barriers to success in the court; goals of mental health court; rules upon admission; the judge role in the court; and the judges’ attitudes toward PTSD.
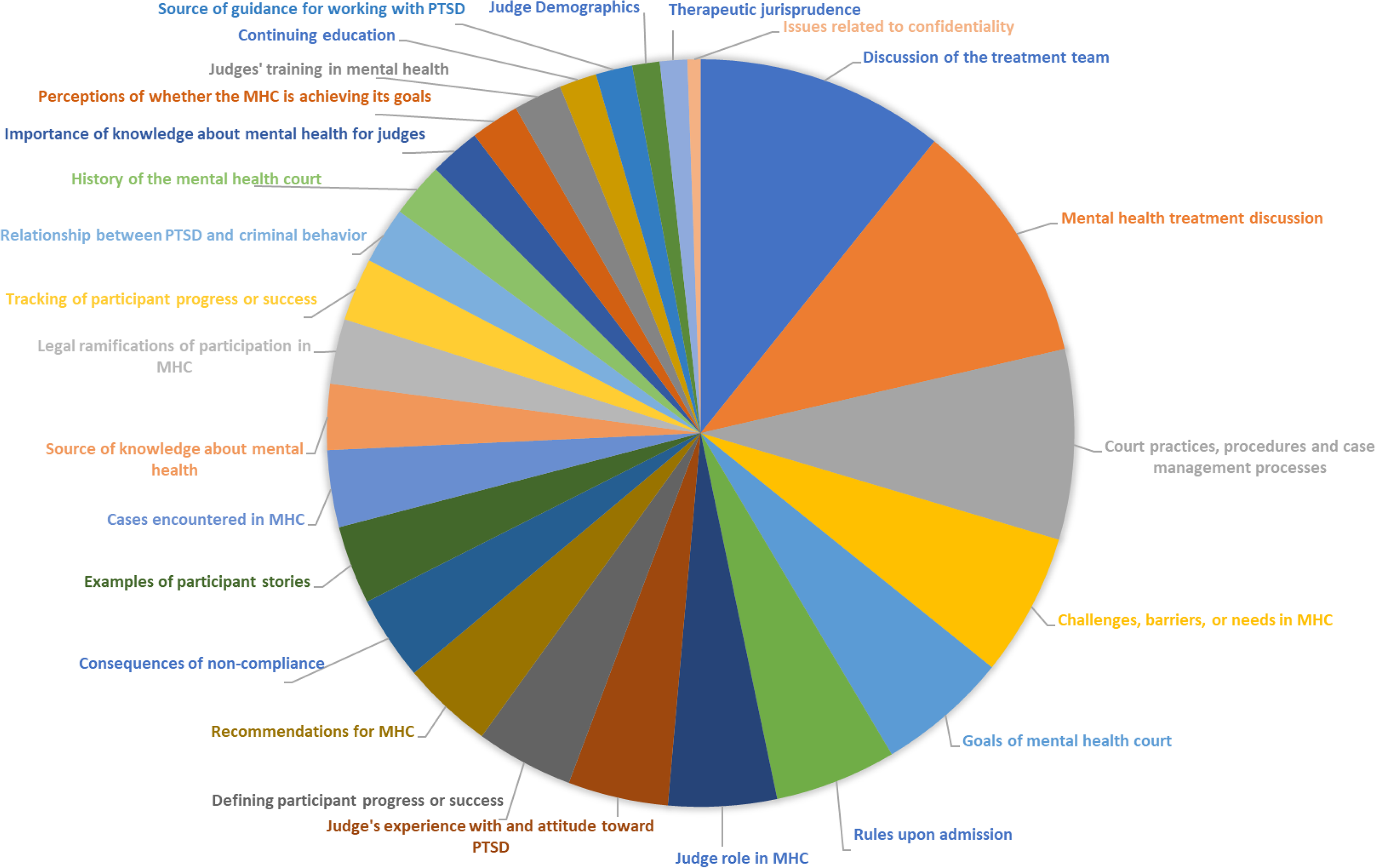
Average proportion of interview content across all mental health court (MHC) judges.
