
Abstract
The occurrence of Wischnewski spots in fatal hypothermia has been considered an important indicator of reduced core temperatures, its incidence varying between 40 and 100%. Though many human and animal studies have been conducted to study this phenomenon, the underlying mechanisms contributing to the formation of Wischnewski spots are still not clearly understood. They have been largely reported in human deaths occurring from exposure to freezing temperatures. This is the first reported case of Wischnewski spots observed in a case of fatal burns.
Introduction
Wischnewski spots were first reported as gastric or duodenal haemorrhages by Wischnewski in 1895. 1 Since then, the presence of these spots have been considered a classical indicator of reduced core temperatures. Observations in human and animal studies, however, have shown variable results in this regard, with the occurrence of Wischnewski spots in hypothermic deaths ranging between 40 and 100%.2–6 Researchers have therefore considered other factors that may lead to the occurrence of these spots. Stress as a contributing factor has been considered by many. Researchers have attempted to correlate the occurrence of gastric erosions under varied conditions of stress alone, hypothermia alone and hypothermia with stress. These experiments conducted on animal models, however, have been inconclusive.7–10
Despite the variability of its incidence as observed in hypothermic deaths and inconclusive studies on animal models, these spots are considered characteristic, or at least an important indicator, of hypothermia. In human fatalities, these spots have been largely reported in deaths occurring from exposure to freezing temperatures. We report a case of fatal burns where Wischnewski spots were observed at autopsy. To the best of our knowledge, this is the first reported case of Wischnewski spots being observed in a case of fatal burns.
Case report
A 40-year-old man was brought to the primary health centre (PHC) after having sustained near-fatal burn injuries involving approximately 90% of the total body surface area (Figure 1). The incident happened after midnight in a rural part of coastal South India from a fire accident caused by a kerosene lamp that gutted the hut where the victim was sleeping. The victim was administered first-aid at the PHC and shifted to the nearest district hospital, about 200 km away from the PHC; he was pronounced dead on arrival at the hospital. Thus, the survival period was a few hours. At autopsy, the scalp and facial hair of the deceased were burnt and singed. Carbonaceous (soot) deposits were found on the anterior teeth and trachea. The stomach contained watery liquid with scanty carbonaceous particles dispersed in it. Diffuse, oval to circular, dark brown-black punctate lesions, measuring about 1 × 1 mm to 3 × 2 mm in size, were observed all over the gastric mucosa (Figure 2). These lesions appeared similar to Wischnewski spots described in the literature. All other internal organs appeared congested on cut section. Death was attributed to fatal accidental burns sustained as a result of a house fire.
Distribution pattern for burns in the male victim (approximately 90% total body surface area involvement). Wischnewski spots on the gastric mucosa as observed in a case of fatal burns.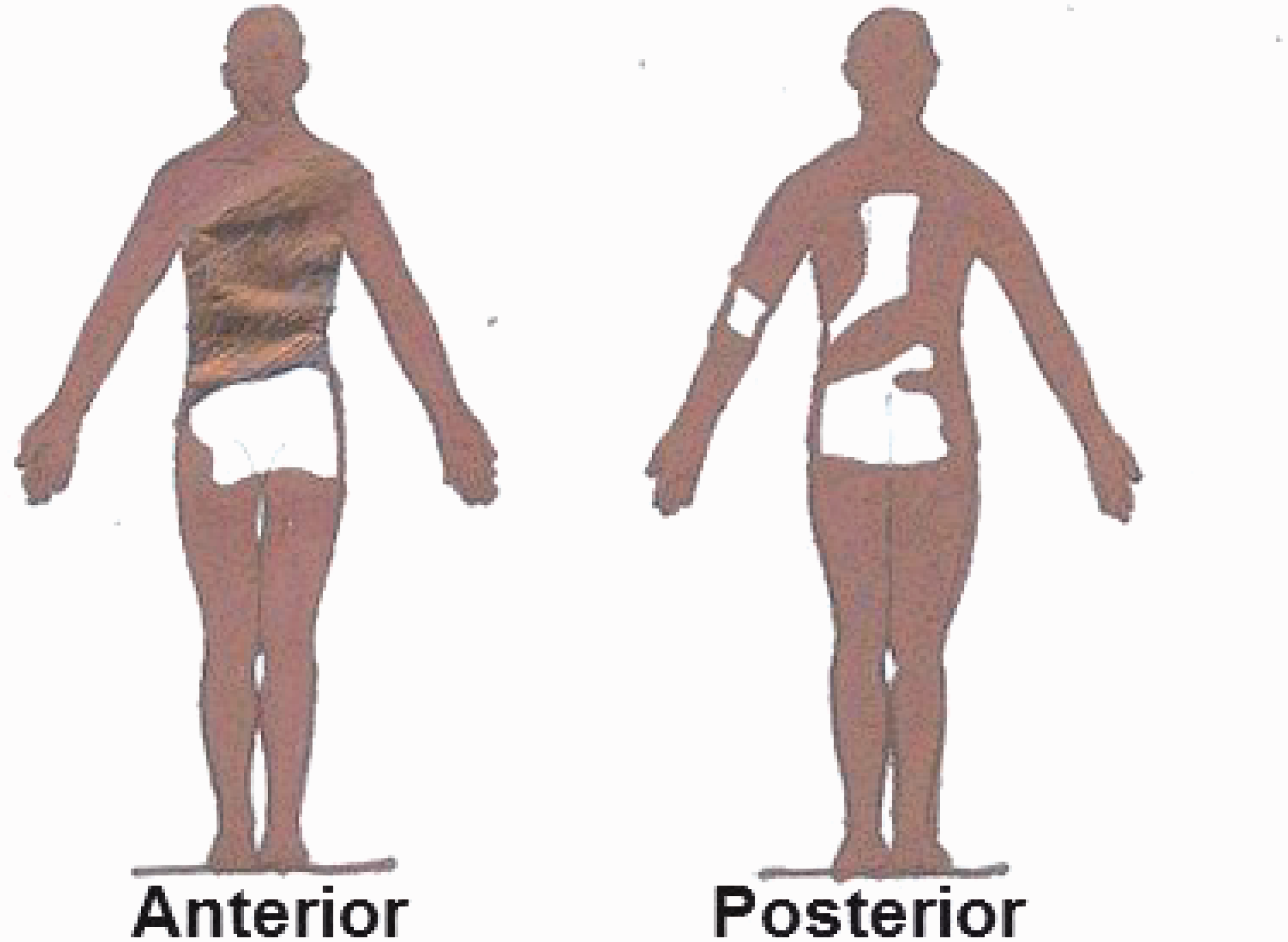

Discussion
Wischnewski spots are described as haemorrhagic spots on the gastric mucosa. In forensic literature, they have been regarded as highly indicative or supportive of fatal hypothermia. Wischnewski reported the presence of these spots in 91% of cases of hypothermia. 2 Later, Mant 4 observed these spots in 86%, Haba et al. 5 in 87% and Mizukami et al. 6 in 43.5% of the diagnosed cases of hypothermia. A recent study conducted by Bright et al. 3 on two different human populations showed the presence of these spots in 92% and 100% cases diagnosed with hypothermia. Further, isolated cases of the presence of Wischnewski ulcers are reported in accidental hypothermia among hospitalised patients 11 and in partially mummified bodies. 12
