
Abstract
This is the first study to examine mental health issues, substance use, and suicide risk among incarcerated women in Paraguay, aiming to identify factors associated with these conditions, such as age and medical history. A cross-sectional study was conducted on 215 incarcerated women. Participants were assessed using the Symptom Checklist-90-Revised (SCL-90-R) to evaluate mental health symptoms, Columbia Suicide Severity Rating Scale (C-SSRS) for suicide risk, and MULTICAGE CAD-4 to measure alcohol and drug addiction. The chi-square test and odds ratios were applied to identify associations between mental health outcomes and associated factors, with a significance level of 5%. Our findings revealed that 40% of the participants had some level of suicide risk. Alcohol consumption was reported by 36.7% of the participants; 59.5% screened positive for alcohol-related problems, and 45.6% used drugs, with 73.5% screening positive for drug-related problems. Depression (23.7%) and somatization (21.4%) were the most frequent dimensions of mental health symptoms. Younger women (aged 18–38 years) were significantly more vulnerable to hostility, psychoticism, and interpersonal sensitivity. The study also identified a significant relationship between substance use and suicide risk, with substance users more likely to exhibit suicidal tendencies. Our study highlights the urgent need for integrated mental health and substance use interventions in Paraguayan prisons, especially for younger women who are at higher risk of mental health disorders. Suicide prevention strategies should be prioritized by incorporating mental health and substance use treatments. Further research is needed to explore these issues longitudinally and in different prison environments.
Introduction
The prevalence of mental health problems among prisoners has been consistently observed across various countries and regions, with rates of mental disorders significantly higher in prison populations compared to the general population.1,2 Imprisonment often worsens existing mental health issues and introduces new psychological challenges that complicate successful reintegration into society. In particular, female prisoners have unique health needs that require specialized attention within the prison system. 3
In Paraguay, research on the mental health of incarcerated women is limited. Previous reports have primarily focused on general prison conditions, human rights, and healthcare access, with little emphasis on mental health.4–7 However, recent studies have highlighted the mental health challenges faced by female prisoners. One cross-sectional study found that 38% of incarcerated women experienced depression, while 36.1% were at risk of suicide. Furthermore, women with depression were nearly five times more likely to exhibit suicidal tendencies. 8
Globally, female prisoners have shown significantly higher rates of mental health problems than those of the general population. Studies have indicated that these individuals are five times more likely to experience mental health disorders. 9 The most frequently observed psychological issues include depression, anxiety, and substance use disorders. 10 Furthermore, women with mental health problems in prison have been found to face increased risks of victimization, particularly sexual victimization. 11
Given the scarcity of research in Paraguay, this study aims to contribute to the understanding of mental health issues among female prisoners. Data were collected on a range of psychological symptoms, suicide risk, and substance use, along with sociodemographic variables (such as age, education level, and family structure), prison context variables (such as legal status, type of offense, and length of incarceration), and health-related variables (such as medical and mental health history). By analyzing these factors, this study sought to provide a comprehensive understanding of the mental health needs of female prisoners in Paraguay and to explore potential correlations between these variables and mental health outcomes.
This study is the first of its kind in Paraguay, addressing a critical gap in the existing literature. We believe that our findings will provide a foundation for future public health interventions and policies aimed at improving mental health services in prisons.
Methods
Design and setting
This descriptive, observational, cross-sectional study 12 was conducted at the “Casa del Buen Pastor – Women's Penitentiary,” the oldest and largest women's prison in Paraguay, located in the capital city, Asunción. It is the only women's penitentiary in the capital and one of only three exclusively for women in the entire country. Additionally, there are nine separate wings designated for women within men's penitentiaries. At the time of the study, Buen Pastor housed 594 of the 972 women deprived of liberty throughout the country.
Participants and sampling
A total of 594 potential participants were initially approached, considering the total prison population of “Casa del Buen Pastor” in June 2024. Based on this population, the sample size was calculated using the epidemiological package Epidat 4.2 (Pan American Health Organization, Health Board of Galicia, and Universidad CES de Colombia). Assuming an expected frequency of common mental disorders of 38% in female prisoners, 8 a confidence level of 95%, and a precision of 5.5%, the minimum sample size was set at 200 participants. 13 Finally, 215 participants were randomly selected using simple random probabilistic sampling from the aforementioned total. None of the participants were excluded due to risk concerns, nor were they lost due to being transferred or released before the research team approached them. None of them was removed because of significant language barriers. None of the participants withdrew from this study.
Measures
Sociodemographic data
Participants were asked to report their age, their nationality (Paraguayan, Foreign national), and whether they belonged to an Indigenous group in Paraguay (yes, no). Participants also indicated whether they had children and how many, their educational level (no formal education, primary, secondary, or university education), if they had employment before imprisonment (yes, no), and monthly income (less than the minimum wage, minimum wage, more than the minimum wage).