Proportion of interview content by participant (%).

Treatment team
Approximately 10% of interview content was dedicated to discussion of the treatment team. Examples include: We actually have an entire team that works together. What happens is someone identifies the defendant as having a mental health issues. That could be the police officer at the time of the arrest, it could be the defense attorney, it could be the prosecutor, it could be the court clerk, it could be anyone.
Another example referenced external members of the treatment team: There's a retraining of police to recognize mental illness, and not necessarily arrest somebody and send them to prison, but to bring them to the crisis center. And then the police are changing their function substantially. They’re recognizing mental illness.
Mental health treatment options
Approximately 10% of the interview content covered mental health treatment options. Many of the examples focused on adherence to medication and attending appointments. No judge mentioned reference to evidence-based practices without prompting. Examples include: We are looking for people meeting more of their treatment goals, so getting to more appointments, staying on their medicines more consistently, having more stable housing situations, getting arrested less times, drinking and drugging less, obtaining and maintaining employment, whether it's supported or not, part time or full time, and obviously reuniting people with their families when that's part of the issue.” Another example along this theme: “It's not just a matter of what the illnesses are and what medicines might be appropriate or successful for certain illnesses or what therapies, what therapeutic prescriptions could be employed. Therapy, yoga, acupuncture, anything that might be a possible avenue for giving someone relief from their symptoms to help them be able to function better…I need to understand enough about it to know the reason why someone might not be complying with the court order. It may be directly related to their mental illness.
When explicitly assessed about knowledge of evidence-based PTSD treatments, six judges reported having no knowledge about this, and one reported that their court does not provide services for PTSD. In the remaining 5 judges, self-reported knowledge about PTSD treatment varied. As an example: In terms of the different therapies, I don't know that I can speak to that specifically. I know that anybody that we would have that is dealing with PTSD obviously, we would make sure if they haven't already been, that they would get linked with the appropriate mental health care provider.
Three judges mentioned a particular type of therapy, eye movement desensitization and reprocessing (EMDR), which is not a first-line PTSD treatment: They say to this person [in eye movement desensitization and reprocessing], “I want you with your eyes to follow my finger, because I go back and forth like this. And then as you’re doing this, I want you to think about the crises that you went through, all right?” And it has something to do with communicating with both sides of the brain, of being on both sides of the brain. What in the hell is that?
Also on the topic of EMDR, another said: We see a lot of PTSD for sure, and we try to be mindful that most people probably have that. There's really no medication for PTSD, but there is therapy for PTSD. I’m actually very familiar with trauma therapy, EMDR, and we do have people who have done that in our program who use those kinds of modalities. I kind of stay on top of that, but I have a family member who has PTSD, so I’m very familiar with the models of therapy.
One judge mentioned Moral Reconation Therapy (MRT). While MRT has evidence for reducing recidivism, it is not an evidence-based practice for PTSD. See if you take the definition of PTSD and think about it, I mean, most men will not admit to sexual and physical abuse and the percentage, no one knows how high it is, but there's so many people in our system now who have been traumatized again and again and again. In my view if you aren't using PTSD techniques and like with my parolees, I send them to MRT, moral recognition [sic] therapy. They don't like it, they rebel, they argue, because they’re so traumatized that it's so hard to bring them back. It's so hard, but that's all PTSD treatment.
One judge expressed skepticism about the concept of evidence-based treatments in general: And when they say evidence based, I’m not sure what that actually means. Because actually, you’re talking about statistics, and really anecdotal information when you’re talking about mental health. It's not like oh, we can test this person's blood, and find out if maybe this is what he needs. They do that, they do med checks to make sure that the levels of the medicine are the right thing… no matter how good the evidence based data is, it's still dealing with mental illness is still radically unpredictable, even with the medicine.
