
Abstract
Child abuse, including physical, sexual, or emotional violence or neglect, is a global problem with serious and long-term consequences for children. Even though child abuse is prohibited in Denmark, the estimated number of physically and sexually abused children is relatively high, whereas the annual number of forensically examined children is low. We present the Danish practice and legal foundation for the clinical forensic medical examination (hereinafter referred to as “forensic examination”) in suspected child abuse cases. Forensically documented findings may contribute to the police investigation and legal assessment of child abuse cases, safeguarding the rule of law for both children and suspected perpetrators. The forensic examinations are accredited according to international and European standards, and the Department of Forensic Medicine is regularly assessed for the fulfillment of accreditation. Accreditation, delimitations from medical treatment and police employment, and the fact that the department refers to the University of Copenhagen ensure impartiality from the police and the judicial system. A cross-sectoral intervention project has significantly increased the annual number of forensically examined children at the Danish Children's Advocacy Center (CAC) in Copenhagen, which supports children's legal rights and holds research potential due to systematic and continuous data collection.
Keywords
Introduction
The estimated global prevalence of children aged 2–17 years having experienced past-year physical, sexual, or emotional violence or neglect is approximately 1 billion,1,2 and a significant proportion are related to physical and/or psychological discipline at home.3–5 In Denmark, corporal and disciplinary punishment of children is banned by legislation. 6 Despite this, a national survey from 2022 revealed that 22% of children in 8th grade (13–14 years) had experienced violence during the past year. 7 Similar prevalences are seen in comparable countries, such as Sweden (13%) 8 and Norway (19%). 9
In contrast, the number of cases processed in the Danish Children's Advocacy Centers (CACs), in 2022, was 1754, which corresponds to approximately 0.15% of all children in Denmark 10 ; 74% concerned physical abuse and 28% sexual abuse. The police conducted a video-recorded investigative interview (hereinafter referred to as “video-recorded interview”) in 65% of the cases (1140 children), whereas a clinical forensic medical examination (hereinafter referred to as “forensic examination”) was conducted in only 5% of the cases (88 children). 11 In the same year, the Department of Forensic Medicine in Copenhagen conducted more than 200 examinations of children outside the CACs.
Child abuse and neglect constitute major health and safety problems for children worldwide and may have lifelong impacts on families, communities, and nations. The list of documented long-term consequences for children is extensive and includes behavioral, physical, and mental health problems.2,4,5
Worldwide, cases of suspected child abuse are investigated in different settings and with different approaches, not least due to national legislation and infrastructure. In addition, several studies have reported variability in the medical assessment of children suspected of being subjects of abuse.12–14 This variation may challenge the consistency of such assessments.
In a previous article, we described forensic examinations of adult victims and suspected perpetrators of perilous crimes. 15 This paper aims to describe the current Danish practice regarding forensic examinations of children as police-reported victims of abuse, exemplified by the setup in Eastern Denmark, including the Copenhagen area, thereby catalyzing a discussion on the most appropriate setup to ensure the highest quality of rule of law for the victims, their guardians, and suspected perpetrators. Moreover, we will present an intervention to increase the number of CACs-anchored forensic examinations of children in cases of suspected physical abuse.
Forensic examination of children in eastern Denmark
Which children are forensically examined?
Children of all ages (0–17 years) may be forensically examined, most often at the request of the police. Most cases concern physical abuse, including abusive head trauma, and sexual abuse; less frequent are cases of neglect and medical child abuse.
Who conducts forensic examinations of children?
Forensic examinations are conducted by medical doctors who are either board certified, in training, or certified medical doctors employed in a forensic department. All examinations and forensic reports are supervised by a senior board-certified forensic doctor or a chief/deputy chief forensic pathologist, with the latter being responsible for the overall quality of forensic assessments and reports.
The board certification takes four years and ensures competence in the practice of autopsies, including postmortem imaging and histology, and clinical forensic medicine, including examinations of victims and suspected perpetrators of perilous crimes.15,16 With this approach, competence in documenting and assessing the entire panorama of injuries is achieved.
Hereinafter, the examiner will be referred to as a “forensic doctor.”
Why are children forensically examined?
By Danish law, only medical doctors conduct physical examinations of the body as part of a police investigation. 17 The standard forensic examination consists of a thorough external examination of the body and securing biological and technical evidence, which is handed over to specialized departments for analysis. The police subsequently receive a written forensic report, which includes an assessment of the specific types of injuries observed, the manner and time of the injuries’ origin, including whether there are any injuries suggestive of abuse, and their severity. 15 If the Prosecution Service decides to bring the case to court, the forensic report may serve as technical evidence. The court might also summon the forensic doctor as an expert witness to explain the procedure of the forensic examination and elaborate on the findings and assessments.18–20
Without examining the body, the opportunity to document injuries (or the absence of injuries) and secure evidence is missed. Without this evidence, the police and judicial system may have difficulty assessing whether the child has been exposed to abuse.
