
Abstract
Cultural competence among healthcare professionals and providers is pivotal to providing effective, safe, and quality services. This paper considers the feasibility of using a tool to measure cultural competence within forensic mental health services, adapted from the Cultural Competence and Linguistic Competence Policy Assessment (CLCPA) developed in the United States (US). The adapted tool was piloted at a secure forensic unit in England; this consisted of a two-phase approach to data collection comparing the results from an initial assessment (time 1, n = 50), with those of a follow-up assessment conducted three years later (time 2, n = 100). The aim was to assess the practicability of using the tool to measure perceptions of cultural competence among 150 staff members, as part of a wider quality assurance and improvement process. The results indicate that the tool has utility in measuring perceptions of cultural competence and that the information gathered can be used to plan service improvements. Yet, it is recommended that the tool is modified at site-level as part of a collaborative exercise with staff and patients and according to service need prior to implementation.
Introduction
The term ‘culture’ can be understood as a set of beliefs, values, and attitudes shared and conserved by a population of people. The group's collective shared traditions, customs, language, and norms guide behavior. The organization of these principles contributes to the existence and wellbeing of its members and offers meaning and purpose throughout life. 1 Within medicine, culture shapes the way in which health conditions are framed in meaning and response, including the delivery of appropriate and equitable care.2,3 Achieving health equity in healthcare delivery requires recognition and engagement in working towards cultural competence and cultural safety at individual, organization and system level. 2
Cultural competence refers to the capacity of an individual and an organization to function effectively in relation to the cultural factors and needs presented by patients and their communities.4,5 By understanding how an individual's identity, their interpretation of illness, and their moral values factor into their life experiences, healthcare professionals can be better equipped in the provision of culturally competent and holistic care. 6 Cultural competence is a concept that incorporates behaviors, attitudes and policies that can collectively influence how effectively health care professionals work in cross cultural scenarios.4,7,8 It is the conscious application of knowledge of different cultures to clinical environments and the adaptation of service delivery to meet these culturally unique needs that improves treatment outcomes for different patient populations.9,10
Several strategies are commonly deployed for improving cultural understanding at individual and organizational levels, such as improving knowledge and skills through training and cultural awareness initiatives, incorporating culture-specific attitudes and values, and co-production activities with patients and communities. 11 However, challenges exist in knowing what works in improving health outcomes across such diverse population groups. 5 One of the key barriers to constructive patient-practitioner relations is a lack of understanding and appreciation for patients’ health beliefs, medical practices and use of alternative medicine. Evidence suggests that educational interventions are effective in improving knowledge, attitudes, and skills of cultural competence among healthcare professionals, reducing stereotyping and discrimination based on ethnic, racial, cultural, or social status, and its impact on clinical decision-making.7,12,13 Promoting culturally competent approaches fosters effective communication, mutual understanding, and inclusivity. 14 An incorporation of these considerations positively impacts on the adherence of patients to treatment plans and patient satisfaction.11,15 Other measures focused on addressing racial and ethnic disparities in healthcare systems include recruiting professionals from minority groups to reflect the cultural diversity within the served community, providing translation services and information in the languages used by the population, and demonstrating a culturally competent approach in policymaking. 9
However, cultural competence is limited in that it focuses primarily on an adaptation of services to meet these culturally unique needs and largely neglects the influence of power relationships on the delivery of quality care. 2 This is particularly important within forensic mental health services where the liberty of the patient is constrained, and therapeutic principles are balanced with the management of perceived risk and maintaining safety and security. Although rooted in evidence-based practice, it cannot be ignored that the management of patients within secure settings is also influenced by concepts of risk and social values and beliefs. 16
Conversely, the term ‘cultural safety’ focuses on the social determinants of health and addresses this notion of power between providers and patients. It questions the impact of healthcare professionals’ and providers’ own culture on clinical interactions and how this may contribute to a lower quality of care provided.2,17 These biases may be conscious or unconscious and are often experienced as poor communication, perceived disrespectful actions, and uncollaborative care planning and decision-making. 17 For patients in secure settings, such as those from minority populations, this may translate into a higher use of restrictive practices. Thus, recognizing and tackling power differentials can lead to reduced health inequities and more appropriate care and treatment for all patients. 18 However, cultural competence must first be accomplished before a service can achieve cultural safety. This paper offers a means to assess cultural competence and support individuals and services in the development of culturally competent and culturally safe services.