Prison context data
Participants provided information on various prison context variables, including their legal status (sentenced for an offence with a penalty of more than 5 years, sentenced for an offence with a penalty of less than 5 years, remanded), the cause of their imprisonment (property crimes, drug-related offences, violent crimes), and whether they were in a maximum-security regime (yes, no). They also indicated whether they had a family member in prison (yes/no; if yes, specify relationship), whether they had prior offenses (yes, no), the length of their current prison stay (years), and their age at first incarceration.
Health related data
Participants provided information on their health background, including whether they had any medical condition (yes/no; if yes, specify), any history of mental illness (yes/no; if yes, specify), and whether they were currently receiving treatment (yes/no; if yes, specify type: medical, psychological/psychiatric).
Assessments
Participants were assessed on various dimensions of mental health and substance use. The Symptom Checklist-90-Revised (SCL-90-R) was used to measure a broad range of psychological symptoms and provide an overall psychological distress profile, including dimensions such as somatization, depression, anxiety, and psychoticism. The Columbia Suicide Severity Rating Scale (C-SSRS) evaluated suicide risk, while the MULTICAGE CAD-4 assessed issues related to alcohol and drug use.
The SCL-90-R is a 90-item questionnaire rated on a five-point scale (0–4), designed to assess psychological symptoms across nine primary symptom dimensions and three global distress indices. The symptom dimensions include Somatization (SOM), which evaluates perceived bodily dysfunctions; Obsessions and Compulsions (OBS), which assesses unwanted thoughts and repetitive behaviors; Interpersonal Sensitivity (SI), focused on feelings of inferiority; Depression (DEP), covering symptoms of depressive disorders; Anxiety (ANS), which assesses general anxiety symptoms; Hostility (HOS), reflecting anger and irritability; Phobic Anxiety (FOB), which measures irrational fears; Paranoid Ideation (PAR), addressing suspiciousness and fear of losing autonomy; and Psychoticism (PSIC), which evaluates symptoms related to isolation and thought disorders. The three global distress indices include the Global Severity Index (GSI), which measures overall distress by combining symptom number and intensity; the positive symptom total (PST), which counts the number of symptoms reported; and the positive symptom distress index (PSDI), which evaluates the severity of reported symptoms. Additionally, the SCL-90-R contains seven supplementary items assessing issues, such as sleep disturbances and appetite problems. The inventory takes approximately 15 min to complete and is suitable for individuals aged 13–65 years. For those with reading difficulties, the items can be read aloud, although the inventory is not recommended for individuals with severe intellectual disabilities or psychotic disorders, as these conditions may affect response validity.14,15 In this study, the Spanish version by Casullo and Pérez for the Universidad de Buenos Aires and the National Scientific and Technical Research Council (Consejo Nacional de Investigaciones Científicas y Técnicas [CONICET]) was used. 16 This version has shown utility in both adolescents and adults across South America.17–19
The SCL-90-R provides raw scores that can be transformed into T-scores for comparison with clinical thresholds. According to the original manual, 14 “caseness” is typically defined by a T-score ≥ 63 on at least one primary dimension, or T-scores ≥ 63 on two or more of the global indices (GSI, PST, and PSDI). However, in the present study we did not apply these clinical thresholds, as our primary aim was to describe the distribution of symptoms rather than to identify probable clinical cases. Accordingly, results are presented as prevalence rates and mean scores, without categorization based on caseness criteria.
The C-SSRS is a widely used tool for assessing suicide risk, with various versions tailored to different contexts, purposes, and populations (such as adults or adolescents).20,21 While the complete version varies in length, the abbreviated six-item version, known as the C-SSRS Screener, focuses on rapidly assessing suicidal ideation and immediate risk, making it particularly useful in settings where time is limited, such as emergency services, primary care, and mental health assessments in schools or workplaces. The six-item C-SSRS Screener is structured into two main sections. Suicidal Ideation (five questions) assesses the presence, frequency, and intensity of suicidal thoughts, including whether the individual has thought it would be better to be dead, has wished to be dead, has had suicidal thoughts without a specific plan, has thought of a method without intent to act, or has had thoughts of suicide with a specific method and intent to carry it out. Suicidal Behavior (one question) examines whether the individual has made a suicide attempt in the past or has made preparations to do so.22,23 The six-item C-SSRS Screener effectively identifies suicide risk levels, helping determine if a more comprehensive assessment or immediate intervention is needed. In this study, we used the Spanish version of the C-SSRS Screener, accessed through The Columbia Lighthouse Project website, which provides downloadable versions tailored to different contexts (such as clinical and educational settings) and translated into multiple languages: https://cssrs.columbia.edu.
