
Abstract
Nonthrombotic pulmonary embolism is defined as the partial or total occlusion of the pulmonary circulation by various nonthrombotic agents, such as biological, nonbiological and foreign body material. A case is reported of lethal embolism of fragments of a renal calculus: A 64-year-old woman collapsed and died following laser lithotripsy. At autopsy calculous debris was found in the calyces of the right kidney with widespread microscopic fragments of birefringent foreign material in keeping with renal calculus within the pulmonary arterioles. Death was due to pulmonary calculus embolism complicating lithotripsy of a right renal calculus. Review of other causes of nonthrombotic pulmonary embolism revealed fat, bone marrow, amniotic fluid, trophoblast, tumours, septic material, hydatid cysts, bone, soft tissue/organ parenchyma, gastrointestinal tract contents/bile, gas, and foreign material that was introduced iatrogenically and non-iatrogenically. All of these possibilities should be considered at autopsy in the appropriate setting, with pulmonary microscopy often being essential to establishing the diagnosis.
Introduction
Embolism of material through the venous circulation to the pulmonary vasculature is generally caused by thrombotic material arising from the deep veins of the legs. Underlying mechanisms involve alterations to blood flow, blood components and vessel wall integrity with common risk factors including local factors such as limb immobilisation, and general factors, such as malignancy, obesity and recent surgery.1–3
Pulmonary thromboembolism is a major health issue with approximately 10 million cases occurring globally per year, representing the third leading cause of cardiovascular death after acute myocardial infarction and stroke.4–6 Much less commonly, however, other material may embolise to the lungs with similar lethal effects. Nonthrombotic pulmonary embolism has been defined as the partial or total occlusion of the pulmonary circulation by various biological, nonbiological and foreign body materials.7,8 Large emboli may occlude the pulmonary outflow tract and arteries resulting in rapidly lethal right ventricular decompensation, while smaller emboli may reach peripheral vessels and over time cause pulmonary hypertension and cor pulmonale. Following a rare case of lethal embolism of fragments of a renal calculus after surgery a review was undertaken of the range and nature of causes of nonthrombotic pulmonary embolism.
Case report
A 64-year-old woman with a medical history of type 2 diabetes mellitus, hyperlipidaemia, asthma and a staghorn calculus of the right kidney had undergone a right ureteropyeloscopy, laser lithotripsy, retrograde pyelogram and insertion of a stent for the calculus. Several weeks later she presented with haematuria, dysuria, frequency, urgency and pain and so was admitted for right ureteroscopy, repeat laser lithotripsy and replacement of the ureteric stent. Although the procedure was performed without incident she became hypotensive on completion and then suffered a cardiac arrest which was not responsive to prolonged resuscitation (1.25 h).
At autopsy major findings in the abdominal cavity included calculous debris in the calyces of the right kidney (Figure 1(a) and (b)) with a right ureteric stent. Within the chest cavity the lungs were oedematous and congested with small bilateral serous pleural effusions. The heart weighed 382 g and was structurally normal with cardiac chambers of normal size and mural thickness. The myocardium was normal except for minor fatty infiltration of the anterior wall of the right ventricle. There was no scarring. The foramen ovale was probe patent but guarded. The cardiac valves were normal. The dominant coronary artery circulation was left. The right coronary artery was of relatively small calibre and terminated in a marginal branch. It showed no atheromatous narrowing. The left anterior descending coronary artery had patchy calcification proximally and in its mid-course, but showed no significant luminal narrowing. The left circumflex coronary artery was generally of small calibre (approximately 2 mm internal diameter proximally and 1–1.5 mm internal diameter proximal to the posterior descending branch) but showed no significant luminal narrowing. The aorta exhibited only occasional isolated atheromatous plaques with fully patent major branches.
