
Abstract
Accurate identification and evaluation of spinal column injuries in post-mortem settings are crucial for forensic investigations. While traditional autopsies have long been the gold standard, post-mortem computed tomography (PMCT) has emerged as a promising non-invasive and beneficial tool. This systematic review aims to compare the findings of PMCT scans with autopsies in cases of spinal column injuries. Out of 428 articles screened, 11 studies matched the inclusion criteria. PMCT was superior in visualizing fractures in the atlas, axis, and upper cervical spine compared to autopsies. Moreover, PMCT demonstrated efficacy in detecting spinous and transverse process fractures, which are often overlooked in conventional autopsies, but also had limitations in identifying intervertebral injuries and determining the timing of injuries; in addition, the presence of degenerative changes could mask certain fractures. Autopsy demonstrated superiority in detecting dislocations in the craniocervical region and specific types of intervertebral separation. In conclusion, combining both PMCT and autopsy yields more accurate results. Autopsy remains the gold standard, particularly in cases where clearly visualized fractures or injuries are not evident on PMCT scans. Further research and standardization of protocols are warranted to optimize the diagnostic capabilities of both approaches in spinal column injury assessments.
Keywords
Introduction
Spinal column injuries may be associated with spinal cord injuries and death could result from different immediate causes, including pneumonia, septicemia, and pulmonary embolism. Notably, the extent to which these causes can lead to death differs between cases of quadriplegia and paraplegia. 1 This entity mainly results from trauma caused by motor vehicle accidents (MVA), including pedestrian injuries, falls, and, less frequently, sporting accidents. 2 Yeo et al. 2 have retrospectively analyzed 1453 spinal cord injured patients, concluding that patients with quadriplegia had a life expectancy of 70% of the normal population.
Post-mortem computed tomography (PMCT) has been progressively employed in the field of forensic pathology. Yet, autopsy remains the gold standard as it encompasses the act of anatomical dissection as well as collection of samples for ancillary investigations. However, its use in certain settings has recently declined as it is an invasive approach,3,4 while PMCT cannot analyze microbiological, toxicological, or histological aspects, it is highly effective for detecting spinal fractures, ligamentous injuries, and disc tears.3,5 The usefulness of PMCT is explained in its non-invasiveness, fast acquisition, providing detailed anatomical location, and easily accessible digital data. 4 PMCT when used as an adjunct to autopsy can lead to increased identification of fractures of the spine. 6 To our knowledge, the findings of PMCT scans in spinal column-injured patients in comparison to conventional autopsies have not been widely examined in systematic reviews. The present systematic review aims to explore PMCT findings of spinal column injuries in comparison to autopsy.
Methodology
A systematic search of the literature was conducted to identify studies that examined PMCT findings in spinal column injuries compared to autopsy using the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 7
Criteria for inclusion
To be eligible, articles were selected based on the following criteria: (1) inclusion of post-mortem investigation, (2) comparison between autopsy and PMCT scans, and (3) related to spinal column injuries. Additionally, the selected studies aimed to determine the cause of death and/or major injury, and the patients included were defined as trauma victims, wherein trauma referred to a physical injury or wound caused by an external force.
Criteria for exclusion
The following criteria were used to exclude articles: (1) studies that included non-human subjects, (2) studies that mentioned other radiological findings without separating the data, (3) case reports, (4) case series, (5) reviews, (6) experimental studies, (7) foreign-language studies that were not translated into English.
Assessment of study quality
Two independent researchers evaluated the quality of the selected articles to be included using the Joanna Briggs Institute (JBI) critical appraisal tool, 8 which consists of items that reflect the possible sources of bias. No discrepancies between the appraisals of the two independent researchers were found.
Search strategy
A systematic search of the Web of Science and PubMed databases was conducted in March 2024 to identify the relevant literature. The search utilized the following search terms: (“postmortem” [Title/Abstract] OR “post-mortem” [Title/Abstract] OR “autopsy” [Title/Abstract] OR “dissection” [Title/Abstract]) AND (“CT findings” [Title/Abstract] OR “computed tomography” [Title/Abstract] OR “radiological” [Title/Abstract] OR “CT” [Title/Abstract] OR “radio*” [Title/Abstract]) AND (“spinal cord injury” [Title/Abstract] OR “spine injury” [Title/Abstract] OR “spinal column injury” [Title/Abstract] OR “spinal injury” [Title/Abstract]). The search yielded a total of 428 articles, which were de-duplicated using Rayyan Software (Rayyan Systems Inc) to 342. Four independent researchers reviewed full-text articles for eligibility, and in case of disagreement, two other independent researchers were consulted. Lastly, 11 articles that matched the inclusion criteria were incorporated into the final review (Figure 1). There were no restrictions on the age of the victim or the publication year.