This same judge replied in the affirmative when asked specifically about knowledge on PE or CPT, saying the following: Yeah, we have that [evidence based practices for PTSD]. So the therapies that they use in mental health court are something called dialectical behavioral therapy.
Of note, two other judges spontaneously mentioned Dialectical Behavior Therapy in reference to treatment options for PTSD despite the fact that dialectical behavior therapy (DBT) is not an approved therapy for PTSD treatment. Yet another judge responded affirmatively when asked about knowledge of evidence-based treatments in the following manner: Everything that I’ve heard about cognitive therapy is that it's one of the most effective ways to actually help people get better. I have another thought. The other thought is that it's my understanding that that is lots of time, and lots of money. That's something we don't have here at all. That's behavior change. What I have read about that is it's very successful, but you have to have someone who can provide that service, and you have to have the money to pay for it.
Court practices, procedures and case management
Approximately 7.5% of all interview content discussed issues related to court practices, procedures, and case management. Examples include: “Our theory is we’re using the teeth of the court to force them to get the treatment that they need.” An example from another judge: There's usually an effort to reengage and to bring people into compliance. That can take many forms, it can be just through their case manager going out and trying to find them, it can be a courtroom discussion, it could be a number of persuasive techniques. If none of those things work and a person fails to appear in court then we have to issue a warrant.
Challenges and barriers to success in the court
Approximately 6% of interview content referred to challenges and barriers to success. Every judge mentioned a lack of resources as a barrier to the success of court, especially lack of stable housing and transportation options. Examples include: The nature of our docket makes it very difficult to study outcomes. I would say that we feel a sense of success in that we are taking the time to try to do something different then what would happen in a case where an individual did not have a mental health disorder and we all see successes. We also struggle with failure, I would say part of the failure is lack of resources and part of the failure is that we do not have an ability to force treatment. For many people, without treatment they have a very difficult time maintaining behavior.
Along those lines, another judge mentioned studying outcomes as a challenge: Part of our dysfunction as a court is that we don't have any recidivism data.” An example from another judge includes: “Having lost that (trauma-focused) grant I can tell you has been a tremendous negative event for us, tremendous negative. We were so much more effective when we had the benefit of this (trauma-focused) counselor.
Goals of mental health court
Approximately 5% of interview content referred to goals of the mental health court. Examples included: That comes back to we are a criminal justice system, and we have an obligation to the community. We will offer this to you, and we would like to work with you on this, and we will do everything we can to pull together every community resource we have, but if you’re not going to show up, I cannot keep you in this program because our obligation is beyond just that. It's not a clinical therapeutic relationship, it's a criminal justice relationship.
Another judge provided an example:
So we as a community really wanted to have a mental health court that would promote human rights and essentially do no harm. So that also, if you will, gets into the therapeutic jurisprudence framework. We consider the court to be a human rights strategy.
Rules upon admission
Approximately 5% of interview content discussed rules upon admission. Examples include: They have to voluntarily agree to participate with us. We are very clear with them about what the program requirements are, what the expectations are, they go through agreements with us indicating that they understand those things and they’re willing to participate in it, and if they don't, that's fine, but I guess everybody kind of comes into it eyes open, eyes wide open about what they’re agreeing to do. It's a minimum of 18 months, we do make sure that they understand that in addition to navigating and maintaining connectivity with their treatment providers, whatever may be appropriate for that, if there's gonna be obligations to come to court, and if that's gonna be on a more frequent basis than probably a traditional probation would be.
All of the judges described consequences for not following the rules. As one example: If they don't show up for their group meetings or their therapy sessions, or their doctors appointments, that is brought to my attention when mental health court meets.
The judge role in the court
Approximately 4% of interview content covered the role of the judge. Key themes included taking on a role of a coach or parental figure. Examples include: I become that father figure. They don't want to displease me and I see them every Thursday morning. The ones that, we wean them as they get better and adapting and looking like they’re more successful in the program and they have jobs and they’re doing what they’re supposed to be doing.