The MULTICAGE CAD-4 24 consists of 32 items that investigate various forms of addiction and problematic behaviors: alcohol abuse/dependence (Items 1–4); pathological gambling (Items 5–8); substance addiction (Items 9–12); eating disorders (Items 13–16); Internet addiction (Items 17–20); video game addiction (items 21–24); compulsive spending (Items 25–28); and sex addiction (Items 29–32). Originally designed in Spanish, each problem area is explored through four questions that follow the CAGE scheme 25 : self-perception of the problem, perception by cohabitants, feelings of guilt, and signs of withdrawal or inability to control behavior. The questionnaire is self-administered and uses a Yes/No format. A score of zero or one affirmative response indicates the non-existence of the problem; two affirmative responses indicate a possible problem; three affirmative responses suggest the very probable existence of a problem, and four affirmative responses strongly suggest the presence of a problem. A criterion of two or more affirmative responses per scale is used to define problematic behavior. Both the complete scale and its subscales demonstrate good psychometric properties. 24 For the purposes of this study, only the subscales corresponding to alcohol abuse/dependence and substance addiction were used, as these dimensions were considered most relevant in the context of the population of incarcerated women in Paraguay.
Procedure and ethical considerations
The researchers involved in the participants’ assessments (G.V., D.A., N.L., and S.G.) had postgraduate training in psychiatry and received specific training in administering each of the screening tools prior to the start of the project. Initial assessments conducted by these researchers were observed by the first author (J.T.), with additional spot checks made throughout the project to ensure quality assurance and standardization. These researchers were also supervised by the first author during the entire data-collection process. Informed consent was obtained from all participants before beginning the assessment sessions, which were conducted between July and September 2024. To ensure full comprehension, all screening tools were read aloud by the researchers. Each session was conducted on a one-to-one or two-to-one basis, following the advice of prison staff to address operational and risk-related considerations. The assessment sessions typically lasted between 55 and 75 min.
This study was conducted within the framework of the Scientific Research Improvement Program of the Research Group on Epidemiology of Mental Disorders, Psychopathology, and Neurosciences and received approval from the Department of Medical Psychology of the School of Medical Sciences, National University of Asunción, Paraguay (Reference 001-006-2024). All participants provided written informed consent prior to participation. Data were handled with strict confidentiality, equality, and justice, in accordance with the principles of the Declaration of Helsinki.
Data analysis
The data were entered into a spreadsheet and then processed using the statistical software packages RStudio 2023.09.1 + 494 and Jamovi 2.5.2.0. Frequency tables were used for categorical variables, while measures of central tendency and dispersion were calculated for numerical variables. For inferential analysis, the chi-square test and odds ratios (OR) were applied, with a significance level of 5%.
