
Abstract
Black oesophagus, or acute necrotising oesophagitis, is characterised by diffuse circumferential black discolouration of the distal oesophagus associated with mucosal necrosis. A consistent feature is a very sharp line of demarcation at the gastro-oesophageal junction. Two cases are reported to demonstrate differences in the lower margin. Case 1: a 63-year-old man who died of gastrointestinal haemorrhage complicating black oesophagus was noted to have an irregular lower border located approximately 5 cm from the gastro-oesophageal junction. This was associated with columnar mucosa typical of Barrett oesophagus. Case 2: a 79-year-old man who aspirated gastric contents following gastrointestinal haemorrhage due to black oesophagus had diffuse black discolouration of the oesophageal mucosa with the more usual sharply demarcated inferior margin at the gastro-oesophageal junction. Sparing of the distal oesophagus in case 1 was most likely due to the protective effect of metaplastic columnar epithelium, a finding that may, therefore, be a potential macroscopic marker for Barrett oesophagus in individuals with black oesophagus.
Introduction
So-called ‘black oesophagus’ refers to acute oesophageal necrosis or acute necrotising oesophagitis. Although also known as Gurvits syndrome 1 it was actually first described by Goldenberg in 1990 in a post-operative patient who presented with a massive haematemesis. 2 The aetiology remains unclear; however the characteristic features are of diffuse circumferential black discolouration of the distal oesophagus associated with mucosal necrosis. Typically, there is a very sharp line of demarcation at the normal-appearing gastro-oesophageal junction. 3 A case is reported where the necrotic area identified at autopsy terminated at an irregular border some distance proximal to the gastro-oesophageal junction due to underlying Barrett oesophagus.
Materials and methods
Following a case of black oesophagus where the black mucosal discolouration did not extend to the gastro-oesophageal junction, as is usual, a review was undertaken of the pathology archive at Forensic Science SA to look for cases with similar features. None were found. The details of the sentinel case and a more typical case for comparison are reported.
Case reports
Case 1: A 63-year-old man with a history of alcoholism had been complaining of ‘stomach pain’ with an episode of haematemesis. He was found dead at his home address.
At autopsy there were early putrefactive changes with the major findings limited to the gastrointestinal tract where there was dark-grey and patchy black discolouration of the proximal two-thirds of the oesophagus (black oesophagus) associated with altered blood in the stomach, duodenum, small intestine and large intestine. The dark discolouration ceased approximately 5 cm from the gastro-oesophageal junction (Figure 1(a)). There was micronodular cirrhosis of the liver. Other findings included diffuse coronary artery calcification without significant occlusion, patchy calcification of the anterior leaflet of the mitral valve without evidence of endocarditis, incidental gallstones and a 4.5-cm diameter renal cell carcinoma of the right kidney with no evidence of local or metastatic spread.
