
Abstract
On 11 February 2025, Tuscany became the first region in Italy to approve a law regulating medically assisted suicide. However, the law makes no provision for psychological support or educational and training programs for healthcare professionals involved in the procedure. Studies from countries where assisted suicide has long been legal highlight its significant psychological and emotional impact on care providers. In response, various forms of psychological support have been implemented to help and protect healthcare staff from the side effects of these events. Moreover, specialized training programs have been developed to equip healthcare providers with the necessary skills to handle assisted suicide requests appropriately. Tuscany's initiative may pave the way for other regions to adopt similar measures and, ideally, for a parliamentary law to regulate the practice nationwide. Therefore, this paper strongly argues that the inclusion of structured psychological support and specialized training programs is a fundamental requirement for developing an ethical, sustainable, and comprehensive end-of-life framework in Italy.
Introduction
On 11 February 2025, Tuscany became the first region in Italy to approve a law 1 regulating medically assisted suicide, marking a significant shift in the national discourse. In Italy, the debate on this topic began to gain public and legal significance in the early 2000s, driven by several high-profile cases that garnered widespread national attention, and has been highly contentious since then. The absence of clear national legislation has led many individuals to seek assisted suicide abroad, especially in Switzerland, where the practice is legally regulated and available to foreign citizens. Article 580 of the Italian Penal Code 2 criminalizes the incitement or assistance of suicide, prescribing a prison sentence of 5–12 years, not only for those who induce or reinforce another person's suicidal intent but also for anyone who facilitates its execution in any way. However, in recent years, the Italian Constitutional Court has issued two important judgments on the matter, significantly reshaping the legal landscape. Judgment No. 242/2019 3 declared the partial unconstitutionality of Article 580 of the Penal Code, establishing that individuals who assist in the suicide of a person who autonomously and freely makes such a decision—provided they are kept alive by life-sustaining treatments, suffer from an irreversible condition causing intolerable physical or psychological distress, and are capable of making free and conscious decisions—should not be held criminally liable. The ruling stipulated that these conditions, along with the method of execution, must be verified by a public healthcare facility within the national health service, with prior approval from the competent ethics committee. Judgment No. 135/2024 4 further clarified the criteria for accessing medically assisted suicide and emphasized the need for the legislature and the national health service to take action to ensure the implementation of the principles set forth in these rulings. While the decision of Tuscany aims to fill a legislative gap in accordance with the Constitutional Court's directives, it is likely that the newly introduced law will be met with both criticism and praise in equal measure. Setting aside personal opinions, this law potentially paves the way for similar decisions by other regions and, ideally, for a parliamentary law that regulates the practice nationwide. However, beyond the legal aspects, it is essential to consider the practical, ethical, and psychological implications for healthcare professionals responsible for implementing such measures. Addressing these elements now will help ensure that the future implementation of assisted suicide laws prioritizes not only ethical considerations from the patient's perspective but also the well-being of those providing care.
The regulatory framework in Europe
In Europe, while assisted suicide—and, in some cases, even euthanasia—is legalized in some countries (Table 1), it remains illegal in others, and the debate surrounding its regulation continues to evolve, with differing views on individual rights to self-determination and end-of-life choices. In Germany, similarly to Italy, it is not yet regulated by specific national legislation but rather by Constitutional Court rulings. 5 In other countries, such as France, the issue has been widely discussed, but assisted suicide is still illegal.
European countries and their legislation on assisted suicide and/or euthanasia.

