
Abstract
The present study examines how different chronic illnesses and mental illness comorbidity (chronic illness with complexity [CIC]) associate with components of advance care planning (ACP). We also explore the role self-perceived burden plays in the relationship between illness and ACP. Data were gathered from a cross-sectional survey of 305 elderly participants from the New Jersey End-of-Life study. Participants with diabetes and those with cardiovascular disease (CVD) are less likely, while participants with CIC are more likely, to plan for the end-of-life. Participants with diabetes are less likely to make formal plans, whereas those with CVD are less likely to hold informal discussions. CIC is associated with increased odds of having an advance directive, but no other form of ACP. Self-perceived burden did not appear to be the gateway by which illness groups differentially engaged in ACP. Future research should investigate what aspects of illnesses drive ACP.
Recent enactment of the Patient Protection and Affordable Care Act (U.S. Department of Health and Human Services, 2010) in the United States, and the rhetoric surrounding it, has brought the issue of advance care planning (ACP) from the obscurity of hospital in-take paperwork to the forefront of national consciousness. All 50 states have enacted some form of legislation to promote ACP, which consists of a variety of legally binding documents that specify an individual’s preferences at the end-of-life (EOL) in the absence of autonomy due to cognitive or physical incapacity. These ACP documents generally fall into three categories: (a) advance directive/living will (AD/LW), instructions about type of EOL care and medical interventions desired by a patient; (b) durable power of attorney for health care (DPAHC), health-care surrogate to make medical decisions at the EOL; (c) will, estate and financial planning documentation. In addition to legislative incentives, there appear to be many psychosocial, economic, and quality-of-life benefits to engaging in ACP. Discussions with physicians about ACP resulted in better understanding of future treatment options and reduced fear and anxiety among patients (Ditto et al., 2001; Smucker et al., 1993). Patients who have formulated ADs also report that they have fewer concerns regarding communication, have greater satisfaction with their care, and demonstrate greater hospice use (Bischoff, Sudore, Miao, Boscardin, & Smith, 2013; Ditto et al., 2001; Smucker et al., 1993; Teno, Sabatino, Rouse, & Lynn, 1993; Tierney et al., 2001). Temel et al. (2010) found that when patients and families engage in early discussions about the explicit goals of palliative care, this improves quality of life, mood, and compellingly, patient survival. Contrary to rhetoric surrounding death panels, individuals seem willing to discuss EOL plans and are open to the concept of ADs (Morrison & Meier, 2004). These findings are not limited to American adults, but extend internationally, as well. A study conducted by the Japanese Ministry of Health, Labour, and Welfare revealed that almost 75% of older Japanese adults show positive dispositions toward LWs (Matsui, 2007).
ACP is becoming increasingly important due to the changing nature of the EOL. The EOL is no longer an abrupt event but is instead characterized by a sometimes lengthy state of chronic illness. Moreover, the convergence of chronic physical illness with mental illness, termed chronic illness with complexity (CIC), can further necessitate engaging in ACP. CIC occurred in roughly 31% of diabetics and led to greater diabetes-related complications (Banerjea, Sambamoorthi, Smelson, & Pogach, 2007). Task and social role functioning is also profoundly negatively impacted when chronic physical illness is accompanied by mental health morbidity (Druss et al., 2008; Lee, 2009). However, ACP is often studied within the context of a single chronic illness or context (e.g., cancer patients, terminally ill in a nursing home setting; Dow et al., 2010; Hall & Jenson, 2014; Happ et al., 2002; Schonfeld, Stevens, Lampman, & Lyons, 2011). In fact, most studies intentionally exclude those with comorbidities due to the complexity this generates. However, comorbidity happens and is likely to impact EOL preferences and ACP, particularly when the comorbidity is mental illness.
Despite potential benefits and legislative incentives, rates of ACP remain surprisingly low. Fewer than 50% of critically or terminally ill patients (Kass-Bartelmes & Hughes, 2004) and fewer than 30% of older individuals in general (Later & King, 2007) have an AD. The low prevalence of ACP is undoubtedly multifactorial. Socioeconomic factors have emerged as one of the primary predictors of ACP; those who are European American (EA), well educated, and upper class preferentially engage in ACP. Minorities are less likely to engage in ACP (Degenholtz, Arnold, Meisel, & Lave, 2002; Hopp & Duffy, 2000; Teno, Gruneir, Schwartz, Nanda, & Wetle, 2007; Waters, 2000), with African Americans (AAs) and Hispanics less likely than EAs to have formal ACP or conversations with family about EOL planning (Carr, 2012; Hopp & Duffy, 2000; Smith et al., 2008) and less likely to know about ACP altogether (Waters, 2000); 70% of those with high levels of educational attainment engaged in ACP (Carr & Khodyakov, 2007), although the high degree of racial homogeneity (>90% EA) likely makes this estimate greater than for the general population.
