
Abstract
Death from plastic bag suffocation is unusual and rare in under-developed countries. Initially, deaths were accidental mostly of children but with time homicides, suicides and deaths in auto-erotic situations were noted. It is not always possible to discover the dynamics leading to the death especially when suicide is suspected. Often, the typical signs of asphyxia – petechial haemorrhages, facial congestion, oedema and cyanosis – are not there. The authors present two cases of plastic bag suffocation, where a multi-disciplinary approach was applied. This study reviews international literature on plastic bag suffocation, analysing the frequency of suicides, homicides and accidental deaths associated with plastic suffocation.
Introduction
Plastic bag suffocation is a rare cause of death, mainly occurring in developed countries; deaths involving plastic sheets appeared in the late 1950s, when single-use plastic carrier bags began to replace paper ones.
Accidental asphyxias were first connected with in appropriate use of plastic bags, especially when children put their heads inside them.
International literature has analysed different aspects of plastic bag suffocation over the years; several studies provide a general overview of its epidemiological correlations, while there are studies that have analysed different methods of asphyxia death.
The range of different situations involving deaths from plastic bags mean that a wide range of specialist services may be applied including forensic toxicology and criminology.
At present, asphyxia using plastic bags, although rare, is recognised as occurring in different circumstances including autoerotic activities, homicides, infanticides, 1 accidents and suicides.
Suicides account for most deaths especially in elderly people and mentally ill patients, 2 and this may be combined with sedative drugs3,4 or with toxic gas inhalation.5,6
Plastic bags are readily available, death is non-violent and achieving it requires no special advance preparation.
Dealing with plastic bag suffocation can be a challenge for the forensic pathologist as in most cases the classical signs of asphyxia and histopathological findings are absent or vague and non-specific.
Consequently, establishing whether it was homicide, suicide or accidental death requires the accurate collection of evidence.
We report two cases of suicide involving a plastic bag, in which autopsy findings, histologic, immuno-histochemical and toxicological examination and crime scene investigation led to the correct diagnosis. This paper aims to review the international studies on plastic bag suffocation, emphasising the pivotal role of a multi-disciplinary approach to detect the cause and manner of death.
Methods
Relevant scientific articles were identified from PubMed, Cochrane Central, Scopus, Web of Science, Science Direct, EMBASE up to January 2019 using the following keywords: “plastic”, “bag”, “suffocation”, “death”, “asphyxia”. The keywords were individually searched for in association with each of the others. Unsuitable papers for the purpose of the review were excluded; hand search was performed through the reference lists of the included articles.
Results
Using the most popular search engines, a selection of appropriate scientific articles was performed. Only 25 papers (21 articles, 4 books) were included.
Johnstone et al. 7 described four cases of rapid asphyxia death as a result of covering the face with plastic sheeting in accidental auto-erotic circumstances. Later, Hunt et al. 8 reported three deaths from suicidal occlusion of the airways using plastic.
According to Polson 9 in 1984, no homicides were committed using a plastic bag until then. However, in 1991 Knight 10 mentioned three homicides related to plastic bags.
Pullar 11 categorised plastic bag suffocation in two groups: suicides and those associated with sexual activity (men only).
Crompton 12 reported 32 cases of plastic bag suffocation of which 29 were suicides, one was an accidental erotic death and two were uncertain.
In 1993, Perez Martinez et al. 13 identified 18 cases of suicides by plastic bag suffocation (more women than men) where it was found that all of these suicides but one had a history of psychiatric illness, specifically depression.
Haddix et al. 4 reported 53 suicides using plastic bags in Washington, D.C., from 1984 to 1993; there were more women (53%) and 80% of those who committed suicide were over the age of 50. The authors inferred that this method offered a possible means of “self-deliverance” from terminal illness as described by the book Final Exit: The Practicalities of Self Deliverance and Assisted Suicide for the Dying, released in March 1991 by the Hemlock Society; 11% of the deceased had the book.
Marzuk et al. 14 found the book Final Exit at the scene of 9 out of 33 reported cases of suicides by asphyxiation.
In a 17-year study, Morini et al. 15 identified 24 cases of suicides with plastic bags in a total of 27,600 autopsies performed in the Milan area; 17 of these had depression.
