
Abstract
Carbon monoxide (CO) is an odourless and tasteless gas which can be produced by the incomplete combustion of carbon-containing fuels. Compared to vehicular CO suicides, unintentional cases (excluding those related to fires) are much less common. Increased education surrounding the risks associated with the accumulation of CO in enclosed spaces has contributed to a reduced incidence of unintentional CO poisonings. However, such cases may remain undetected, particularly in domestic and recreational settings where scene findings are often non-specific. The current study of unintentional CO poisonings in South Australia and the Northern Territory, each with a unique climate (Mediterranean and tropical respectively), demonstrated differences in the circumstances of death. Several cases where individuals used carbon-producing fuel sources for heat, both in domestic and vehicular settings and without adequate ventilation, resulted in fatal outcomes. Less common scenarios involved faults in equipment (e.g. a hot water heater), vehicle faults resulting in the accumulation of fatal levels of CO in enclosed spaces, and inadvertent introduction of CO into a diving oxygen supply in a recreational aquatic setting. In ascertaining the cause of death, other considerations include the potential role of underlying chronic cardiovascular and respiratory disease and age which may increase an individual's susceptibility to CO toxicity. Understanding the wide variety of presentations and contributing factors in cases of fatal CO poisoning including consideration of climate-specific differences in domestic and extra-domestic settings may enable improved detection at autopsy.
Introduction
Carbon monoxide (CO) is a colourless, odourless, tasteless gas present in the atmosphere in minute concentrations that may be produced in larger amounts by the incomplete combustion of carbon-containing fuels.1,2 While vehicle-related CO poisoning is a very common method of suicide in certain communities (where exhaust is deliberately diverted into the interior of a vehicle cabin), 3 accidental cases are far less common.4,5 The majority of unintentional CO poisonings are preventable with appropriate education and implementation of protective measures. 6 However, unintentional fatal CO poisonings, particularly those associated with recreational activities or those that occur in domestic settings, are often not as easily detected due to non-specific scene findings. A case study was undertaken to analyse features of fatal unintentional CO poisonings (excluding those related to fires) in two Australian jurisdictions (South Australia (SA) and the Northern Territory (NT)) over a 20-year period.
Materials and methods
Cases of accidental CO poisoning occurring in SA between 1 January 2000 and 31 December 2019 were identified from pathology records held at Forensic Science SA (FSSA). Cases involving accidental exposure to CO from domestic, industrial or bush fires were excluded. The Toxicology Database at FSSA was searched for all post-mortem CO detections over the same time period. Cases with CO detected in post-mortem samples were then cross-referenced against autopsy reports to identify deaths due to accidental CO poisoning.
Cases of accidental CO poisoning in the NT between 1 January 2000 and 31 December 2021 were identified from the Royal Darwin Hospital (RDH) Forensic Pathology Unit database and records.
Additional information was retrieved from coronial autopsy reports including age, sex, cause of death, location of death, medical histories, scene findings, autopsy and toxicology findings, and manner of death.
Seasons in SA are summer (December–February), autumn (March–May), winter (June–August) and spring (September–November). Seasons in the NT are the wet (November–April) and dry (May–October) where temperatures range between 20°C to 33°C with corresponding variations in humidity and rainfall. 7
Age (in years) was categorised as the following: infant (<1 year), toddler (1–3 years), child (4–14 years), young person (15–24 years), adult (25–64 years) and elderly person (65 years and older).
Statistical analyses were performed using R (version 4.2.2). 8
Ethics approval for the SA data used in this study was granted by the University of Adelaide Human Research Ethics Committee (H-2020-033) and the Forensic Science SA Management Group. Permission to include NT data was granted by the NT coroner's office.
Results
Across both jurisdictions, a total of 10 fatal unintentional CO poisonings were identified. In SA, there were seven cases between 2000 and 2019 and three cases in the NT between 2000 and 2021 (Table 1). This constituted 1.4% of all CO-related deaths in SA (7 out of 502) and 8.8% of all CO-related deaths in the NT over the same time period (3 out of 34 deaths). There were no significant trends in incidence across the time period most likely due to the small number of cases.