Specific rights for Danish children
In Denmark, children's legal rights are safeguarded by laws and regulations to ensure the child's well-being and protection from abuse. Healthcare providers, teachers, and other professionals working with children have strict obligations to notify the social authorities if they suspect child abuse or identify serious concerns about a child's well-being. However, all citizens must notify the social authorities if they become aware that a child is being subjected to abuse. 21 The legislation regarding the protection of children is described in the Promulgations of the Act on Social Services, 22 the Parental Responsibility Act, 23 the Danish Penal Code, 24 and since January 1, 2024, the Law of the Child, 25 whose purpose is stated as: “Help and support … must be provided based on the perspective of the child or young person, resources and needs in order to ensure the best interests of the child or young person.” 21
When the social authorities receive a notification regarding suspected child abuse, they must investigate the case as soon as possible, most often achieved with a child interview within 24 h of receiving the notification. 25 A social worker is responsible for the interview with the child, which takes place in the presence of a person with whom the child feels safe, such as a teacher. The interview requires no consent from or participation of the child's parents. 25 After the interview, the social authorities may contact the police to seek advice from consultants within a designated assault group regarding whether to formally report a suspicion of child abuse to the police.
If the matter is formally reported, the police decide whether to conduct a video-recorded interview with the child. The police must conduct the video-recorded interview within seven days of receiving a formal report of a suspicion of child abuse. 26 A possible protest from the child's guardians against conducting the video-recorded interview can be overruled by the court.17,26 The video-recorded interviews are conducted in specially designed rooms in the Danish CACs. Besides the specially trained police officer and the child, a companion of the child and/or an interpreter may participate in the interview, which is also attended by the suspect's defense lawyer, the child's legal advocate, and a prosecutor in an adjacent room. 26 The children are informed about their rights regarding witness exemptions and are exhorted to tell the truth. The purpose of the video-recorded interview is to document the child's witness statement early in the process to assess whether the suspicion should be investigated further and to preserve the witness statement to prevent it from being influenced by the family and others later in the process. The recording of the child's witness statement can be used as evidence during the legal hearing; that is, the child does not have to testify in court. During court proceedings, the defense lawyer and/or the child's legal advocate may oppose the use of the video-recorded interview, after which the court will decide whether the circumstances of the case require the video to be used as evidence. 17
Concurrently with criminal proceedings, a holistic child protection assessment, also referred to as a Section 20 Assessment, is performed and should clarify the child's situation and what kind of support and actions are relevant. 25 If it is known or suspected that a child has been subjected to abuse, the social authorities must conduct the Section 20 Assessment at the CAC in its geographical region.25,27
CACs in Denmark
CACs in Denmark were established in 2013, and their purposes are described in the Promulgation of Children's Advocacy Centers, 27 inspired by similar centers in other countries, including Sweden 28 (2005) and Norway (2007). 29 In Europe, the first Barnahus was established in 1998 in Iceland. The Barnahus model refers to a multidisciplinary and interorganizational framework, which promotes a neutral, child-friendly, and safe environment to perform (1) video interviews according to evidence-based protocols ensuring valid testimonies suitable as evidence in court; (2) medical examinations to document forensically important findings and ensure the child's physical well-being and recovery; (3) psychological support, including both short- and long-term therapeutic services; and (4) an assessment of the need for protection of the child and any siblings. 30 The Barnahus model was designed based on the CACs in the United States,31,32 which were founded in 1985, 33 and today, the centers support local and state efforts to coordinate the investigation, treatment, and prosecution of child abuse cases. 34
Despite having the same purpose, the legal and financial structure of the organizations vary between countries. For example, in Norway, the Barnahus are organized under the police, 35 whereas in Denmark, the CACs are organized under a government agency under the Ministry of Social Affairs,36,37 and in the United States, the CACs receive private funding. 38
Where are children forensically examined?
