
Abstract
Introduction
The Coronavirus Disease 2019 (COVID-19) pandemic caused enormous challenges in every aspect of society. To slow down the spread of the virus, governments worldwide applied a wide variety of restrictions such as stay-at-home policies, travel bans and closure of places of entertainment, which reshaped daily social interactions and economic activities. 1 Restricted movement in time and space potentially contributed to a decline in public order crimes and certain property crimes including robbery, theft and burglary. 1 Conversely, these containment policies heightened levels of strain, forced cohabitation and limited avenues to seek support, with implications for child maltreatment, intimate partner violence (IPV) and elder abuse.2,3 Financial stress, job insecurities and substance abuse all intensified interpersonal violence. Research conducted in 2020 in Australia surveyed 15,000 women on their experience of domestic violence. One in three reported experiencing IPV for the first time and 53.1% of women who were abused previously noted an escalation in frequency in 2020. 4 Internationally, the rate of domestic violence tripled in China through the pandemic and there was a 30% increase in France, and a 40–50% increase in Brazil. 5 Many complainants of interpersonal violence are referred to clinical forensic medicine specialists for a forensic medical examination (FME) and documentation. The examinations are undertaken in a variety of hospital and community-based settings. During the pandemic, the delivery of clinical forensic medical assessments became challenging as COVID-19 precautions impacted on face-to-face contact and the availability of services, and altered the quality, quantity and scope of forensic activities. Diversion of police and hospital workforces and a fall in referrals also increased the difficulties in seeking assistance for complainants. 6
The speciality of forensic psychiatry that offers mental health evaluations in secure settings, faced similar challenges. Reductions in the inter-hospital flow of medical professionals and the number of available staff further hindered access to forensic psychiatric assessment. 7 While telemedicine has been incorporated into forensic psychiatric evaluations, the loss of subtle facial cues and body language may weaken the reliability of virtual evaluation. 8 Clinical forensic medicine and forensic psychiatry as frontline forensic health services have seen several changes to patient demographics and case trends over time. These services have had to undergo many pivots and adaptations during the pandemic in response to the changing needs of the patients, and the risks and challenges brought about by the pandemic.
Pandemic-related changes in clinical forensic medicine and forensic psychiatry emerged in February 2020 and are still evolving. To date, studies have been published to report crime trends, changes in FME volume and impacts of telemedicine. There has not, however been an analysis of the spectrum of changes to forensic practices in the living, to enable the identification of the challenges, successes and persistence of any modifications to practice. It is crucial to recognise and understand these changes as seen through both patient and clinician lenses to identify strategies for improvement.
The COVID-19 pandemic brought many challenges that impacted on the practice of clinical forensic medicine and forensic psychiatry. This included the need to: rapidly adjust guidelines to meet the evolving demands of public health measures; embrace appropriate technology; and enhance both clinical and legal considerations to encompass the modifications that would enable staff to continue to provide frontline services. An understanding of the changes that occurred in clinical forensic medicine and forensic psychiatry is key to learning from the lessons of the past three years and adopting sustainable positive strategies for the future. An evaluation of the impacts of the changes in the post-COVID-19 era will help to build on the resilience demonstrated during the pandemic, so that clinical forensic medicine and forensic psychiatry can continue to pivot and adapt to meet expected and unanticipated demands on practice. Therefore, the objectives of this narrative review are to explore what changes were made by clinical forensic medicine and forensic psychiatric services in different jurisdictions in response to the pandemic and seek an understanding of the processes, settings and the outcomes that occurred to inform future directions.
Methodology
Search strategy
A narrative review with a systematic approach was undertaken. A preliminary search on MEDLINE was performed to look for keywords contained within the titles and abstracts and index terms used to describe the studies. Key words searched were ‘forensic medicine’ OR ‘forensic science’ OR ‘forensic psychiatry’ AND ‘coronavirus’ or ‘COVID’ OR ‘Sars-CoV-2’ OR ‘lockdown’ AND ‘impact’ OR ‘adjustment’ OR ‘change’ OR ‘domestic violence’ OR ‘partner violence’ OR ‘child abuse’ OR ‘physical abuse’ OR ‘bullying’ OR ‘assault’. A second extensive search was conducted across Ovid Medline, Ovid Embase, Ovid Emcare and PubMed, and webpages of governments and other organisations. Forward and backward citation tracking of included studies was conducted to identify any additional eligible studies in the reference lists.
