
Abstract
A case of septic pulmonary thromboembolism arising from thrombophlebitis of the prostatic venous plexus associated with long-term urinary catheterisation in a 51-year-old man is reported. Despite a previous autopsy having been conducted in the country where he had been resident overseas, a re-examination showed histological evidence of mild patchy chronic prostatitis with a florid, focally purulent, thrombophlebitis of the periprostatic venous plexus with abscess formation and evidence of bacterial overgrowth. Corresponding microscopy of the lungs showed septic microthromboemboli within small pulmonary arteries with variable degrees of necrotising acute inflammation and thrombosis. Death was not due to ‘acute pulmonary oedema’ as had been originally certified but to septic thromboembolism. This case demonstrates the need to carefully evaluate the prostatic venous plexus at autopsy, and also the type of problems that may arise at the time of the re-examination of repatriated remains.
Keywords
Introduction
It is estimated that 10 million cases of pulmonary thromboembolism occur annually worldwide, 1 being responsible for approximately 5% of sudden deaths in hospitalised patients, and a significant number in medicolegal settings.2,3 It is a diagnosis that may be difficult to make clinically 4 and may occur at any age, although it is more often found in adults. 5 Most commonly pulmonary thromboemboli arise from deep vein thromboses of the lower legs associated with a well-recognised and wide range of predisposing factors. However, a variety of alternate and uncommon aetiologies exist. The following case is reported to demonstrate yet another rare variant where septic pulmonary thromboemboli arose from a region of septic thrombophlebitis of the prostatic venous plexus associated with long-term urinary catheterisation. Issues that may arise in assessing deaths that have occurred in countries with different medical and medicolegal standards are also discussed.
Case report
A 51-year-old man who had been living in South East Asia for a number of years had an indwelling urinary catheter in-situ for reasons that were not clear from the medical records that were provided when his body was returned to Australia. He had been complaining of pain and discharge of mucus through and around the catheter with sudden deterioration followed by collapse and death.
An autopsy was performed in the country of his death with the lethal episode being attributed to ‘acute pulmonary oedema’. After his embalmed body was repatriated to Adelaide, South Australia the State Coroner directed a second autopsy to be performed at Forensic Science SA, 3 weeks after his death.
There was evidence of the previous autopsy examination with opening of the cranial cavity, thorax and abdomen. A sutured midline post mortem incision extended from the point of the chin to the pubis. There was no evidence of embalming via vascular perfusion or cavity cannulation although copious brown watery fluid in the abdominal and thoracic cavities had an odour in keeping with embalming fluid. There was patchy green discolouration with skin slippage of the face, arms, legs, and back with putrefactive skin blistering over the legs. Dissections were in some instances rudimentary with absence of some organs.
Both lungs were still attached to their bronchi and were intact other than evidence of removal of a portion of tissue from the upper lobe of the left lung. No dissections had been performed. The heart was absent except for a 28 gram slice of the apices of the left and right ventricles. The descending thoracic aorta had been mobilised from the spine but remained unopened. The abdominal aorta was undissected and still attached to the spine. The stomach had been opened in two places along the greater curve. The liver was normally located and intact except for removal of a portion of tissue from the antero-inferior aspect of the left lobe. The left kidney was incomplete with the lower pole attached to the retroperitoneum in continuity with its ureter. A separate portion of kidney tissue was located free within the abdominal cavity. The right kidney was unexamined, intact and in its normal location. The brain had been dissected.
The most significant findings were limited to the genitourinary system and lungs. Both kidneys showed moderate hydronephrosis with scarred, thinned cortices, and moderately dilated ureters which were inserted normally into the bladder. A Foley catheter was present within the bladder with chalky encrustation around the distal end suggesting that it had been left in situ for some time. The lungs were congested and oedematous with unusual patchy subpleural consolidation suspicious of pneumonia. The heart was largely absent as a result of the previous examination.
Histological assessment of the bladder revealed chronic cystitis with mild chronic inflammation of the ureters. Both kidneys showed extensive scarring with hypertensive vascular changes, chronic pyelonephritis and subtle luminal dilatation of the proximal convoluted tubules associated with flattening of the lining epithelium suggestive of acute renal injury. No acute inflammation was identified in the kidneys, ureter or bladder. The prostate showed mild patchy chronic prostatitis with focal thrombosis of the periprostatic venous plexus, florid, focally purulent, thrombophlebitis (Figure 1), abscess formation and evidence of post mortem bacterial overgrowth.