The location of the forensic examination may vary (Figure 1). If the child is hospitalized, the forensic doctor conducts the examination at the hospital. Otherwise, the location of the examination is determined by the case circumstances. In cases of suspected sexual abuse, the examinations are conducted at a pediatric department, the highly specialized Department of Social Pediatrics at Herlev Hospital (0–15 years), 39 or at the Centre for Victims of Sexual Assault (>15 years), which is located in the Gynecological Department in the nearby university hospital, Rigshospitalet.40,41 In cases of suspected physical abuse, the police may request an urgent forensic examination, which takes place at the Department of Forensic Medicine in specially designed examination rooms, ensuring optimal examination conditions, including optimal lighting and necessary equipment. Lastly, some of the CACs in Denmark have an examination room in which forensic doctors conduct forensic examinations. The examinations at the CACs are most often conducted following a police video-recorded interview with the child, and the examinations are planned a couple of days beforehand.
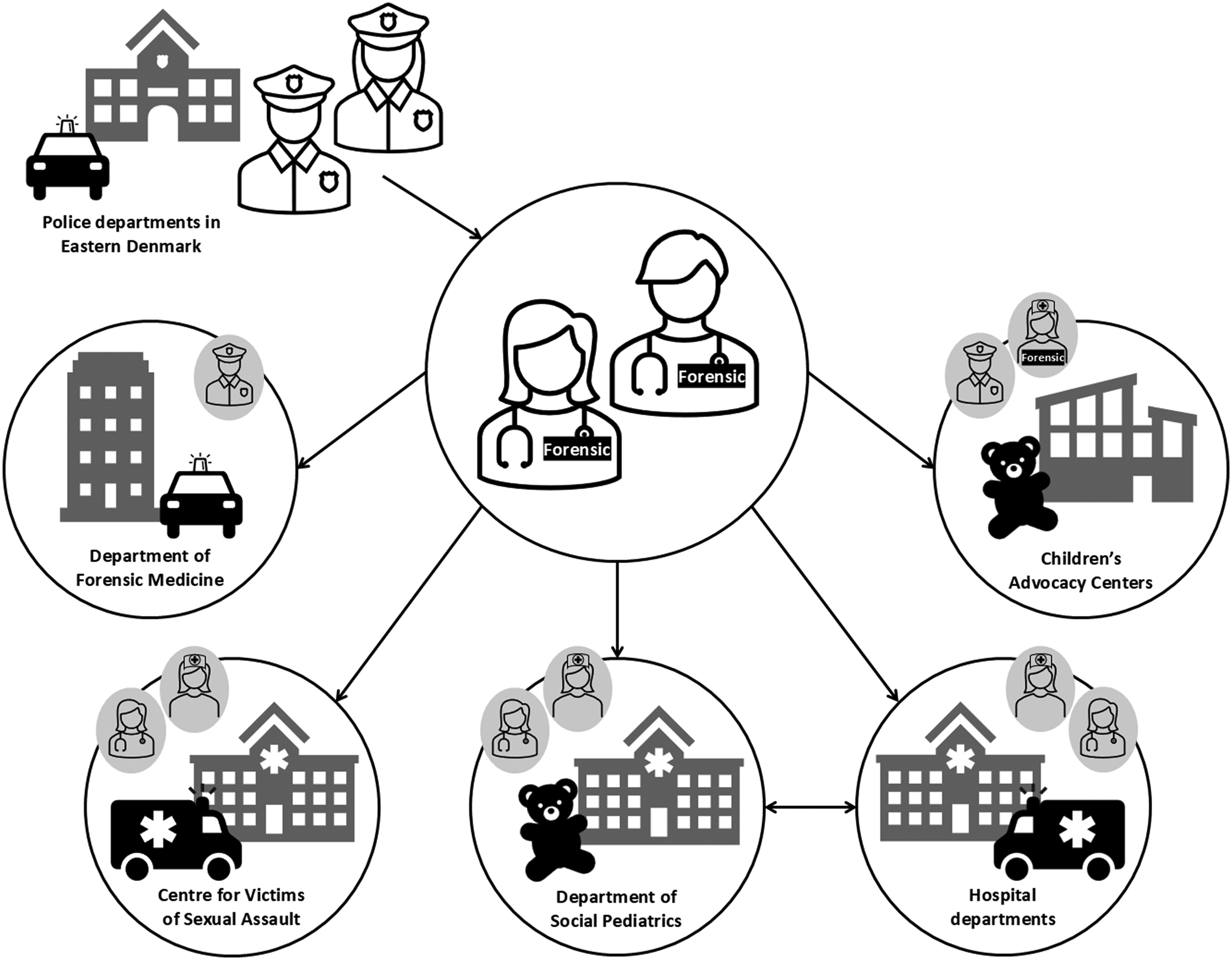
Locations of forensic examinations of children in cases of suspected child abuse and forensic collaborators. The police departments in Eastern Denmark request the forensic examinations of children conducted by forensic doctors. In cases of physical abuse, unhospitalized children may be forensically examined at the Department of Forensic Medicine in Copenhagen with the participation of the police, or at the Children's Advocacy Centers with the assistance of a forensic nurse. Hospitalized children are either forensically examined at the specialized Department of Social Pediatrics or the most relevant hospital department, such as a surgery or intensive care department. In cases of sexual abuse, forensic examinations are either conducted at the Centre for Victims of Sexual Assault or the specialized Department of Social Pediatrics in collaboration with medical doctors and nurses.