The underlying mechanisms contributing to the formation of Wischnewski spots are still not clearly understood. Wolf et al. 11 theorised the presence of cold-induced mucosal ischaemia, followed by collapse of thermoregulatory mechanisms causing loss of vascular smooth muscle constriction, hence leading to mucosal reperfusion and haemorrhage. Murakami et al. indicated that hypothermia causes an increase in blood viscosity, resulting in a decrease in mucosal blood flow and the development of gastric mucosal lesions. Hyperacidity may be a permissive factor in the pathogenesis of mucosal lesions. 13 Tsokos et al. hypothesised that circumscribed haemorrhages of the gastric glands can be caused by cooling of the body in vivo or during the agonal period. They proposed that subsequent autolysis of RBCs and haematinisation of the released haemoglobin by gastric acid leads to the blackish-brown appearance of Wischnewski spots observed at autopsy. 2
At the same time opinions on the cause of Wischnewski spots as seen in cases of hypothermia are in conflict with the role of stress as a contributory factor and this is being studied. In a study conducted by Arai et al. 7 on animal models, the presence of marked ulceration was seen in animals subjected to stress and hypothermia as compared to those exposed to stress alone. This highlighted the role of low body temperature in the development of gastric lesions. In another study on the effect of hypothermic restraint stress in the development of gastric lesions, Murakami et al. reported that hypothermia, but not restraint, was related to the development of these lesions. 13 In a study conducted on animal models by Landeira-Fernandez, it was concluded that conscious rats that were exposed to cold water stress developed severe gastric ulcerations as compared to the unconscious ones that were exposed to the same stress. 8 This study suggested that the contribution of the level of consciousness is relevant in the development of gastric erosions. Similarly, Goldman and Rosoff conducted a study on rats that were subjected to stress in the form of immobilisation and fasting for almost 20 h without the development of hypothermia in them. 9 The presence of gastric erosions in this study contributes to the evidence of the role of stress in their development. Significant in this regard is a recent study conducted by Bright et al. 10 which reported the absence of gastric lesions in 100% of the anesthetised rats that were exposed to low temperatures for 2–4 h.
Wischnewski spots in human fatalities have been observed mostly in deaths from primary hypothermia in freezing temperatures. The geographic location of this reported case is by contrast a tropical zone where climatic conditions are hot and humid during most parts of the year. To the best of our knowledge, this is the first case of Wischnewski spots being reported in a case of fatal burns. The circumstances of death suggest the possibility of development of secondary hypothermia due to rapid heat loss in the reported case. Burns are an extremely stressful event; the stress caused by extensive burns exceeds that associated with any other injury. 14 This case of Wischnewski spots being found in a victim of fatal burns suggests the possible effects of factors such as stress and secondary hypothermia in the development of these spots. So far sensitivity and specificity of Wischnewski spots in cases of reduced core temperatures have not been accurately determined. We believe further exploration is needed into whether the spots are a reliable indicator of primary hypothermia in cold related deaths.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.