Results
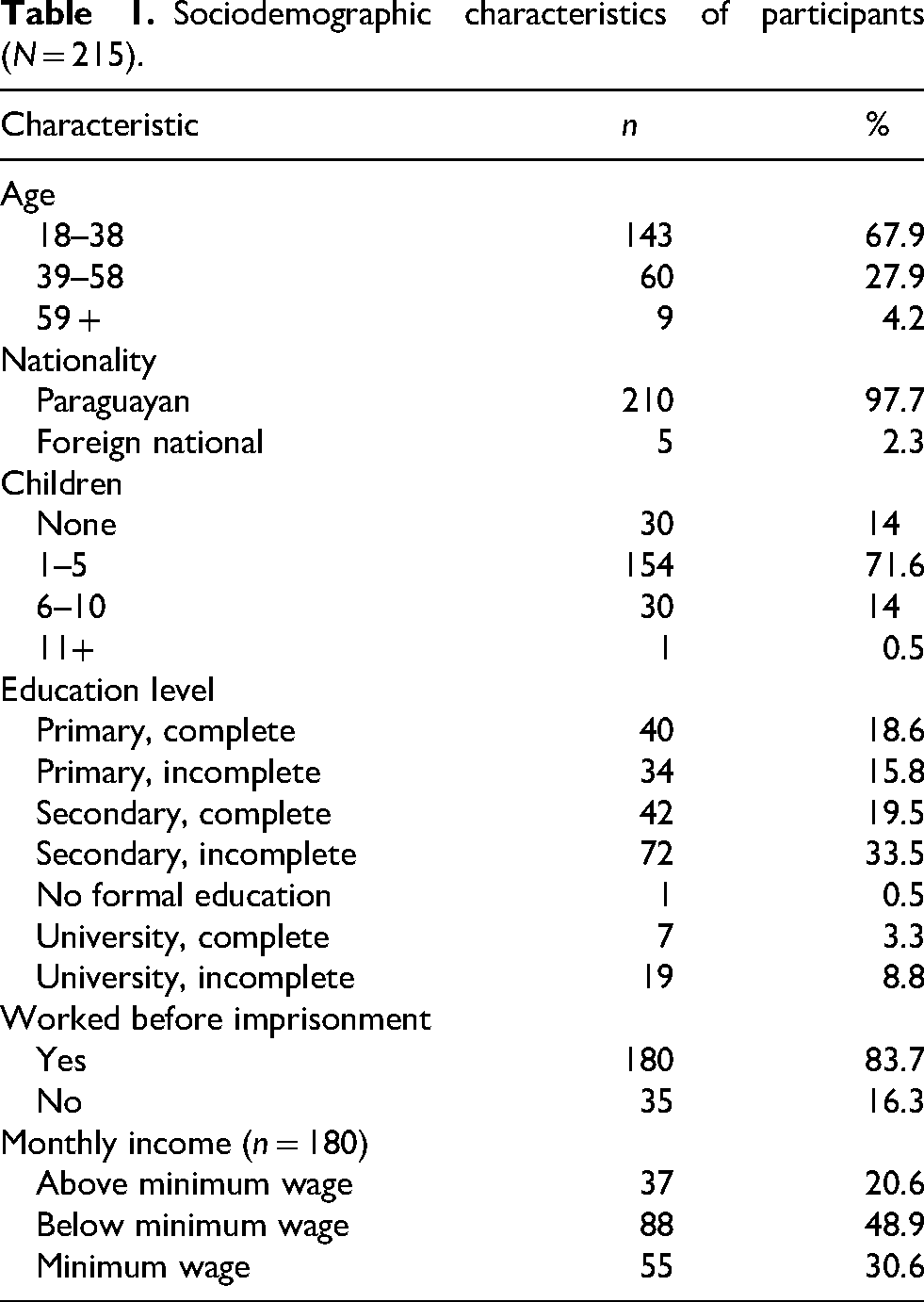
A total of 215 women aged between 18 and 69 years were included, with a mean age of 34.67 ± 11.3 years. The most common age range was 18–38 years (67.9%). The majority were Paraguayan, and none belonged to an indigenous group. Of the participants, 86% had children, 33.5% had incomplete secondary education, 83.7% had worked before imprisonment, and 48.9% had earned less than the minimum wage (Table 1).
Sociodemographic characteristics of participants (N = 215).
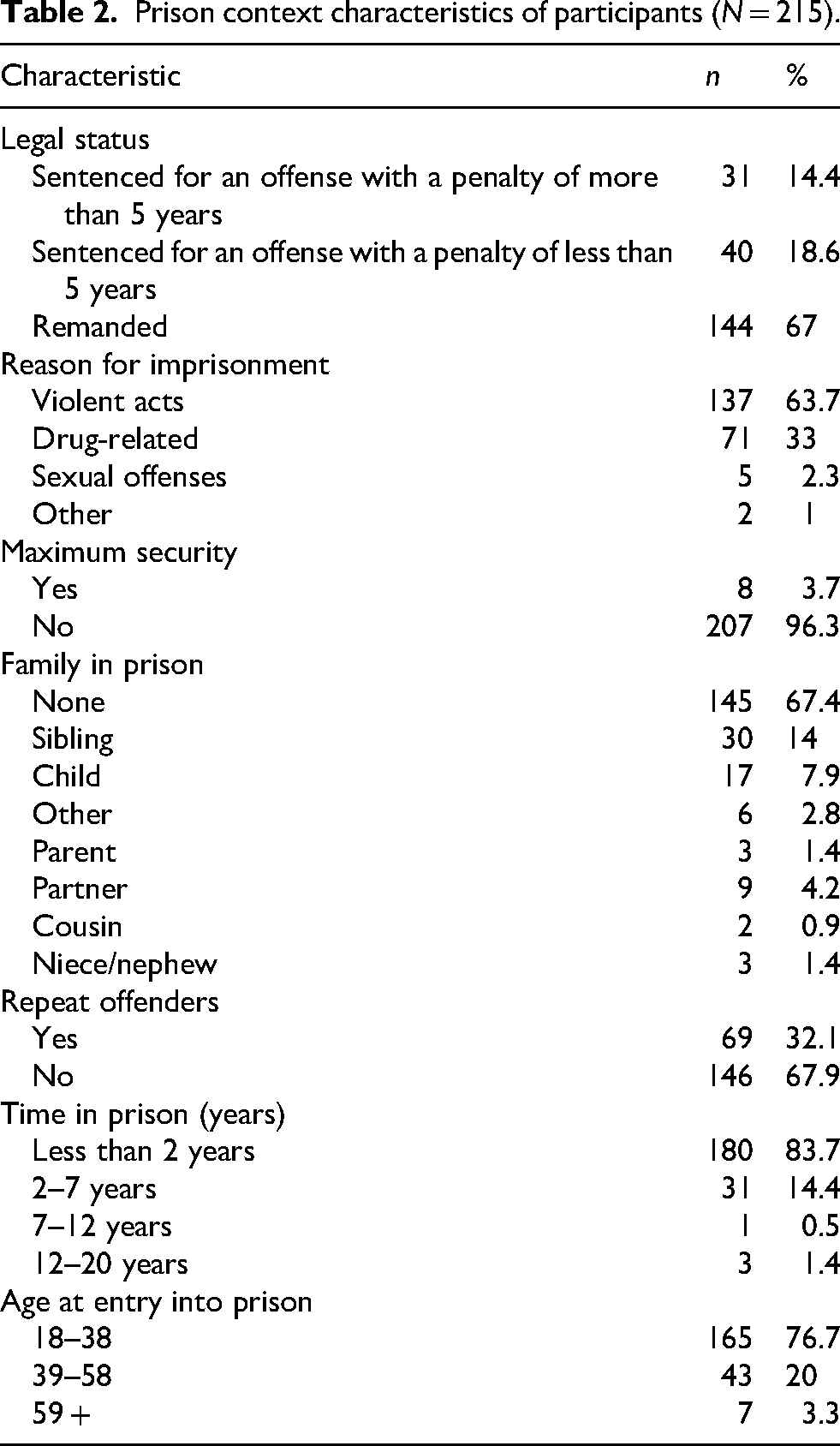
Of the total sample, 67% had not yet been sentenced, 63.7% were imprisoned for violent acts, and 3.7% were placed in a maximum security unit. Of the participants, 67.4% did not have a family member in prison and 32.1% were repeat offenders. The age of entry into prison ranged from 18 to 66 years, with a mean of 31 ± 11.5 years. The most common age range was 18–38 years. Time in prison ranged from 1 month to 20 years, with a mean of 1.42 ± 2.3 years, with less than 2 years being the most frequent time. Table 2 presents the detailed prison context characteristics of the participants.
Prison context characteristics of participants (N = 215).
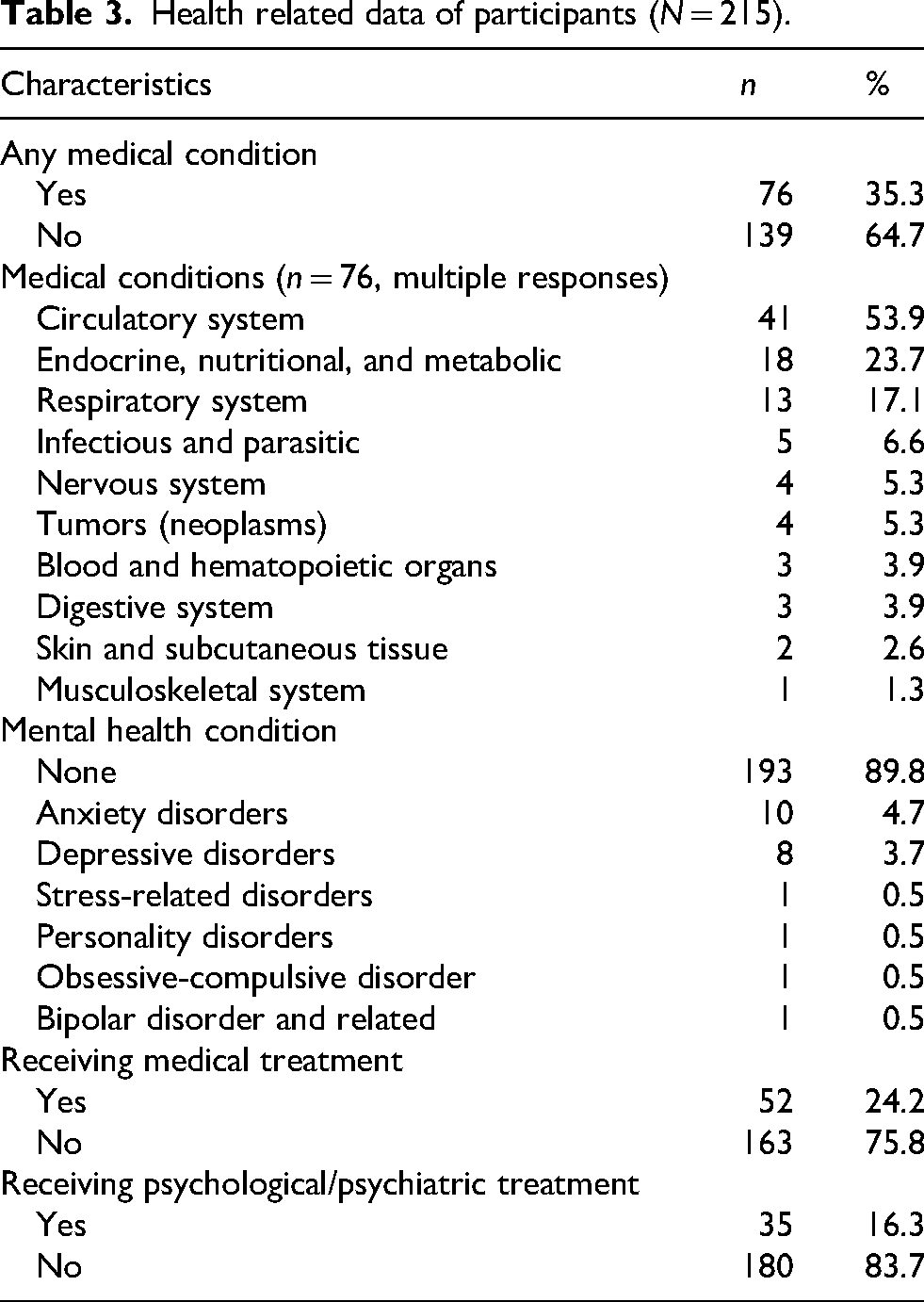
Among the participants, 35.3% had a medical condition, with the most frequent being circulatory system issues (53.9%). Furthermore, 10.2% had a previous mental health diagnosis, with the most common being an anxiety disorder (4.7%). Of the participants, 24.2% were receiving medical treatment and 16.3% were receiving psychological or psychiatric treatment (Table 3).