Jones's study 2 found that over a period of over 15 years, 30 deaths were attributed to plastic bag asphyxia, and 27 were suicides, of whom 59% suffered from chronic psychiatric illness.
Between 1993 and 1997, Bullock et al. 3 identified 110 cases of suicides by plastic bag suffocation in Ontario, Canada; in 40% of cases the deceased was seriously ill and 92.6% tested positive to one or more drugs at toxicological tests: benzodiazepines, diphenhydramine and antidepressants were the most common.
In 2001, Nadesan et al. 16 presented two cases of plastic bag suffocation in Malaysia: the first was diagnosed as suicide and the latter as sexually related asphyxia; this paper noted them to be the first of their kind in an Eastern country.
An interesting paper by Goj et al. 17 reported five cases of plastic bag suffocation out of 89 suicides identified in a correctional institution.
Paganelli et al. 18 observed 273 suicides from 1998 to 2002 in the area of Genoa of which 50.5% were diagnosed as violent mechanical asphyxia; five deaths were attributed to plastic bag suffocation.
In a 20-year study, 19,411 autopsies were performed in Adelaide, South Australia and it was found that 45 deaths were plastic bag asphyxia 19 : 42 cases were diagnosed as adult suicides and the remaining three involved children of whom two were homicides and one accidental death. Among the 42 adults, toxicological tests revealed the presence of benzodiazepines in 10 cases; 17 victims had a history of depression and five were significantly ill.
Number of cases reported as plastic bag suffocation and distribution of manner of deaths.
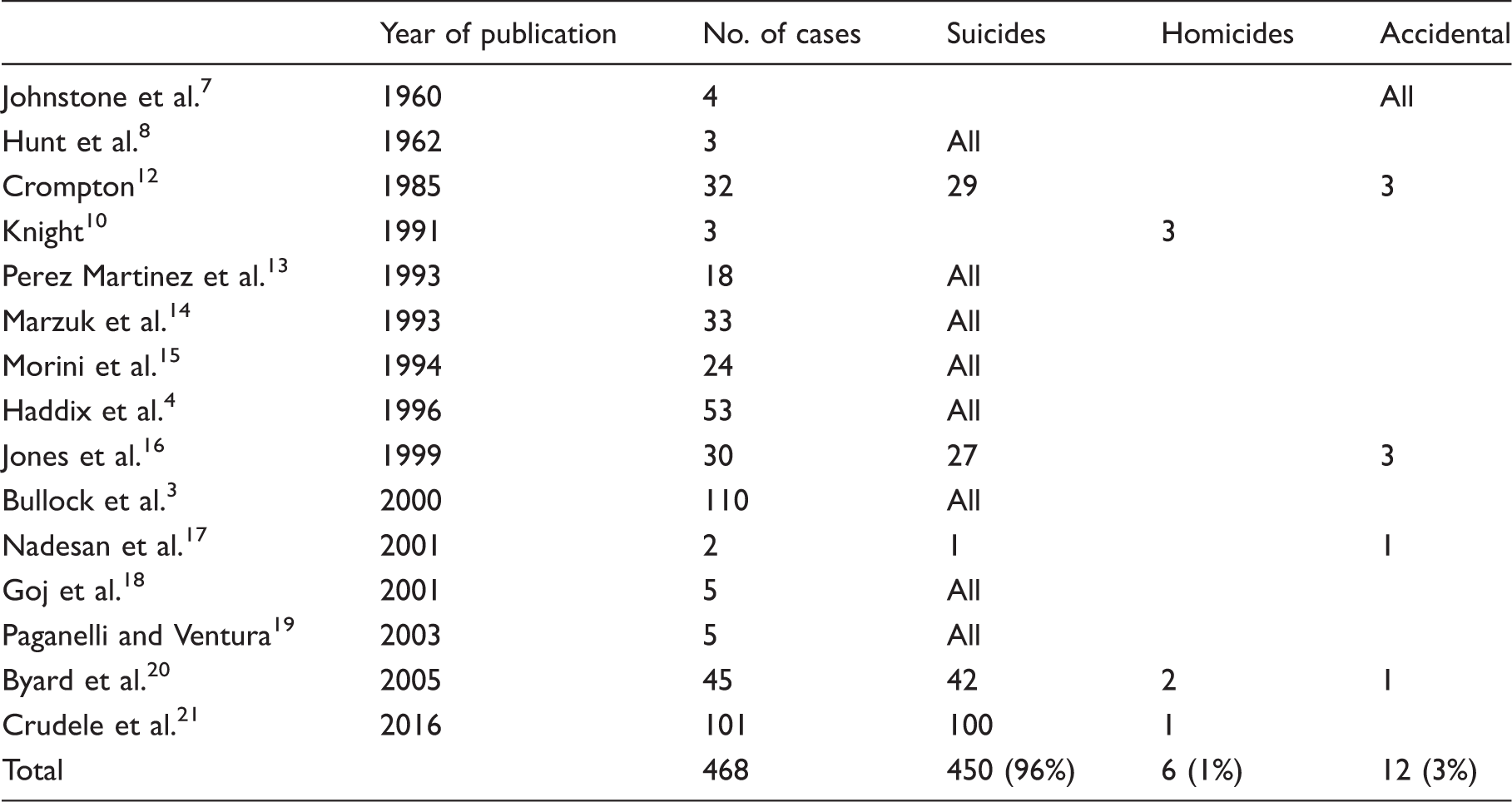