Regardless of the examination location, the unhospitalized children are brought for forensic examination by the police, together with a companion and sometimes a social worker.
Accreditation and impartiality
The regulatory work conducted by the Danish Departments of Forensic Medicine is accredited by the Danish Accreditation Fund (DANAK), 42 including the forensic examination of children: DS/EN ISO/IEC 17020:2012. 43 The annual inspection ensures validated procedures, competences, and qualifications of the staff, facilities, and equipment.
Accredited forensic standards, protocols, and checklists (Supplementary Material A, B, C) document the custody chain and ensure objective, neutral, and standardized examinations.
The Departments of Forensic Medicine are anchored at Danish universities (Figure 2), which safeguards the delimitation between the police authorities’ investigations and the treatment obligations of the Danish healthcare system.
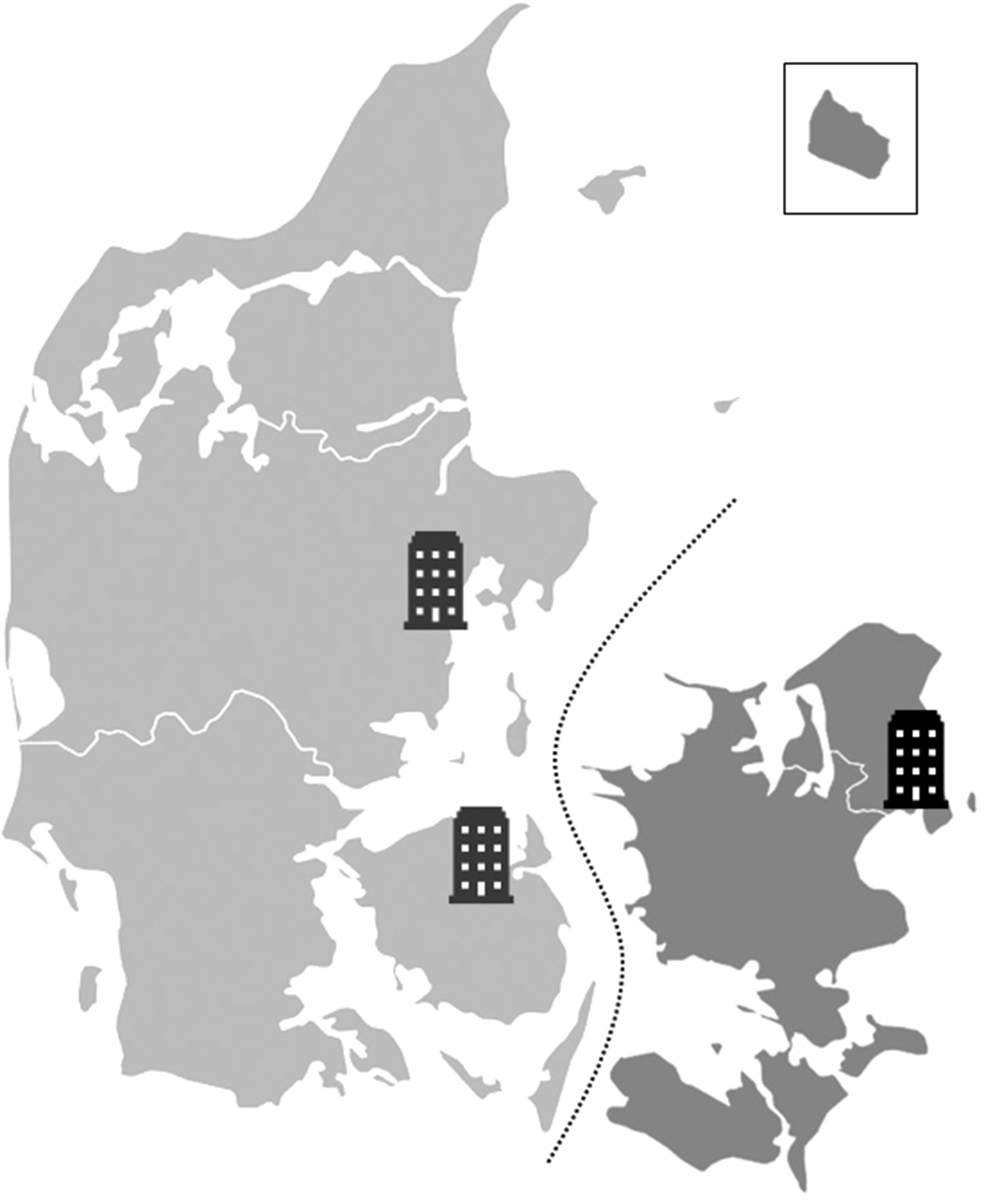
Geographic location of the Departments of Forensic Medicine in Denmark. The three Departments of Forensic Medicine in Denmark are anchored at Aarhus University, University of Copenhagen, and University of Southern Denmark and are located in Aarhus, Copenhagen, and Odense, respectively. The Department of Forensic Medicine in Copenhagen covers the dark grey area, which constitutes approximately half of the Danish population, 5.9 million inhabitants in total. The police can request a forensic examination 24 h a day, and the location of the forensic examination is determined by the case.
