
Abstract

Tonight we are here to give you a surprise. We have chosen that word ‘surprise’ to be a rather mild word, but in fact it really should be the word ‘shock’, because what we are going to describe and talk about is truly shocking. We didn’t want to start the evening with too much of a jolt, but we will bring you into that subject now and help you to understand what we mean by that and why this is a global surprise.
If we were to ask people what was the major cause of death worldwide, most would be likely to suggest cardiovascular disease, cancer or, for younger people, HIV-AIDS, malaria or TB. Until very recently, if you were to go to publications about the causes of death, these would give similar results. However, in recent years and with new data this situation has changed dramatically. And the true figures are very different, as we will see in a moment, with trauma being a huge contributor to mortality.
Sadly, this message is not getting through: only last week, the BBC quoted figures saying, ‘This is what people are dying of worldwide, including young people’, and there was no distinction between older and younger in their report and they left trauma at the very bottom of the list: that is really quite misleading.
The BBC, to their credit, did actually say, deeper in their online version of the news, ‘Road accidents incur a high death toll in the richest and poorest countries alike, claiming 1.2 million lives in 2017’. Well, that is an advance, though unfortunately it is a misquotation.
Let me correct what the BBC statement says this way. With the 1.2 million, they are covering rich and poor nations alike. In fact, it is biased extremely towards the poor nations, and, secondly, that figure is only for quite a segment of the population, adolescents and teenagers basically, who die of preventable causes, and the total number of people dying of untreated physical injury is about 5 million. In fact, some figures say it is nearly 6 million every year. And the BBC and others have used the word ‘accidents’, road accidents. Well, they are not accidents. Most injuries caused on the road could be prevented if more care was taken in all kinds of ways, better roads, better drivers, better education, better policing, less corruption, more money, and so on.
But those facts and figures don’t actually tell us what the real problem is. Why is there a problem out there with injury? The problem is this, that the health professionals who go to treat those injured patients – and they could be doctors of any level, or nurses, paramedics, various health professionals from various disciplines, all expert at their job – they are not trained to treat people in those conditions. They are trained in systems typically in the capital city, in the capital city university, and they are trained in a system which is more like what we would find here in the UK.
Let me just use for example the nation of Tanzania, where, if you are in Dar es Salaam, you can definitely get a good ambulance and a good hospital. The Muhimbili Hospital is excellent, good doctors, good everything, systems just like ours, right in the centre. However, go a few kilometres out and you will not find them, and even the doctors and nurses and other medics who practise out there feel paralysed when they don’t have access to the equipment, the facilities, the sterile environments, the services that you get in a major hospital like that. They are stuck in a situation where there is practically nothing, or very little. That is the problem. The shock is that people die in those rural and poor areas.
Now, you may think that sounds like it is on the fringe. Actually we are on the fringe, because those people I just described number 5 billion. So this is the majority of the world. This is not just a trivial point, this is the majority of the world, and they are not getting treatment.
The major cause of such injuries is road traffic. That is the major cause. There are other causes. We will come to them in a moment, too. But what happens is that somebody might save a life. Somebody might know first aid, know some just basic principles and keep them alive. Then along comes the health professional who can do something about it, but cannot actually do much because they don’t have the facilities, the equipment or even an ambulance or means of transportation.
So let me now just show you a little bit more imagery of the context (Slide below).
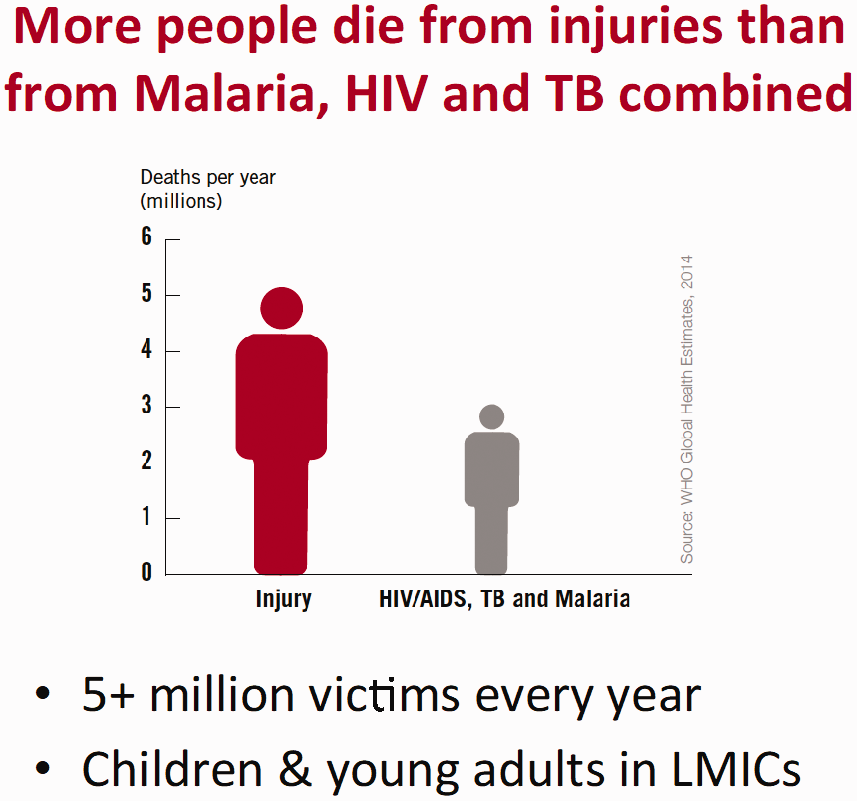
I have already mentioned that more people die from injuries than from malaria, HIV and TB combined, and the special victims are the children and young adults in the LMICs. You have probably heard that language ‘LMICs’. About a year ago we talked about ‘Developing Countries’ – the terminology has now changed to ‘Lower and Middle Income Countries’.