Self-Perceived Burden and the Common-Sense Model of Illness Representation
Another emergent factor associating with ACP is burden. Individuals have expressed concern with not being a physical burden (84%) or financial burden (62%; Dinger, 2005). Impairments in crucial aspects of daily functioning are central to the construct of self-perceived burden (SPB), which has implications for ACP. SPB may negatively affect treatment adherence, use of EOL medical interventions, and ACP (Cousineau, McDowell, Hotz, & Hebert, 2003). ACP is often used as collective outcome encapsulating LW, estate planning, and DPAHC; yet, the burden literature suggests that SPB may have very different implications for AD/LW and DPAHC. For example, one may be afraid to appoint a DPAHC for fear of increasing the burden of responsibility to others, whereas an AD/LW may be seen to ease caregiver burden since the decision-making process has been completed by the patient. In addition to its relationship with ACP, SPB has also been associated with depression (Wilson, Curran, & McPherson, 2005). SPB has mainly been studied in caregivers and rarely from the patient’s perspective.
Our model of SPB is derived from the common sense model (CSM) of illness representations (Leventhal, Brissette, & Leventhal, 2003) and incorporates both the self and other. The CSM asserts that individuals are active problem solvers who use changes in tangible physical experiences as cues to understand illness and future health status, make comparisons to prior experiences of self and others, and ultimately use these representations to guide behavior. Using the CSM as our theoretical foundation, we propose that different chronic illnesses (i.e., physical experiences) will show varying degrees of burden (i.e., representations of consequences) and thus associate with different advance care plans (i.e., health behavior). Our study will examine whether ACP differs across three different chronic illness diagnoses that subsume the largest portion of chronic illness diagnosis and medical expenditures: diabetes, cardiovascular disease (CVD), and cancer. Unlike prior studies, we will compare across multiple diagnoses and investigate how comorbid mental illness (CIC) relates to ACP and whether individuals with multiple physical chronic illnesses (e.g., diabetes and CVD) engage in ACP differently. Hence, this article seeks to answer the following questions: (a) Will patients with different chronic illnesses engage in ACP differently? (b) Do those with CIC differ from those without comorbid mental illness in likelihood of engaging in ACP? (c) Does SPB mediate associations between diagnoses and ACP, and between CIC and ACP?
Methods
Participants
The New Jersey End-of-Life (NJEOL) study sample consists of data from 305 noninstitutionalized older adults in New Jersey, 55 years of age and older. Patients were recruited to participate if they were either English- or Spanish-speaking, had no cognitive limitations, and had one or more of the following health conditions: cancer, type II diabetes, or congestive heart failure (CHF). A group of patients without these diagnoses was also recruited to provide a comparison sample. Recruitment was conducted over the telephone from two large university hospitals and one cancer center in New Jersey. The initial sampling frame consisted of a pool of 1,146 patients identified as potential recruits for the study through the University of Medicine and Dentistry New Jersey, general internal medicine department.
Three hundred and five participants were locatable, met exclusion and inclusion criteria, and consented to participate in the study, representing 27% of the original potential pool. This low response rate was due mainly to functional attrition rates, patients either being too ill to participate or having died during the recruitment period, and cognitive limitations precluding participation, in addition to the general reluctance for patients at the EOL to participate in such a study. The interview process consisted of a one-and-a-half hour face-to-face structured interview with a trained graduate student interviewer. The survey included questions regarding sociodemographics, religion or spirituality, social support, health status and behaviors, attitudes toward treatments, and ACP.
Dependent Variables
The dependent variable of interest in this study was whether respondents had engaged in ACP. The survey queried respondents whether they had made, or had discussions with others about, plans or preferences for their future health care. These plans could range from informal conversations with families and friends to more formal EOL planning activities such as AD/LW or naming a DPAHC. To assess informal engagement in planning, respondents indicated whether they had discussed their preferences at the EOL with their loved ones. Formal EOL planning was assessed by respondents indicating a Yes or a No to the following two questions: (a) “Do you have a living will or an advance directive? This is a set of written instructions about the type of medical treatment you would want to receive if you were unconscious or somehow unable to communicate.” (b) “Have you made any legal arrangements for someone to make decisions for you about your medical care, if you become unable to make those decisions for yourself? This person is sometimes called a Durable Power of Attorney for Health Care.” The outcomes for ACP were three binary variables describing whether respondents had engaged in different measures of EOL planning: engaging in informal discussions of ACP, drafting an AD/LW, and appointing a DPAHC. We conducted separate models, as we anticipated that different factors may drive each outcome.