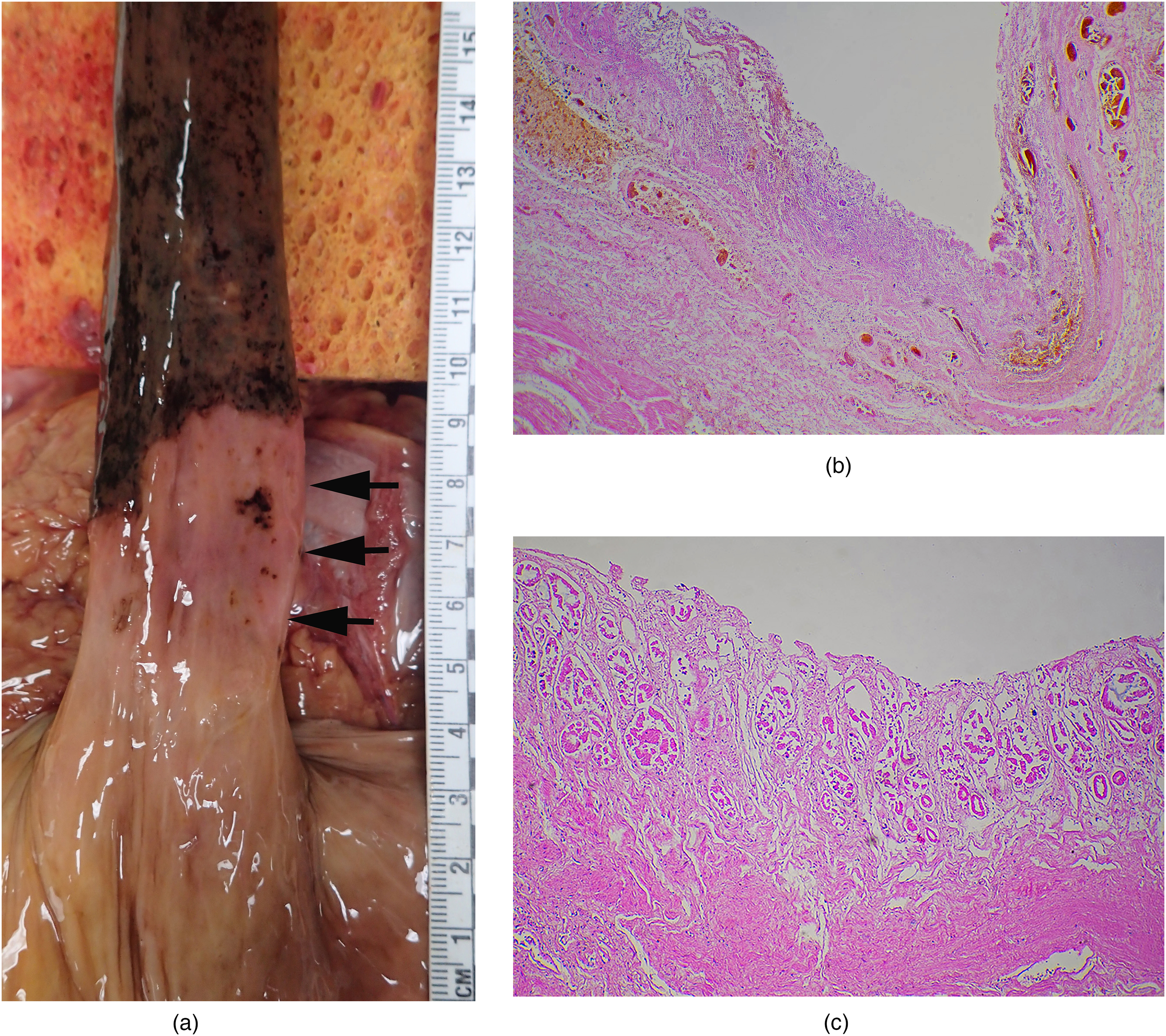
Case 1: dark black discolouration of the oesophagus without involvement of the distal 5 cm (arrows) (a). Histology of the dark areas showed extensive acute oesophageal ulceration extending into the submucosa with a patchy surface coating of altered blood and focal extension of the acute inflammatory cell infiltrate into the muscularis propria (haematoxylin and eosin, H&E 100×) (b). Sparing of the distal oesophagus was associated in case 1 with autolytic columnar mucosa typical of Barrett's oesophagus (H&E 100×).
Histological examination of the oesophagus revealed extensive acute mucosal necrosis with loss of the surface epithelium and diffuse ulceration extending into the submucosa (Figure 1(b)). There was an associated patchy surface coating of altered blood. In areas the acute inflammatory cell infiltrates extended into the muscularis propria. Sparing of the distal 5 cm of the oesophagus that had been noted macroscopically was due to columnar mucosa typical of Barrett oesophagus (Figure 1(c)). Oesophageal varices were also noted which may have contributed to the gastrointestinal bleeding. Toxicology revealed no alcohol or common drugs. There were no injuries or other underlying organic disease which could have caused or contributed to death. Death was attributed to gastrointestinal haemorrhage complicating acute oesophageal mucosal necrosis (black oesophagus).
Case 2: A 79-year-old man with a history of adenocarcinoma of the prostate with recent weight loss was found dead at his home address.
At autopsy there was diffuse black discolouration of the oesophageal mucosa (black oesophagus) extending to a sharply demarcated inferior margin at the gastro-oesophageal junction (Figure 2), with altered blood in the stomach and small intestine. A single, superficial duodenal mucosal erosion was also present. In addition, gastric contents containing altered blood were present within the peripheral airways of both lungs. Other findings included mild to focally moderate coronary artery atherosclerosis, hypertensive changes of the kidneys and a mildly enlarged and indurated prostate gland.

Case 2: dark black discolouration of the oesophagus with a more typical acute line of demarcation at the gastro-oesophageal junction.
Histology confirmed the presence of black oesophagus with loss of surface epithelium and a diffuse neutrophilic inflammatory exudate over the exposed muscularis mucosae capped by small amounts of altered blood. The submucosa was oedematous and was diffusely infiltrated by neutrophils and scattered mast cells. The muscularis propria was normal.