How is forensic examination of children conducted?
Below, we present the accredited, standardized forensic examination of children in cases of suspected child abuse. By Danish law, the conduction of forensic examinations requires informed consent, including the examination's purpose and method. Depending on the child's age, the police obtain consent from either the child's parents, social authorities, or the child itself (15–17 years).17,44,45 The police are obliged to notify the social authorities, either before the examination (<15 years) or after (15–17 years). 46
General information
Prior to the forensic examination, the police summarize the case circumstances, which are registered (Supplementary Materials A and B). The forensic doctor registers the date, time, and location of the examination, as well as the participants. A companion of the child must participate; however, this person may leave the room during the physical examination at the child's request. 46
Anamnesis
Depending on the child's age, the child or the child's companion answers standardized questions regarding the child's health and well-being. The list of questions depends on the case type (Supplementary Material B). Moreover, the forensic doctor can ask questions related to specific findings on the body, such as, “Can you recall how you got that bruise?” The forensic doctor must document from whom the information originates, including spontaneous statements.
Physical examination
The overall appearance of the child is noted, such as level of consciousness, mental status, mental and physical development, including secondary sex characteristics, cf. Tanner stage,47,48 whether the clothing is appropriate for the season, hygiene, and dental status. Height and weight are measured and plotted in a chart, cf. charts from the Danish Pediatric Society. 49
A thorough external examination of the body is performed, with documentation of all findings, including skin injuries, scars, signs of diseases, maltreatment, and, if initiated, treatment equipment. The anatomical location and type of injuries are noted in the forensic report complemented by sketches and photographs (Supplementary Material C). The presence or absence of petechiae in the conjunctivae, eyelids, face, or mouth are noted, and if indicated, the eardrums are also examined. The labial frenula are standardly examined. Specific characteristics, such as atypical birthmarks and congenital dermal melanocytosis, are also registered.
Suspected sexual abuse
In cases of suspected sexual assault, the forensic examination is conducted in collaboration with pediatricians and pediatric nurses at the specialized Department of Social Pediatrics at Herlev Hospital (0–15 years), or with gynecologists and nurses at the Centre for Victims of Sexual Assault (>15 years).
The examination of the anogenital region in girls and boys <12 years of age and in some cases between 12 and 15 years of age is performed by the forensic doctor using a photo colposcope connected to digital video recording according to international recommendations. 50 The examination of the female genitals includes an inspection of the inside of the thighs, groins, the perineum, major and minor labia, the mucous membrane around the clitoris and urethra, vestibulum, hymen, and anal region. The examination of male genitals includes an inspection of the inside of thighs, groins, perineum, penis, scrotum, and anal region. Using different positions of the body and different techniques, such as the supine labial separation method, supine labial traction technique, prone knee-chest position, and lateral decubitus, the visualization of anogenital injuries and signs of diseases, including sexually transmitted diseases, is performed without instrumentation. Moreover, age-specific changes in the genitals are described.
Suspected abusive head trauma
One of the most prominent examples of complicated and interdisciplinary child examinations is cases of suspected abusive head trauma. If abusive head trauma is suspected, the child is hospitalized at the specialized Department of Social Pediatrics, which serve as the anchoring of the extensive program conducted by several medical specialties. If urgent neurosurgical/pediatric surgical intervention or highly intensive care is required, the child is transferred to the relevant department and the Department of Social Pediatrics is kept continuously informed. The typical medical examinations are described in the following sections. 51
The radiological examinations include a complete body x-ray, which is repeated after 10–14 days, an MRI of the cerebrum and spine after 3–5 days, and a CT scan of the cerebrum, thorax, and/or abdomen in cases with symptoms.