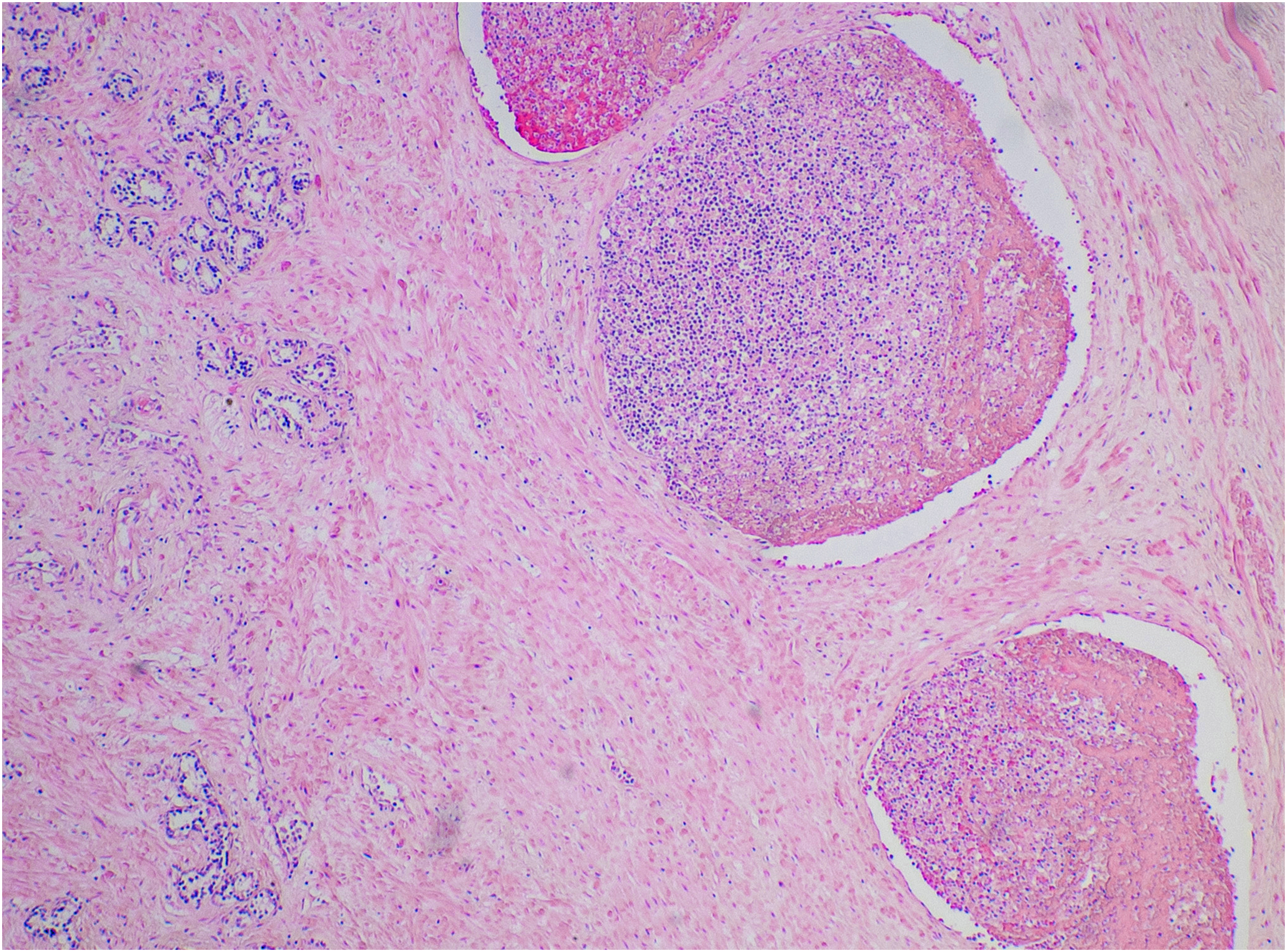
Focal purulent thrombophlebitis and thrombosis of the periprostatic venous plexus with adjacent prostatic glands (haematoxylin and eosin, H&E x 100).