Toxicology revealed no alcohol or common drugs apart from prescribed anti-hypertensives. There were no injuries or other underlying organic disease which could have caused or contributed to death. Death was attributed to aspiration of gastric contents complicating gastrointestinal haemorrhage due to acute oesophageal mucosal necrosis (black oesophagus).
Discussion
Black oesophagus is a rare entity that has a very characteristic appearance at autopsy with often complete black discolouration of the oesophageal lining that is due to full thickness mucosal necrosis. It has been most often reported in the clinical literature with an incidence in patients having upper gastrointestinal endoscopies of 0.0125–0.2%.4–6 At autopsy the incidence has been reported as 0.2% 4 with less than 90 reported cases found in a review in 2007. 1
A very characteristic feature is the abrupt termination at the gastro-oesophageal junction.7,8 The differential diagnosis includes caustic ingestion, acanthosis nigricans, anthracosis, malignant melanoma, melanosis and pseudomelanosis.9–14 Histologic examination reveals full thickness mucosal necrosis overlying a band of polymorphonuclear leucocytes in the upper submucosa. The adjacent mucosa of the stomach is unremarkable.7,8 A clinical staging system has been proposed to characterise the progression of the disease. 1
Other causes of unexpected death from oesophageal lesions involve obstruction, perforation, rupture or haemorrhage. 15 While black oesophagus may be an incidental finding at autopsy, it may also present with significant upper gastrointestinal haemorrhage causing haematemesis and/or melaena (in 78% of patients). Other symptoms include epigastric pain, dysphagia, nausea, vomiting, fever and syncope. 16 Complications include strictures, perforation and mediastinitis/abscess formation. It is most commonly found in elderly males (84%) (Mage = 65 years) who often have one or more underlying comorbid conditions which have included duodenal ulceration (33%), malignancy (20–29%), renal insufficiency (29%), diabetes mellitus (24–28%), hypertension (20%), alcohol abuse (10%) and coronary artery disease (9%).3,4 The mortality rate of 32% has been attributed mainly to these comorbidities. Clinical associations have included general debility, malnutrition, multi-organ failure, sepsis, hypoperfusion, alcohol intoxication, diabetic ketoacidosis, traumatic aortic transection, gastric volvulus and thromboembolic phenomena. 3
The aetiology of black oesophagus remains uncertain with proposals that the tissue insults are multi-factorial involving reduced blood flow, impairment of mucosal defence barriers, thromboembolic events and exposure to acidic gastric contents. The latter may have been exacerbated by oesophagogastroparesis and gastric outlet obstruction. 3 The distal oesophagus is most vulnerable to ischaemic insult as it is less vascularised 16 ; hypercoagulable states associated with malignancy may also cause microvascular thrombosis contributing to decreased perfusion. Other associated factors are oesophageal infections with herpes simplex and Candida albicans, acute blood loss, dehydration, hypothermia and anti-phospholipid anti-body syndrome.4,17–19
Barrett oesophagus refers to the presence of metaplastic columnar epithelium (with or without goblet cells) replacing the usual squamous epithelium of the distal oesophageal mucosa. It is caused by chronic injury from gastro-oesophageal reflux and is found in 10–15% of those with reflux and 5.6% of adults in the United States. 20 Some of the risk factors such as advancing age and male sex are similar to those for black oesophagus, with other pre-disposing factors being obesity, cigarette smoking, Caucasian race and family history. 21 A major consequence of Barrett oesophagus is that it represents a pre-malignant transformation with an increased risk of oesophageal adenocarcinoma 22 with the incidence of oesophageal and gastro-oesophageal junction adenocarcinoma increasing by 600% in the United States over the past 30 years. 23 Barrett oesophagus may also come to forensic attention with cases of sudden death occurring due to ulceration with haemorrhage or perforation. 24 The significance in Case 1 was the absence of mucosal necrosis in the areas of metaplasia.
It has been suggested that sparing of the gastric mucosa from blackening (Figure 2) is due to the relative vulnerability of ischaemic/hypoperfused oesophageal mucosa to acid damage, compared to the epithelial lining of the stomach. Acid injury had also been proposed as an explanation for the association of black oesophagus with duodenal ulceration, again with sparing of the intervening stomach.1,4,25 The lack of changes in the distal oesophagus in the reported case could therefore be due to a protective effect from the presence of metaplastic columnar epithelium from a Barrett oesophagus. This finding is in keeping with vulnerability of residual squamous epithelium to acid damage, as well as being a potential macroscopic marker for heterotopic columnar epithelium. Both should be considered at autopsy if there is no clear termination of a black oesophagus at the gastro-oesophageal junction with an irregular distal margin.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.