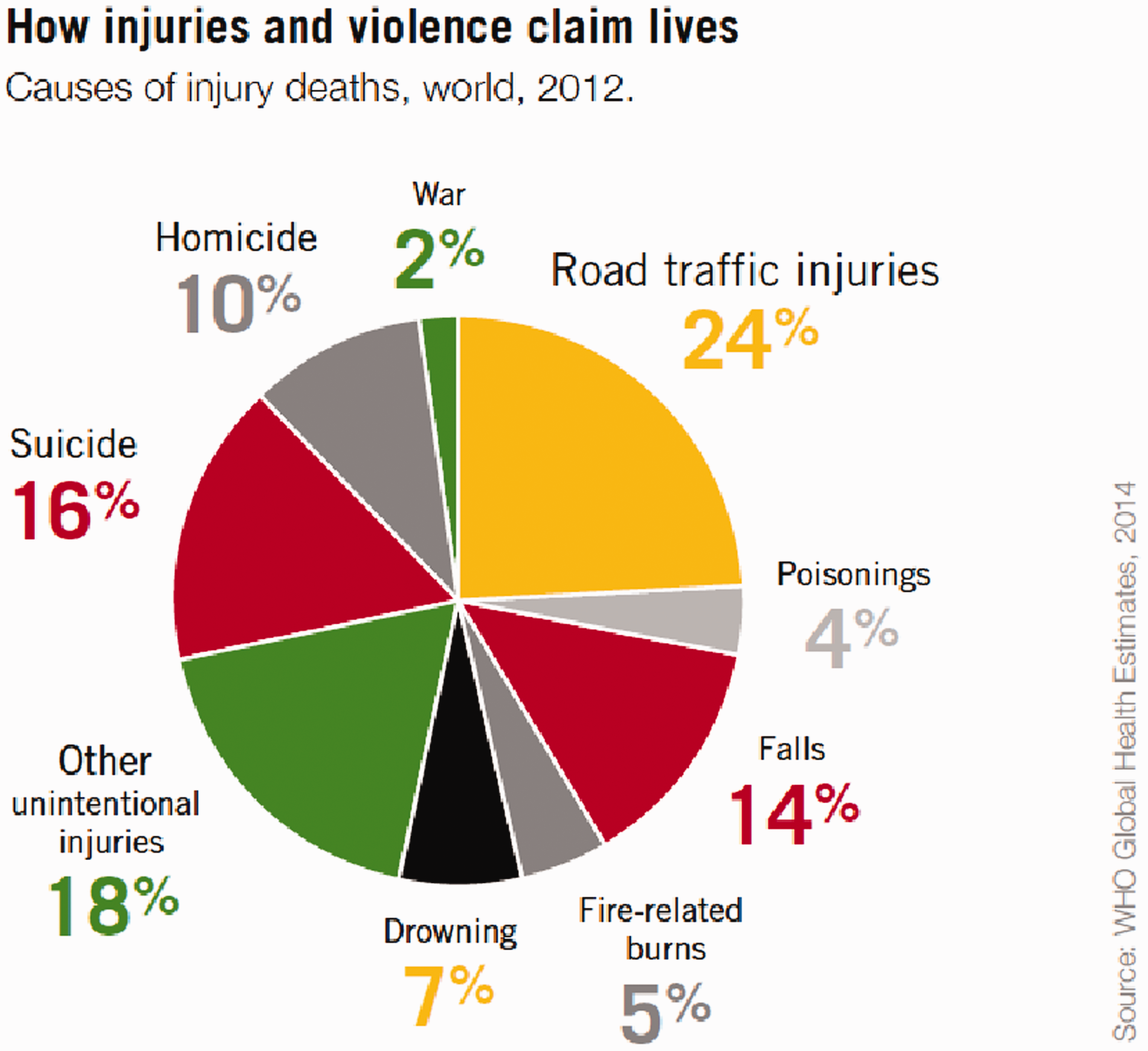
You can see there that the injuries have various causes, not just road traffic though that is the largest (slide above). That figure of 24% was in 2012, and that figure is now much higher. Additionally, don’t forget that we are talking about people who live in out-of-sight places so getting the facts and figures can be very hard. There is no-one standing on the street corner clicking a counter to document how many deaths and disabilities there are.
Most of the burden of trauma is in the poorest countries, and in the most populated areas.