The newly introduced Italian regional law
The law approved by the Regional Council of Tuscany 1 incorporates the requirements established by the Italian Constitutional Court and stipulates that individuals wishing to resort to assisted suicide must submit a request to their local health authority, which will forward the citizen's request to the competent ethics committee and to a specific commission. This commission will be responsible for verifying whether the requirements are met and will be composed of seven members: a palliative care physician, a psychiatrist, an anesthesiologist, a psychologist, a forensic physician, and a nurse, as well as a specialist relevant to the specific pathology, who will be appointed on a case-by-case basis. Once all assessments have been completed, if the commission votes in favor of assisted suicide, it will define the procedure for carrying out assisted death, which the ethics committee must approve. At this point, the local health authority shall ensure the provision of technical and pharmacological support, as well as healthcare assistance for the preparation of the self-administration of the authorized drug. The members of the commission, as well as those providing healthcare assistance, participate voluntarily, and their activity must be carried out during working hours without any additional financial compensation. Nevertheless, there is no mention in the law for psychological support measures or educational and training programs for healthcare professionals involved in the practice.
Experiences from countries with established practices
Over the past few years, several countries have enacted laws regulating assisted death, with policies ranging from physician-assisted suicide (PAS) to voluntary euthanasia. While these measures aim to respect the wishes of individuals suffering from unbearable physical or psychological conditions who are seeking to end their lives, they also pose unique challenges for healthcare providers, particularly concerning the risk factors associated with being exposed to these challenging situations that might be emotionally, ethically, and physically demanding. Professionals who are constantly exposed to dying and death scenarios are vulnerable to developing compassion fatigue, secondary traumatic stress, and burnout. 13
Emotional and psychological impact on healthcare professionals
In countries where medically assisted suicide has been legally available for years, several studies have examined the psychological and emotional impact on healthcare professionals involved in the process. A systematic review of healthcare professionals’ perspectives on assisted suicide 14 identified several emotional challenges experienced by them. These include fear—particularly of making legal mistakes or errors during the administration process—intense emotional conflict when dealing with relatives who oppose the decision of the patient, a lack of emotional support leading to feelings of isolation, and the burden of internalized stigma.
Switzerland was the first country in the world to legalize assisted suicide in 1942. Under the Swiss Penal Code, 6 the practice is permitted as long as it is not carried out for selfish motives. PAS was further regulated in 2004, 2013, and 2018 when the Swiss Academy of Medical Sciences issued specific guidelines15–17 on the matter. A qualitative study 18 conducted among healthcare professionals in the cantons of Fribourg and Vaud found that most respondents reported a personal impact from involvement in assisted suicide, ranging from moderate (experiencing emotions such as sorrow, anger, and powerlessness) to significant (e.g. intrusive images, anxiety, intense emotional distress, and avoidance behaviors) emotional discomfort. Another qualitative study 19 focusing on palliative care physicians highlighted the challenges they faced in reconciling the principles of their specialty with a patient's request for assisted suicide.
In the United States, assisted suicide is not legal at the federal level, with its regulation determined by individual state laws. Currently, several states have legalized assisted suicide, with Oregon being the first to do so in 1997 through the enactment of the “Oregon Death with Dignity Act.” 20 After the act came into effect, several studies have investigated physician's experiences in Oregon regarding assisted suicide requests. A qualitative study 21 found that physicians often felt unprepared when faced with assisted suicide requests, particularly those who had limited experience in caring for terminally ill patients. Engaging in the practice carried a significant emotional burden and was described by participants as an intense and deeply affecting experience. Despite this, the majority did not seek support from colleagues or close contacts, and those who did often found it unavailable or, in some cases, felt rejected. After the procedure, most physicians reported no major regrets, and many acknowledged experiencing personal and professional growth. A more recent survey conducted in the state of Colorado 22 found that most participants described providing this service as emotionally fulfilling and professionally rewarding, despite being time-consuming. Nearly half found it ethically challenging, while a minority perceived it as professionally risky. The most reported barriers to physician participation in assisted dying included a lack of knowledge about the procedure, the emotional toll involved, time constraints, ethical concerns, the time it requires and potential repercussions on their professional reputation. Additionally, physicians cited personal religious beliefs and a lack of support from colleagues as further deterrents.