PRISMA flow diagram demonstrating the systematic search strategy.
Results and discussion
Out of 428 articles screened, 11 aligned with the inclusion criteria and were added in this systematic review (Table 1).4,6,9–17 Some of the studies limited their observations to the cervical spine4,9,14,16,17; others involved two or more segments of the spine.6,10–13,15
Overview of the included studies.
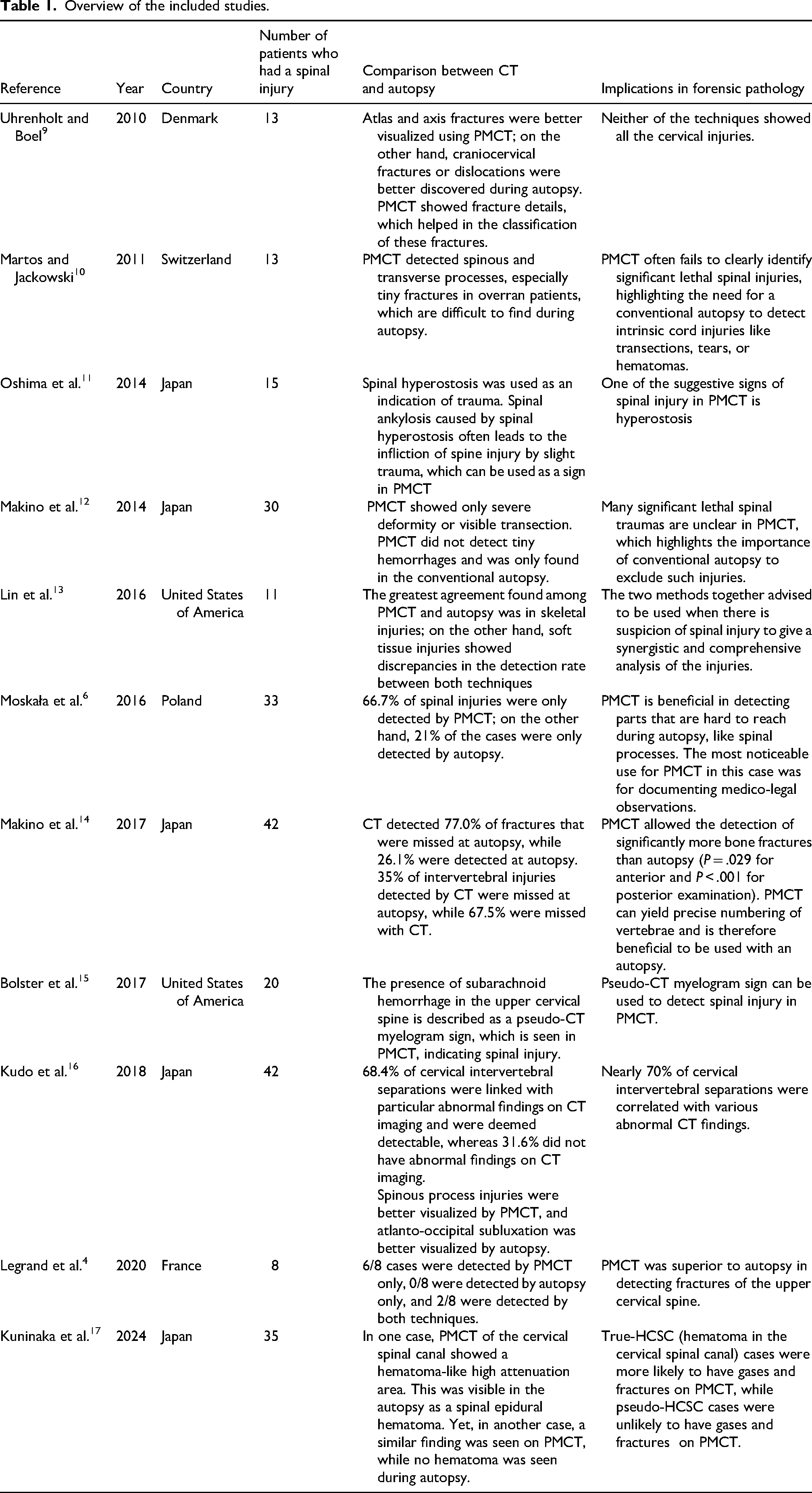
Some studies involved multiple forms of trauma,4,9,11–16 and some focused only on motor vehicle accidents.6,10 Martos and Jackowski 10 showed that computed tomography (CT) helps to discover overrun accidents due to better visualization of tiny bilateral fractures in spinous and transverse processes.