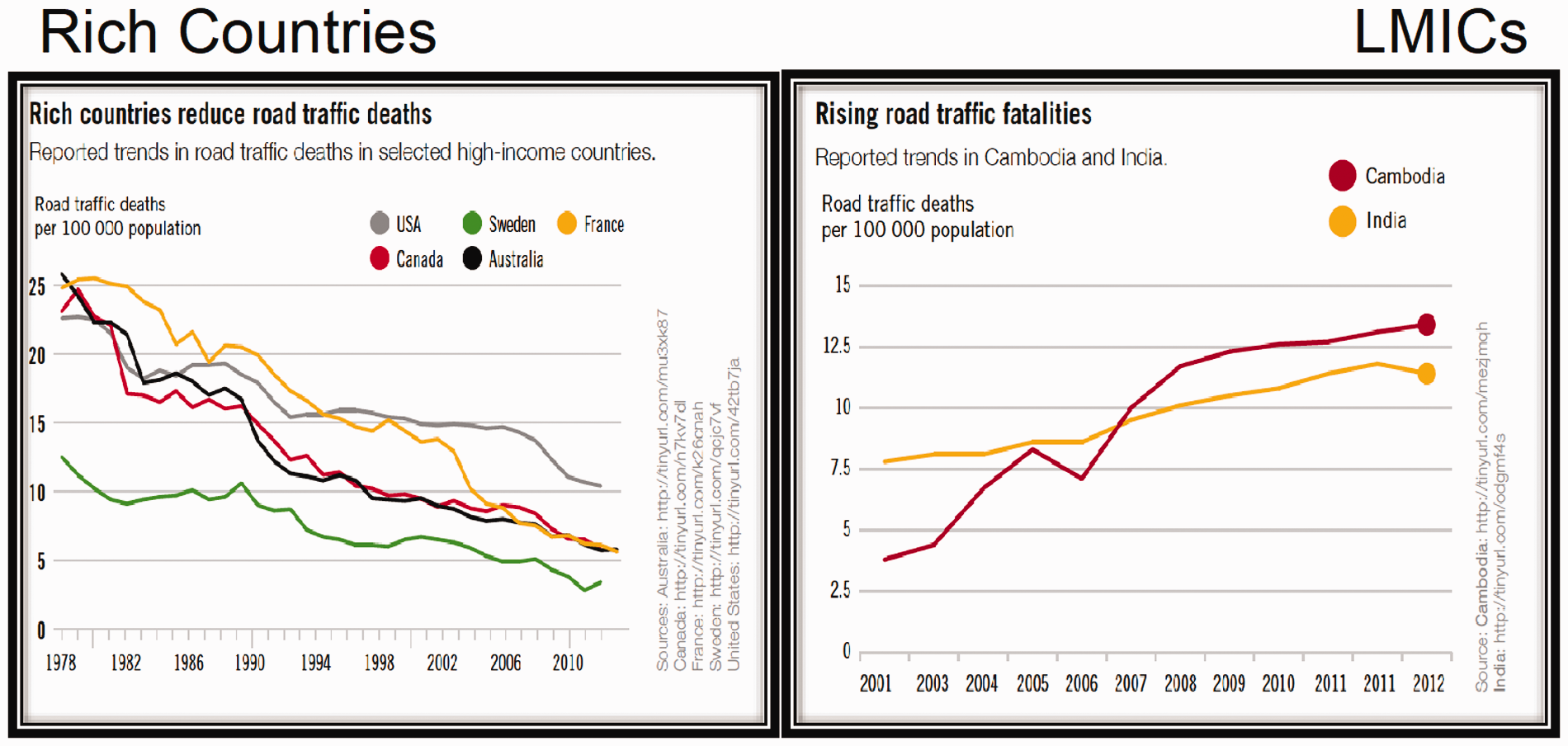
But look at this. In the rich countries – and the coloured lines in the graph above left are in are a sample of five such countries – the trends in road traffic deaths have been dropping substantially. From 1978 to 2010 and just a bit beyond look how they are falling.
Now in contrast, if we go to the graph on the right showing Cambodia and India, which are typical for LMI countries, this trend is reversed.
Why are we getting contrasting situations like this?

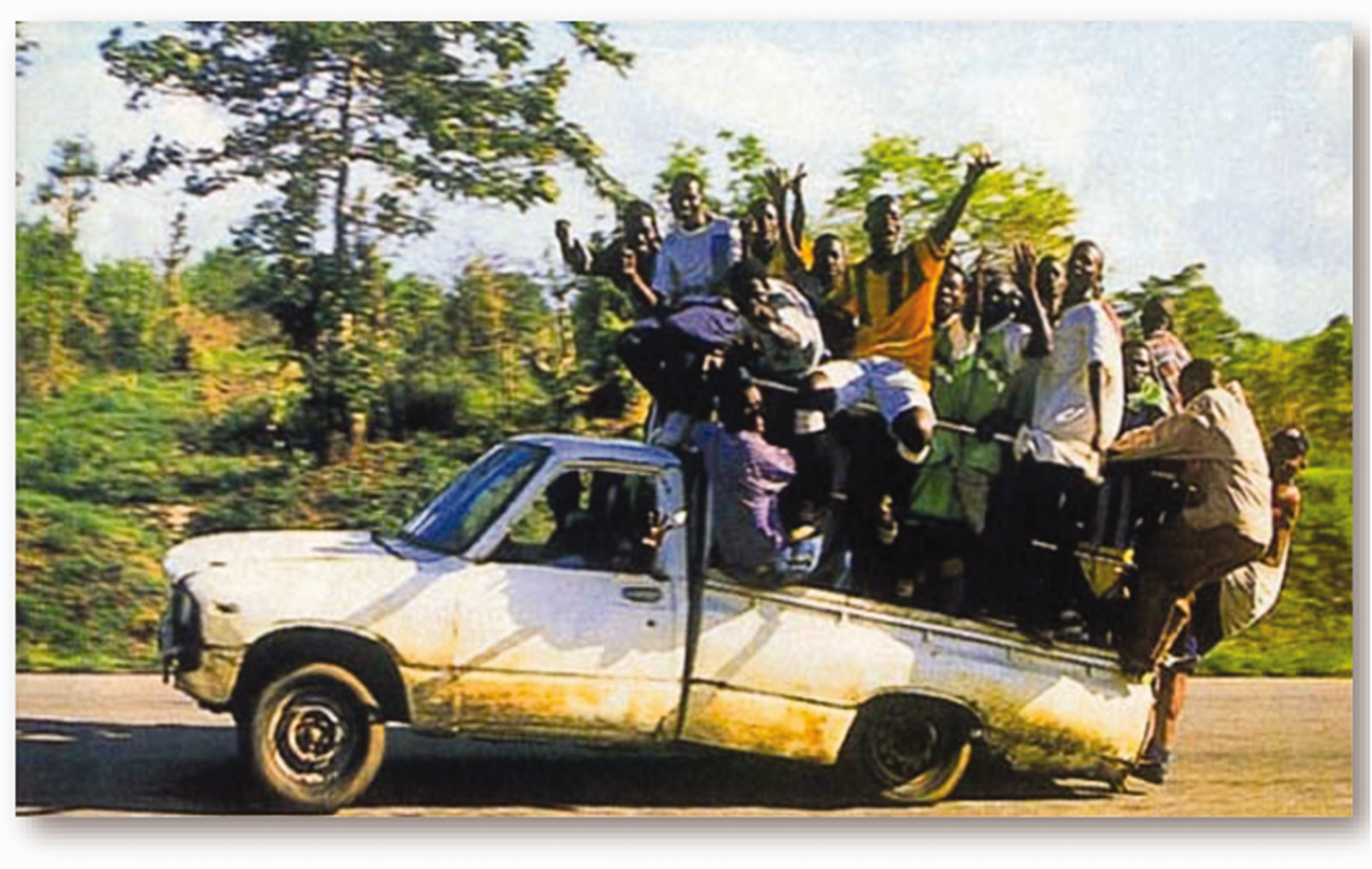
We are very fortunate in our environment, but in much of the world road and other standards predispose to trauma.