Key Independent Variables
There were two main independent variables in our analyses: chronic illness category and CIC. Chronic illness category comprised a categorical variable with five levels, based on patient reports of ever having been diagnosed with or treated for one of the following chronic conditions: (a) diabetes; (b) CVD (including myocardial infarction, hypertension, and CHF); (c) diabetes and CVD; (d) comorbid cancer (cancer in addition to diabetes or CVD); and (e) other diagnosis (e.g., respiratory disease, ulcers, kidney disease, seizures, hepatitis, and tuberculosis). As expected in a study examining patients at the EOL, very few had no chronic illness and as such the other diagnosis group was used as referent in all analyses as a proxy for a true control group. CIC was specified as the presence of comorbid chronic physical and mental illness (present or past history of depression and anxiety, indicated by ICD-9 codes in patient charts).
An important covariate in these analyses was the number of comorbid physical conditions experienced by patients. Each subject was read a list of health conditions and asked whether a doctor had told them that they have such a condition or whether they were taking medication for such a condition. The conditions were as follows: asthma, lung problems, diabetes, cancer, ulcers, heart disease, high blood pressure, heart attack, seizures, hepatitis, kidney problems, tuberculosis, and depression or anxiety. The number of health conditions reported ranged from 0 to 9 health conditions, with only nine respondents reporting no comorbid health conditions at all.
Mediator or Moderator Variables
Perceiving illness as a burden (SPB) was the key mediator variable in this analysis. The four survey questions that comprised the “perceived illness burden” scale (each rated from 1 = strongly disagree to 5 = strongly agree) captured patients’ characterization of their illness as a burden to themselves and to friends or families. The items in the SPB scale were as follows: (a) “My illness has major consequences for my daily life.” (b) “My illness causes difficulties for those who are close to me.” (c) “The treatment for my illness has major consequences for my daily life.” (d) “The treatment for my illness causes difficulties for those who are close to me.” Principal components factors analysis yielded a single factor with high inter-item reliability (Cronbach’s α = .863). Scores for the 267 participants who answered the four questions ranged from 1.00, indicating a low SPB, to 5.00 indicating high SPB. For the 32 respondents who were not asked or did not answer the questions in the survey, mean imputation was used to address the missing information from the four variables used to construct the scale. While a dummy variable was created and factored into the analysis to ascertain whether those 32 nonrespondents differed from those who answered the questions, inclusion of this flag variable did not significantly alter results and as such findings are reported without it.
Control Variables
Other variables controlled in this preliminary analysis included age (in years), gender (male referent), education (highest level completed, with less than high school, high school referent, and college degree), marital status (married referent, widowed, or divorced or never married), and recent experience with death of a loved one. Race or ethnicity was coded into four categorical dummy variables: EA non-Hispanic (referent), AA non-Hispanic, Hispanic/Latino, and other. Due to the breadth of literature illustrating the significance of race and ethnicity on ACP (Degenholtz et al., 2002; Hopp & Duffy, 2000; Teno et al., 2007; Waters, 2000), we controlled for race or ethnicity in the second block of all models.
Analytic Approach
Appropriate transformations were performed on variables as outlined earlier. Using Stata 11 SE software, we examined the sample characteristics of the diagnostic categories with chi-square and analysis of variance (ANOVA). Three separate step-wise logistic regression models were run to assess the relationship between chronic illness diagnosis and three distinct forms of ACP: having an AD/LW (Model 1), appointing a DPAHC (Model 2), and having discussed EOL preferences (Model 3). Each model consisted of six nested steps: primary predictors (Block 1); race, gender, and age (Block 2); marital status (Block 3); educational attainment (Block 4); recent death of significant other (Block 5); and number of comorbid physical conditions and SPB (Block 6).
Results
Bivariate Analyses
Descriptive Statistics for all Variables Used in Regression Analyses.