Eligibility criteria
This review considered studies published from January 2020 to current (March 2023), limited to those published in English. To be included in this review, studies must have assessed at least one of the main outcomes demonstrating any change that occurred in clinical forensic medicine or forensic psychiatry at the time of the COVID-19 pandemic. This included but was not limited to changes in the settings of assessment; changes in the examination/procedure performed, incorporation of COVID-19 preventative measures; impacts of these changes; and suggested strategies to improve the practice. Due to the relatively short time period that was being studied, the search was expanded to grey literature including government reports, policy statements and conference abstracts to more thoroughly explore any emerging changes.
Study selection
One researcher screened the title and abstract for inclusion against the predetermined eligibility criteria. The full texts of these studies were assessed by the same researcher. Any issues were resolved through discussion with two senior researchers. The results of the search were summarised in a narrative description accompanied by the PRISMA flow chart.
Data extraction
An electronic data collection form on Excel was utilised to inform the data collection process. The data collection process was performed by one researcher. The table was refined and revised during the data extraction process. The key variables collected from each study that were included in the finalised data sheet were: author; name of publication; year of publication; country; study aim; changes and outcomes of these changes; likely persistent changes; and suggested strategies to improve the practice.
Data synthesis
The extracted data was summarised and descriptively mapped to the objectives. Study characteristics such as publication details, study design and participant details were summarised narratively. Quantitative data including case trends, and changes in quantity of practice, were reported mainly in narrative and tabular forms.
Results
A total of 763 records were identified, consisting of 749 records via database search and 14 from other sources (websites, organisations and citation searching). Seventy-two full-text articles were reviewed, and 27 articles were included (Figure 1).
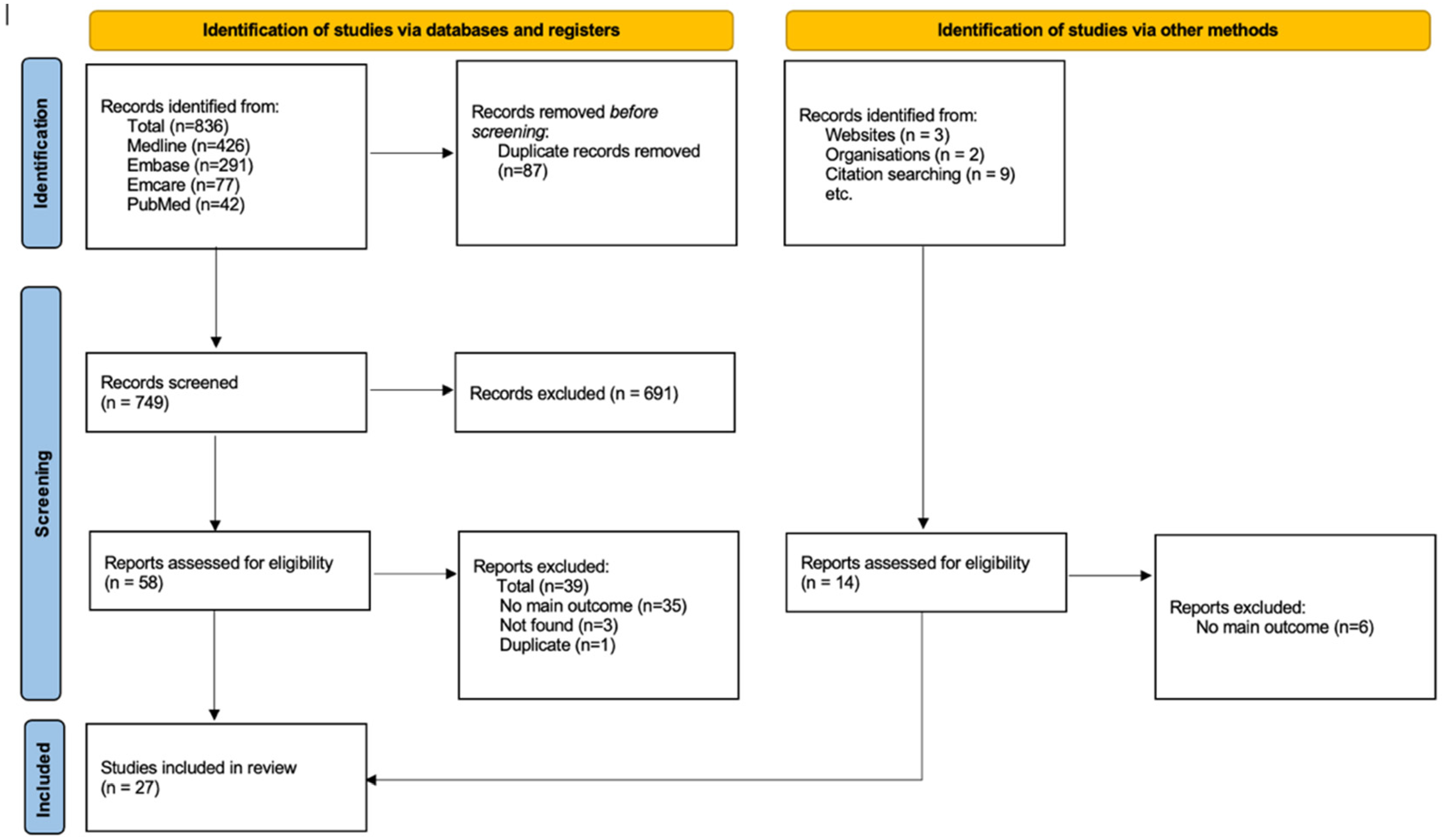
PRISMA flow chart.
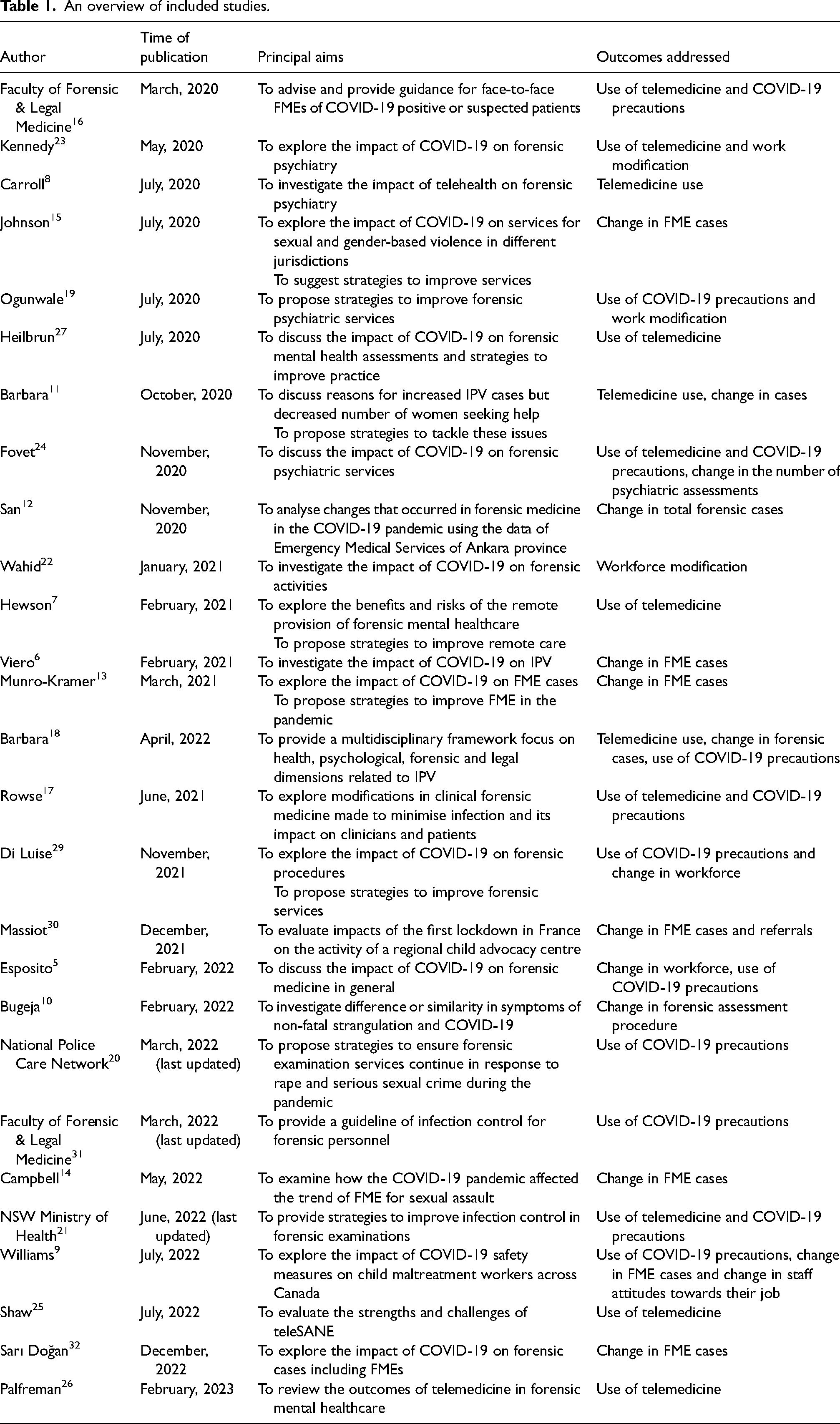
Of the 27 studies that were included, the majority were from high income countries amongst which the United States was the most frequent country of research (6/27). The two middle income countries were Turkey and Pakistan, and the low-income country was Nigeria. COVID-19 precaution measures and the use of telemedicine were the most common outcome addressed by included studies (12/27) (Table 1), followed by change in the number of forensic assessments (11/27). Some other outcomes addressed by individual studies were staff perceptions of the impact of COVID-19 on their practice, as reported by Williams et al., 9 and challenges in diagnosing domestic violence given shared manifestations of injury with COVID-19 symptoms, discussed in the study of Bugeja et al. 10
An overview of included studies.
Changes in the volume of forensic assessments
Eleven studies reported the volume change in clinical forensic assessments (Table 2). Barbara et al. 11 in Italy and San et al. 12 in Turkey both showed an approximately 50% reduction in the clinical forensic cases whilst Munro-Kramer et al. 13 noted a complete cessation of FMEs in April 2020, in the United States. Campbell et al., 14 also in the United States, noted that numbers were trending down from 24 to 5 cases between March and May 2020 and following lockdown increased to 27 in July 2020, compared to 28–37 cases on average per month prior to the COVID-19 pandemic. Conversely, Kenya reported no difference in the total number of in-person FMEs conducted in 2020. 15
Changes in the quantity of forensic assessments during the pandemic.
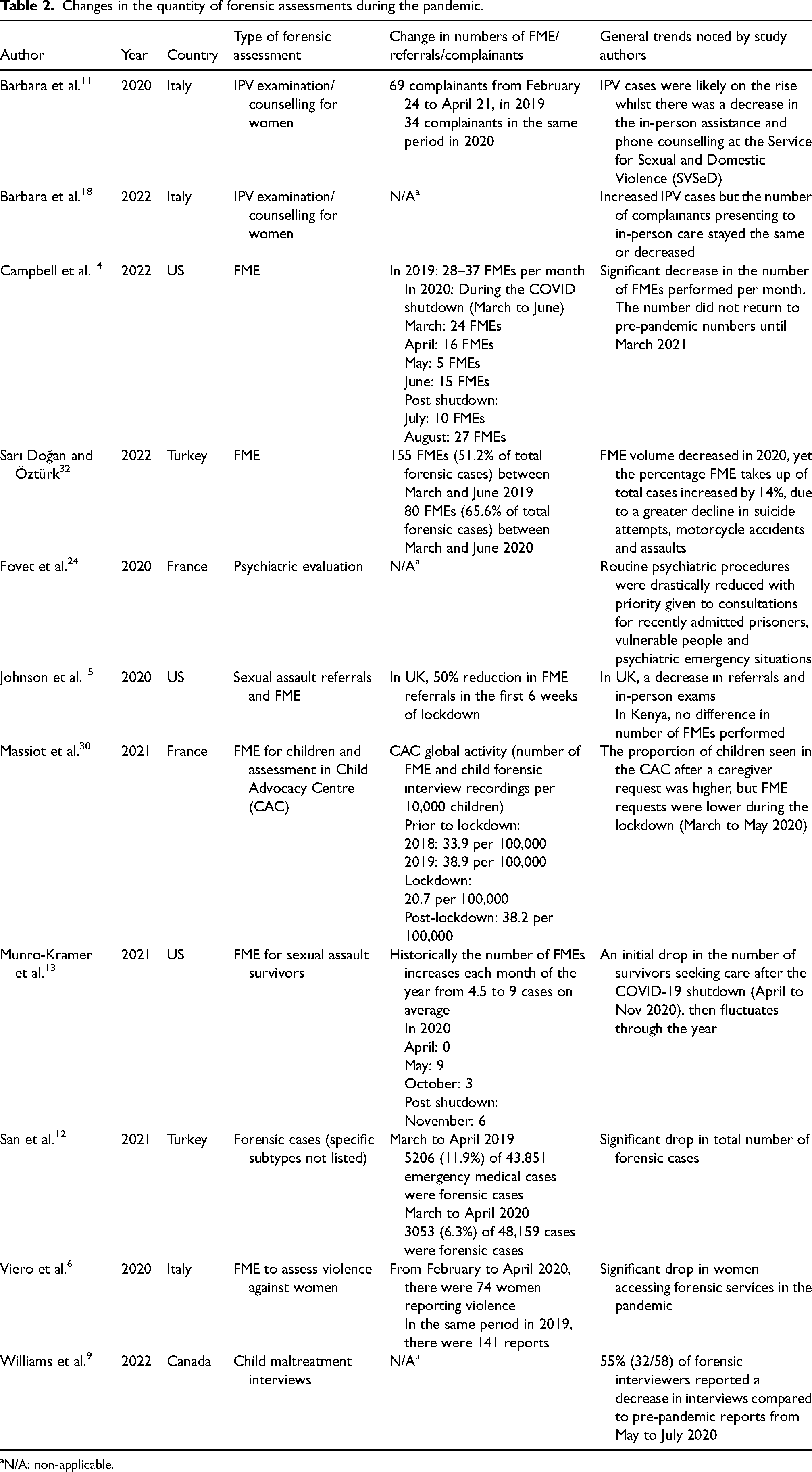
aN/A: non-applicable.
Increased implementation of telemedicine and COVID-19 precautions
Twelve studies reported increased use of telemedicine, among which five focused specifically on telemedicine implementation in forensic psychiatry (Table 1). Ten studies described COVID-19 precautions in clinical forensic medicine. Protocols and guidelines enforced COVID-19 safe practices including full use of personal protective equipment (PPE) in emergency departments (EDs), compulsory mask wearing, social distancing and hand hygiene. In one Australian jurisdiction where five hospital-based crisis units and a multidisciplinary centre were in use by a single clinical forensic medical service for sexual assault examinations, the number of sites attended by the service was reduced to three to minimise COVID-19 spread. Likewise in forensic psychiatric assessments, the inter-hospital rotation of psychiatrists was reduced. 7 The Faculty of Forensic & Legal Medicine 16 and Rowse et al. 17 recommended the use of a designated COVID-19/Suspected COVID (SCOVID) area. Rowse et al. 17 in Australia and Barbara et al. 18 in Italy reported the use of a COVID-19 hot zone for examinations while preparation of forensic equipment and PPE donning were conducted in a cold zone. A similar adoption of a hot zone was implemented in forensic psychiatric services, where a holding bay was set up for newly admitted inmates who were SCOVID before being transferred to their destination. 19 Examination rooms were required to be deep cleaned and decontaminated before and after use.