James took these pictures on the streets in Ho Chi Minh City – where every cargo possible gets carried on motor scooters – even up to sheets of glass and fridge freezers.
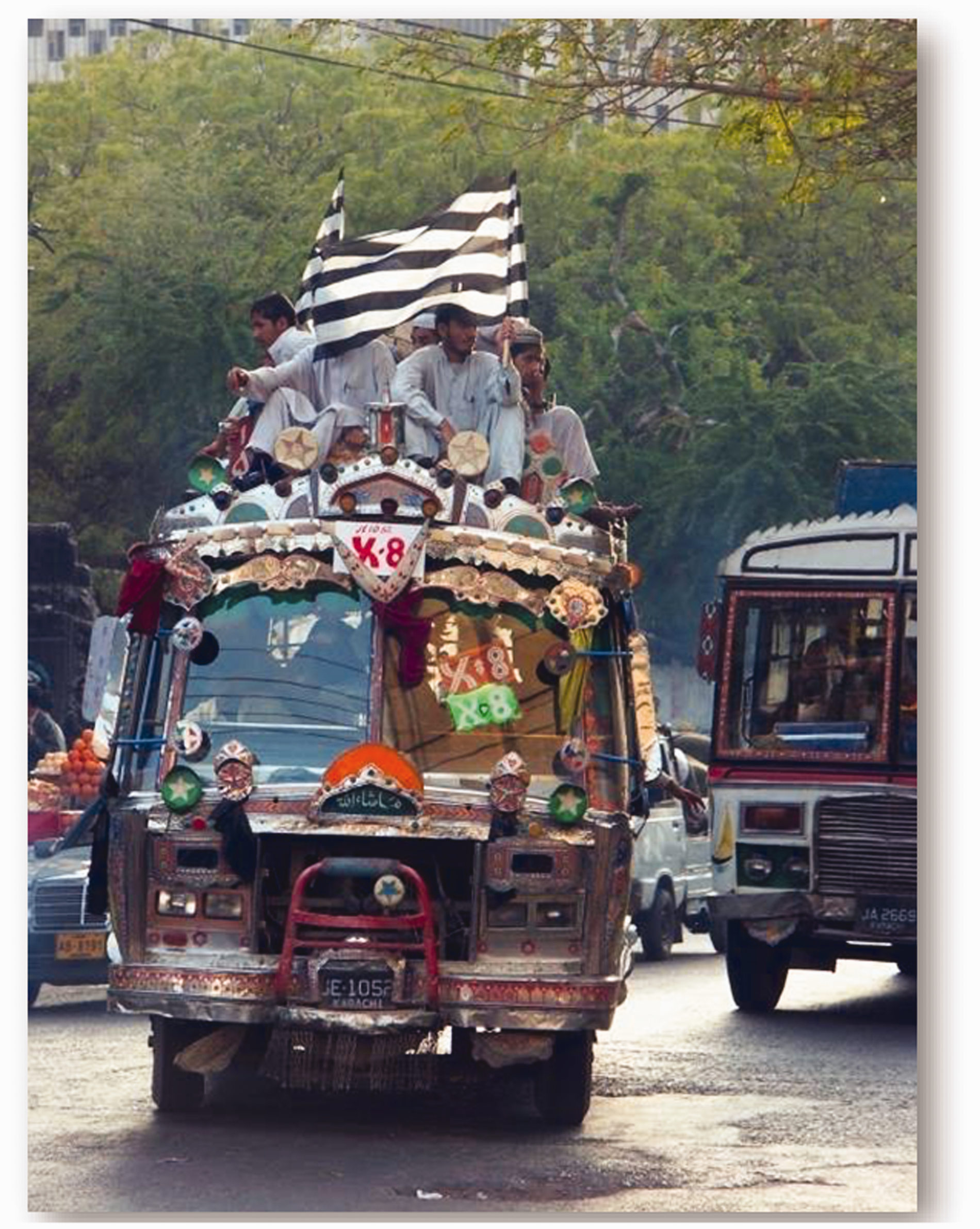
This is a typical bus in many parts of the world.
That is a typical taxi, isn’t it, in many parts of the world.

And motorbikes may be overloaded with whole families on one machine. And countless times in LMI countries you get a combination of similarly overloaded bikes with poor road conditions and unsafe other vehicles…

And sadly then this is what can happen. James has chosen this picture to be one that is showing you a lot less blood and gore, just for the sake of our decency this evening.