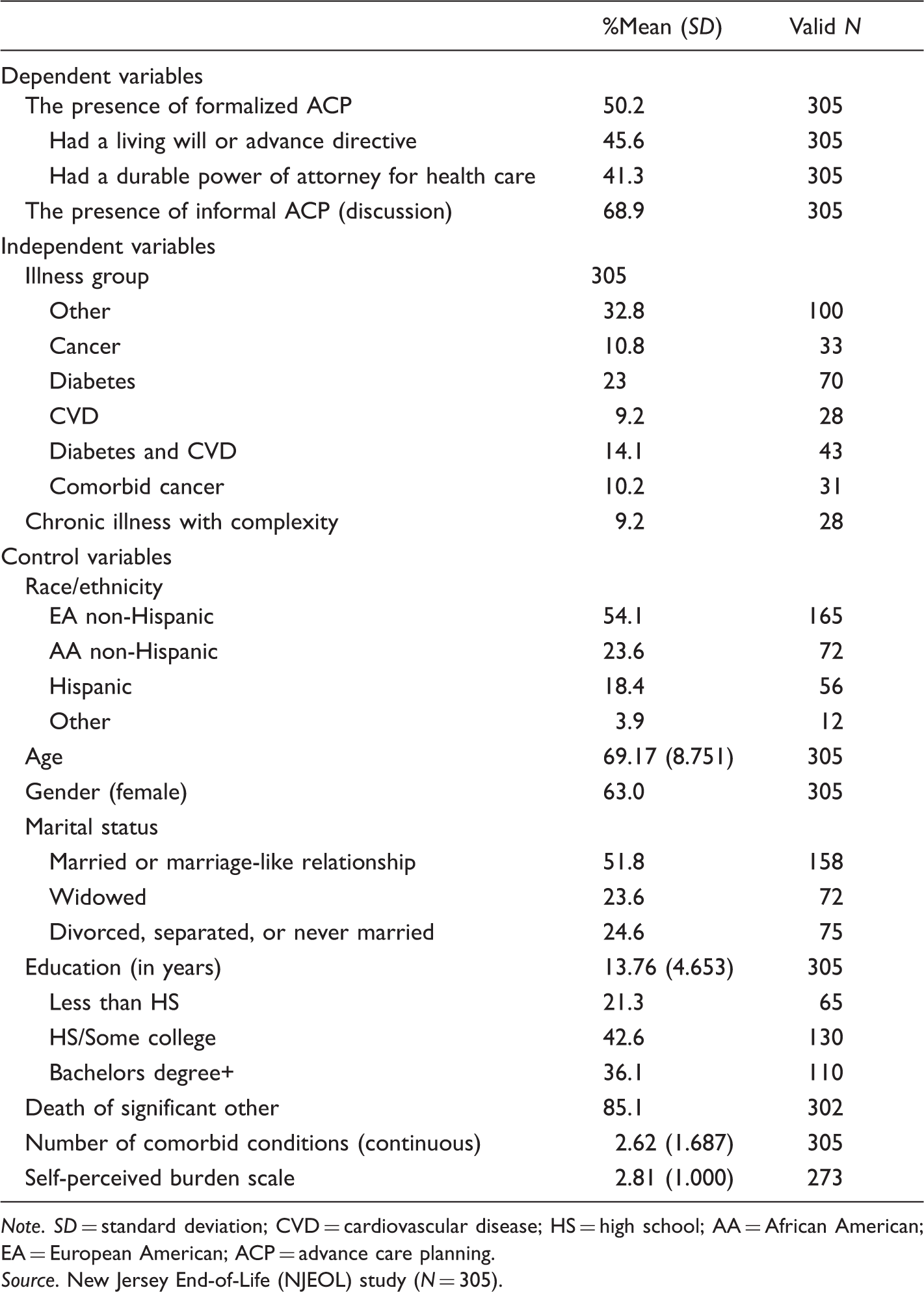
Note. SD = standard deviation; CVD = cardiovascular disease; HS = high school; AA = African American; EA = European American; ACP = advance care planning. Source. New Jersey End-of-Life (NJEOL) study (N = 305).
Means (Standard Deviations) and Proportions for all Variables Used in Analyses, by Illness Category.

Note. NJEOL = New Jersey End-of-Life; SPB = self-perceived burden; ANOVA = analysis of variance; DPAHC = durable power of attorney for health care; AD/LW = advance directive/living will. Source. NJEOL study (2005–2008). N = 305. Asterisks denote significance level of either F- (for ANOVA) or χ2 statistic, where †p ≤ .10, *p ≤ .05, **p ≤ .01, ***p ≤ .001. Bonferroni post hoc comparisons were used for ANOVA.