The use of PMCT is becoming more common in the field of forensic pathology. In 1983, a diving casualty was the first documented case of PMCT. 18 The use of PMCT has increased in recent years; however, autopsy continues to be the gold standard for post-mortem assessment. 4 PMCT is recommended for routine post-mortem examinations of trauma victims and has been proposed as a substitute for conventional autopsy in cases when it is not available or refused.4,19
While some authors contend that the gold standard for establishing the cause of death should be a mix of PMCT and autopsy, PMCT should be utilized as an added aid rather than a substitute for autopsy, as it can identify additional injuries that are difficult to detect and sometimes overlooked in conventional autopsies. Nevertheless, by combining autopsy and PMCT, the determination of the cause of death can be more precise compared to relying on just one of these methods.14,20–23
Among the benefits of PMCT are its speed and non-invasive nature. 4 Even so, it requires a significant investment for both the purchase and operation of the CT scanner, as well as specialized training. 24
In this systematic review, some studies were found to favor the use of PMCT.
Studies that favor PMCT over autopsy
Assessing cervical spine injury at autopsy can be challenging due to the complex anatomy involved. PMCT is especially useful for examining these difficult-to-access areas, such as the spine.4,6,13,14
Martos and Jackowski 10 supported that CT is better at detecting spinous and transverse process fractures due to the tendency of these fractures to be small and distal, and easily overseen in conventional autopsy. That is also narrated in another study by Moskala et al. 6 where 66.7% of the spinal injuries were only seen by CT; however, 21% were only positive in conventional autopsy for those who had an intervertebral disc injury without change in spine axis. Legrand et al. 4 also supported that PMCT was more accurate regarding upper cervical spine fractures.
Cervical spine injuries are the most common type of spinal trauma. 25 These lesions might be elusive and challenging to detect during an autopsy. Moreover, undisplaced fractures and the absence of bleeding can sometimes mask upper cervical injuries.9,21 CT scans can accurately depict them. 20
Still, numerous cervical spine injuries may go unnoticed, such as a tear in the intervertebral disk, posterior ligament injuries, or a partial fracture of the vertebral bone without dislocation.14,21 Additionally, while PMCT can detect bone fractures, it is unable to determine if the injury was sustained while the individual was still alive or not, due to the inability to accurately visualize blood in the surrounding connective tissues or muscles. Furthermore, cervical spine injury might occasionally resemble subarachnoid hemorrhage resulting from a ruptured cerebral artery aneurysm. In such cases, an autopsy of the neck may be necessary even if PMCT reveals a subarachnoid hemorrhage. 21
Makino et al. 14 found that the spinal bone fractures found only by CT were significantly higher than those only found by autopsy, 77% and 26.1%, respectively. On the other hand, autopsy was better than CT for detecting intervertebral injuries, 67.5% and 35%, respectively.
Bolster et al. 15 showed that PMCT is better for detecting spinal injuries, specifically upper cervical ones, where the sensitivity was 92.86% for detecting atlanto-occipital joint injury, and 100% for detecting atlantoaxial joint injuries. Also, they documented that a case that had spinous process fractures from C6 to T1 was not recognized as a spine injury during autopsy. As an extra benefit of PMCT in cervical injury, it helped in the fracture classification, giving more information regarding the injury and its mechanism. 9 Nevertheless, one study has demonstrated that PMCT has limitations in detecting anterior cervical spine fractures. 14
Finally, PMCT scans did not accurately show minor hemorrhages. 20
The detection of anterior and posterior subluxation of the cervical spine is affected by the position of the neck when the image is taken. PMCT cannot identify subluxated vertebrae, 21 at least not without positioning the neck appropriately first. 23
Therefore, in certain studies discussed below, conventional autopsy is still the preferred choice for post-mortem investigations.
Studies that favor autopsy over PMCT
Despite the complexity of spine anatomy, each region is characterized by a unique structure, plus the ligaments and muscles covering the spine. Performing an autopsy remains an integral part of forensic investigations as proposed by Uhrenholt and Boel 9 Yet, careful and complete dissection technique of the spine is not frequently performed during autopsy unless a strong suspicion of spinal cord injury (SCI) has been established based on the condition of the body and/ or external findings. 17
Uhrenholt and Boel 9 reported 3 cases out of 13 with cranio-cervical dislocation/fractures that were better visualized by autopsy rather than PMCT, which can be attributed to the advantage of manually examining the stability of the spine during autopsy, unlike PMCT. Hence, failing to detect such significant findings via radiological investigations alone could diminish the accuracy of the investigation.
Despite the high sensitivity of PMCT in detecting atlanto-occipital and atlantoaxial joint injuries, 92.86% and 100%, respectively, as reported by Bolster et al., 15 one case of atlanto-occipital subluxation was missed upon radiological assessment.