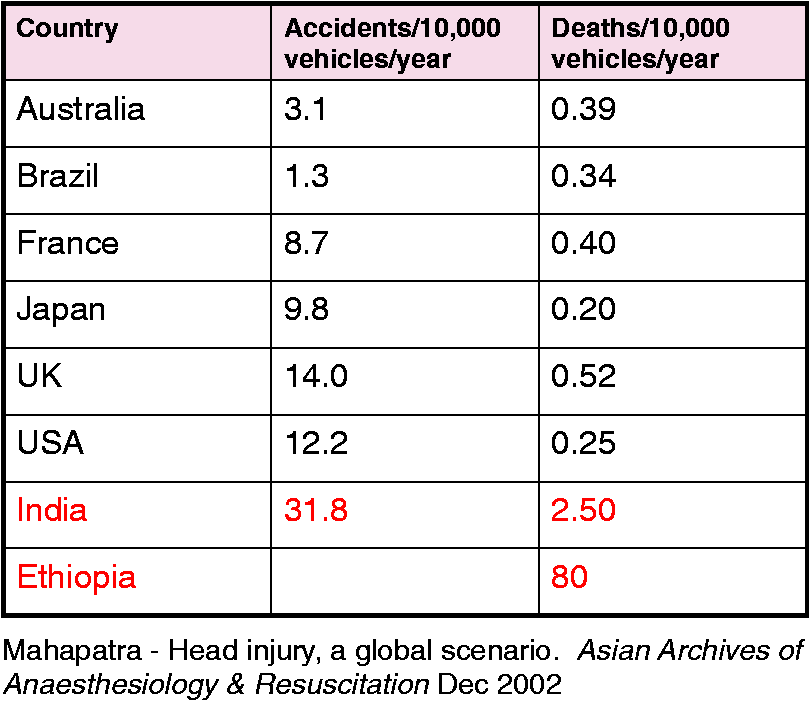
Let me now show you something about the facts and figures again (see the Table above). Concentrate on the upper lines for a moment – Australia, Brazil, France, Japan, UK and USA – you may know these countries personally, all of them perhaps – accidents per year and deaths per year. Just take in the numbers for a second. But now add India and Ethiopia, in red on the lower lines, and you can see a stark difference. On accident numbers per 10,000 there is nothing else in those other countries near India’s level. And look at Ethiopia: the deaths per 10,000 is 80, whereas in the UK it is 0.52.
The problem that lies behind all these deaths is adverse conditions and infrastructure, and we can add various other causes, like war and conflict, and so on. But from our standpoint here is the problem: the medical professionals are not trained to manage trauma victims in the way that is appropriate for the situation and there isn’t awareness of what to do. Even where I live in Oxford if someone was run over on the street I think most people would know to keep them warm and safe and dial 999 and wait for the ambulance in, supposedly, 5.5 minutes.
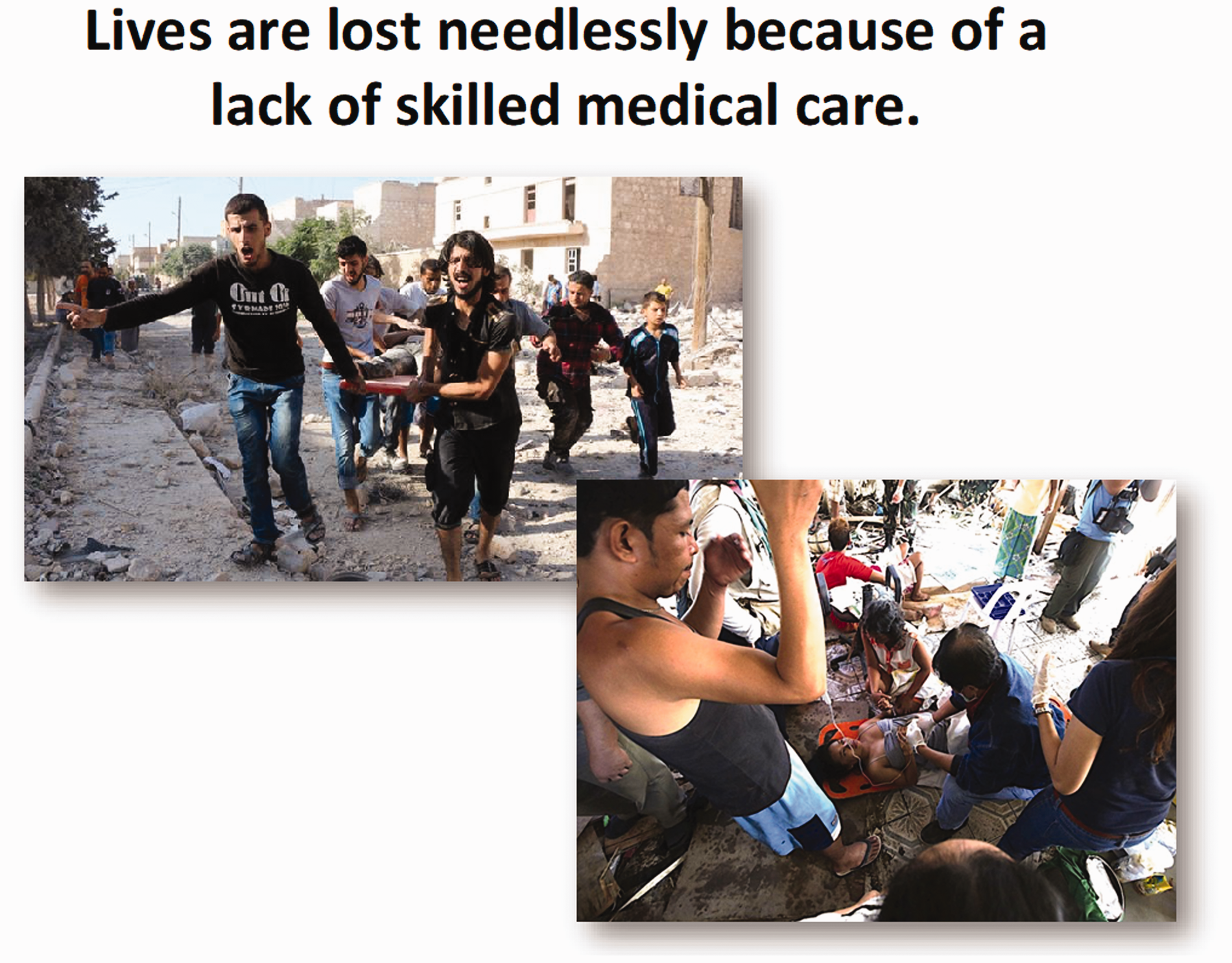
But this is how people are carried very often to any medical facility in various parts of the world all the time. They are manhandled on the backs of bicycles. I’ve seen them on donkeys and cows, on the backs of trucks, motorcycles, over someone’s shoulder, carried with four men holding a limb each. At the roadside, during transfer to hospitals and in hospitals lives are lost needlessly because of a lack of skilled medical care.