Cultural Competence and Linguistic Competence Policy Assessment (CLCPA)
Published in the United States (US), the purpose of the Cultural Competence and Linguistic Competence Policy Assessment was to support community health centres to improve access to healthcare, enhance the quality of services within culturally diverse and underserved communities, and promote cultural and linguistic competence. 19 The framework assumes that cultural competence is achieved as part of a developmental process at both the individual and organizational level, and that individuals can enhance their cultural awareness, knowledge, and skills with the right support. They also recognize the often-overlooked cultural expertise within organizations or networks of professionals that could be used to support organizational growth and development. In the United States (US), cultural competence has become a key feature in standards and accreditation processes assessing the quality of healthcare provision, focusing largely on effective communication, cultural competence and patient and family-centred care. 5 Within the UK, however, a universal tool and framework for measuring quality in relation to cultural competence does not exist. Although this tool was first introduced nearly 20 years ago, it still has the potential to support service improvements in this area.
The principal aim of this paper is to introduce and assess the feasibility of using an adapted tool to examine cultural competence among clinical and non-clinical staff members within forensic mental health services, as part of a wider quality assurance and improvement process. This paper offers insights into measuring cultural competence within forensic mental health services and identifies the potential benefits for organizations and patients.
Method
Design
A naturalistic design was implemented. Cross-sectional data was recorded using a quantitative survey approach. The key grouping independent variables were sample (time 1 versus time 2) and staff group (clinical versus non-clinical). Additional predictors included age, gender, ethnicity, religion, and languages other than English spoken (LOTES). The total and sub-scale scores of the survey were utilized as dependent variables.
Sample
One hundred and fifty respondents took part in this study. The sample consisted of permanent clinical and non-clinical staff members from across six wards at a secure unit. Fifty participants took part in the first phase of the study in 2013, and 100 participants were involved in the second phase in 2016. Non-clinical staff members were included in the sample for two reasons: firstly, due to the substantial role they play in a patient's experience of being an inpatient in a secure service; and secondly, the involvement of clinical and non-clinical staff members offers a more holistic picture when considering feasibility.
An opportunistic sampling method was used for selection of staff members using a combination of planned and random approaches. This method enabled the researchers to adopt a flexible approach in gathering data and was deemed more suitable to the clinical environment and to minimize sampling bias. 20 To aid in recruiting the first pool of participants, a list generated by the human resources department at the hospital was used. The staff members were then contacted electronically via an email inviting them to partake in the study. The email briefly introduced the project and included a participant information sheet and proposed some dates and times when the subsequent questionnaire-based interviews could take place. To promote the project around the hospital site, posters were displayed at various locations and a leaflet was circulated within the hospital grounds.
In the second stage of recruitment, researchers actively went to the six wards to consult the ward manager to directly approach staff members with an invitation to take part in the study. After a brief consultation and agreement from the members of staff, the researcher could start collecting data (details in the ethical considerations and procedure sections of this paper). Time with the researchers was protected, which meant staff could go off the ward to participate in a comfortable and quiet place. Anonymized responses meant an overlap of participation between samples could not be identified.
Measures
Cultural Competency Policy Assessment (CCPA)
The first part of the questionnaire investigated how a range of variables impact the acquisition of cultural competence by staff members, including: clinical status, age, ethnicity, languages spoken and duration of employment at the hospital. The main tool consisted of a questionnaire adapted from the Cultural and Linguistic Competency Policy Assessment developed in 1999 and revised by the National Centre for Cultural Competence. 19 Modifications were required for application in the UK. These centered on grammar, vocabulary, and the cultural groups referenced. Additionally, the questions pertaining to linguistic competence were excluded to focus solely on the cultural competence aspect, resulting in a 47 item Likert-type scaled questionnaire. It was thus re-named the Cultural Competency Policy Assessment (CCPA). The CCPA tool consisted of four dimensions: values, policy, structure, and practice. Within these dimensions, it assessed seven subscales: Knowledge of Diverse Communities (KDC), Organizational Philosophy (OP), Personal Involvement in Diverse Communities (PIDC), Resources and Linkages (RL), Human Resources (HR), Clinical Practice (CP), and Engagement of Diverse Communities (EDC). A brief description of each subscale preceded the questions pertaining to that section.
Demographics
The last section of the questionnaire collated demographic information such as: age, gender, ethnicity, religion, professional workshop attendance, and living in diverse communities, as it aimed to assess the level of diversity in staff members at the unit.