The eyes are examined, and the presence of retinal hemorrhages is documented using ophthalmoscopy, within 24 h after hospitalization. The number of hemorrhages and their location are documented, including the involvement of ora serrata, that is, the serrated junction between the choroid and the ciliary body.
Blood tests are also performed to confirm or rule out suspected differential diagnoses, such as coagulation disorders, infections, congenital disorders (Ehlers-Danlos [I-X], osteogenesis imperfecta, and glutaraciduria type 1), deficiency conditions (Rickets, vitamin K, vitamin C, and copper), and poisoning.
Clinical genetic testing is performed only if indicated.
Photo documentation
Besides the specific findings on the body, eight standard photographs are taken: face from the front, front teeth in the maxillae, both hands (posterior manus and palm), torso including arms in situ from front and back, and both legs in situ from front and back.
Securing evidence
If the forensic examination is conducted urgently, that is, within 7 days of suspected physical or sexual abuse, the forensic doctor may secure a standard panel of DNA swabs and possibly extra swabs related to anamnestic information about the type of abuse and its location (points of contact from the perpetrator, around injuries, visible contamination with soil, blood, semen, etc.) and predilection sites for violence against children related to the child's age (Table 1).
List of standard panels and extra DNA swabs.
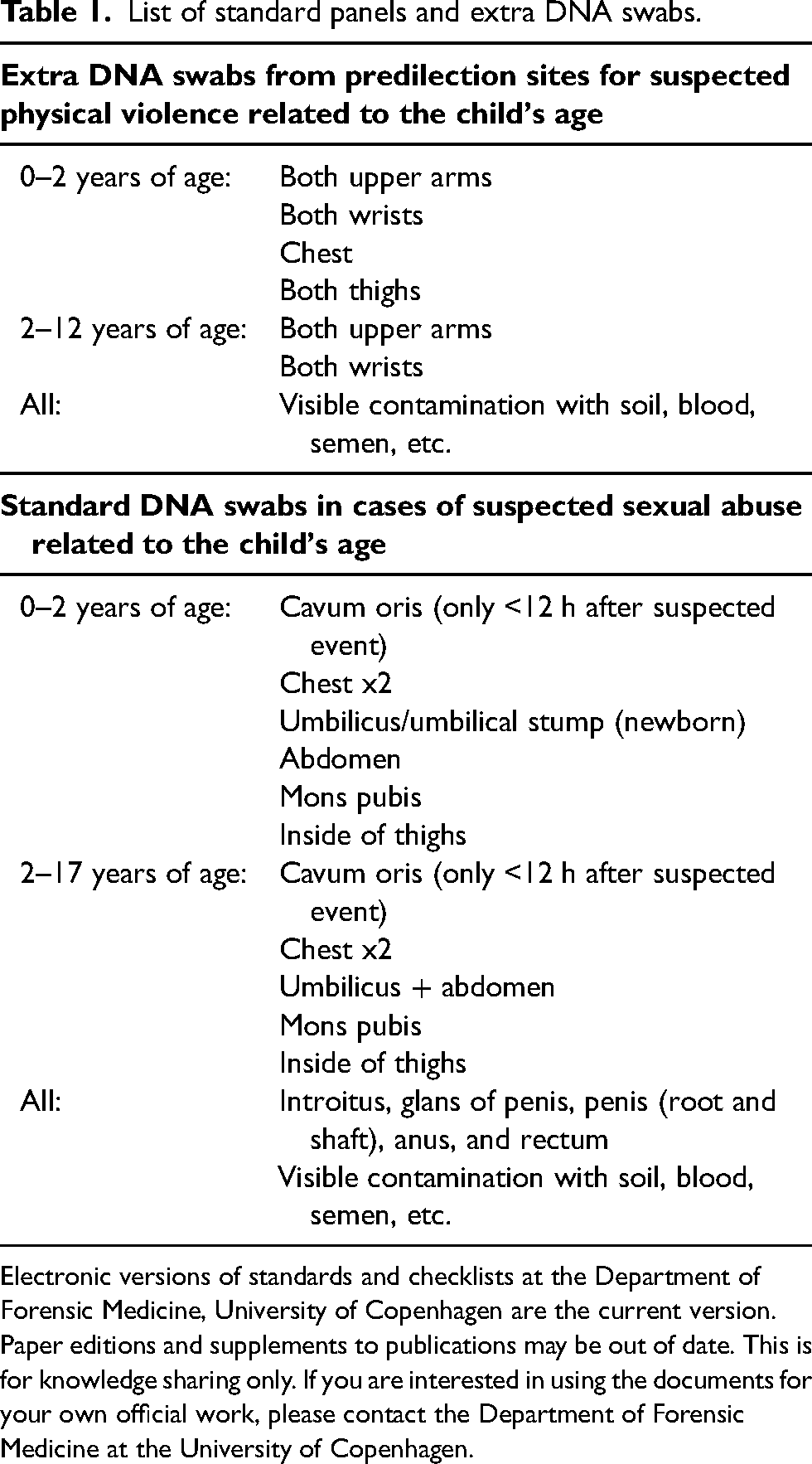
Electronic versions of standards and checklists at the Department of Forensic Medicine, University of Copenhagen are the current version. Paper editions and supplements to publications may be out of date. This is for knowledge sharing only. If you are interested in using the documents for your own official work, please contact the Department of Forensic Medicine at the University of Copenhagen.