Kudo et al. 16 studied the association between findings of PMCT and autopsy of patients with intervertebral separation. It showed that only 70% of autopsy-proven cervical intervertebral separation was associated with abnormalities in PMCT, namely: intervertebral gas, backward intervertebral widening, forward intervertebral widening, anteroposterior misalignment, spur fracture, and hematoma anterior to the vertebral body. The first sign is the most common one, and is attributed to the vacuum phenomenon caused by external force allowing gas entry to intervertebral separations. 26 The remaining 30% were not detectable by PMCT. Several studies have shown the insufficiency of using PMCT solely, suggesting the incorporation of both methods for a greater level of precision.11,12,14
The imperative role of the autopsy has been highlighted by Kuninaka et al. 17 and Makino et al., 12 stating that an autopsy is needed in some cases where clearly visualized fracture or injury is impossible to see and only hematomas are present, as it could lead to misdiagnosing the cause of death in such cases. 17 Some spinal injuries can potentially have normal PMCT findings; among 30 deceased who were previously determined to have SCI via autopsy, the incidence reached up to 20%. This is also known as spinal cord injuries without radiographic abnormalities (SCIWORA), which is more associated with disc injuries and peri-vertebral hemorrhage rather than fractures. As a consequence, it hinders the detection of traumatic deaths. Especially when there are ambiguous death circumstances, which ultimately necessitate a conventional autopsy. It has been considered that ossification of the posterior longitudinal ligament, ossification of the ligamentum flavum, and cervical spinal stenosis serve as predisposing factors to SCIWORA, as they were seen in 67% of cases. 12 Association of SCIWORA with disc injuries rather than fracture proves limited PMCT precision in detecting soft tissue injuries.12,13
Signs in PMCT
In our systematic review, we encountered studies that reported specific signs indicating SCI, such as bilateral spinous and transverse processes could be a specific sign in overrun victims that are mostly seen in CT rather than autopsy, as mentioned above. 10
PMCT hyperostosis could be a sign of spine fractures that could not be seen clearly due to the absence of dislocation in CT, as 14 cases out of the 25 positive hyperostosis cases had spinal injury, and only one patient who had spinal injury had a negative hyperostosis sign in the control group. 11 That supports the association between hyperostosis and spinal fracture. However, Makino et al. 14 showed that some bone fractures, especially anterior cervical spine ones, can be masked by degenerative hyperostotic changes.
Bolster et al. 15 showed that pseudo-CT myelogram sign (PCMS) could indicate a spinal injury. Localized subarachnoid hemorrhage in the upper cervical spine was specifically reported in this article. Kuninaka et al. 17 found that pseudo-hematoma in the cervical spinal canal (pseudo-HCSC) can be seen in PMCT in cervical spine injury cases where there are no fractures and gases; however, they supported the need for confirmation by autopsy in such cases. The hypothesis behind this is that epidural vascular congestion after the injury gives a hematoma-like appearance in PMCT.
Some studies investigated the presence of intervertebral gas as a diagnostic clue for cervical intervertebral separation.16,27
Several studies reported how limited PMCT is in detecting spinal findings compared to autopsy. Multiple factors could implicate imaging interpretation, such as post-mortem changes, 28 intervals between the onset of injury, medical intervention, autopsy, 13 and changes of deceased position during transport. 6 Thus, a thorough understanding and comparison between antemortem CT and autopsy findings with post-mortem radiological features is crucial for accurate interpretation. 13
Conclusion
The comparison between traditional autopsies and PMCT scans in cases of spinal column injuries reveals that neither technique alone identified all spinal injuries comprehensively. While PMCT excelled in visualizing certain fractures like those in the atlas, axis, and upper cervical spine, it had limitations in detecting intervertebral injuries and determining injury timing. On the other hand, traditional autopsies were superior in detecting specific types of intervertebral separation and dislocations in the craniocervical region. Combining both methods provides a synergistic result, enhancing the accuracy of identifying spinal injuries. Traditional autopsies remain the gold standard, especially when clearly visualized fractures are not evident in PMCT scans.
PMCT scans’ speed and non-invasiveness make it a valuable tool, but require specialized training and significant investment. While PMCT can detect certain injuries that may be overlooked in traditional autopsies, it may not always provide a complete assessment, necessitating the use of both techniques for a comprehensive evaluation of spinal injuries.
The limitations of this systematic review include the restriction to only two databases, Web of Science and PubMed. While these databases are widely recognized, incorporating additional databases could have ensured a more comprehensive retrieval of relevant literature. Moreover, the included studies had limitations such as small sample size, retrospective design, unknown effects of post-mortem circumstances on imaging, and the potential for missed injuries due to the lack of standardized procedures. Also, while PMCT detected fractures missed by autopsy, this may reflect selective spinal examination in severe trauma cases rather than autopsy limitations. Standardized protocols ensuring complete spinal dissection regardless of other findings would strengthen future comparisons.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.