Procedure
The study was carried out in 2013 and 2016 at a secure mental health unit in England. The first phase consisted of a self-evaluation by clinical and non-clinical staff members of current practice in relation to cultural competence. The CCPA questionnaires were administered in offices or ward meeting rooms onsite. Participants were briefed on the aims of the study and ethical guidelines were followed (see ethics section). Each respondent was then presented with a paper copy of the questionnaire and encouraged to complete one response for every question. A time frame of 25–30 minutes for completion was advised. A member of the research team was available to answer any questions. After time 1, the results were fed back to the organization as part of the audit process. The audit cycle was completed three years later with a re-administration of the same audit tool to staff working in the unit.
Ethical considerations
The hospital's clinical governance committee and King's College Research Ethics Management Application System approved the service evaluation. Those who agreed to participate provided written informed consent and were briefed on the details of the project as per the participant information sheet. Deception was not an issue, as the aims of the research were not disguised and all participants were offered the right to withdraw from the study. Anonymization of participants’ identities and confidentiality of their data was exercised.
Data analysis
An a priori power analysis using G*Power 3.1 21 indicated that a total sample size of 102 would be sufficient to detect a medium effect size (d = .5) with 80% power and an alpha of .05, to test the difference between two independent means. Thus, our proposed sample size of N = 150 was more than adequate for detecting differences between time 1 and time 2 samples regarding test outcome scores. An additional power analysis revealed a total sample size of 55, with 80% power and an alpha of .05, would be appropriate to detect a medium effect size (f2 = .15) to test the relationships between the demographic variables and the CCPA's scores. The sample sizes were adequate or close to adequate for this analysis (time 1 n = 50, time 2 n = 100). The internal reliability of the scale was very good as Cronbach's alpha value was 0.978, confirming this tool had strong internal consistency. Participant characteristics for both samples are reported in table 1. A series of independent sample t-tests were conducted to compare the differences in average scale scores between time 1 and time 2 samples. A series of multiple linear regression analyses were conducted whereby total CCPA scores were regressed onto the model which comprised of six key predictors to include age, gender, LOTES, ethnicity, religion and clinical vs. non-clinical staff. These regressions were analyzed separately across time 1 and time 2 samples for all subscales. Finally, several paired t-tests were conducted to see if there was a significant difference in cultural competence between time 1 and time 2 for clinical staff.
Baseline characteristics across samples.
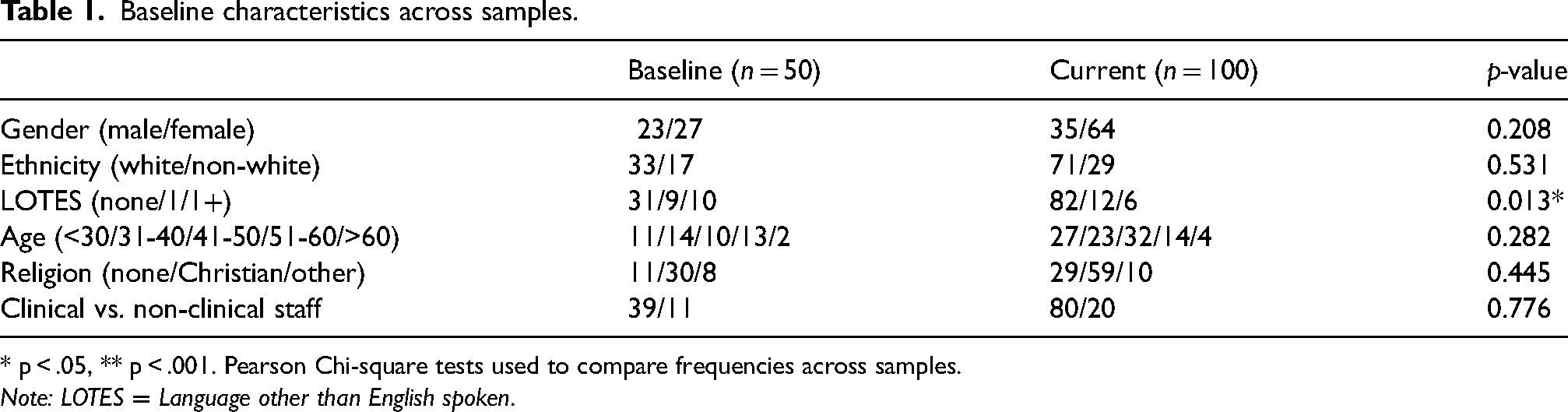
* p < .05, ** p < .001. Pearson Chi-square tests used to compare frequencies across samples.