Another judge noted: What I find that my role is, week after week, is mostly being something like a parent. Being both a cheerleader and the boundary setter and an enforcer of rules.
Along those lines, another added: A lot of them, it's amazing, a lot of them never had anybody in their life recognize achievements that they’ve made. A lot of them have too much in the way of achievement. But here's a judge, here are the lawyers, here's the service providers, they’re all clapping for you, because you’ve done something really great. And that works very nicely, in a lot of cases. So it's a great thing to watch unfold.
Still another noted: I sign off on the participant's treatment plan, but because I am not a doctor or a psychologist or a therapist of any sort, I feel like I have to stay away from pretending that I am one. But I would like to know more and be better educated, so I think that that would be useful to me.
Another judge also cited the importance of mental health knowledge for making informed decisions in the court. I don't know how you could do mental health court without having some understanding of the diagnosis and the treatment. You have to make an informed decision as to what the court order is going to say or what the treatment plan ultimately…is.
Yet another explained how mental health knowledge allows them to identify when mental illness interferes with a participant's ability to comply with court orders. I need to understand enough…to know the reason why someone might not be complying with the court order. It may be directly related to their mental illness. While they may not be deliberately trying to violate the order, they may be sick enough that it's hard for them to comply. I just think I need to understand that. Not as a doctor, not as a practitioner, but I need to understand that there might be more than one thing happening.
Judges’ attitudes toward PTSD
Approximately 4% of interview content covered judges’ attitudes toward PTSD. All judges were mindful of the trauma experienced by court participants, with all but two reporting that PTSD was common among mental health court participants. One judge also noted that incarceration itself is traumatic. Another judge connected trauma to marginalization, which often brought participants into the system. Examples include: For some reason, I don't have that information about the people in my mental health court. But my general belief is that probably a very large number of them are suffering from PTSD, or have serious trauma or traumas in their history.
Another judge noted: A very high number of individuals in the criminal justice system have trauma. If they haven't been traumatized before they were incarcerated, it's certainly a traumatic event to be incarcerated. We see a lot of individuals who have very high ACE [adverse childhood event] scores for example. We try to be mindful of it and treat everyone as if they have been traumatized because most people have been.
And another commented: I think a significant number of the people that do come before the court have experienced traumas that are going to impact their ability to be successful. If you’re in a criminal justice system, the chances are pretty darn good that you’ve been victimized, and actually pretty darn good that you’ve been doing some of the victimization…It's part of what happens when you are living in the margins, and you’re not getting the things you need to survive in a healthy way.
On the other hand, one judge avoided discussion of trauma because of a perception that there was no way to know if a participant in the court had been traumatized. The same judge also said they did not categorize PTSD as a serious mental illness and that individuals seen in their court rarely have PTSD as a standalone diagnosis. Another judge also said that PTSD takes a “backseat” to serious mental illness in their court. We’re kind of warned in a way not to talk to them about that [abuse], and I don't bring it up. But I know that it happens. I think they carry it with them all their life…And it's like in general, how do you know these things really happen or not? They’re not going to tell you about it.
And another: It usually comes in a package of things. It's never standalone PTSD. There's always PTSD, and schizophrenia, or bipolar illness, right?
And another: When a person has a severe mental illness, the PTSD takes a bit of a back seat. When a person doesn't have a serious mental health disorder but only has PTSD usually they’re higher functioning…and might be appropriate for a different type of docket than the mental health docket.
Suicide prevention
When asked about best practices for reducing suicide risk in incarcerated populations, all judges agreed on the importance of suicide risk assessments. Four judges mentioned jails as the point for assessment. Well number one, the jails need to have appropriate facilities and areas that deal with the mentally ill. They need to have a screening process when people are brought into the jails, ensuring that they’re not missing, and they also may be suicidal. And I don't know that all jails are equipped, or have mental health units, separate units that deal with individuals with mental illness. So I think, because they’re not identified in screening, and often missed, the fact that somebody's suicidal.