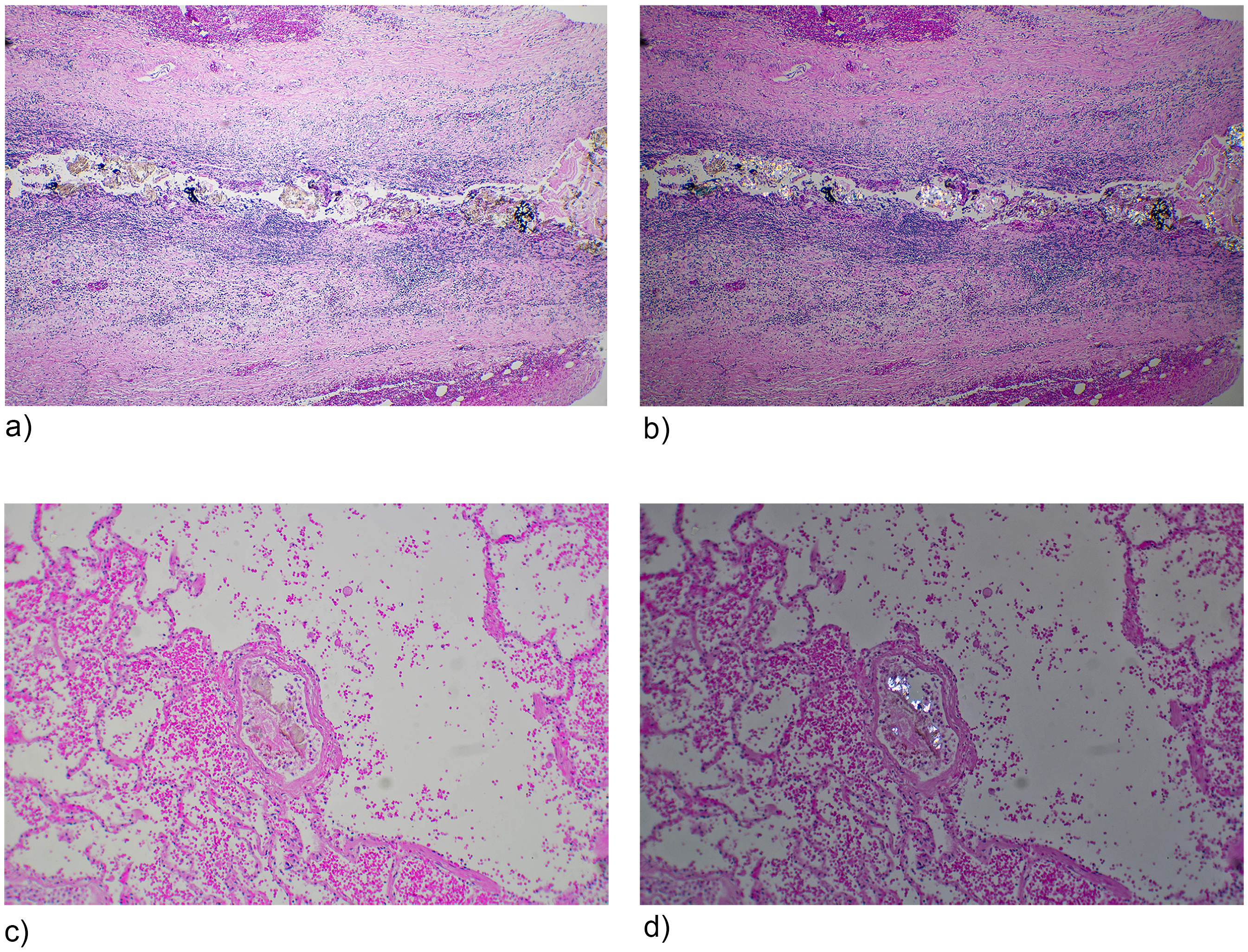
Fragments of renal calculus within a chronically inflamed calyx of the right kidney following laser lithotripsy (a). The material was found to be birefringent on polarised light microscopy (b). Fragments of embolised renal calculus within pulmonary arterioles (c). The material was again found to be birefringent on polarised light microscopy (d). (Haematoxylin and Eosin; H&E 140×).
Histological examination of the myocardium revealed no acute or chronic ischaemic changes. Histology of the lungs showed widespread intra-alveolar haemorrhage with scattered microscopic fragments of intravascular birefringent foreign material in keeping with renal calculus (Figure 1(c) and (d)). Fragments were also seen in very occasional small arterial vessels in sections from the heart and the thyroid gland consistent with paradoxical systemic embolism via the probe patent but guarded foramen ovale. In the heart fragments were observed at only two sites in the anterior wall of right ventricle and in the subendocardium of the anterior wall of the left ventricle. In the thyroid gland a relatively large fragment of birefringent foreign material, similar to that seen in the right kidney and lungs, was observed in a single small arterial vessel.
A haemoperitoneum arising from lacerations of the liver and of the distal small bowel mesentery, with rib and sternal fractures, were attributable to prolonged resuscitation attempts. There was no other evidence of trauma or any other underlying natural disease that could have caused or contributed to death. Toxicological evaluation of blood demonstrated therapeutic levels of prescribed medications with no alcohol. Death was, therefore, due to pulmonary calculus embolism complicating lithotripsy of a right renal calculus.