Now let’s just look at the figures again (see the Table above). I said it was a shock. Take a look at the chart here. This is now much more up-to-date. This is 2018, last year, and this is a critical age group, 15–29 years of age. Actually, it starts with age 5. Look at the bottom half of that page. 5–14 years of age: road traffic injuries are the second most common cause. 15–29 years of age: road traffic injuries are the main cause of death. Then after that, at 30 years upwards, they are the third most common cause.
Now, it doesn’t take much thinking to realise that this is a critically important age group for any society, but especially for the Low and Middle Income Countries, where the productivity of those countries depends a lot on these young adults and their education and their health. Using a rule of thumb in many countries in Africa, for example, you can expect about 30 dependants for every working person: so if one of those working people gets injured, if they survive and they’re injured and can’t work, whatever the result, about 30 people will suffer as well. Now, that is the shock. That is the horrible news. That is what needs to get out there. The media doesn’t get it yet. It is very little published. It is lagging behind.
And I just remind you of what I said earlier, that ordinary situations are where this happens. It is not so much bombs and wars, not so much floods and violence and collapsed huge buildings, and things like that. They always get media attention. In the UK there is a fly-out service. There are doctors and medical professionals who are ready on standby. It is a super service, a wonderful thing. They can fly out at very short notice and be somewhere else in the world very quickly with what is effectively a field hospital. Well, that is great. That is wonderful if you have earthquakes and disasters like that, but for the other 5 billion people, they just never receive such care. That doesn’t reach them, it is way beyond them.
What is needed is to find a way to improve the knowledge and skills of those who will be caring for all the people who are suffering and dying from trauma daily in these countries.
This need has given birth to a new approach, and James will now tell us about the Primary Trauma Care curriculum.
So let’s recap on what Charles said. We are facing a global epidemic. If I went round to most people and asked them what is the major cause of death in developing countries they would be likely to say HIV, AIDS, malaria or TB. However, trauma far exceeds all those put together. Putting the impact of this into perspective, I live in Gloucestershire and the worldwide death toll is 10 times the population of Gloucestershire per annum, 6 million people.
As the Global Alliance for Care of the Injured (GACI) pointed out, ‘We can save 2 million lives each year. What is needed is the strengthening of trauma care systems’.
Now, we may not all agree with politicians, but I think Tony Blair got it right on one thing when he commented, ‘Ask me my three main priorities for government, and I tell you: education, education and education’. It is far more productive to teach people and to teach them to teach others. You know the story about giving someone a fish and you feed them for a day, teach them to fish and you feed them for life. Teaching people to teach others is the key.
The aim of what we, in the Primary Trauma Care Foundation, do is to train doctors and first responders in the management of severe injury in LMICs, and to create a sustainable and self-maintaining cascade by teaching people to teach this to others.
Now I said earlier I teach on ATLS. There is also a course called EMST in Australia, and there are several others. They are all good. However, they are all courses designed for use in developed countries, that require and assume expensive equipment and facilities.
There is a lot of debate about whether these courses work. Some say yes, some say no, but I think those of us who have done ATLS and other courses would feel that the key thing is that it gives to you and to everyone else involved a system, something to hang your hat on. As far as I am concerned, as a doctor practising in trauma, that is something which works, because I know that the nurses, the radiographers, the other doctors in the department will all know what we do.
But if I run an ATLS course as Course Director the doctors who come on our course pay about £600. Of that about £150 goes straight to America as a copyright fee to the American College of Surgeons, because they developed this course arising out of the experience of an orthopaedic surgeon, James Steiner, who crashed his plane in Nebraska. He was taken with his family, all severely injured, in a little cottage hospital. The doctor eventually turned up and Dr Steiner had to show the doctor how to resuscitate his family members and then talk him through sorting out his own injuries. This gave him the incentive to start the design of the ATLS Course and it has developed from there.
It is very much an American course, which is great in its context, but it is expensive and its price is fixed irrespective of where it is run. But it is very centralised, it has to be done the American ATLS way. We have to run it with the right ATLS facilities, teaching aids and equipment, otherwise we get our licence to teach it taken away. We have to have 10 instructors per 20 candidates. That is hard enough to organise in the UK, let alone abroad, and the course is not allowed to be altered or adapted.
The recognition of this issue and of the lack of trauma training in LMICs led to a number of publications, including one written by my colleagues in Oxford, Mike Dobson and Douglas Wilkinson, for the WHO, which we suspect is still mouldering in the archives of the WHO somewhere. Nothing happened, so Douglas and our colleague Marcus Skinner from Tasmania decided that they needed to get on and do something themselves.
So they wrote a document called the Primary Trauma Care Manual, and out of that grew the PTC course, which is designed to be appropriate for resource poor environments and not to depend on equipment or assume developed world resources.
When we go to a country to teach PTC we feel that it is essential to teach the course with what they have got and what they will be using clinically, and with what they will be teaching the course, to encourage ease of replication.
We teach people to work within skill levels, so we have the flexibility to teach it sometimes at different levels. When I taught PTC in Colombo, in Sri Lanka, the participants were all senior surgeons and anaesthetists who had all worked in the UK or Australia, so we taught it at a similar level to ATLS, but in other countries we have often taught it at rather lower levels, and, as we will say in a minute, we have been into 77 different countries teaching it.