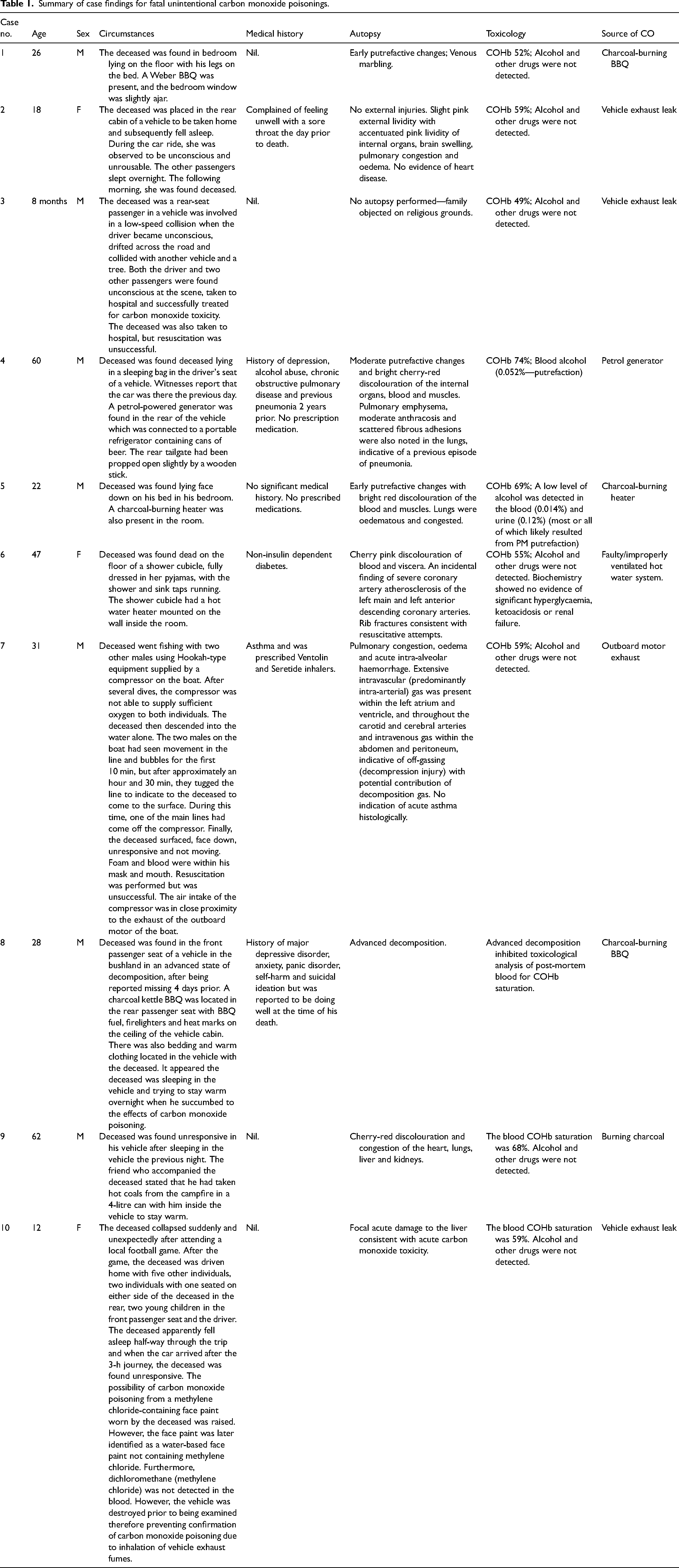
Summary of case findings for fatal unintentional carbon monoxide poisonings.
Demographics
The 10 decedents included six adults, two young persons, one child and one infant. The age range of decedents was 8 months to 62 years (mean 31 years). There were three females (age range 12–47 years, mean 26) and seven males (age range 0.6–62 years, mean 33).
Seasonality
In SA, two cases occurred during summer, four during winter and one during autumn. In the NT, all of the cases occurred during the dry season.