Health related data of participants (N = 215).
Regarding mental health variables, 40% of the participants were at some level of suicide risk according to the C-SSRS. Alcohol consumption was reported by 36.7% of the participants, and of these, 59.5% screened positive for alcohol-related problems (alcohol subscale of MULTICAGE CAD-4 ≥ 2). Furthermore, 45.6% of the participants used drugs, with 73.5% screening positive for drug-related problems (drug subscale of MULTICAGE CAD-4 ≥ 2). According to the SCL-90-R, the most frequent symptom dimension was depression (23.7%), followed by somatization (21.4%). The total number of positive symptoms ranged from 3 to 78, with a mean of 33.7 ± 13.5. Of the participants, 37% exaggerated their symptoms, and 0.5% attempted to present a positive image. The PSDI ranged from 1.3 to 3.6, with a mean of 2.5 ± 0.5. In addition, 7.5% of the participants presented either extreme dramatization or dramatization. The GSI ranged from 0.1 to 2.9, with a mean of 1 ± 0.5 (Table 4). These scores were interpreted descriptively, without applying SCL-90-R caseness thresholds (e.g., T-scores ≥63), 14 as our objective was to characterize the prevalence of symptom dimensions rather than establish clinical diagnoses.
Mental health variables of participants (N = 215).

Note. SCL-90-R = Symptom Checklist-90-Revised; C-SSRS = Columbia Suicide Severity Rating Scale.
Alcohol-related problems defined as ≥2 affirmative responses on the alcohol subscale of MULTICAGE CAD-4.
Drug-related problems defined as ≥2 affirmative responses on the drug subscale of MULTICAGE CAD-4.
Multiple responses possible.
Statistically significant associations were found between the SCL-90-R symptom dimensions and the other variables. Having a medical condition was statistically significant for the somatization dimension, with an OR of 2.45 (χ² = 7.25, df = 1, p = .007), suggesting it as a risk factor.
Age at entry into prison was associated with the SI dimension. Individuals who entered prison between the ages of 18 and 38 years were more than nine times more likely to receive the diagnosis than those between 39 and 59 years or older (OR = 9.16, χ² = 6.61, df = 1, p = .01). Alcohol consumption was associated with an increased risk of depression (OR = 2.18, χ² = 5.83, df = 1, p = .016) and drug use was associated with anxiety (OR = 2.6, χ² = 5.37, df = 1, p = .020).
The hostility dimension was associated with several risk factors. Younger age at entry into prison (18–38 years) was linked to a higher risk compared to those aged 39 years or older (OR = 14.6, χ² = 11.43, df = 1, p = .001); working prior to imprisonment (OR = 2.5, χ² = 4.97, df = 1, p = .026); imprisonment for violent acts (OR = 3.1, χ² = 6.92, df = 1, p = .009); imprisonment for drug-related offenses (OR = 2.6, χ² = 4.89, df = 1, p = .017); recidivism (OR = 2.1, χ² = 4.32, df = 1, p = .038); alcohol use (OR = 2.7, χ² = 7.92, df = 1, p = .005); and drug use (OR = 2.9, χ² = 6.49, df = 1, p = .011).
Having a medical condition was associated with the FOB dimension (OR = 3.74, χ² = 6.96, df = 1, p = .008) as was alcohol use (OR = 4.69, χ² = 9.1, df = 1, p = .003). Paranoid ideation dimension was associated with working before imprisonment (OR = 2.7, χ² = 6.27, df = 1, p = .012), alcohol use (OR = 2.69, χ² = 8.16, df = 1, p = .04), and drug use (OR = 2.4, χ² = 6.49, df = 1, p = .011).