Performing a statistical analysis of the selected reports, the authors identified a total of 468 cases of plastic bag suffocation; 96% were suicides, 1% was homicide and 3% occurred in accidental circumstances which included all deaths in auto-erotic situations.
Case Reports
Case #1
A 66-year-old Caucasian man was found dead in a hotel room two days after he had checked in; scientific police along with a forensic pathologist investigated.
The corpse was found lying supine on the right side of the bed with the head partially enclosed in a transparent plastic bag (water droplets were trapped inside the bag). A black baseball hat was found inside the plastic bag.
A little pile of manuscripts was found on a writing desk in front of the bed; further analysis revealed these manuscripts were farewell notes; a lot of medications were found on the bedside table and in the bin. The medications were pain killers (diclofenac), anti-hypertensive drugs (telmisartan), anti-acid drugs (hydrotalcite), anti-diarrheal (loperamide) and anti-emetic drugs (metoclopramide), one blister pack each. Empty blisters of benzodiazepines (zolpidem), pain killers (tramadol and ibuprofen) and anti-hypertensive drugs (nifedipine) were found in the paper basket (Figure 1).
Numerous medications' blisters found on the scene.
There was no evidence of violence in the room. The autopsy was performed at the University Morgue of Rome; external examination found wine-red hypostasis involving the back, the lateral sides of trunk and neck, the face and the arms. Post mortem rigidity appeared almost overcome; a dark red fluid leaked from nostrils and mouth. The internal examination showed systemic congestion involving the encephalon, lungs, liver. The histological examination performed on encephalon, lungs, liver and heart specimens stained with haematoxylin/eosin confirmed the presence of congestion (Figure 2(a) and (b)).