Both the Netherlands and Belgium legalized voluntary active euthanasia and medically assisted suicide in 2002. A series of interviews with Dutch physicians 23 revealed that they often felt pressured by patients or their relatives to proceed with assisted suicide, sometimes experiencing subtle moral pressure. The study also highlighted the occurrence of complex and unforeseen situations that physicians occasionally struggled to manage, leading the authors to propose group counseling sessions where doctors could share experiences and reflections. Another qualitative study 24 found that some physicians were hesitant to confront the emotional toll of being involved in ending a patient's life and expressed the need for personal support during this process. In Belgium, a survey conducted among psychiatrists 25 revealed that they sometimes found it challenging to assess whether a patient met the eligibility criteria for assisted suicide. Similar to Dutch physicians, 23 they reported feeling pressured by either the patient or their relatives. Moreover, 72% of participants acknowledged experiencing significant emotional strain due to the request, with more than 50% seeking emotional support to manage these feelings.
In Canada, where medical assistance in dying (MAiD) has been legal since June 2016, palliative care providers who took part in a qualitative study 26 reported significant emotional impact resulting from their exposure to voluntary assisted dying, with many expressing concerns about the social stigma attached to their involvement. Nevertheless, some participants also conveyed a sense of fulfillment from supporting the patient's wishes and acknowledging the importance of their role. Similarly, a series of interviews with physicians conducted in British Columbia 27 revealed that while many physicians found MAiD personally rewarding, they also faced emotional challenges, such as the difficulty of denying MAiD to patients who did not meet the eligibility criteria, conflicts with colleagues, and the emotional toll of supporting grieving family members.
In Victoria, Australia, voluntary assisted dying was legalized in 2019 and has since been adopted by other states. A survey 28 found that clinicians involved in the practice experienced significant emotional distress, primarily due to a lack of support and conflicting views on the topic within the workplace. Notably, 65% of respondents reported receiving no form of psychological support. The study also highlighted that the burden of providing assisted dying services fell disproportionately on a small number of physicians handling the majority of cases.
The benefits of training
As more countries adopt voluntary assisted dying legislation, the need for structured and comprehensive education and training programs for healthcare professionals involved in these procedures becomes increasingly evident. Physicians, nurses, and other healthcare professionals are tasked with navigating complex legal, ethical, and emotional landscapes when assisting individuals in ending their lives. The responsibility of assisting in such a profound decision requires specialized knowledge, skills, and emotional support, which can mitigate the psychological burden often reported by professionals. Inadequate training and support can lead to a cycle of uncertainty, anxiety, and potential legal or ethical dilemmas.
The systematic review by Byrnes et al. 14 revealed a significant concern among healthcare professionals involved in assisted dying: the lack of proper training and specialized knowledge. None of the participants in the study had received formal education on handling requests for assisted suicide, which led them to rely on their perceptions of “best practice,” institutional guidelines, or the approaches of senior colleagues. This gap in formal training often leaves healthcare providers to manage the responsibility of assisted suicide without adequate preparation. Such a lack of training creates a vicious cycle, heightening the psychological strain on clinicians as they grapple with the legal, ethical, and emotional implications of their roles. The uncertainty increases anxiety, as healthcare providers fear both failing to adequately support patients and making errors with potentially serious legal or ethical consequences. This distress further emphasizes the need for tailored training programs to prepare healthcare professionals to manage assisted dying cases competently and with confidence.