The forensic doctor may secure other forms of evidence, such as the clothes and diapers in separate, accredited paper bags, alongside a description of potential tearing or contaminations. In relevant cases, blood, urine or hair samples can be secured for forensic chemical analysis. Blood, urine, or microbiological samples can also be taken on clinical indication.51,52
Discussion
Forensic examination can be an important investigative initiative by the police at an early stage. Thus, the injury assessment may help substantiate a suspicion of abuse, not least in cases of children who cannot speak for themselves and where a parent or guardian is suspected, challenging the loyalty of the child. Moreover, forensic documentation and secured trace evidence may be some of the most significant evidence presented during a trial. The formalized and standardized forensic education, alongside accredited protocols and checklists, ensures an objective, uniform forensic practice and enables detection of the chain of custody.
When suspicion of child abuse arises, the relevant authorities must promptly intervene. It can be complicated to clarify the child's current situation and the need for action. The CACs should form the framework for such multidisciplinary and interorganizational collaborations, where the contribution of each involved profession is described in cross-sector protocols that ensure that one sector does not compromise the others and that responsibilities are distributed appropriately. Thus, the child does not become a toss-up between different professions and is spared from having to tell their story multiple times.
Despite the intended centralization of all relevant professions at the CACs, an annual inventory report from 2019 from the Danish CACs revealed that only 3.8% and 2.3% of children who were affiliated with the centers due to a suspicion of either physical or sexual abuse were examined by a pediatrician or forensic doctor, respectively. 53 The reason for these small numbers is unclear, but the potential consequences for the children are serious; for example, the Prosecution Service's case may be weak if the injuries and scars are not documented. As a result, a cross-sectoral intervention project at the CAC in Copenhagen was launched in 2020. According to the intervention protocol, children who are subject to a video-recorded interview by the Copenhagen Police due to suspicion of physical abuse are now systematically offered a subsequent forensic examination, including a questionnaire-based, physical, and well-being screening. Forensic doctors perform the examinations with the support of the first-of-its-kind Danish forensic nurses employed in the Department of Forensic Medicine. The police receive a preliminary conclusion, which can be used as a decision-making tool in the police's screening of which cases to investigate further. If relevant, the police request a formal forensic report, which is a legal document and may be used in trials. Since implementation, the annual number of forensic examinations of children has increased, with approximately 100 examinations per year (Eastern Denmark). Such a development carries several advantages. First, more children can have their injuries documented. Second, the forensic examination may reveal physical and/or mental issues that should be followed up on by medical doctors at hospitals, a family doctor, or a dentist. Third, the high annual number of forensic examinations of children ensures the forensic doctors maintain their competences, which is also included in DANAKS’ annual evaluation of the accredited forensic regulatory work.
Forensic examinations of hospitalized children require professional teamwork. The roles must be clear and rely on the respective medical expertise and examination purposes: (1) forensic documentation, securing biological evidence, and preparation of forensic reports for the subsequent police investigation and trial; (2) medical treatment of injuries, assessment of any differential diagnoses for abuse, a thorough health examination, disease treatment, health education of the child and the guardian, and follow-up. Medical expertise becomes critical regarding the certainty and causality of findings in rare cases, as misinterpretations can have major human and legal consequences.
To achieve internationally standardized handling of cases of child abuse, initiatives such as the PROMISE Barnahus Network are set in motion. Through resources, tools, training, and so on, the network supports the European implementation of the Barnahus model as a standardized practice, that is, the legislative, administrative, health, social, and educational efforts needed to ensure the uniform identification, reporting, referral, investigation, and treatment of abused children. 2 However, national or even local conditions can make the realization of the PROMISE vision difficult. In Denmark, the forensic contribution consists of a systematic approach due to accredited, standardized protocols and checklists, but only two CACs have facilities to conduct forensic examinations of children in cases of suspected physical abuse. Thus, no national consistency or due process exists for the protection of children in Denmark. However, child abuse is currently receiving political attention and there is a potential will to further improve the legal position of children in Denmark.