We teach, as I say, with what they have got.

For instance, in Sierra Leone they had different needs as well, as these two pictures illustrate (see above). The picture on the left illustrates the equipment they had: tubes, condoms, not much else. You can actually improvise a very good chest drain, i.e. something to drain a leak of air from the chest cavity, with a catheter and a condom – not necessarily something we would advocate in the UK. But also, in Sierra Leone, common injuries included attacks with machetes severing limbs, so what they wanted was how to deal with stump injuries and landmine injuries. So that was built into the course because that is what they wanted.
The other thing is that the PTC course is free. We don’t charge for it, and we have a small course manual which is freely downloadable on the internet.
But the other key thing is that we want to give ownership and responsibility to local doctors, local teachers, as quickly as possible, and in a moment I will outline how we do that.
So, to summarise, PTC is a system of training for front-line staff in trauma management, aimed at preventing death and disability in seriously injured patients, using available resources with the aim being to train clinicians to teach PTC principles in their hospitals. That last part is key, training doctors to train others, thereby to make it sustainable.
So let us outline the content of the PTC Course:
Prevention Triage Primary survey Secondary survey Stabilisation Transfer Definitive care
This system is similar to other trauma courses. Triage is the application of the system to situations with many injured people, sorting out who is the one to treat first and to deal with; and then a system of what is called primary and secondary survey.
Primary Survey involves looking quickly at the patient. It takes 2 minutes just to say ‘What is the injury that is going to immediately kill you?’
Let me illustrate this. So if I come down the front row and approach three of the audience, and give each of you different injuries – [to the first] if I injure your larynx shut so you now cannot breathe, and I come to you [the second] and I make a hole in your lung and give you an expanding and compressing leak of air in the chest called a ‘tension pneumothorax’ so you now can’t breathe and have compromise of your circulation, and I come to you [the third] and I cut your femoral vein so that you are bleeding heavily, who is going to die first? [answer – the first].
So you have got a prioritisation of injuries to the airway, then breathing, then circulation. These are the injuries that commonly kill people fast, and if we deal with those rapidly you can save many lives. During the primary survey, as you find injuries you treat them. This does not require high-tech interventions, and is a rapid process.
So the primary survey is rapidly looking for and treating these airway / breathing / circulation injuries, treating them as we find them. We then teach people to go back and check for other and maybe hidden injuries in more detail with a detailed head to toe examination using special investigations if available. We call this the Secondary Survey. These injuries may not be immediately life-threatening but may have a big impact on the patient’s future life and ability to work and provide for themselves and their dependants.

But I talked about sustainability, which is critically important. What we do to encourage this is what we call a ‘2-1-2’ system. For the first two days of an introductory course at a new place we will take a group of senior doctors and nurses who have been selected as potential future instructors, normally 20, through a 2-day primary trauma care course. We teach and model this to them in the same way as we hope it will be taught in the future. So they finish the two days having seen that course and learned its content. The next day they then go on to a one day instructor course, where we teach them to teach. Anyone who has done things like the ATLS Instructor or Generic Instructor courses will be familiar with the design of this course, which is similar to those. Then the participants, fresh from that, before they have a chance to lose their impetus, go on and teach another course with 20 new participants with us mentoring them. In fact this second course will often then generate more potential instructors.
Let me give you an example: Pakistan. I went there in 2003, to Peshawar in the North-West Frontier Province. We taught 20 senior doctors and surgeons. They then split and taught 60 (3 × 20) people on courses, with us mentoring them and supporting them. So we left Peshawar at the end of the week with 80 trained people, of whom there was a cadre of 20 instructors who were experienced, who knew they could run the course and knew that it would work.
The team in Peshawar then carried on running courses. Colleagues in Karachi heard about it, got in touch with us and said ‘We would like this too, please’. So I went to Karachi, taking some of the Peshawar instructors with me, and we ran courses there. It has now spread throughout the whole of Pakistan. We have trained – well, they, not us, have trained around 4500 doctors. Even more importantly, as far as I am concerned, those doctors have now gone into Iran, Iraq, Afghanistan, Delhi, and various other places, and taken the courses to those other countries. It is like throwing a stone into a pool and watching the ripples spreading.
The course itself is run with lectures, skill stations, discussion groups and simulated trauma scenarios. We have compiled a slide set in PowerPoint (I am always amazed at the availability of computers and projection equipment in very poor locations, but we also train instructors not to rely on this technology but to use blackboard presentation, discussion groups etc as alternatives – and to deal with the consequences of power cuts which are very common).

We teach skills with what equipment and facilities they have locally, so in the picture on the left this was the airway management training equipment that they already had in Karachi, which we used in the training. We don’t need expensive kit. We can actually use bits of sheep’s chest, for instance, to teach a lot of skills such as teaching people to put tubes into chests to drain leaking lungs.

Sometimes that can backfire and we may have to improvise. In Kenya last year, as you can see from the picture top left, the sheep’s chest was totally frozen, so you couldn’t do anything with it, and I was left thinking ‘How are we going to teach people to put tubes in between the ribs?’
And I walked out to the courtyard outside and thought (top right) ‘That’s interesting. That grating looks a bit like ribs’ – we can make jokes about chest drains for the medics! [Laughter]. So we wrapped the grating up in a cloth and taught people how to put chest drains in (bottom). [Laughter] And it worked, because the lovely thing is we don’t need expensive equipment, we can make it up as we go along.

We use demonstrations and scenarios – which are always very successful and enjoyed by everyone. In the scenarios, you give them a trauma scenario story relating to a volunteer actor (normally one of the participants) as a simulated patient and they act out their management, using the skills that they have learnt in the lectures and skill stations.
