
Abstract
A medical examiner (ME) system was introduced to England and Wales in 2019 intended to ensure appropriate notification of cases to HM Coroner (HMC). The aim of the study is to determine and compare: (a) the nature of notifications to HMC for Norfolk from the Norfolk and Norwich University Hospital (NNUH) in 2018 compared with 2022; (b) to determine the outcome of those notifications and (c) to establish patterns of change in the number and nature of such notifications. HMC and ME datasets were interrogated to determine differences between notifications to HMC and outcomes in 2018 compared with 2022. From deaths at NNUH (2018 – n = 2605; 2022 – n = 2969), there were significantly fewer HMC notifications in 2022 compared with 2018 (25.3% vs. 17.6%). A decrease in notifications was noted for persons undergoing any ‘treatment or procedure of a medical or similar nature’ (24.0% vs. 16.2%) p < 0.0014. An increase in notifications was noted for neglect, including self-neglect (3.3% vs. 12.2%) p < 0.001. Of the coronial outcomes, there were significant increases in the numbers of post-mortem (PM) examinations (29.3% vs. 35.5%) p = 0.0276 and inquests (26.0% vs. 31.4%) p = 0.0485). There was a significant decrease in no further action by HMC (5.7 vs. 2.3) p = 0.0485. The study shows that the introduction of the medical examiner service has resulted in significant change in the nature of HMC notification categories. The notifications appear to be more appropriate, with an increased proportion of inquests and PM examinations and with a reduction in 100 A or ‘no further action’ outcomes.
Introduction
Until 2013, coroners operated under the Coroners Act 1988 1 which was a consolidation of the Coroners Act 1887. 2 A fundamental review of the coroner and death certification systems was commissioned by the Home Office, and this was reported in June 2003. 3 It concluded that neither the certification nor the death investigation system was fit for purpose in modern society, and that substantial reform was needed.
The criminal activity of serial killer, Harold Shipman, a general practitioner who was found guilty of 15 counts of murder at Preston Crown Court in 2000, provided the unanticipated drive to reform the coroner service and ensure that all deaths, whether suspicious or not, should be subject to scrutiny. 4 The Fundamental Review 3 and the Shipman Inquiry 5 provided the necessary impetus for reform which culminated in the Coroners and Justice Act 2009, 6 which came into force on 25 July 2013.
One of the Shipman Inquiry recommendations was to establish a medical examiner system to provide independent statutory scrutiny of all deaths. Sections 18–21 of the Coroners and Justice Act 2009 laid down the framework for such a service. A number of hospital-based scandals of which the most significant driver for a medical examiner system was the 2013 Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry 7 chaired by Robert Francis QC, identified numerous, serious failings in care between 2005 and 2009. The report made 290 recommendations, of which a number made specific reference to the need for an independent medical examiner system. The common theme for most of these scandals has been that the concerns of bereaved families and whistleblowers have been ignored. 8
After many delays, the medical examiner (ME) system was introduced in England and Wales in May 2019.9,10 For pragmatic reasons, the ME system was rolled out in acute hospitals as a non-statutory process before it became a statutory system. The intention was to ensure all hospital deaths were reviewed by the independent ME system. This review is referred to as a ‘scrutiny’. All acute hospitals were required to develop their medical examiner service (MES) with the intention of eventually scrutinising all community deaths as well. Although the MES sits within acute trusts, it is independent of them with separate reporting lines to regional medical examiner teams and ultimately the national medical examiner.
Since 2019, the ME system has been expanded across England and Wales from scrutinising all hospital deaths to an increasing proportion of community deaths with the intention of ensuring that every death in England and Wales will be reviewed by an MES. After a number of delays (caused in part by the COVID-19 pandemic), it has at last been announced that from 9 September 2024, it will be a statutory requirement that every death in England and Wales (irrespective of where that death occurs) which is not covered by the 2019 notification requirements to HM Coroner (HMC), will in the first instance be subject to ME scrutiny. 11
The ME system has the aims of independently:
Providing bereaved families with greater transparency and opportunities to raise concerns, improving the quality/accuracy of medical certification of cause of death, ensuring referrals to HMC are appropriate, supporting local learning/improvement by identifying matters in need of clinical governance and related processes, providing the public with greater safeguards through improved and consistent scrutiny of all non-coronial deaths, and support healthcare providers to improve care through better learning, aligning with related systems such as the national learning from deaths framework and universal mortality reviews. What did the person die from? (ensuring accuracy of cause of death on the medical certificate of cause of death [MCCD]). Does this case need to be reported to a coroner? (ensuring timely, accurate referral). Are there any clinical governance concerns? (ensuring the relevant authority is notified). Review the medical records and any supporting diagnostic information. Discuss the proposed MCCD with the doctor who was treating the patient on their final illness (the qualified attending practitioner – QAP) and enquire about any concerns of care. This may be done by an ME – or medical examiner officer [MEO] under delegated authority. Agree the proposed cause of death and the overall accuracy of the MCCD with the QAP. Discuss the cause of death with the next of kin (NOK)/informant and establish if they have any concerns with care (this may be done by an ME – or MEO under delegated authority).