Forensic samples were handled with additional precautions during the pandemic. Forensic samples collected in COVID-19/SCOVID zones were handed to police in an outdoor area to reduce the need for police attendance inside the hospital. 17 All collected samples were double-bagged and labelled with COVID-19 risk stickers.16,17,20 Oral samples were recommended as the last sample for collection and if an oral rinse was required, patients were provided with instructions for self-collection. 21
Discussion
Summary of key findings
There was a notable decrease in the rate of clinical forensic assessments in early 2020, including FMEs for child assault, adult sexual assault, IPV and forensic psychiatric evaluations, as compared to the pre-pandemic era. However, the volume began to recover when COVID-19 restrictions were lifted. Telemedicine and COVID-19 precautions were incorporated into a wide range of clinical forensic services, which were seen to affect forensic assessment in the building of rapport, setting of examinations, work processes and handling of samples.5,9,22,23
Lower volume of forensic assessments
The reduction of in-person FMEs and phone counselling was not necessarily reflective of a decrease in the rates of violence and assault but were likely attributable to multiple factors associated with the shutdown policies and COVID-19 precautionary measures. Johnson et al. 15 reported a 50% decrease in referrals to clinical forensic services. Campbell et al. 14 found that although the police, ED and SANE (Sexual Assault Nurse Examiner) programs were operational during COVID-19, referrals to hospitals by them were significantly reduced, even stopped. Although the SANE programs tried to promote FMEs in the community clinics, the inter-agency communication and referral networks were poorly functional early in the pandemic. Even when referrals were made, some non-urgent FMEs had to be cancelled due to the overwhelmed healthcare system.14,15
Restrictive measures exacerbated interpersonal conflicts and increased perpetrators’ control over women in cohabitation, who were socially isolated and unable to seek help. 11 Overworked healthcare staff experiencing burnout may not have offered adequate referrals and potentially became less sensitive to the evidence of violence.11,18 During the pandemic, hospital settings generated community concern, such as fear of acquiring COVID-19 or a lack of support with visitor restrictions, which led to some complainants deferring their assessments. 11
Challenges in implementing telemedicine in forensic psychiatry
Implementation of telemedicine in forensic psychiatric services was not without technical and judicial challenges initially. In early 2020, judges in France proposed the use of mental telehealth assessments which was opposed by most French psychiatrists who were doubtful about conducting valid court-sanctioned psychiatric evaluations through videoconferencing. 24 At that time, resource centres for professional caregivers working with sexual offenders were the only forensic facilities in France that were able to incorporate telehealth into their daily practice. 24 This issue had not been resolved before their report was published. In the United Kingdom, forensic psychiatrists encountered some technical difficulties in making telemedicine a practical option at the outset. Prior to the pandemic, 50 of 117 prisons in the UK did not have reliable internet connectivity. During the pandemic however, 4G tablets were introduced that enabled telemedicine capabilities in all prisons. 7
Impact of telemedicine
Despite the challenges encountered by some jurisdictions in the implementation of telemedicine, its utilisation accelerated during the COVID-19 pandemic. In forensic psychiatry, telemedicine assisted prisoners’ court appearances, lowering the risk of escape and the use of restrictive measures. 23 Staff could provide regular mental health assessments and services to remote populations that were out of reach before COVID-19. 23 Telemedicine improved time efficiency due to the removal of the need for commuting.7,23
In regards to the experience of clinical forensic medicine staff, Shaw et al. found that some SANEs thought the initial intensive planning in response to the pandemic contributed to the successful rollout of the teleSANE program. 25 In contrast, other SANEs reported feeling stressed upon the implementation of the teleSANE program, due to its rapid change and the complexity of hospital systems causing information asymmetry. 25 Regarding patients’ experiences, anxiety provoked by an unfamiliar environment was addressed by telehealth for people with anxiety disorders. The subtle transference dynamics on telehealth may have encouraged disclosure of difficult topics such as sexual abuse due to less visibility, although patients’ acceptability of this form of assessment varied with their needs.7,8 Younger people tend to be more open to telemedicine, due to the familiarity with information technology. 26 However, specialised psychological measures were insufficiently validated in telehealth and loss of non-verbal cues such as emotional responses conveyed by facial micro-expressions affected the depth of rapport and potentially compromised the quality of the evaluation.8,27
In clinical forensic medicine, telemedicine was a good platform for online counselling, routine psychological support and for obtaining information prior to an FME. Telemedicine could not fully replace hands-on forensic procedures including health checks, examination and photography of injuries and swabbing for evidence.11,21 Telemedicine can be conducted via phone calls or videoconferencing. When comparing phone calls to videoconferencing, phone calls may better address issues with privacy, unfamiliarity and the potential for exacerbation of pre-existing suspiciousness. This is however, at the cost of visual information provided by videoconferences, so such trade-offs should be taken into consideration. 27 Scenarios in which each telemedicine mode is best suited should be discussed in future studies or guidelines.