Discussion
Venous thromboembolism most frequently originates from deep vein thromboses in the lower extremities and often results in lethal embolism to the pulmonary circulation. The incidence varies, with an age-adjusted mortality rate of 1.73 per 100,000 population in Australia, 3.8 per 100,000 population in England and 4.2 per 100,000 population in the United States.9,10 This contrasts with lower rates in Asian countries, although there have been recent increases. 11
In contrast, nonthrombotic pulmonary embolism is much less common. 12 In the present case this involved embolised fragments of renal calculus following laser lithotripsy; there are two similar case reports in the literature.13,14
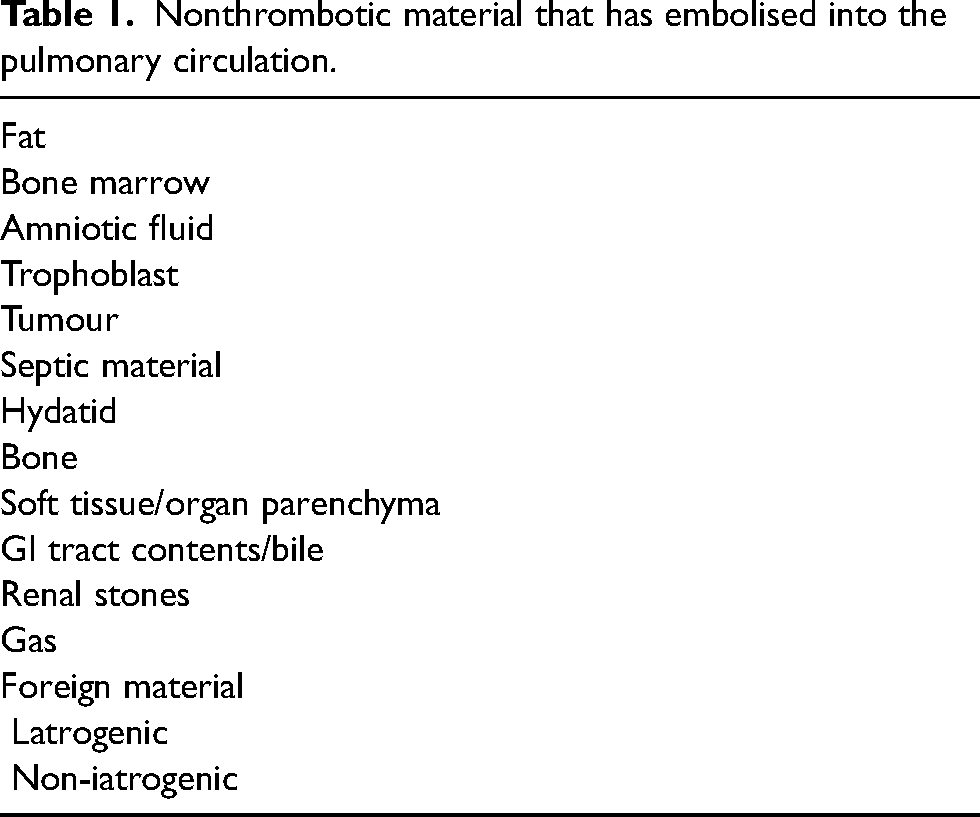
A wide range of other material may also cause nonthrombotic pulmonary embolism (Table 1). For example, focal fat and bone marrow emboli are not infrequently seen at autopsy, particularly after prolonged attempts at resuscitation. Fat embolism was first reported in 1861 and may occur after long bone fractures being found in 1–20% of trauma patients.12,15 Other causes of fat embolism are blunt force soft tissue injuries such as seat belt compression of the abdomen in a high-speed vehicle accident, pancreatitis, burns, suction lipectomy, renal transplantation, decompression illness, intra-osseous infusions, bone marrow harvesting, haemoglobinopathies, blood transfusion, osteomyelitis, diabetes mellitus, neoplasms, severe infections and orthopaedic surgery. 16 It has also occurred after accidental or deliberate injection of vegetable oils, and acupuncture.12,15,17,18 The clinical presentation is typically of respiratory distress (dyspnoea and hypoxaemia), neurological manifestations (confusion, agitation, delirium, stupor, hemiplegia, blindness and coma), and a petechial rash. 19 Bone marrow embolism has been reported in up to 6% of individuals who have suffered trauma, 20 but may also be associated with non-traumatic aetiologies involving malignancy, disseminated intravascular coagulation and sepsis. 21
Nonthrombotic material that has embolised into the pulmonary circulation.