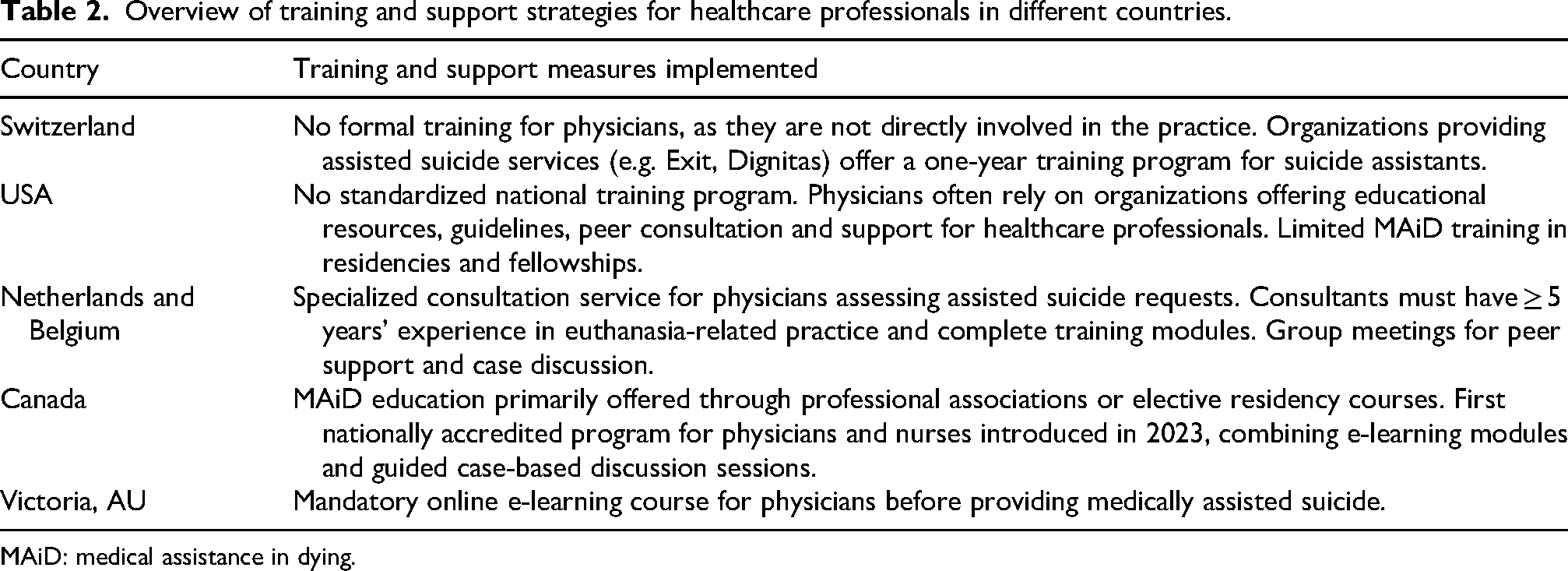
Countries where assisted suicide is legally permitted have experimented with a variety of specialized training and support strategies for healthcare professionals, aiming to ensure that end-of-life care is delivered safely, competently, and ethically (Table 2).
Overview of training and support strategies for healthcare professionals in different countries.
MAiD: medical assistance in dying.
In Switzerland, assisted suicide requests must be validated from a medical perspective, and a physician is required to prescribe the lethal medication. However, a physician's direct participation in the process is not mandatory. 29 As a result, physicians are typically involved only in assessing the patient's condition and issuing the prescription, and there is no formal training program specifically designed for them. Instead, organizations such as Exit and Dignitas provide training for suicide assistants, who are responsible for supporting the patient and their relatives, delivering the prescribed medication, and remaining on-site for the police inspection following the patient's death. These assistants undergo a 1-year training program covering the medical, legal, and psychological aspects of assisted suicide, as well as best practices for patient care. The inclusion of psychological aspects in training highlights the necessity of emotional preparedness when dealing with end-of-life scenarios. In the United States, the regulation of assisted suicide varies by state, and there is no standardized national training program, despite the demonstrated lack of specific knowledge and the expressed interest in improving it among medical residents 30 and physician assistants. 31 Physician education and preparation often rely on organizations such as End of Life Choices Oregon, which offer resources and support for healthcare professionals, including guidelines and peer consultation. On a national scale, the Academy of Aid-in-Dying Medicine, established in 2020, provides educational courses for clinicians and is currently developing a comprehensive curriculum for teaching aid-in-dying care, set to launch in 2026. However, the absence of standardized training across states reflects a fragmented approach that leaves many healthcare providers without the necessary skills and psychological support to navigate assisted dying cases effectively. As for residencies and fellowships, there is still only a limited number of programs offering comprehensive MAiD training. 32 Both the Netherlands and Belgium have implemented specialized consultation services to support both colleagues and patients in cases involving requests for assisted suicide. 33 These services are provided by trained physicians who are responsible for assessing whether patients meet the legal criteria for voluntary assisted dying. In this framework, the Support and Consultation for Euthanasia in the Netherlands (SCEN) and the Life End Information Forum (LEIF) in Belgium were created. SCEN and LEIF require their physicians to have a minimum of 5 years of experience in euthanasia-related practice, as well as to complete specialized training modules that cover various aspects of the procedure, communication with patients and colleagues, and palliative care. Additionally, both services facilitate group meetings where healthcare professionals can discuss cases and share experiences, fostering ongoing professional support and knowledge exchange. Studies on the implementation of these consultation services indicate that training is beneficial and enhances the quality of consultations.34,35 The structured approach in these countries emphasizes the importance of peer support and shared professional experiences, which contribute to better psychological resilience for healthcare providers.