Two judges indicated they assess for suicide risk during court proceedings. They say, and the people in mental health court do this too, that you should always ask someone the question, “Are you thinking of taking your life?” And you’ll always get an honest answer. I didn't believe that at first, but the VA convinced me. If somebody's thinking of taking their life, they want someone to stop them. They want a way out. They want help. They’re not really seeking oblivion.
Another example: What they’re doing is they’re trying to get relief from their problems. So they will tell you if they’re going to take their life. And you’ll get an honest answer. I’m not sure that happens in every case, but yeah. So that's their protocol, and when people come to the service providers in mental health court, and with the VA, and [de-identified health center], I always ask them that question. So they kind of get used to being asked. And they don't regard it as an insult, and it shouldn't be regarded that way.
Discussion
All of the judges interviewed in this study reported that PTSD is highly prevalent among their participants. Despite this, judges also reported not having received formal education about evidence-based practices for PTSD or other psychiatric diagnoses. They largely reported relying on their team members to provide recommendations for treatment planning and viewed their role as the enforcer of the treatment teams’ suggestions. This reliance on other team members necessitates appropriate training of the mental health teams in evidence-based practices as well as in thorough assessment and communication of their findings to the court. Over half of the judges reported little to no knowledge of evidence-based treatments for PTSD. The remaining judges mentioned treatments that are not evidence-based or first-line treatment options for PTSD, including dialectical behavior therapy, eye-movement desensitization and reprocessing, or MRT. Finally, judges also reported that suicide prevention is an important consideration and that there is a need for universal suicide risk assessments.
These findings are consistent with epidemiological studies in which 48% percent of incarcerated individuals meet criteria for PTSD. 44 There are likely a number of contributing factors to high rates of PTSD among the incarcerated population, including that PTSD increases risk for being arrested, 45 that being incarcerated increases risk for subsequent trauma exposure, 44 and that PTSD is associated with higher rates of recidivism. 46 The high prevalence rates of PTSD among participants in mental health court necessitates a focus on dissemination of evidence-based practices for PTSD.
A number of evidence-based practices for PTSD exist, including prolonged exposure therapy (PE) and cognitive processing therapy (CPT), among others. 34 Access to evidence-based practices for PTSD remains a challenge across most healthcare systems, including in the VA 47 and in community mental health. 48 Thus, it is not surprising that mental health courts similarly have challenges in the dissemination of evidence-based practices for PTSD. Unlike in other settings, mental health court plays a role in mandating receipt of treatment. If a treatment is mandated to an individual, at a minimum, that mandated treatment should be evidence-based.
In this study, judges’ self-reported knowledge about existing evidence-based practices for PTSD was low. Some judges mentioned having heard about EMDR and MRT. As mentioned above, MRT is not an empirically supported treatment for PTSD (Department of Defense, 49 ). While EMDR has empirical support for PTSD, PE and CPT each have a significantly larger body of evidence to support their efficacy (Department of Defense, 49 ). Dialectical behavior therapy is an evidence-based practice for borderline personality disorder, not PTSD. 50 For judges to recommend gold-standard therapies for PTSD, they first have to be aware that those therapies exist and that there are differences between PTSD therapies, in terms of efficacy, effectiveness, and impact on secondary conditions ( 34 e.g. suicidal ideation, depression, substance use disorders, etc. 51 ).
Judges also reported limited formal training in any topic related to mental health. Many cited personal or family experiences with mental health as the source of their knowledge. There was variability in interviewees’ desire for additional mental health training, with some judges expressing enthusiasm for continuing education and others reporting that it was unnecessary. Judges reported that they relied on their in-house mental health team members to make recommendations about treatment planning. None of the judges explicitly mentioned relying on expert witnesses outside of their established team as needed, which was somewhat surprising given the common use of expert witnesses in court proceedings. This is an area that would benefit from greater exploration in future studies. For those judges who indicated that additional training was not necessary, a common theme was reliance on team members (i.e. social workers or contracted behavioral health providers) for providing recommendations about treatment planning. Reliance on team members for recommendation is appropriate and consistent with team-based care. 52 However, the power afforded to mental health court judges may necessitate additional training to ensure that recent advances in evidence-based practices are considered when issuing treatment mandates or penalties.