Suicide risk, as evaluated by the C-SSRS, was associated with alcohol use (OR = 2.37, χ² = 9.018, df = 1, p = .03), drug use (OR = 2.54, χ² = 10.88, df = 1, p < .001), somatization (OR = 4.29, χ² = 18.29, df = 1, p < .001), obsessions and compulsions (OR = 9.6, χ² = 6.3, df = 1, p = .012), SI (OR = 5.29, χ² = 14.93, df = 1, p < .001), depression (OR = 10.89, χ² = 45.45, df = 1, p < .001), anxiety (OR = 9.61, χ² = 25.53, df = 1, p < .001), hostility (OR = 5.18, χ² = 20.07, df = 1, p < .001), FOB (OR = 8.19, χ² = 13.79, df = 1, p < .001), paranoid ideation (OR = 4.31, χ² = 16.89, df = 1, p < .001), and psychoticism (OR = 4.61, χ² = 15.75, df = 1, p < .001).
Discussion
Main findings
Our results indicate that the prevalence of mental disorders among incarcerated women is considerably high, particularly when considering the multiple associated factors identified in this study. This is consistent with global research, which shows that female prisoners experience significantly higher rates of mental health issues–for example, up to five times more than the general population.9,10 Research indicates that incarceration, social marginalization, and prior trauma significantly contribute to the deterioration of mental health among incarcerated women.26,27 Pre-incarceration living conditions, such as low educational levels and incomes below the minimum wage, are key determinants that not only limit life opportunities but also correlate with greater psychological vulnerability within the prison environment.26,28
Comparison with previous literature
In our study, the high proportion of women who were employed prior to incarceration but earned insufficient incomes highlights that these women were already entrenched in economic and social precariousness, which likely exacerbated their mental health problems.29,30 This finding is consistent with previous research on Latin American prisons, where women face significant socioeconomic and psychological challenges. 31 Furthermore, the prevalence of substance use in our study (45.6%) exceeds that reported in European contexts (35%), indicating that the South American context may be associated with higher substance use risks. 32
The lack of adequate mental health resources in prison settings exacerbates these challenges, as documented in studies in other Latin American countries. 33 Insufficient access to mental health services and trained professionals contribute to the worsening of mental health symptoms, such as depression and anxiety, as observed in this study. Evidence from other regions, including the USA and Europe, suggests that improving access to mental health services in prisons not only enhances psychological well-being but may also reduce recidivism rates.34,35 Therefore, our findings highlight the urgent need to integrate mental health programs into the Paraguayan prison system, in alignment with the recommendations of the World Health Organization. 35
Suicide risk and associated factors
One of the most alarming findings of this study was the high risk of suicide, with 40% of the participants presenting some level of suicide risk. This figure aligns with international studies showing elevated suicide rates among incarcerated populations, particularly among women. 36 Suicidal ideation and attempts at prison are often associated with pre-existing mental health issues, the trauma of incarceration, and the isolation and stress that prison life induces.37,38 Our findings also showed that women with depression were nearly five times more likely to exhibit suicidal tendencies, reinforcing the well-established link between depressive disorders and suicide risk. 36 The significant relationship between substance use and suicide risk identified in this study further highlights the complex interplay between mental health and addiction in prisons. Research has consistently shown that substance abuse exacerbates the risk of suicide, especially in vulnerable populations, such as incarcerated women. 39 Given that 73.5% of the women who used drugs in our study did so problematically, it is critical to address substance use disorders as part of suicide prevention strategies in prison settings.
Other correlates of mental health
Age also plays a critical role in mental health outcomes, as our study showed that younger women entering prison exhibited greater vulnerability to hostility, psychoticism, and SI. This vulnerability could be attributed to a lack of coping mechanisms and the significant impact of incarceration during critical developmental phases.40,41 The literature supports the notion that younger individuals face greater challenges in adapting to prison life, particularly if they have not experienced prior long-term confinement, as younger inmates are more prone to anxiety and hostility, which are responses to perceived threats in hostile prison environments. 42 Additionally, anxiety and hostility may be interpreted as adaptive responses to perceived threats in the prison environment, a situation exacerbated by legal uncertainties faced by many women who had not yet been sentenced at the time of this study.43,44 This suggests that judicial reforms aimed at expediting legal processes can alleviate the psychological burden associated with prolonged detention.