(a, b) Lung specimens stained with hematoxylin/eosin showing diffuse edema, rupture of alveoli and blood congestion; (c) immunohistochemistry examination showing diffuse positivity to HIF-1 α; (d) immunohistochemistry examination showing diffuse positivity to SP-A.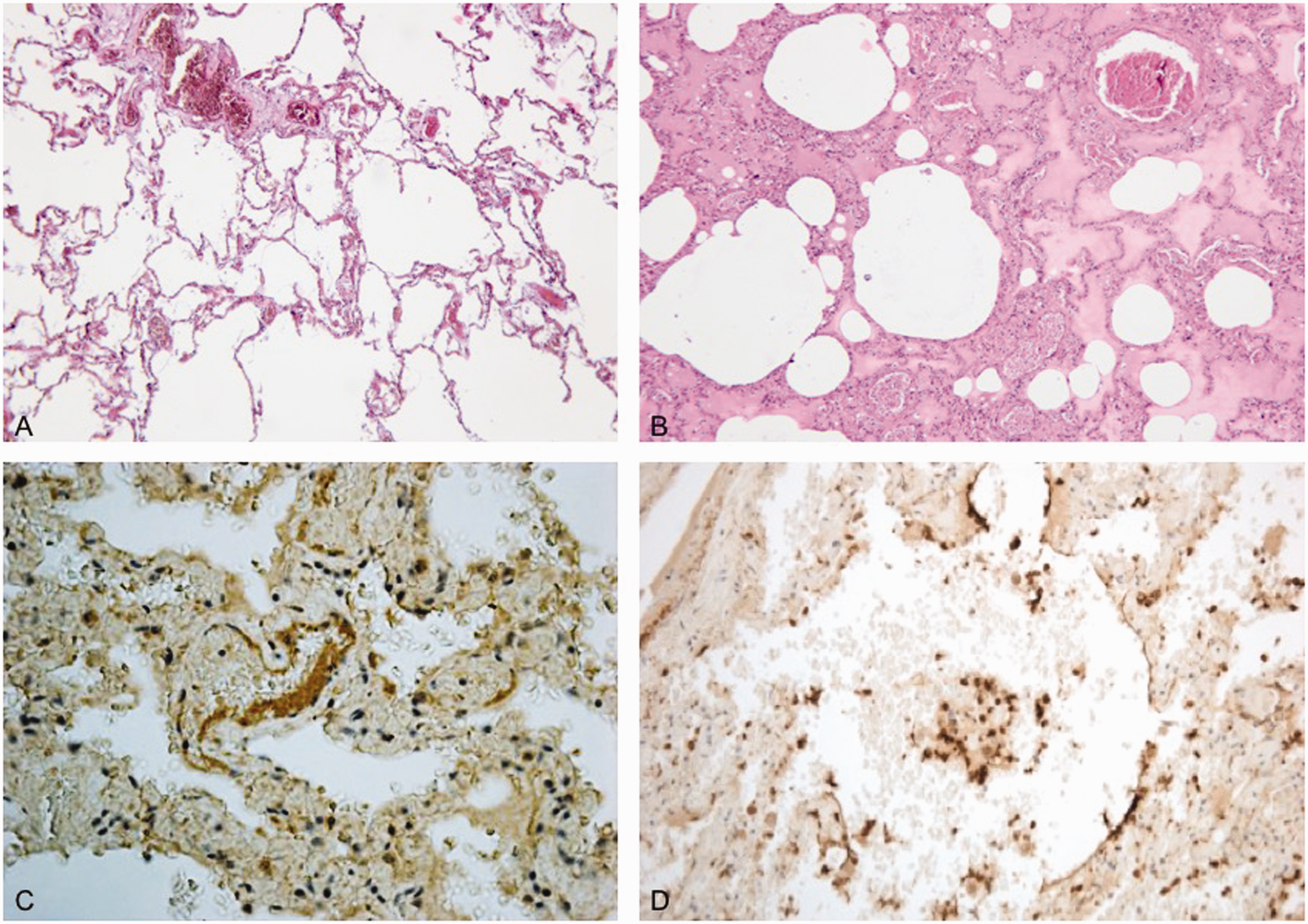
Immunohistochemistry examination was performed on pulmonary samples, analysing the expression pattern of HIF-1 α SP-A, which both resulted diffusely positive.
Toxicological examinations performed on peripheral blood, urine and bile showed positivity for tramadol and zolpidem; tramadol concentration in blood sample was 3.37 µg/ml, 2.39 µg/ml in urine and 325.1 µg/ml in bile. Zolpidem concentration was >0.5 µg/ml. The final diagnosis was suicidal asphyxia by plastic bag associated with drugs intoxication.
Case #2
The corpse of a 47-year-old Caucasian woman was found in her flat; scientific police had investigated the scene before the forensic pathologist arrived.
The body was found on the bed in a foetal position, lying on the right side with the head wrapped in a black pair of stockings and partially enclosed in two plastic bags. A blue and white rope was found around the neck. Later the pathologist discovered that the police had moved the plastic bag from its original position.