Microscopy of the lungs showed foci of necrosis with patchy post mortem bacterial overgrowth, but without acute inflammation. In some sections, however, small pulmonary arteries contained septic microthromboemboli, with variable degrees of necrotising acute inflammation and thrombosis (Figures 2A & B). The appearances were in keeping with focal areas of necrosis and infarction due to septic thromboembolism of small pulmonary arteries.
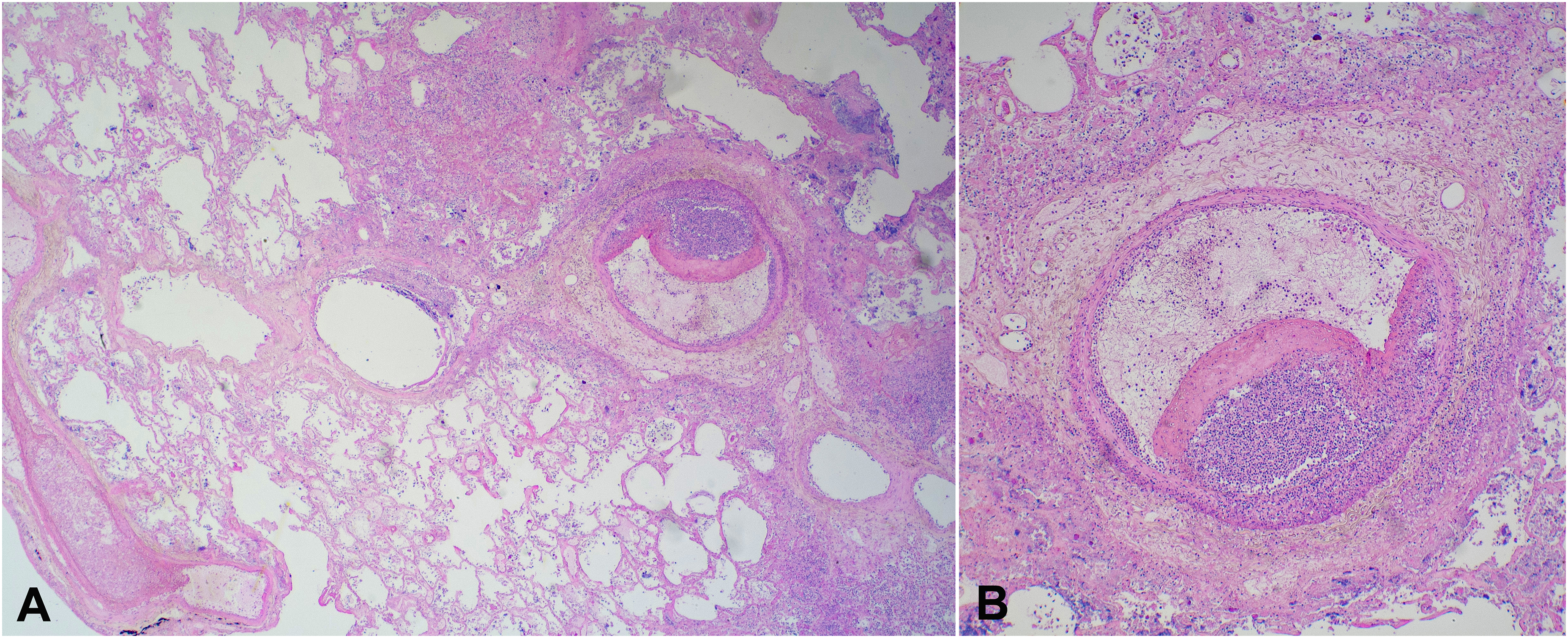
(A) Lower power view of the lungs showing foci of necrosis with patchy post mortem bacterial overgrowth, but without acute inflammation. In scattered areas small pulmonary arteries contained septic microthromboemboli (H&E x 50). (B) A small pulmonary artery containing a septic microthromboembolus with acute inflammation and a fibrin thrombus (H&E x 100).
Death was, therefore, attributed to septic pulmonary thromboembolism arising from thrombophlebitis of the prostatic venous plexus associated with long-term urinary catheterisation.