In all those cases not further investigated by HMC, the MES addresses the following issues:
To achieve this, the MES completes the following steps to arrive at their decision:
Completion of these steps is referred to as a scrutiny. Clarification of the statutory requirement to notify a particular death to the coroner was provided by the introduction of the Notification of Deaths Regulations 2019 guidance which specified what deaths must be notified to HMC.
12
The most significant difference of the new regulation was that deaths within 24 h of admission to hospital no longer had to be notified to HMC (unless it fell into one of the groups identified in the notification of deaths regulations) unlike prior to 2019.
The MES at the Norfolk and Norwich University Hospital (NNUH) has documented the reasons for, and the outcome of, notifications from the MES to the Norfolk Coronial Service since June 2020. Notifications and outcomes of notifications prior to this were previously documented solely by the Norfolk Coronial Service. Payne-James et al. 13 studied the workload of the MES at NNUH from 1 June 2020 to 31 May 2021 and noted that in this period, 458 (17.04%) of deaths scrutinised were notified to HMC for Norfolk.
Coroners must decide whether they have a duty to investigate the death, as set out in Section 1 of the Coroners and Justice Act 2009, 6 and may decide, without a post-mortem (PM), that the duty does not apply. In these cases, a Form 100 A will be completed and sent to the Registrar so that the registration of death process can be completed. Potential outcomes following notifications to coroners are summarised in the Ministry of Justice ‘Guide to Coroners’ Statistics. 14
In a previous study from the MES at NNUH between 1 June 2020 and 31 May 2021, 192 (41.9%) Form 100 As were issued. Two hundred and fifty-two (55%) cases were taken for inquest (135–29.4%) or PM examination (135–25.5%). 14 (3%) were ‘no further action’ and required the patient's general practitioner to complete the MCCD. 13
ME services have been present in most acute hospitals in England and Wales since 2019. 10 In 2022, there were 577,160 deaths registered in England and Wales; this was 9174 (1.6%) fewer deaths than in 2021 and 33,747 (6.2%) more deaths than the 5-year average (2016–2019 and 2021). 15 Of these 208,400 deaths (36%) were notified to HMC an increase of 7% since 2021. 16 In 2022, PM examinations were held for 90,200 deaths notified to HMCs.
In 2022, coroners opened 36,300 inquests an increase of 11% from 2021. In 2022, 35,600 inquest conclusions were recorded in total, an increase of 10% on 2021. Inquest findings that death was by natural causes, accident/misadventure or unclassified conclusions had the largest increases, up 40%, 14% and 7% in 2021, to 5100, 8800 and 8700 in 2022, respectively.
In 2022, 252,539 deaths were reviewed by all ME services in England and Wales.
17
On 28 June 2022, the Coroners and Justice Act 2009
4
was amended to enable coroners to discontinue an investigation when a death from natural causes becomes clear before inquest, even where there has been no PM examination. Before the amendment coroners could not discontinue an investigation unless a PM revealed a natural cause of death. That meant that if a natural cause of death became clear after an investigation had commenced, the coroner either had to order an unnecessary PM, or proceed with an inquest. The amendment has widened the circumstances in which discontinuance can occur. Except where there is reason to suspect that the death occurred in custody or state detention, a coroner must discontinue an investigation if:
A natural cause of death becomes clear before inquest and the coroner thinks that it is not necessary to continue the investigation. where there has been a PM or where there has been no PM, but the cause of death has become clear by other means.
This means that investigations can now be discontinued either:
If a coroner decides to discontinue an investigation, Regulation 17 of The Coroners (Investigations) Regulations 2013 provides that the coroner must record the cause of death and notify the next of kin or personal representative of the deceased using Form 2 (a Notice of Discontinuance).