Commonly shared weaknesses of telemedicine were technological barriers in communication.7,26,28 Access by either the examiner or the patient was hampered if there was unfamiliarity with new technology or poor connectivity, background noise and low speaking volume. The challenges were amplified by additional needs for patients with hearing loss, intellectual disability, educational deficits, acute psychiatric problems or cognitive impairment.7,17,18 Confidentiality, data security and safe sharing of documents were also identified as issues of concern.7,17,27
Impact of COVID-19 precautions
Although COVID-19 precautions were put in place for the safety of both clinicians and patients, wearing full PPE notably shifted the patient–doctor dynamics. Building rapport and expressing empathy for complainants of sexual assault or IPV was more challenging, particularly where complainants already perceived the hospital setting as a dehumanising and traumatising environment. 8 When asked about the impact of COVID-19 safety measures, 63% of child maltreatment staff reported a negative impact on rapport-building and 44% reported decreased willingness of children to disclose abuse. 9 Medical staff who used masks, gloves and physical distancing, noted significantly higher stress levels and reported increasing tension between colleagues, and concerns about adequate PPE due to shifting protocols.9,15
Disrupted continuity and quality of care
Work processes and workforce reforms as a result of COVID-19 may result in suboptimal care in forensic medicine. On prison wards, there was a decline or a halt in multidisciplinary care to avoid over-crowding and cross-team COVID-19 transmission. Day-long ward rounds were replaced with shorter focused ones.19,23 In one service, a mental health nurse was integrated into the general medical clinic under intramural service provision. This nurse-driven service initiated interim treatment pending psychiatrists’ review based on symptom profiles, but the nurse was not expected to document a full mental health assessment or prescribe atypical psychiatric medication. Medication switching or long-acting depot injection were thereby all postponed for patients. 19 In clinical forensic medicine, recruiting non-specialist doctors and newly graduated doctors favoured the frequency of errors in practice and the increase in cases of malpractice claims, leading to a potential increase in litigation within hospitals. 5 These reforms significantly affected the quality and quantity of practice delivered.
Suggested strategies
Resource issues in healthcare heightened by the COVID-19 pandemic have driven the need for solutions and the deployment of medical professionals. A surge in IPV cases has created more demand on clinical forensic medicine services. The burden of this issue needs to be clearly defined through systematic research and addressed by prioritising IPV prevention strategies. IPV care can be integrated into existing healthcare services rather than offered as stand-alone services that may limit complainants’ access to hospitals. 11 Any divergence from routine forensic procedures should be accurately documented to guarantee forensic evidence taken is held up to high-quality standards. Staff need new training in the utilisation of telemedicine and modified work processes. Whether telemedicine is acceptable or inadvisable is ideally a carefully considered case-by-case decision, to be made by forensic experts. 8 Patients’ individual circumstances, location and other factors that may contribute to greater difficulties in engaging with remote care should be carefully considered. 7 For those working in ED, there is a need to improve the ability to distinguish between violence and COVID-19, as symptoms of non-fatal strangulation are often shared with COVID-19 symptoms such as sore throat, headache, cough and dysphonia. Failure to recognise these symptoms risks either missing delayed onset of life-threatening complications or not following COVID-19-adapted models of care. 10
Limitations
The paper was limited by the absence of studies from 2022 exploring changes in the post-COVID-19 era. This gap may be due to the natural lag in research time frames and the evolving nature of infection control measures. With the increased vaccination rate since 2021 and inevitable exposure to COVID-19 in social settings, hospitals have gradually de-escalated the infection precautions. Consequently, many changes in forensic medicine and forensic psychiatry were no longer needed for the purpose of minimising risks of infection.
The paper was also limited by a lack of available evidence regarding clinical forensic issues outside of forensic psychiatry, sexual assault, IPV and child maltreatment, for example, detainee assessments and elder abuse.
Conclusion
This review provides the first overview on the pandemic-driven changes in clinical forensic medicine and forensic psychiatry in respect of volume changes in forensic assessments and incorporation of COVID-19 precautions. These changes have been necessary but have disrupted rapport building, complicated the sample handling steps and restricted in-person evaluations and areas dedicated to forensic assessments. The COVID-19 pandemic highlighted the need for adaptability and flexibility in healthcare and forced forensic services to explore and adopt new strategies for conducting assessments. The ability to embrace and integrate technology was critical and demonstrated that telemedicine was a viable option for the assessment of forensic patients. So, importantly, the introduction of technology such as telemedicine in the COVID-19 setting paved the way for its continued use within forensic services, thereby enhancing accessibility, particularly for those located in remote or high-risk settings who might otherwise not have timely access. Forensic medicine will continue to adjust to the evolving needs in the post-COVID-19 era and some adaptations will persist and be built upon. It is critical to reassess the changes in the future and re-evaluate the impact of those that persist.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.