Note: LOTES = Language other than English spoken.
The range of possible values and answer scores were described as follows: -1: ‘Unanswered’ 0: ‘Omitted’ (relevant to question 47_6 in the time 1 set and question 33_7 in the current set)/ ‘I do not know’ 1: ‘Not at all’/ ‘None’/ ‘No’/ ‘No policy’/ ‘Never’ 2: ‘Hardly’/ ‘Some’/ ‘Yes’/ ‘Informal policy’/ ‘Sometimes’ (questions 13 to 18 and 21 to 31) 3: ‘Fairly often’/ ‘Fairly well’/ ‘Quite a few’/ ‘Developing policy’/ ‘Sometimes’ (questions 40 to 44 and 46) 4: ‘Very often’/ ‘Very well’/ ‘Regularly’/ ‘Many’/ ‘Formal policy’
Results
A total of 150 respondents took part in this study. All participants were clinical and non-clinical staff members of a secure forensic unit in the UK spread across six wards. Fifty respondents took part in the first phase of the study and 100 in the second phase conducted three years later. There were 59 males and 91 females involved in the study. Thirty-eight participants were under the age of 30, 106 were between the ages of 31 and 60, and six were aged over 60. It was noted that 104 participants were white Caucasian and the rest originated from other ethnicities. 89 subjects identified as Christian, 40 identified as having no religion, and 18 identified as either Buddhist, Hindu, Jewish, Muslim or another religion.
These time 1 characteristics are illustrated in Table 1, which indicates that there are no significant differences in demographic features except Languages other than English spoken (LOTES), where participants in the time 2 sample spoke fewer languages other than English.
Difference in the average scale scores between time 1 and time 2 samples across all domains
It was found that the time 2 sample had significantly greater Resources and Linkage Policy scores (M = 1.67, SD = 1.59) compared to the time 1 sample (M = .97, SD =1.30), (t (147) = 2.66, p = .01, 95% CI [-1.21, −.18], d = .48).
Regarding Human Resources Policy, the time 2 sample had significantly greater scores (M = 1.97, SD = 1.33) compared to time 1 sample (M = 1.30, SD =1.21), (t (147) = 3.07, p = .00, 95% CI [-1.11, −.23], d = .53). For Clinical Practice Policy the time 2 sample had significantly greater scores (M = 1.94, SD = 1.43) compared to the time 1 sample (M = 1.09, SD =1.13), (t (147) = 3.65, p = .00, 95% CI [-1.31, −.40], d = .66).
Similarly, t-tests carried out for Engagement in Diverse Communities subscale indicated that the time 2 sample had significantly greater scores (M = 2.63, SD = .53) compared to time 1 sample (M = 2.33, SD = .58), (t (148) = 3.14, p = .00, 95% CI [−.50, −.11], d = .55). For Engagement in Diverse Communities Policy the time 2 sample had significantly greater scores (M = 1.87, SD = 1.51) compared to the time 1 sample (M = 1.28, SD = .83), Policy (t (142) = 3.99, p = .00, 95% CI [-1.55, −.52], d = .74).
T-tests found that the time 2 sample had significantly greater Cultural Competence Policy scores (M = 1.91, SD = 1.28) compared to the time 1 sample (M = 1.25, SD = .94), (t (148) = 3.23, p = .00, 95% CI [-1.06, −.26], d = .59).
The time 2 sample had a significantly greater Total CCPA mean scores (M = 2.49, SD = .48) compared to the time 1 sample (M = 2.32, SD = .45), (t (148) = 2.14, p = .04, 95% CI [−.33, −.01], d = .37).
The results of the assessment are presented in Figure 1, all other comparisons were found to be non-significant.