18
The coroner has a duty to consider, in every case, whether to make a Report to Prevent Future Deaths (often referred to as PFD or Regulation 28 report). Four hundred and three PFD reports were issued in 2022, a decrease of 8% compared to 2021. This duty to consider a PFD report arises under Part 7 to Schedule 5 of the Coroner and Justice Act 2009 and is exercised under Regulation 28 of the Coroners (Investigations) Regulations 2013. 10 The reports come in an established format, laid down by the Chief Coroner, within which the Coroner will state their concerns and why they think action should be taken to prevent future deaths. 19 The coroner cannot make recommendations.
The new notification guidelines 2 clarified and expanded reasons for notification to HMC shortly after the introduction of the ME Service. No previous study has explored the differences between the nature and the outcome of coronial notifications before and after the introduction of the MES, one aim of which is to improve and ensure appropriate coronial notification. This study has been designed to explore those differences.
Aims of study
The aims of this study are to determine and compare:
The number and nature of notifications to HMC for Norfolk from NNUH in 2018 and comparing this with the number and nature of notifications in 2022 (after the introduction of the NNUH MES and the new Notification Guidelines). To determine the outcome of those notifications. To establish patterns of change in the number and nature of notifications in 2022 compared with 2018.
Methods
HMC for Norfolk accepts notifications via the WPC Coroners software system (WPC Software Ltd, Bristol) which is a case management and workflow system designed to manage all coronial cases from the point of referral, through to closure. It is a web-based system to help meet the needs of the coroner's service alerting users when there are steps or actions to be taken. It records the reasons and circumstances for notification to the Coronial Service. The MES at NNUH maintains its own database of all notifications to coroners. Table 1 lists the relevant data retained in the two databases.
Data collected by the WPC portal and NNUH MES database.
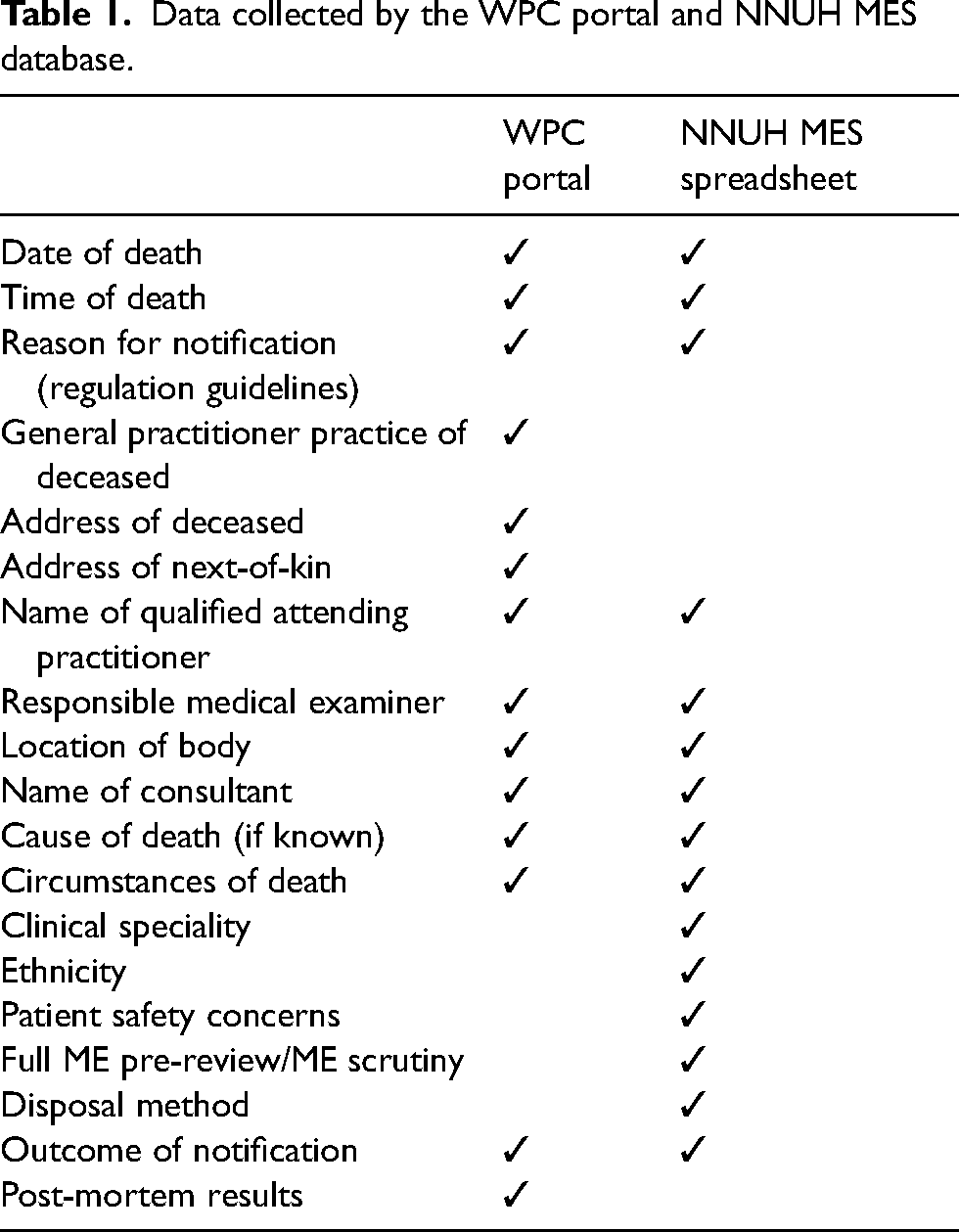
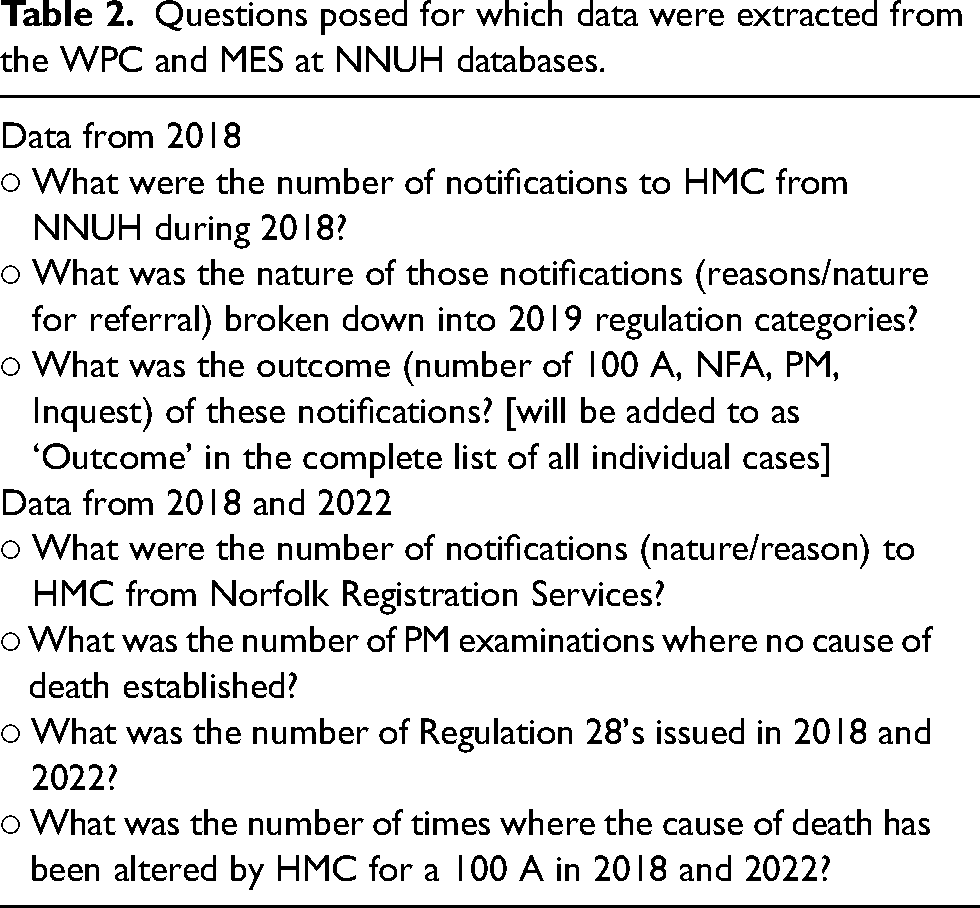
Table 2 lists the questions posed for which data were extracted from the two databases.
Questions posed for which data were extracted from the WPC and MES at NNUH databases.
Comparisons of the two datasets have been made to determine any differences and how these have impacted on workloads.