Means (Standard Deviations) and Proportions for all Variables Used in Analyses, by Depression and Anxiety diagnosis.
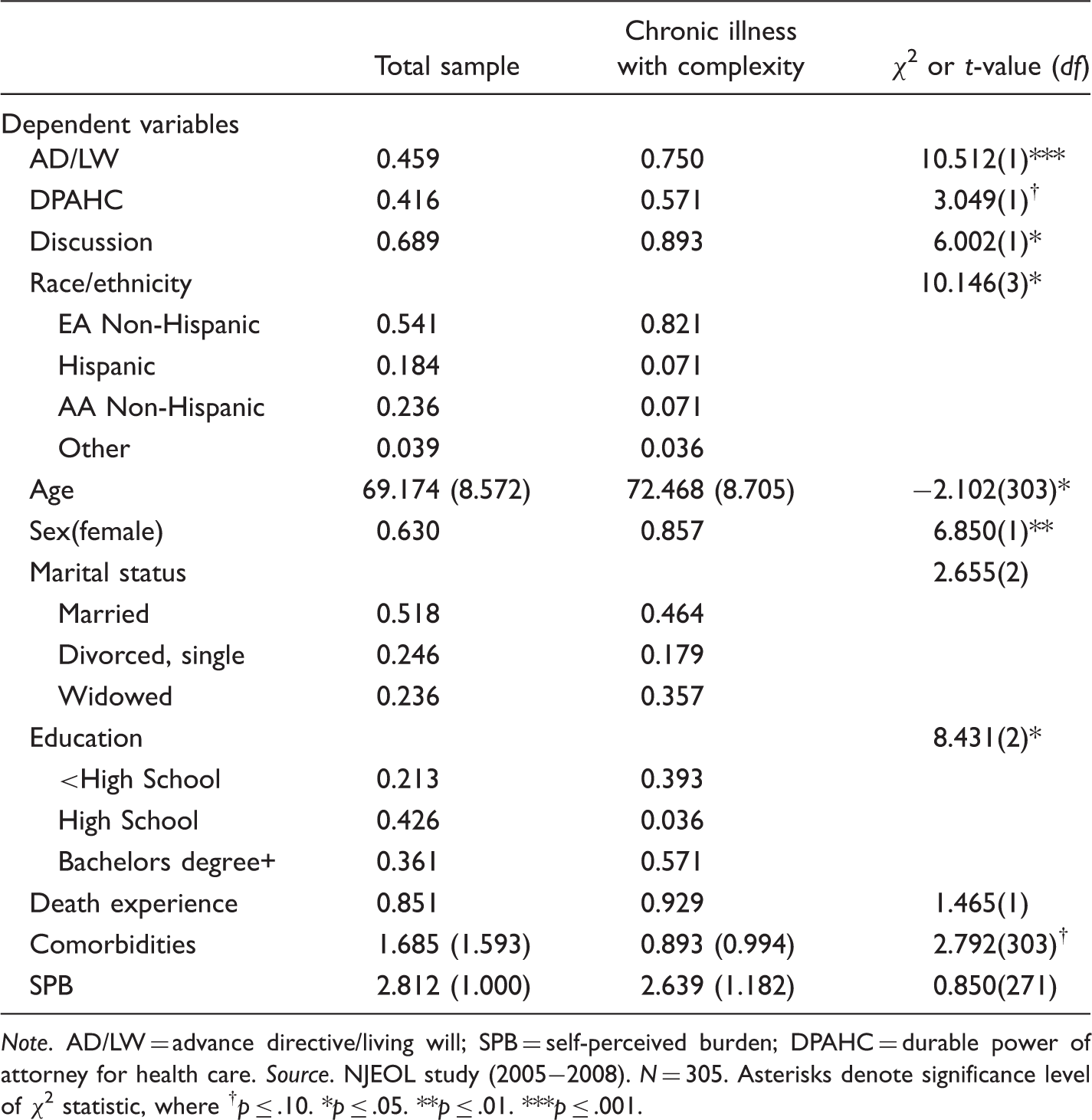
Note. AD/LW = advance directive/living will; SPB = self-perceived burden; DPAHC = durable power of attorney for health care. Source. NJEOL study (2005−2008). N = 305. Asterisks denote significance level of χ2 statistic, where †p ≤ .10. *p ≤ .05. **p ≤ .01. ***p ≤ .001.