PTSD is associated with a number of deleterious psychological and physical conditions, including risk for suicide. 53 In light of this, it was valuable to learn that judges agreed about the importance of universal suicide risk assessment. Jails and prisons should follow guidelines in their implementation of universal suicide risk assessments. 54 However, a robust body of literature demonstrates inconsistent assessments, even among jails that have a very regimented intake assessment.55,56 Some judges noted the importance of suicide risk assessment as part of the court proceedings. It might be important to formalize suicide risk assessment in the mental health court intake process. This would ensure that participants are assessed for suicide risk at the time of entry to jail, which is a very high-risk time for suicide, 57 and then reassessed upon inclusion in the mental health court program. An individual's suicide risk may fluctuate dramatically over time. 58 Therefore, repeated assessments of suicidal thoughts and behaviors are extremely important among individuals involved with the criminal justice system.
Several important limitations of these study require consideration. First, we recruited a small sample of participants due to the limited number of mental health courts and challenges in recruitment. However, 9–17 interviews is typically sufficient for qualitative work 59 and our last 3 interviews did not reveal any new themes, suggestive of reaching a point of saturation with 11 interviews. Thus, this study represents an initial snapshot that captures the views of a small cohort of judges pertaining to mental illness, PTSD, and their own expertize. More research involving mental health court judges is required before system reforms are identified and implemented. Second, judges reported some heterogeneity across their courts in terms of the court team members, partnerships with community members, and collection of standardized outcome data. Nonetheless, despite heterogeneity across courts, several consistent themes emerged. Third, many courts had other diversion programs for special populations, such as veterans court, drug treatment court, and other court settings where mental health conditions are highly prevalent. We only recruited judges from mental health courts, but important insights could be gained from other diversion programs in the future.
There are a number of important clinical implications of these findings. These findings highlight the essential role that mental health providers can play in disseminating information about evidence-based practices for PTSD among mental health court judges in their local communities. There may be a need to formalize continuing education focused on evidence-based practices for judges in mental health court. This continuing education should ideally focus on topics including and beyond PTSD, namely mood disorders, psychotic disorders, and substance use disorders. Given the robust guidelines for recommendations on evidence-based practices for PTSD, there are strong justifications for focusing on disseminating these practices to mental health court participants. In addition to providing education to judges who oversee mental health court, it is also extremely important to provide training and support in evidence-based practices to the behavioral health providers who are tasked with providing services to the court's participants, an area for future research.
In summary, we found that judges report exposure to trauma and PTSD are significant stressors among participants in mental health court, yet judges are unfamiliar with evidence-based treatments for PTSD. It is essential to ensure that mental health court participants have access to not only knowledge about evidence-based practices in general, but especially for PTSD where treatment recommendations are robust and plentiful. Judges agreed about the importance of universal suicide risk assessment, which is significant in light of the role that PTSD can play in increasing suicide risk. These findings offer insights into opportunities for collaboration between mental health experts and mental health court judges to improve treatment planning for participants in the court.
Supplemental Material
sj-docx-1-msl-10.1177_00258024221096250 - Supplemental material for Knowledge of evidence-based practices for PTSD among mental health court judges
Supplemental material, sj-docx-1-msl-10.1177_00258024221096250 for Knowledge of evidence-based practices for PTSD among mental health court judges by Lily A. Brown, Reem AlRabiah, Melanie Terasse, Valeryia Aksianiuk and Dominic Sisti in Medicine, Science and the Law
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Quattrone Foundation,
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.