As the Notification Guidelines 2 had not been published until October 2019 (after the introduction of the MES) in order to enable comparisons to be made it was necessary to review all coronial notifications in 2018 and assign them to categories as if they had been notified after the introduction of the new Guidelines. The 2018 data were derived from a search of the Norfolk WPC Coroners portal data and the reason for the notification to HMC was reviewed by the authors (TB – ME and LP – MEO) and by consensus allotted to the 2019 Notification categories to allow comparison. For some cases (n = 48 for 2018 and n = 1 for 2022) it was not possible (based on the limited information available) to accurately allot a notification category.
Results
There were 2605 deaths at NNUH in 2018 and 2969 in 2022. There were significantly more notifications to HMC from NNUH in 2018 than there were in 2022 (659 [25.3%] vs. 522 [17.6%]) (Chi-square: 49.47, p-value < 0.001).
Table 3 shows the nature of notifications (reasons/nature for referral) broken down into 2019 regulation categories. For both 2018 and 2022, the most common reasons for notification were unchanged and remained, respectively, ‘violence, trauma or injury’ (27.7%, 27.8%); ‘cause of death unknown’ (22.3%, 25.9%) and ‘person undergoing any treatment or procedure of a medical or similar nature’ (20.2%, 16.1%). The categories most rarely requiring notification were ‘died in custody or state detention’ (0.3%, 1.3%); ‘identity of deceased is unknown’ (0.2%, 0.2%) and ‘poisoning, including by an otherwise benign substance’ (0.2%, 0%).
Distribution of reason for notification by year.
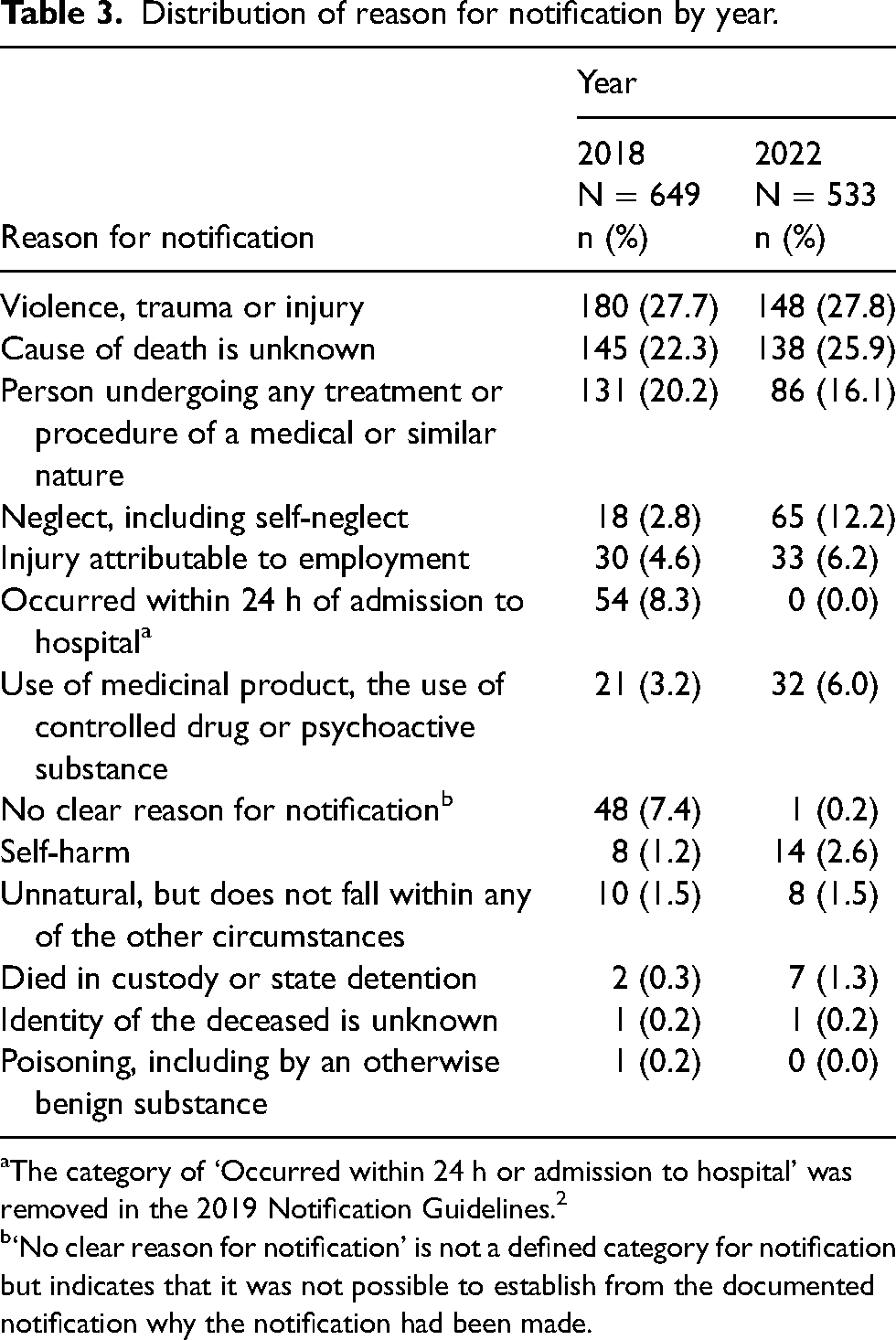
The category of ‘Occurred within 24 h or admission to hospital’ was removed in the 2019 Notification Guidelines. 2
‘No clear reason for notification’ is not a defined category for notification but indicates that it was not possible to establish from the documented notification why the notification had been made.