For the five SA cases in the cooler seasons (i.e. autumn and winter), two were associated with the use of alternative fuels for heating, two with car travel and one involved a fuel generator used to supply a refrigerator located within a vehicle. The two remaining cases in the warmer seasons (i.e. summer and spring) were associated with a water heater system fault in one case and a fault during scuba diving in the other.
Two of the NT cases were associated with the use of alternative fuels for heating, and the remaining case was related to a vehicle fault during travel. While the average temperatures in the NT are consistently warmer compared to SA, the two decedents using carbon-containing fuels as a heat source were located in areas where the average overnight temperature was 3°C. Both decedents had used alternative fuel sources for heating in a vehicle overnight.
Autopsy findings
A full autopsy was performed for nine of the 10 cases. In one case, the family of the deceased objected to autopsy on religious grounds (Case 3). Furthermore, one additional case was markedly decomposed which obscured characteristic autopsy findings of CO poisoning and interfered with toxicological analysis of a post-mortem blood sample (Case 8). For the remaining eight cases, autopsies showed characteristic signs of CO poisoning including cherry-red lividity of the skin and internal organs, and pulmonary oedema and congestion. Some additional circumstance-specific findings were noted, particularly for the case involving CO poisoning with subsequent drowning (Case 7).
Evidence of comorbid conditions associated with reduced respiratory or circulatory function were noted in the medical history of two decedents. One decedent demonstrated severe coronary artery atherosclerosis, and the other had a history of emphysema with recent pneumonia. One additional decedent had a medical history of asthma; however, no evidence of acute asthma was observed at autopsy. There was no significant difference in the carboxyhaemoglobin (COHb) levels between decedents with pre-existing cardiovascular or respiratory disease and those without.
Toxicology
The average blood COHb saturation was 57% (range 49–74%). Alcohol and common drugs were not detected in any of the cases, with the exception of two cases which both demonstrated putrefactive changes and an associated low blood alcohol level which were attributed to post-mortem bacterial generation.
Source of carbon monoxide
The source of CO was most often vehicle or generator exhaust (n = 5), most frequently related to a vehicle exhaust leak (n = 3). One of these cases occurred in a moving vehicle where the remaining passengers only experienced mild CO poisoning symptoms. Four additional cases were associated with burning charcoal in an enclosed space without adequate ventilation. While it appears that efforts were made to maintain adequate ventilation in two cases by propping open a window, this was not sufficient to provide adequate ventilation. The remaining case was attributed to a faulty and improperly ventilated hot water system.
Discussion
Unintentional cases of fatal CO poisoning are not frequently encountered in forensic practice.4,5 If CO poisoning associated with fires is excluded, the most common unintentional causes of CO poisoning are associated with leaking heating appliances and inhalation of vehicle exhaust due to faulty exhaust systems. 4 For unintentional vehicle-related CO poisonings, potential sources of CO include exhaust pipe defects or faults, inadequate ventilation and exhaust system obstructions causing CO to accumulate within the cabin of a vehicle. 4 Unattended vehicles idling within an enclosed space such as a garage or shed, may also cause CO levels to increase to fatal levels. 9 Rare cases of CO inhalation have also occurred in open spaces. 10 It is important to note that CO emissions in vehicles fitted with a catalytic converter may still exceed the toxic/lethal limit when the vehicle is idling from a cold start with a short time delay before the catalytic converter begins to operate efficiently, or in older vehicles.9,11 It has long been accepted that COHb concentrations in excess of 60% are considered fatal, 12 with severe poisoning occurring at concentrations greater than 30%. 13
While vehicles are the most well-documented setting for CO poisoning, there are also examples of fatal unintentional CO poisoning occurring in domestic settings, where the source of CO may be burning charcoal, faulty gas heating systems and petrol-generators or cooking appliances that are being operated without adequate ventilation.1,14,15 The discovery of multiple bodies in an apartment or house with no evidence of scene disturbance or violence must raise the possibility of CO toxicity. Similarly, this should be considered when two infants are found dead in a cot at the same time rather than automatically assuming that their deaths were due to coincident sudden infant death syndrome.