The course programme is a busy two days:
Day 1
Introduction MCQ and Local trauma perspective ABCDE of Trauma and Primary survey Airway and Breathing Circulation and Shock Demonstration Scenario and practices Scenarios practice Secondary survey demonstration Chest injuries
Skill stations
Airway (Basic and Advanced) Cervical spine/logroll Chest drains/needle decompression/ pericardiocentesis Overview and summary
Day 2
Head and Spinal injuries Abdominal and Limb injuries Paediatrics and Obstetrics Burns
Workshops
Analgesia and Paediatrics Neurological assessment Disaster management Difficult situations and transport
Scenarios
Multiple choice paper Feedback and discussion Certificates and close
We then teach them the Instructor Course, which is based upon the ones we use for ATLS and ALS and other courses in the UK and which covers background knowledge on aspects of teaching and learning such as how adults learn, questioning, presentation styles, feedback and language issues and then small group workshops putting these into practice, and practicalities of course organisation. During this day they prepare for their own teaching of the course to a second group of participants, with our support and mentoring, over the following two days.
We use and provide various materials including slides, the PTC Manual and Instructor Manuals, and various other resources are available to the new instructors in running further courses. These are available for download at our website, www.primarytraumacare.org. We have been very pleased in fact that the WHO has taken Primary Trauma Care and put it in their ‘Surgical Care at the District Hospital’ book as the recommended trauma system.
We have introduced PTC in many different countries and the course materials have been translated into a range of different languages.
So what is so special about PTC? Well, in a way this is really summarising what we have said already. It is low cost, but it is high standard. We may joke about chest drains and gratings and things like that, but it is teaching important skills in a way that can be replicated. What is important is the feedback that we get, where people say ‘It works. I’ve done it and it is successful’. We are teaching with the kit they have got. It is flexible; we can adapt it if we need to, and most importantly we are training local doctors and instructors to have ownership of it and make a cascade. We talked about Pakistan. It has worked like that in many other countries.
There is good evidence for PTC. Our group in Oxford have produced quite a lot of papers now, as well as there having been other publications. If you want, I can give you a list, but the main thing is there is good evidence that it works.
And I think the thing particularly, when we were analysing what makes it work well, is early cascades. This is why we get them to teach straight away and we say ‘After the first course, you really need to run another course in the next month or two for it to work’, because otherwise the impetus goes. In our experience, in places where PTC has really worked we have had enthusiastic people who have been prepared to take it on and be figureheads. We go back and we mentor, and that is critically important, and also getting it adopted both by governments and by hospitals.

So we have been into 77 countries now (see above). It is difficult to get absolute participant figures because, for instance, every few months we get another letter from Indonesia saying ‘Oh yeah, we have run another 20 courses’, so we had to infer some of their numbers, but we have now trained somewhere about 90 to 100 thousand doctors worldwide.
Charles, I will let you talk a little bit to finish.

We therefore obtained and set up the web domain www.lifesavingaction.org. For fundraising we use this kind of language, and that is a very good illustration also of the ethos of the organisation: pragmatic, get it done, be willing to be flexible, be ingenious, and Life Saving Action is the message we want to give.
I want to close with just a word about the need now. You have heard what we do. You have heard the need. You have heard the shock it is. It is horrible to think – I hope this keeps you awake tonight – that young adults in the world are under such threat. Also we have told you how we are tackling it.
In the course of my work I go to the World Health Organisation and I meet with various people in the world who deal with these sort of issues, and I can tell you there are many interventions in trauma, but almost all of them are of the high-tech kind, a million dollars here, a million dollars there spent on the equipment required in making the emergency room and the operating room as fancy and as technical as possible, because that is what people aspire to, and I say ‘Good. Let’s see more of that. That must happen’, but a colleague in Geneva commented that his estimate of what it would cost to roll that out across the 5 billion people would be about $13 trillion every year for a decade. It is not going to happen. Clearly something has to happen that is cheaper, that is accessible, that is available and can be done now, and that is what we do.
This organisation is unique. There is no other in the world doing this in the way we have and on such a scale; and yet the challenge is, even though we run the courses now in 77 countries, and 5 more countries are waiting, and courses are happening as we speak somewhere – my phone rang this morning from Zambia and the lady running the courses wanted help on a small thing, and we answered that – the challenge now is that, despite our worldwide progress, the need is way bigger than that and we are way too small. We are a small charity based in Oxford, no buildings, three staff, all part-time, very good Board, chaired by James, and yet we are running on a shoestring. Whenever we go to donors and we seek funding for this kind of work and we say ‘We really need to step this up to really match the global scale and roll it out vastly around the world’ they say ‘Well, we could give you large amounts of money but you’re too small to receive it’.
Now, I can tell you I have in my history worked for big international NGOs and big companies in management; I have been CEO four times; and one of the organisations I was with works in billions of dollars, not millions, and I know that they can walk into large donors and sign contracts in the 100 million range, not easily but it happens. We can’t do that. If we try they say ‘No, you are way too small’. We are struggling to run our organisation on less than £100,000 a year, working in 77 countries and having only 3 staff. If you just do the maths of that, it is almost impossible.
So we have to see massive change and we are on the hunt for somebody who can help us, someone that can put money into the organisation to strengthen us, create the base, resource us to have a small increase in staff who can write proposals, prepare documents, access donors and show that we are worth it; and then we are looking for people who can open doors, who can give us access to philanthropists, to companies, to government.
And what I would like to close with is this: to appeal to you, to ask you to go home tonight and say ‘What doors can I open?’ I am asking you now what doors can you open that would give us an entrée to influential people who can help turn this appalling situation you have seen into something where we can roll out the answer we know works and change the situation for millions of young adults in the most vulnerable places of the world.
So be part of that with us, please. Join us in the journey. Come and be our friends and help us to make this a reality, and I hope, if it works, you will invite us back in two or three years and we will tell you the results. Hopefully they will be good. And in the meantime, visit us at www.lifesavingaction.org and www.primarytraumacare.org!
Thank you very much. [Applause]