Amniotic fluid embolism most often occurs in the immediate postpartum period and is associated with a high mortality rate. Risk factors include caesarean section, placental pathology and a high maternal age. 12 Amniotic fluid contains a mixture of fetal urine, skin, lanugo with mucin, maternal extracellular fluid and sometimes meconium with fetal squamous cells being detected in maternal pulmonary arterioles. 22 The precise cause of death in amniotic fluid embolism has been debated with immunological reaction to the embolised material now being favoured over mechanical vascular obstruction. 12 Occasionally embolisation of trophoblastic tissue may occur associated with an exaggerated placental site reaction or a hydatidiform mole.22–24
Tumour embolism most often arises from carcinomas of the breast, prostate, stomach, liver and breast, in addition to choriocarcinoma.25,26 Less commonly other tumours such as adrenocortical carcinoma may cause lethal pulmonary saddle embolism. 27 Tumours may be found within the pulmonary vasculature either by true embolism, or from tumour growth into the pulmonary arteries or from local growth within the lungs. 28 There is variability with age in the type of tumour that embolises with Wilms tumour being more common in the young due to its angioinvasive properties. 29 Macroscopically detectable tumour embolism is associated with renal cell, hepatocellular and breast carcinomas and certain sarcomas, while microscopic emboli characterise pancreatic, hepatocellular and gastric carcinomas and choriocarcinoma. 12
Infectious agents causing nonthrombotic pulmonary embolism range from bacteria to hydatid disease. Infective endocarditis arises when bacteria colonise valves causing irregular excrescences or vegetations. Their development is associated with intravenous drug use, indwelling vascular lines and prosthetic heart valves. 30 Pulmonary embolism of such material arises from right-sided endocarditis as well as infected central venous catheters or pacemaker leads and may involve fungal organisms such as Candida, Mucor and Aspergillus. 12 As the embolised material is not large, complications include pulmonary abscess formation, sometimes with lethal arteriobronchial fistulas, rather than mechanical pulmonary artery outflow obstruction. 31 Hydatid disease due to the tapeworm Echinococcos granulosus may cause death by a variety of factors, one of which is from pulmonary embolisation following rupture of an intracardiac cyst. 32
Rarely fragments of bone may embolise to the lung after hip surgery or trauma, particularly if there is underlying osteomyelitis. It has also been reported following penetrating cranial gunshot wounds and after bone marrow transplantation.20,33 Tissues such as cartilage, skin and skeletal muscle may also travel to the pulmonary vasculature after trauma. Skin embolism may be a complication of percutaneous needle puncture.28,34 Cerebral tissue embolism occurs in two situations involving trauma: penetrating and blunt force head injury, and in neonates after difficult vaginal deliveries.35,36 Similarly, fragments of liver may embolise if there has been a crushing injury, most often associated with vehicular trauma. 35
Both faecal and food material have been rarely reported in pulmonary and systemic emboli associated with rectal surgery, diverticular disease and oesophageal/intestinal ulceration. 37 Trauma to the liver, including surgery, has caused lethal bile pulmonary embolism. 38
Entry of gas into the venous circulation may have a traumatic or iatrogenic aetiology. In forensic situations, the most common causes would be incision or laceration of major veins by either sharp or blunt force trauma such as stabbing or crush injuries. It may also occur following gunshot trauma. 39 Iatrogenic causes of venous air/gas embolism involve a number of procedures ranging from accidents with haemodialysis and central venous catheters to laparoscopic and endoscopic procedures that use carbon dioxide, air or argon. 40 The incidence of air embolism related to surgery has ranged from 7% to as high as 69%. 12 Acute cor pulmonale has resulted from rapid injection of 50 m/s of air or more, with the lethal volume estimated to range from 100 to 500 m/s.15,41
Embolised foreign material may be associated with medical procedures or it may be non-iatrogenic. Examples of the former are catheter emboli that arise when catheters break or when the ends are sheared off by the tip of an introducing needle. This may also involve pacemaker leads, stents, coils, guide wires and ventriculoatrial shunts. Radioactive seeds may also enter the vaculature and embolise.28,41 Fragments of silicone have migrated from intravenous fluid tubing 42 and bone cement (polymethyl-methacrylate) used during orthopaedic procedures such as vertebroplasty and kyphoplasty may embolise to the lungs. 43 Similar embolisation has been reported with iodinated oils and cyanoacrylate that are used to treat arteriovenous malformations and varices.28,44
The injection of illicit drugs is associated with non-iatrogenic foreign material embolisation to the lungs with granuloma formation and the typical histological finding of birefringent material on polarising.45,46 This is particularly so when tablets have been ground up and injected. Materials that may embolise involve fillers, binders and filters and include talc, cellulose, starch and cotton. 12 These may disseminate systemically if there are right to left shunts in the heart. 47 Titanium dioxide from the coating of tables has been visualised macroscopically in some tissues at autopsy. 46
Liquid silicone has been used for illegal cosmetic procedures involving breast, scrotal and other soft tissue augmentation. In addition to shifting under the influence of gravity it also has a propensity to embolise, sometimes with lethal results.48,49 A number of materials have also been deliberately injected in suicide attempts ranging from mercury to hair conditioner.50–52 Rarely low-velocity bullets may enter blood vessels and then embolise. 28
Thus, a wide range of solid, liquid and gaseous materials may embolise to the lungs that should be considered at autopsy. The material may be endogenous such as fat, amniotic fluid and certain tumours, or it may be introduced either as part of a medical procedure, or during body modification or illicit drug injection. Lung microscopy is often essential in establishing the diagnosis.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.