Table 4 compares the outcome of all notifications to HMC between 2018 and 2022 having excluded the (no longer present) ‘within 24 h of admission to hospital’ and the notifications where reasons could not be established. There are two categories which show significant differences in notifications. These are for ‘person undergoing any treatment or procedure of a medical or similar nature’ which represents 16.2% of 2022 notifications compared with 24% in 2018 (p = 0.0014) and ‘neglect, including self-neglect’ increasing almost fourfold from 3.3% in 2018 to 12.2% in 2022 (p < 0.001). For other categories, there were no significant differences.
Distribution of reason for notification by year (excluding reason only available for the year 2018 and unclassifiable cases).
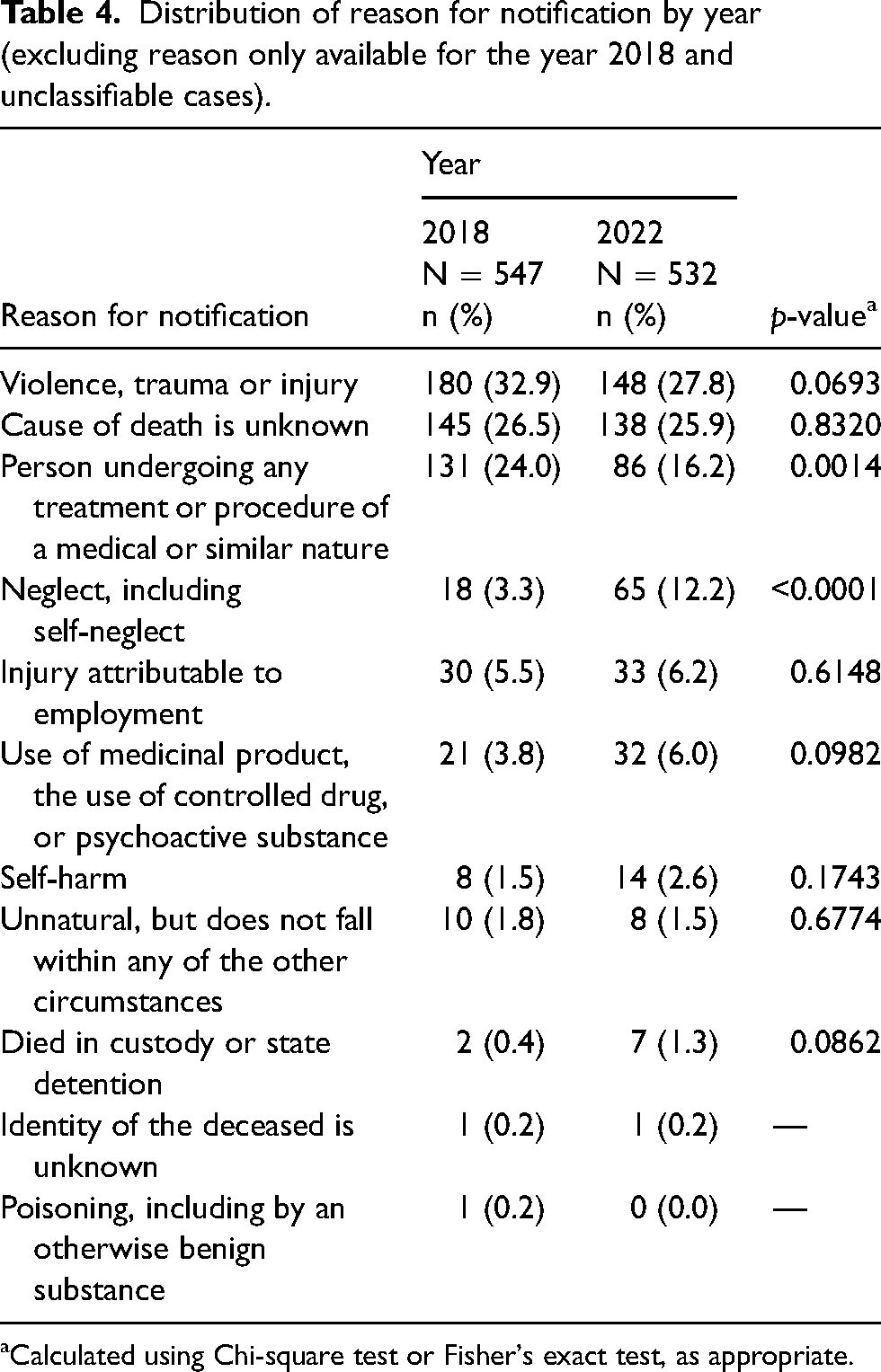
Calculated using Chi-square test or Fisher's exact test, as appropriate.
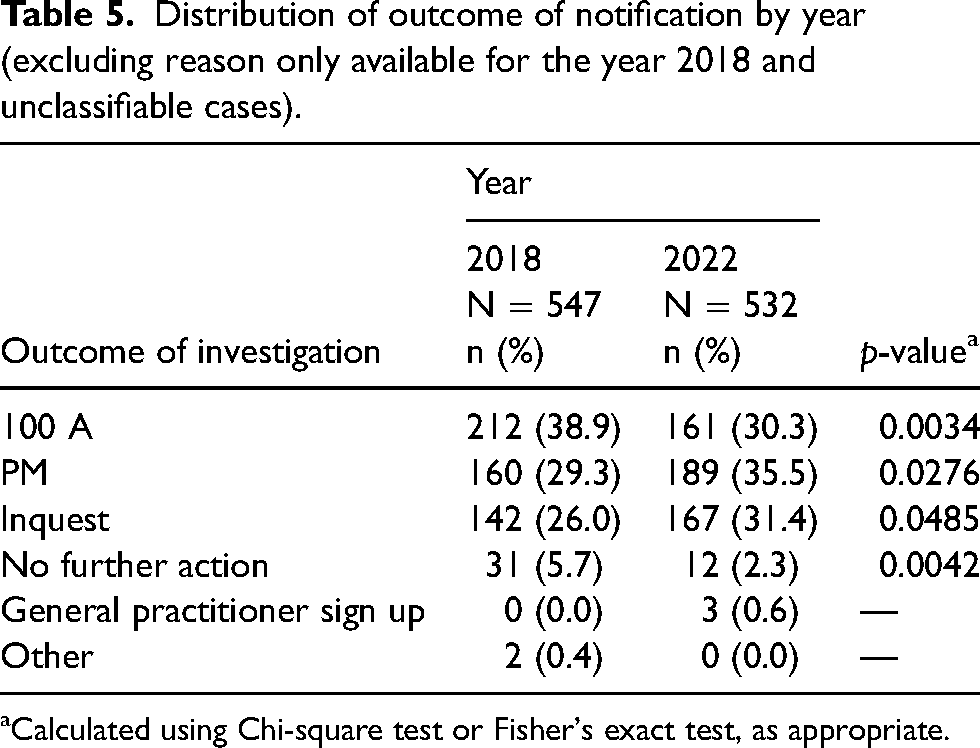
Table 5 shows that there have been significant reductions in the number of 100 A disposal option and no further actions. There has been a significant increase in the number of PMs and inquests.
Distribution of outcome of notification by year (excluding reason only available for the year 2018 and unclassifiable cases).
Calculated using Chi-square test or Fisher's exact test, as appropriate.
Of PMs undertaken to establish a cause of death in 16/162 (9.87%), no cause of death was established (remained unascertained) in 2018 and 14/189 (7.4%) in 2022.