In Canada, education on MAiD has primarily been offered through professional associations or as elective courses in medical residency programs. 36 A standardized national training approach has been discussed.37,38 In response, the Canadian MAiD Curriculum was introduced in 2023 as the first nationally accredited education program for physicians and nurses, available in both English and French and provided through a blend of online self-paced modules and guided case-based discussion sessions. To encourage participation, the Canadian Association of MAiD Assessors and Providers has made the program freely accessible until September 2026. 39 The development of a structured curriculum indicates the recognition of both the technical and emotional complexities of MAiD, reinforcing the need for comprehensive training programs that address the psychological impact on professionals.
In Victoria, Australia, physicians are required to complete a mandatory online e-learning course before providing voluntary assisted dying. This training program covers both the legal requirements and the clinical skills necessary for the procedure. A post-training survey 40 revealed that 97% of participants found the course helpful, and 80% expressed willingness to participate in voluntary assisted dying. Following the training, most respondents reported feeling confident in their understanding of the law and their ability to apply it effectively in practice. The positive reception of training programs in Australia demonstrates that healthcare professionals benefit from structured learning, as it enhances their competence and psychological preparedness when dealing with end-of-life decisions.
Discussion
Ethical conflicts of healthcare professionals
Several studies conducted in countries where assisted suicide has long been legal highlight that involvement in assisted suicide may create an internal conflict for physicians, balancing their professional responsibilities with their personal beliefs. 41 A healthcare professional's duty to alleviate suffering may seem at odds with the principle of preserving human life. However, it is crucial to reframe the concept of care to include alleviating suffering, even when it involves assisting in a patient's choice to end their life. In palliative care, the goal is not always to heal but to provide relief from pain and distress. A broader understanding of care—one that includes supporting patients in their autonomous decisions about death—may serve as a protective factor for professionals, reducing the psychological burden associated with their role. Recognizing that assisting in medically assisted dying can also be an act of compassion and respect for patient autonomy may help healthcare professionals navigate the emotional complexities of their work.
Furthermore, the absence of proper training and specialized knowledge in managing assisted suicide requests can significantly increase anxiety, emotional distress, and uncertainty among healthcare professionals. Without adequate preparation, physicians and other medical staff may struggle with ethical uncertainties, fear of making procedural errors, or difficulties in communicating effectively with patients and their families. This lack of confidence and support can not only affect professionals’ well-being but may also impact the quality of care provided, potentially leading to delays, mismanagement, or inconsistencies in the implementation of the procedure. Integrating death education into training programs, emphasizing that care extends beyond curative efforts to pain alleviation and psychological support, could help professionals build resilience and maintain a sense of purpose in their role. Given these challenges, any future regulatory framework in Italy should incorporate structured forms of psychological support and specialized training programs for medical professionals. Ensuring that healthcare providers receive proper preparation and psychological assistance is crucial for a balanced and responsible implementation of the practice in Italy, one that safeguards both patients and healthcare professionals alike.