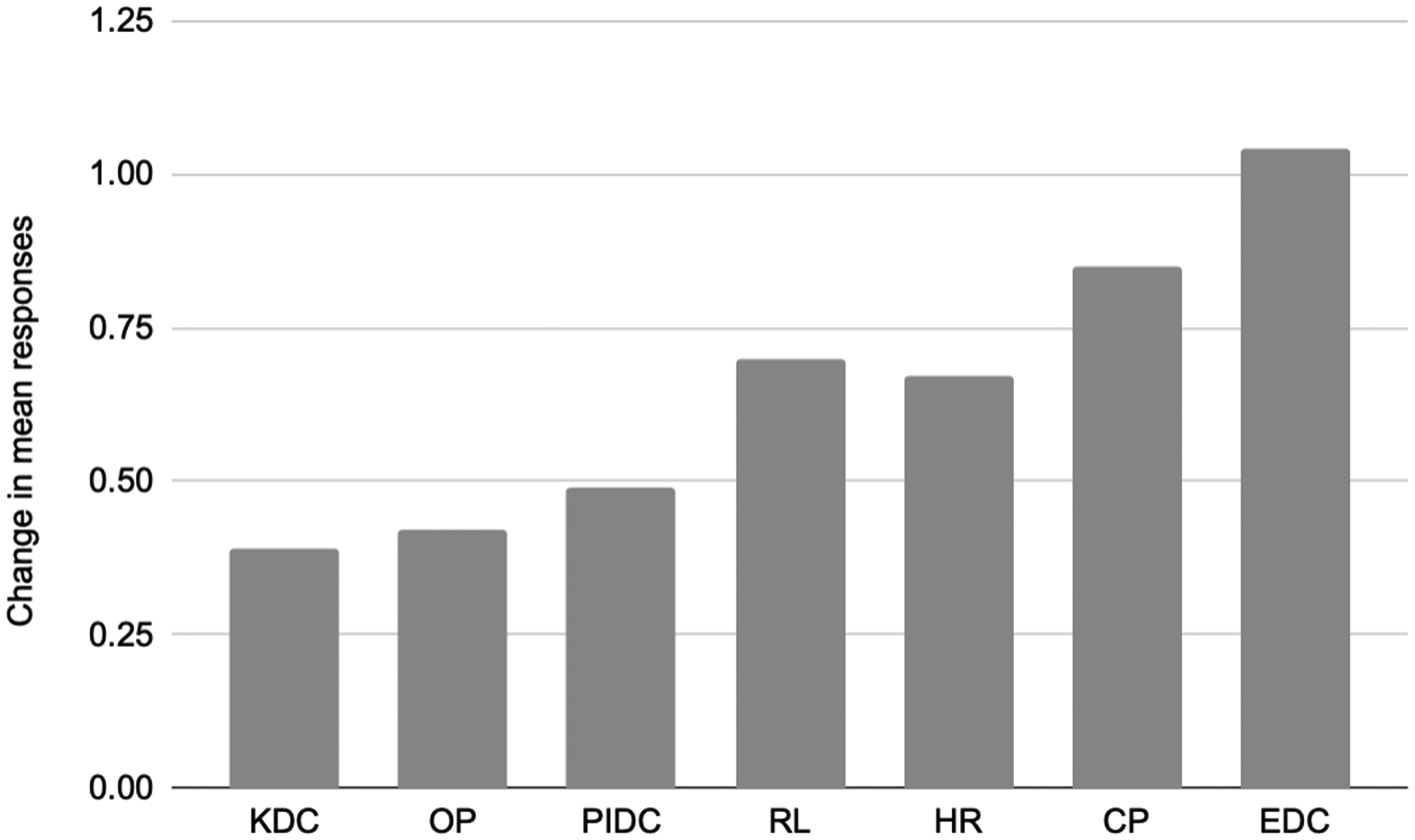
Change in mean responses between baseline and the current data within all seven domains. Note: Change scores were calculated by subtracting mean responses at baseline from current. A positive score indicates a larger mean for the current sample. Knowledge of Diverse Communities (KDC); Organisational Philosophy (OP); Personal involvement in Diverse Communities (PIDC); Resource and Linkages (RL); Human Resources (HR); Engagement of Diverse Community (EDC).
Regression analysis
The strongest predictor of CCPA appeared to be age. Within the time 1 sample, it was established that age significantly predicted mean scores for Clinical Practice Policy answers; the younger the individual, the more competence they had in this component. Gender significantly predicted mean scores for Organizational Policy answers which suggests that males had greater competence.
Staff role significantly predicted total mean scores for Organizational Philosophy answers, Personal Involvement in Diverse Communities Policy answers, Human Resources Policy answers, Clinical Practice Policy answers and Cultural Competence Policy answers. Findings suggest non-clinical staff had greater competence for all these domains. Conversely, Ethnicity and LOTES did not predict the total or subscales.
Within the time 2, LOTES significantly predicted mean scores for Personal Involvement in Diverse Communities with dimension policy answers which suggests that fewer languages spoken meant more competence. Age significantly predicted mean scores for Knowledge of Diverse Communities Policy answers, Personal Involvement in Diverse Communities Policy answers, Clinical Practice Policy answers, and Cultural Competence Policy answers. Therefore, this suggests that the older the individual, the more competence they had in all these domains. There were no significant predictions for gender, ethnicity, or staff role.