Our findings also demonstrated a strong correlation between problematic substance use and mental disorders, with more than 45% of women reporting drug use, most of which were problematic. This relationship is bidirectional; substance use can be a risk factor for developing mental disorders, particularly anxiety and depression, while mental disorders can lead to increased substance use as a coping mechanism.45,46 Harm-reduction programs, including cognitive-behavioral therapy (CBT), have proven effective in addressing both substance use and mental health issues in prison settings. 47
The prevalence of physical illnesses among incarcerated women, with over 35% reporting medical conditions, emphasizes the importance of considering physical health in the assessment of psychological wellbeing. The statistically significant relationship between physical illnesses and somatization and anxiety symptoms illustrates the complex interaction between mental and physical health in this population. 48 Previous research has established that untreated physical health conditions in prisons exacerbate mental health problems, creating a vicious cycle of deteriorating health. 36 In our study, the lack of access to adequate healthcare in the prison system was a significant concern, echoing findings from other contexts in which limited healthcare access increases both physical and psychological distress. 49
Recidivism, observed in 32% of the participants, was another crucial factor. The association between recidivism and mental health, particularly hostility, should be explored further in terms of how a lack of mental health care and reintegration services can contribute to reoffence. Research has shown that individuals with mental health problems such as anxiety and post-traumatic stress disorder (PTSD) are at a higher risk of recidivism. 50 These findings underscore the need for continuous mental health support in prisons and post-release to reduce the likelihood of reoffence and improve long-term outcomes. Prison systems must develop post-release programs that offer psychological services and reintegration support to reduce recidivism rates, especially for those with high levels of hostility and aggression. 51
Strengths and limitations
This study has several notable strengths. The use of well-validated psychometric tools such as the SCL-90-R, C-SSRS, and MULTICAGE CAD-4 ensured that mental health symptoms, suicide risk, and substance use disorders were assessed with high reliability. This study's focus on incarcerated women in Paraguay, an under-researched population, is a key strength that contributes valuable data to the limited literature on this group. Additionally, random sampling and a large sample size (N = 215) enhance the generalizability of the findings within the specific context of the Paraguayan prison system.
However, this study has some limitations. The cross-sectional design precludes the establishment of causal relationships between variables, limiting the ability to infer whether certain factors such as substance use directly contribute to mental health outcomes. The reliance on self-reported data may also introduce response bias, as participants might under-report or exaggerate symptoms due to stigma or perceived benefits within the prison environment. Furthermore, the study was conducted in a single prison, which may restrict the generalizability of the results to other correctional facilities or regions in Paraguay.
Implications for practice and policy
Based on these findings, there are several practical steps that could improve the mental health of incarcerated women in Paraguay. First, implementing routine mental health screening upon entry and periodically during incarceration could help identify those at risk for mental health and substance use disorders. Suicide prevention programs that incorporate both psychological support and substance use treatment are essential given the high suicide risk observed in this population. CBT should be introduced as part of standard care, focusing on mental health and substance use simultaneously. Additionally, training prison staff to recognize mental health problems and provide psychological first aid would enable early intervention and support for those in distress. Together, these measures could significantly reduce psychological distress and suicide risk, while promoting healthier reintegration pathways for incarcerated women.
Conclusions
This study provides a comprehensive view of the mental health challenges faced by incarcerated women in Paraguay. Our data suggest that younger women and those with a history of substance use are particularly vulnerable. Addressing both physical and mental health issues in prisons is critical, particularly when designing interventions that target suicide prevention and substance abuse treatment. Integrating mental health care into prison systems as well as offering post-release support could significantly improve well-being and reduce recidivism. Further longitudinal studies and research in various correctional settings are needed to deepen our understanding of these issues and refine intervention strategies.
Footnotes
Acknowledgements
We would like to extend our gratitude to Yenny Soledad Delgado Vázquez, Director of the Women's Penitentiary Center Buen Pastor, for her invaluable support and collaboration throughout this study.
Ethics approval and consent to participate
This study was conducted within the framework of the Scientific Research Improvement Program of the Research Group on Epidemiology of Mental Disorders, Psychopathology, and Neurosciences and received approval from the Department of Medical Psychology of the School of Medical Sciences, National University of Asunción, Paraguay (Reference 001-006-2024). All participants provided written informed consent prior to participation. Data were handled with strict confidentiality, equality, and justice, in accordance with the principles of the Declaration of Helsinki.
Authors’ contributions
J.T., G.V., G.E., and I.B. conceived and designed the study, and contributed to data analysis and interpretation. JT., P.R.M., G.A., ADT-R., and M.O. drafted the manuscript and conducted the literature search. G.V., D.A., N.L., and S.G. performed participants’ assessments. A.F., T.C.R., A.V., and J.M.C.M. critically revised the manuscript for important intellectual content. All authors approved the final version of the manuscript. All authors meet the ICMJE authorship criteria and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by the National Council of Science and Technology of Paraguay (Consejo Nacional de Ciencia y Tecnología – CONACYT) under its PROCIENCIA program (Project Code: PINV01-899). The funding body had no role in the design of the study, data collection, analysis, interpretation of data, writing of the manuscript, or decision to submit for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Julio Torales is the guarantor of this work. He accepts full responsibility for the integrity of the study, had access to all the data, and controlled the decision to publish.