Two Regulation 28 reports were issued in 2018. Thirteen Regulation 28 reports were issued in Norfolk in 2022. Three of these reports were outside the MES catchment area. In four of the reports issued, the MES had direct involvement in the case and were responsible for submitting the coronial notification in the first instance. In one of the reports, medical advice was sought from the ME during the course of the investigation. Figure 1 summarises the nature of the concerns raised in these Regulation 28 reports and it is notable that these apply variously to acute settings, community settings, mental health settings, ambulances, private providers and care homes.

Summary of concerns raised in reports to prevent future deaths (Regulation 28 reports).
Discussion
The study has shown that the number of notifications to HMC for Norfolk from NNUH in 2018 compared with 2022 was significantly reduced from 25.3% of deaths in 2018 to 17.6% in 2022. The outcome of those notifications has been documented and compared. For both 2018 and 2022, the most common reasons for notification remain for violence, trauma or injury (2018 – 27.7%, 2022 − 27.8%) and where the cause of death is unknown (2018 – 22.3% and 2022 – 25.9%). The results for the former are unsurprising. The small increase in unknown cause of death may reflect settings where a QAP has suggested a mode such as cardiac arrest, without any supportive diagnosis and which the MES has determined is better identified as unknown.
The drop in notifications of deaths occurring within 24 h of admission to hospital (2018 – n = 54 to 0 in 2022) was expected as the need for notification was removed in 2019, although a number of clinicians still believed this to be a requirement until so advised by the MES. Circumstances where there was no clear reason for notification, was significantly reduced from 6.62% of the total to 0.2%. This is a positive aspect of the MES but identifies an area for potential service improvement to achieve 0% as the reason for notification should always be made clear.
When comparing 2018 and 2022, the MES introduced in 2019 resulted in significant reductions in notifications for deaths involving persons undergoing any treatment or procedure of a medical or similar nature from 24% to 16%. This again reflects a positive aspect of the MES, as by liaison with HMC, a better understanding of the relevance of this notification requirement can be conveyed to clinicians. There was a significant increase in notifications for neglect (including self-neglect), from 3.3% to 12.2%, and this likely reflects the MES scrutiny of matters beyond hospital admission and which hospital personnel may not have been aware. These matters could include information from other healthcare teams, ambulance personnel and in particular, the bereaved.
In terms of the coronial process, there has been a significant decrease in 100 A outcomes (2018 – 38.9% vs. 2022 – 30.3%) and a concomitant increase in the proportion of inquests (2018 – 26% vs. 2022 – 31.4%). These figures suggest that the MES is better at appropriately identifying those cases which HMC will then proceed to fully investigate than previously when notifications from hospitals were determined by the clinical teams. This may reflect the medical and healthcare expertise within the MES. This is another positive aspect of MES scrutiny which was a hoped-for outcome following the introduction of the MES.
Despite the limitations of the study, spanning as it does a time period where updated notification requirements for HMC were introduced, and taking into account these changes, the data suggest that there has been a real change in the nature of notifications to HMC following the introduction of an MES, in that the notifications (a) are fewer, (b) are more appropriate and (c) result in an increased proportion of inquests and PMs with (d) reduction in 100 A or no further action outcomes.
Conclusions
This study aimed to identify the number and nature of notifications to HMC for Norfolk from NNUH in 2018 and compare this with the number and nature of notifications in 2022; to determine the outcome of those notifications and to establish patterns of change in the number and nature of notifications in 2022 compared with 2018. These were intended to establish whether some of the intended aims of the ME system were achieved.
The findings of this study show that the MES at NNUH (even prior to its statutory introduction) appears to be fulfilling those aims with respect to coronial notification of death to HMC by reducing their number and improving their quality and appropriately identifying those deaths that need further investigation.
The findings are presented from a well-established, fully staffed MES and it is to be hoped that these findings reflect the nature of changes across England and Wales in all MESs. Other MESs should review their workload to see if similar patterns of change exist, as might be expected, to confirm the relevance and importance of such services to the bereaved, to the clinicians, to coroners and for patient safety.
Footnotes
Acknowledgements
We thank Grace Anderson, Anna Wicks and Emmanuel Ng for their hard work in collating data. Similarly, we wish to thank Tom Ruddock at WPC Software Ltd for his advice and assistance. We thank all our Medical Examiner Officer and Medical Examiner colleagues who have worked with us to develop the Medical Examiner Service at the NNUH and we thank the NNUH management team for their continued support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.