Discussion
The pathogenesis of thrombus formation is underpinned by the tenets of Virchow's triad (endothelial cell injury, hypercoagulability and blood stasis). Thus, a combination of damaged endothelium and venous stasis, in concert with imbalance between coagulation and anti-coagulation factors, promotes the formation of fibrin thrombi. 6
Factors that predispose to the occurrence of clot formation and embolization, therefore, include local or systemic acute or chronic conditions which increase the risk of endothelial damage (e.g., trauma, iatrogenic medical device insertions, infections, including most recently SARS-CoV2, whether asymptomatic or not), hypercoagulability (e.g., inherited coagulation disorders, pregnancy, oral contraceptive use, obesity, disseminated malignancy, antiphospholipid antibody syndrome, sepsis), and venous stasis (e.g., due to prolonged inactivity due to recent surgery, stroke with extremity paralysis, quadriplegia/paraplegia, long-haul travel, or hospitalisations).6–10 On occasion, however, no risk factors will be identified. 11 With infection, such as in the reported case, organisms can induce platelet aggregation and activate the coagulation cascade, resulting in focal accumulation of layers of fibrin and bacteria. 12
Septic pulmonary thromboembolism occurs when an extrapulmonary locus of infection gives rise to thrombi that contain microorganisms embedded in the fibrin matrix. 13 Thrombi are then transported to the pulmonary vasculature through the venous system, sometimes resulting in infarction due to vascular obstruction and on occasion death due to right ventricular decompensation and hypoxaemia with ventilation-perfusion mismatch. Lung abscesses or pneumonia are other potential complications in survivors. 14 Over half of septic pulmonary thromboembolism cases arise from tricuspid endocarditis associated with intravenous drug use 12 (although this is becoming a less common complication due to better needle hygiene 15 ). Alternate causes of septic pulmonary thromboembolism include intravascular device-related infections,16,17 skin and soft tissue infections, 18 liver and kidney abscesses,19,20 and organ transplants. 21 Other foci may involve peritonsillar and periodontal abscesses, cellulitis, osteomyelitis, and urinary tract infections. 22
In contrast, only isolated cases of septic pulmonary thromboembolism originating from the genitourinary tract or from catheter use have been reported, with very rare fatalities. Infection of indwelling catheters and devices is predisposed to compromised immunity and diabetes mellitus,20,22 often associated with the formation of a biofilm (an adherent film that coats a surface, incorporating bacteria) with resulting infection. 23 It is unclear from the history in the reported case whether the decedent had suffered from diabetes mellitus. Septic pulmonary thromboembolism may also arise from acute bacterial prostatitis with prostatic abscesses due to organisms such as Klebsiella pneumoniae. Embolism to the lung may occur via Batson's venous plexus. 14 Other preceding events include urinary tract infections, 22 epididymitis, 24 and kidney abscesses. 25
The reported case also demonstrates problems that may arise with the medicolegal evaluation of repatriated bodies from overseas. Access to reliable antecedent medical histories, death investigations and autopsy reports may be difficult and records that are forwarded may not be complete. Original documents may be in languages other than English and it may not be possible to assess the quality or completeness of translations. The autopsy evaluation of such cases may be incomplete and sometimes hinders second autopsy interpretation; an example in the reported case was virtual absence of cardiac tissue. As well, in the investigation of deaths that may be due to infection, prior autopsy (which redistributes the microbiome) and embalming (which impedes subsequent cultures) are also impediments. In addition, the conclusions based on the primary examination may be idiosyncratic with omission of significant pathological information. Despite these issues, however, the current case shows the usefulness of a second autopsy and that embalmed tissues may be sufficiently preserved to enable adequate histological evaluation.
In conclusion, the current case demonstrates an uncommon source of septic pulmonary thromboembolism associated with purulent thrombophlebitis of the periprostatic venous plexus with abscess formation associated with chronic urinary catheterization. It emphasizes the need for careful examination of the periprostatic vasculature in all cases of pulmonary thromboembolism, particularly if there is a possibility of underlying sepsis. The value of macroscopic and microscopic re-examination of repatriated previously autopsied and embalmed bodies from overseas locations is also confirmed.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.