(a) Lungs specimens stained with hematoxylin/eosin showing diffuse edema. (b) Immunohistochemistry examination showing diffuse positivity to HIF-1 α.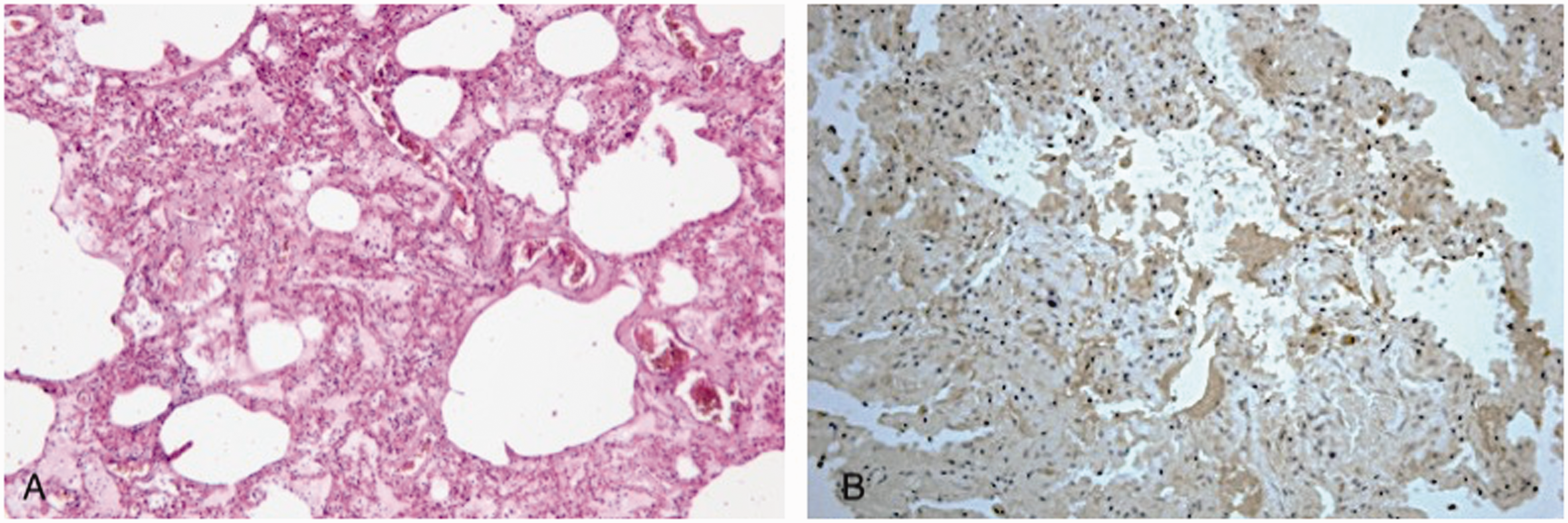
The room appeared cluttered, but the police did not find signs of violence. Inside the bedside table there were various medications: benzodiazepines (clonazepam and alprazolam), anti-depressants (fluoxetine and escitalopram) and the blister packs were mostly empty. The autopsy was performed at the University Morgue of Rome; at the external examination were found wine-red hypostasis involving the back, the right side of trunk and neck, the right side of the face and both arms. A dark brown fluid leaked from nostrils and mouth. The internal examination showed no macroscopic abnormality, except for diffuse congestion; this last datum was also confirmed by histological examination (Figure 3a).
Immuno-histochemical analysis showed diffuse positivity for HIF-1 α and SP-A (Figure 3b).
Toxicological examinations performed on peripheral blood showed positivity for clonazepam (0.7 µg/ml), alprazolam (1.1 µg/ml) and fluoxetine (0.8 µg/ml).
The conclusion of the pathologist was suicide committed with plastic bag and exogenous substances intoxication.
Discussion
Suffocation is a form of violent mechanical asphyxia by occlusion of the respiratory orifices. According to Knight’s 21 definition, the term suffocation refers to death by oxygen scarcity, while smothering refers to external occlusion of external air passages.
Another variety of suffocation is gagging, when the victim's mouth is covered by adhesive tape or a cloth.
When a dead corpse is found with a plastic bag placed over his head, specific attention should be given to the crime scene and checks made on: the presence of the plastic bag in situ, fastening objects that were possibly used, farewell notes, signs of violence, as well as the location of the event itself.