Installation of CO alarms has been shown to be highly effective in decreasing fatal accidental domestic CO exposures, reducing the number of deaths by approximately half.16,17 There were three examples of CO poisoning in a domestic setting in the current study, where burning of charcoal (n = 2) and a faulty gas heating system (n = 1) allowed CO levels to accumulate to fatal levels within rooms. Alternative heat sources such as charcoal or petrol-generators in extra-domestic settings such as inside a vehicle have also been associated with lethal CO exposure. These occur more frequently in winter, where alternative heating sources are used for warmth.5,17–19 Three of the reported cases had used alternative heat sources in stationary vehicles for heating. There was also one additional case where burning charcoal was used for heating in a bedroom.
CO poisoning may also occur in recreational aquatic settings such as scuba diving. One case within the current study, although not associated with faults in diving equipment, occurred due to the close proximity of the boat exhaust to the intake valve of the oxygen supply. There have also been concerns raised more recently about CO accumulation at the rear of houseboats due to uncontrolled generator combustion, 20 with individuals swimming within the vicinity of the deck at increased risk of CO poisoning and death. 21 While there were no cases which demonstrated this particular scenario, it is important to emphasise the risks associated with being in close proximity to engine exhaust. It is, for example, well recognised that accidental deaths due to CO inhalation are a feature of the fishing industry where engines operate in confined spaces below decks. 22 Methylene chloride is an additional, although rare, source of CO which is a common component of paint remover and other solvents. 1
Cherry-red post-mortem lividity is the most common autopsy finding in fatal cases of CO poisoning. 23 However, there exists a small proportion of cases where this may not be found. This may be due to lower than usual levels of CO causing death in an individual who has concomitant conditions such as ischaemic heart disease or anaemia. In these cases, death is due to a negative interaction between the underlying diseases and the toxin, so-called negative disease-drug/toxin synergy. 24 Alternatively, storage of bodies in refrigerated environments may result in artefactual pink skin discoloration due to post-mortem reoxygenation of haemoglobin. 25
Other reported non-specific post-mortem findings associated with CO poisoning include anoxic brain injury, focal pulmonary oedema, passive congestion of internal organs and liquid blood both in the blood vessels and heart chambers.4,10 Cases with survival may show characteristic lesions in the brain, with the basal ganglia, white matter, globus pallidus, and cortex most commonly affected.26,27 Cases may also be overlooked, particularly when the death scene does not indicate that there may be CO exposure, or where there are no obvious post-mortem signs of CO toxicity at autopsy.
There are various demographic and physiological risk factors associated with an increased susceptibility to CO poisoning. Older persons, males, children, pregnant women, individuals with genetic disorders (e.g. haemoglobin abnormalities) and those with a pre-existing disease that compromises cardiac or respiratory function which may impair tissue oxygenation are considered to be at increased risk.5,9,14,18,28–31 While there were three cases identified within the current study with pre-existing respiratory and cardiovascular disease, their post-mortem CO levels were not significantly different to those without pre-existing disease. It is however noted that the lowest detected CO level (49%) was in Case 3, where the decedent was only 8 months of age; three other adult passengers in the vehicle were rendered unconscious but survived the incident. There was also an additional case which demonstrated the same scenario, where fatal CO poisoning occurred in a child in a moving vehicle, with several other adult passengers only experiencing mild, non-fatal CO poisoning symptoms (e.g. headache, dizziness and loss of consciousness). These two reported cases highlight the increased susceptibility of children to the effects of CO poisoning compared to adults.
This study also highlights the difficulty in ascertaining manner of death, particularly when trying to determine whether a CO poisoning was accidental or deliberate. This is often confounded by the presence of a recorded history of psychiatric or neurological issues which may complicate determination of intent.
The cases described within the current study highlight a need to appreciate the importance of adequate ventilation when using CO-producing fuel sources or appliances in enclosed spaces. Even though efforts were made to increase ventilation in some cases by propping windows open, this may not be sufficient to prevent the accumulation of fatal levels of gas. There is a significant responsibility for the forensic pathologist to identify cases, as failure to investigate a source of environmental CO leakage or dangerous practices may put further individuals at risk. 15
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.