Research perspective
In addition to the advantages of centralizing the casework in the CACs, there is also research potential through systematic data collection in the centers. Initiatives such as the intervention project enable not only forensic but also organizational and legal research, including methodological triangulation, such as mixed method studies, both in criminal and social contexts.
From a forensic perspective, the CACs can function as an entry point for systematic and continuous inclusion in research projects such as a standardized injury characterization in cases of suspected physical abuse. The high annual number of examinations, the wide age range of the children, and the possibility of comparing the forensic examination results with registry data from the Danish registers provide a unique opportunity to identify risk factors to guide forensic doctors when assessing the probability of physical child abuse.
Conclusion
A national setup in investigative procedures in child abuse cases ensures examinations of the right children at the right time by the right, specialized professionals. A timely forensic examination is an important piece in this puzzle, as the examinations provide documentation of evidence not otherwise available during police investigations and legal trials. It is necessary to have standardized, accredited protocols that ensure state-of-the-art examinations and evidence-based conclusions for the benefit of the rule of law for children, their families, and suspected perpetrators.
Key points
In Denmark, clinical forensic medicine is accredited by the Danish Accreditation Fund according to an international (ISO/IEC) and European (EN) standard approved by Danish Standards (DS): DS/EN ISO/IEC 17020:2012.
The forensic examinations of children are requested by police authorities and conducted by board-certified forensic doctors with mandatory, specific qualifications. The first-of-its-kind Danish forensic nurses participate in specific forensic examinations. Forensic doctors and nurses are employed in the Departments of Forensic Medicine at Danish universities.
Forensic examinations must be impartial, which is ensured by the delimitation from the police authorities and differentiated tasks when conducting examinations in collaboration with medical staff employed at hospitals (forensic documentation versus medical treatment and follow-up).
Forensic examinations provide documentation of findings that may substantiate or refute a suspicion of child abuse, which is important for police investigation and legal trial, thereby safeguarding the rule of law for both children and suspected perpetrators.
The Danish Children's Advocacy Centers (CACs) enable a cross-sectoral collaboration for the benefit of abused children but also hold a research potential for systematic and standardized forensic examinations of children, resulting in continuous data collection that strengthens evidence-based, objective, and neutral forensic assessments used in the judicial system.
Supplemental Material
sj-pdf-1-msl-10.1177_00258024251348728 - Supplemental material for Clinical forensic medical examinations conducted by the Department of Forensic Medicine in Copenhagen in child abuse cases
Supplemental material, sj-pdf-1-msl-10.1177_00258024251348728 for Clinical forensic medical examinations conducted by the Department of Forensic Medicine in Copenhagen in child abuse cases by D. Justesen, L. Slot, L. Thorlacius-Ussing, A. Bugge, C.J. Wingren and J. Banner in Medicine, Science and the Law
Supplemental Material
sj-pdf-2-msl-10.1177_00258024251348728 - Supplemental material for Clinical forensic medical examinations conducted by the Department of Forensic Medicine in Copenhagen in child abuse cases
Supplemental material, sj-pdf-2-msl-10.1177_00258024251348728 for Clinical forensic medical examinations conducted by the Department of Forensic Medicine in Copenhagen in child abuse cases by D. Justesen, L. Slot, L. Thorlacius-Ussing, A. Bugge, C.J. Wingren and J. Banner in Medicine, Science and the Law
Supplemental Material
sj-pdf-3-msl-10.1177_00258024251348728 - Supplemental material for Clinical forensic medical examinations conducted by the Department of Forensic Medicine in Copenhagen in child abuse cases
Supplemental material, sj-pdf-3-msl-10.1177_00258024251348728 for Clinical forensic medical examinations conducted by the Department of Forensic Medicine in Copenhagen in child abuse cases by D. Justesen, L. Slot, L. Thorlacius-Ussing, A. Bugge, C.J. Wingren and J. Banner in Medicine, Science and the Law
Footnotes
Acknowledgments
The authors wish to acknowledge Anne Cathrine Cole for English language editing and translation of the supplementary materials.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
Not applicable.
Funding
The Danish Victims Fund, (grant number 20-610-00102, 21-610-00133), TrygFonden, (grant number 159063).
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Data availability
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.