Practical support solutions inspired by other countries
Italy could draw inspiration from international approaches, implementing various strategies to provide both emotional and professional support. For instance, Belgium and the Netherlands have developed consultation services that support healthcare professionals by allowing them to discuss complex cases, express their concerns, and receive guidance from experienced colleagues. Debriefing sessions following assisted suicide cases could help physicians and other healthcare professionals process their experiences, reflect on the ethical and emotional aspects involved, and share concerns in a structured and supportive environment. Mentoring programs could pair less experienced physicians with colleagues who have already handled assisted suicide requests, providing guidance and reassurance throughout the process. Peer support networks would allow physicians to exchange experiences and coping strategies, fostering a sense of solidarity and shared responsibility.
Moreover, structured training programs should be developed to equip physicians with the necessary skills to handle assisted suicide requests. Such training should go beyond the legal and procedural aspects, focusing on communication skills, ethical considerations, and strategies for managing emotional distress.
Importance of specialized training and death literacy
Countries with well-established assisted dying laws have demonstrated that structured training not only enhances competence and professionalism but also provides essential emotional coping mechanisms. Even though healthcare professionals are frequently exposed to death during their training and practice, this exposure is not without consequences. 42 On one hand, encountering patient deaths has been associated with a more positive attitude toward the responsibility of caring for dying patients, an improved ability to support their families, and deeper professional knowledge. 43 On the other hand, it can also trigger intense emotional reactions, 44 particularly in professionals who have not developed the skills to regulate their emotional involvement with patients. 45 Thus, training programs should emphasize death literacy, helping professionals reframe their understanding of care and develop resilience in emotionally challenging scenarios. Recognizing that providing medically assisted dying can be an act of compassion and care, rather than a failure to heal, may help professionals find meaning and purpose in their role.
Given the emotional, legal, and ethical challenges related to assisted dying, it is evident that structured psychological interventions and comprehensive training programs are necessary. By integrating these measures into future regulations, Italy could create a framework that acknowledges the complexities of assisted suicide, ensuring that the practice is carried out ethically, safely, and with due consideration for the well-being of both patients and healthcare professionals. A comprehensive, multidisciplinary approach to training and support—one that includes legal education, ethical reflection, emotional resilience-building, and death literacy—can help professionals navigate the moral and psychological challenges of assisted suicide while maintaining the highest standards of patient care.
Limitations
Given the recent implementation of the relevant legislation, this analysis necessarily draws on international evidence and comparative legal frameworks. While these models provide valuable insights, their direct applicability to the Italian context remains to be fully assessed and will require further empirical investigation as the national experience evolves.
Conclusion
In light of the above, specialized training and psychological support are crucial strategies to ensure that healthcare professionals can competently, ethically, and consistently manage assisted suicide cases, while also safeguarding their own mental health. Consequently, the integration of these measures in Italy should not be postponed but recognized as an urgent priority. Without them, the risk remains of fragmented, inconsistent, and ethically fragile practices that fail to meet the needs of both patients and professionals. Embedding these elements into future legislation is therefore not a secondary consideration, but a fundamental requirement for an ethical, sustainable, and comprehensive end-of-life policy in Italy.
Footnotes
ORCID iDs
Ethical considerations
There are no human participants in this article and informed consent is not required.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
GS contributed to conceptualization, data curation, project administration, writing—original draft, and writing—review & editing; MER contributed to writing—review & editing; SB contributed to supervision; SDV contributed to supervision; GC contributed to supervision, writing—review & editing; GB contributed to conceptualization, writing—review & editing, and supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.