External and internal examination of the body should be carefully performed; on external examination, the forensic pathologist may find cyanotic coloration of head and neck, haemorrhagic petechiae (especially subconjunctival) and froth around nostrils and mouth. Classic asphyxia autopsy findings are acute pulmonary emphysema and oedema, froth in lower airways, pulmonary congestion and haemorrhage, sub-pleural and sub-epicardial petechiae and visceral blood stasis. Unfortunately, none of these signs is specific and they are often non-detectable.
Histological examination does not provide a specific indication of asphyxia death; microscopic findings are generic and variable, and also related to the kind of death (i.e. acute or slow, protracted or interrupted).
It is well known that lungs show different adaptation mechanisms in response to low oxygen tension; in addition to physiological changes, acute response to asphyxia involves mediators of the vessel response, which may represent a good marker for forensic purposes.
Hypoxia induced factor 1-alpha (HIF-1 α) is a transcription factor expressed in response to hypoxia, playing a role in the vasoconstriction of pulmonary arteries observed in asphyxia death. A further useful marker is Surfactant Protein A (SP-A) a protein part of the innate immune system, which is used as a practical diagnostic marker in mechanical asphyxia.22,23 Analysing the pattern of expression of these markers could provide further information to the pathologist, confirming death as asphyxia.
Immuno-histochemical analysis on pulmonary samples was performed on both Cases 1 and 2; the results showed positivity for HIF-1 α and SP-A. This, along with other information collected, helped the pathologist to diagnose the cause of death as asphyxia.
Death by plastic bag suffocation is not normally characterised by any osseous lesion or fracture: consequently it does not require a post-mortem TC examination, notwithstanding other asphyxia deaths where such imaging techniques provide useful information.24,25
Cause of death
Asphyxia can result from physical obstruction of the mouth and nose and from decreasing oxygen concentration in the available inspired air. The mechanism of death by plastic bag was formerly thought to be due to the plastic bag becoming electrically charged, adhering to the face and obstructing mouth and nose, this phenomenon being aided by condensation of water vapour. 3 According to another theory, when a plastic bag is placed over the head and in close contact with the face, the sympathetic nervous system is rapidly stimulated resulting in arrhythmias as ventricular fibrillation. 21 This latter interpretation could explain the lack of typical pathological signs of asphyxia in cases of plastic bag suffocation.
It is now established that plastic bag asphyxia derives from a combination of oxygen depletion and increase of carbon dioxide concentration, which rapidly leads to the loss of consciousness.
Post-mortem toxicological examination is essential as different drugs are frequently found both in suicidal and homicidal cases. Analysing biological specimens, the search for specific drugs should be guided by the evidence such as the presence of medicines or packaging, syringes or prescriptions at the scene.
Toxicological examination in both Cases 1 and 2 revealed high concentrations of different drugs. In Case 1, blood concentration of zolpidem and tramadol exceeded even the so-called “toxic” level.
Necropsy, histology and toxicology examinations will not provide the forensic pathologist with all the information needed and crime scene investigation is critical to reach the correct diagnosis.
The inspection of the crime scene in Case 1 guided the pathologist; both autopsy and histological examination showed no determining abnormality. The lack of signs of violence in the room and on the corpse together with the evidence collected at the scene (empty medication blisters, farewell notes) and the toxicological results enabled the pathologist to identify the death as suicide.
Case 2 was particularly challenging; the scientific police were in charge of the case and, during the crime scene inspection, police had moved the plastic bag from its original position before the arrival of the forensic pathologist. Hence, the pathologist had to deal with an altered scene. The crime scene must be investigated only by trained staff in cooperation with the forensic pathologist. Even in Case 2 a multi-disciplinary approach enabled us to diagnose death as suicide.
Conclusion
Plastic bag suffocation is challenging for the forensic pathologist as frequently there are few specific external and internal or pathognomonic histological findings and this makes determining the cause of death extremely difficult. Consequently, the pathologist should first ensure a well-conducted crime scene inspection and must co-operate with the police and ensure that all the evidence and situation data is retrieved. Immunohistochemistry analysis may provide valuable information about the cause of death and toxicological examination is needed to identify any exogenous substance. Only a multi-disciplinary approach can determine whether plastic bag suffocation was suicide, homicide or accidental.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable: only data collected in the process of a routine medico-legal investigation ordered by the legal authorities are described in these case reports.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.