Further t-tests were conducted to see if there was a significant improvement in cultural competence from time 1 to time 2 for clinical staff. These significant improvements in cultural competence for clinical staff across several domains are illustrated in Table 2.
Significant improvements in cultural competence for clinical staff.

Discussion
Cultural competency in mental healthcare is an essential aspect of service delivery to ensure culturally unique needs are met and treatment outcomes for different patient populations are enhanced. Internationally, quality standards and measurement tools exist to support service developments in this area. Despite this, a universal tool to assess cultural competence within these settings is not currently available in the UK.
The study represents a first attempt to assess cultural competence in a secure mental health unit in the UK by surveying staff members’ perceptions of cultural competence. An existing tool utilized in the US was modified to evaluate cultural competence and the present study carries out an exploration of the feasibility of this tool for use within a mental healthcare organization. However, there were some methodological weaknesses.
Notably, the language used in the tool may have limited accessibility and comprehension by those completing it. The tool originated from the US and some components do not translate easily into how the workforce is structured in the UK. Similarly, there is an assumption that non-clinical staff would have an awareness of clinical terminology and thus the relevance to their roles may have impacted the answers provided. It is important to note, however, that the label ‘non-clinical staff’ encompasses a broad category and does not allow for greater exploration as to the roles and responsibilities undertaken by those completing the tool. Further shortcomings were apparent in the length of time required to complete the tool and the supporting administration necessary for data collection.
Within the scope of this project, the application of the tool was not intended as an intervention for improvement as such, but a means of assessing cultural competence. By virtue of a service engaging in this process, it can be suggested that the exercise contributes in some way to an improvement as part of an audit cycle. However, it cannot be concluded that the tool is responsible for improving cultural competence. The tool simply provides a method for capturing and monitoring performance.
Despite these shortcomings, this study illustrated the feasibility of using this tool to measure perceptions of cultural competence within an organization. The findings suggest that cultural competence increased between the two time points. The results obtained are indicative of strengths and weaknesses within this organization (with reference to figure 1). This fits in with points of improvement and deterioration and suggests where the organization may have been receptive to feedback in between audits. Findings indicate a higher level of improvement for the clinical staff over the non-clinical staff, with all domains indicating significant results. Upon considering the factors that underlie the observed improvement, it could be argued that clinical staff were more receptive to the tool due it having greater applicability to their roles. The results pertaining to clinical staff improvements further justifies the use of the tool. The strongest domain was Engagement of Diverse Communities; this is indicated by the largest increase in mean scores for this domain and can be observed with reference to figure 1. Regarding the results obtained from the MLR analysis, the strongest predictor appeared to be age. As older individuals in the time 2 had more competence for several domains of the CCPA, this would suggest that younger staff could be targeted more for improved diversity awareness. The anonymous completion of the questionnaire was a positive aspect, as this limits the likelihood of bias. Lastly, the tool is adaptable and can be customized to local healthcare settings.
For future studies, the design could be improved by collaborating with staff members and service users in the development of the tool. Participation and coproduction would enhance its design, making it more universally comprehensible and applicable to the local population. 22 Similarly, a tool to measure patients’ experiences of cultural competence among staff members and within the organization would be an interesting addition to support service developments in this area. Due to the nature of the topic, a further area for consideration is the possibility of introducing a qualitative element to the study to encompass the experiences of those completing the tool and garnering a richer understanding of cultural competence. 23 Other areas for future examination may include the impact of ethnicity, age, or gender in relation to perceptions of cultural competence, and a re-categorization of job role from clinical and non-clinical to introduce greater insight of cultural competence across different groups.
As documented in current evidence, a shift in approach is required to achieve health equity using the combined principles of cultural competence and cultural safety. 2 Ideally future versions of the tool should be prepared to address power structures on a systemic, organizational and individual level. 17 Nevertheless, this tool provides a useful starting point as a self-review exercise in understanding cultural competence. It assesses the extent to which cultural competence principles are present and fosters a commitment to action planning in identified areas. 2 Most importantly, the tool cultivates awareness of cultural competence across several domains and the present study illustrates how the tool can work to provide interesting findings that organizations can take forward. This paper highlights that, with staff and patient collaboration, this tool can be further adapted to better capture perceptions of cultural competence, from both those providing and receiving the services, and support services in their journey to achieving culturally safe care.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.