ANOVAs were conducted to determine whether chronic illness groups differed from one another on all continuous measures (see Table 2), and chi-square was conducted to examine distributions for categorical measures. These bivariate analyses revealed significant illness group differences in ACP. While a full 60% of diabetics have discussions about EOL preferences, only 25% actually formalize these preferences in the form of either AD/LW or DPAHC. Individuals with cancer are most likely to have both informal (80%) and formal (roughly 60%) ACP. We also observe sociodemographic and health differences between the illness groups. Both cancer groups are predominantly well educated, male, and non-Hispanic EA, which are factors associated with greater propensity for making EOL plans. The cancer group also has a higher proportion of individuals with comorbid mental illness (CIC). The diabetes + CVD group reported higher levels of SPB than the group with other chronic illnesses.
The same comparisons were made to examine whether individuals with comorbid physical and mental illness (CIC) differed from participants without comorbid mental illness. Chi-square was used to examine distributions for categorical measures and t tests were used to examine differences in continuous measures. CIC is associated with a greater tendency to plan, with 89% of these participants having engaged in an EOL discussion and 57% formalizing these discussions by appointing a DPAHC and 75% having an AD/LW. Participants with CIC were predominantly EA non-Hispanic, female, and well educated.
Multivariate Analyses
Three Separate Binomial Models From Multivariate Logistic Regression Examining the Relationships Between Key Independent Variables (Chronic Illness Diagnosis [CIC]) and ACP.

Note. AD/LW = advance directive/living will; CVD = cardiovascular disease; DPAHC = durable power of attorney for health care; ACP = advance care planning. Source. NJEOL study (2005 − 2008). N = 305. Β = odds ratio (exponentiated β), CI = 95% confidence interval. Other illness omitted as reference group; non-Hispanic White omitted as reference group; married or living in marriage-like relationship omitted as reference group; high school as highest educational attainment omitted as reference group. Asterisks denote significance level, where †p ≤ .10. *p ≤ .05. **p ≤ .01.
AD/LW
In the first block, participants with cancer are 3 times as likely and those with comorbid cancer are 2.8 times as likely to have an AD/LW. Similarly, relative to those without comorbid mental illness, those with CIC are 5.4 times as likely to have an AD/LW. However, when race, sex, and age are controlled for in the second block, the effect for both cancer groups drops out. Thus, the association observed between cancer and ACP was a residual of these established sociodemographic factors (particularly race and sex). CIC maintained a strong, significant association with increased odds of having an AD/LW throughout all blocks of the model, to result in those with CIC having 3.8 times the odds of having an AD/LW. Unfortunately, the sample size was too small to run any interactions between comorbid mental illness and the chronic illness groups.
Diabetics, on the other hand, have 46% the odds of having an AD/LW. The relationship between diabetes and reduced odds of having an AD/LW was diminished when sociodemographic variables were entered. Although the inclusion of race and sex diminished the relationship between diabetes and AD/LW, it regained significance in the final model to demonstrate 37% the odds of having an AD/LW when comorbidities and SPB were entered. This suggests that the borderline significant effect of SPB on AD/LW was masking the full effect of diabetes on this measure of ACP.
In the final block, relative to non-Hispanic EAs, Hispanics have 9%, non-Hispanic AAs have 34%, and those who self-identified as another race have 10% the odds of having an AD/LW. Relative to males, females have 47% the odds of having an AD/LW.
DPAHC
Relative to those with other chronic illnesses, diabetics have 44% the odds of having appointed a DPAHC. Diabetics maintained significantly reduced odds of appointing a DPAHC when sociodemographic, relationship, and health variables were included. In the final model, diabetics showed 37% the odds of appointing a DPAHC, while experiencing the death of a loved one and perceiving the self as burdensome increased the odds by factors of 2.8 and 1.4, respectively. In the final block, relative to non-Hispanic EAs, Hispanics have 6%, non-Hispanic AAs have 38% the odds of appointing a DPAHC. Females have 44% the odds of appointing a DPAHC relative to males.
Informal discussions
Those with CIC are 5.5 times as likely to have engaged in an informal discussion about EOL preferences. As with formal planning, adding sociodemographic factors in the second block negated the effect of CIC on informal planning. The relationship between chronic illness group and informal plans did not clearly emerge until the final model when other health variables entered, in which participants with CVD showed 25% the odds of having had a discussion about EOL preferences. Regarding the effect of race and sex on informal planning, similar relationships were observed as seen in formal ACP. These sociodemographic findings are consistent with prior results from the same data set (Carr, 2011).
Summary of Results
Final Multivariate Models for Each of the Three Dependent Variables.
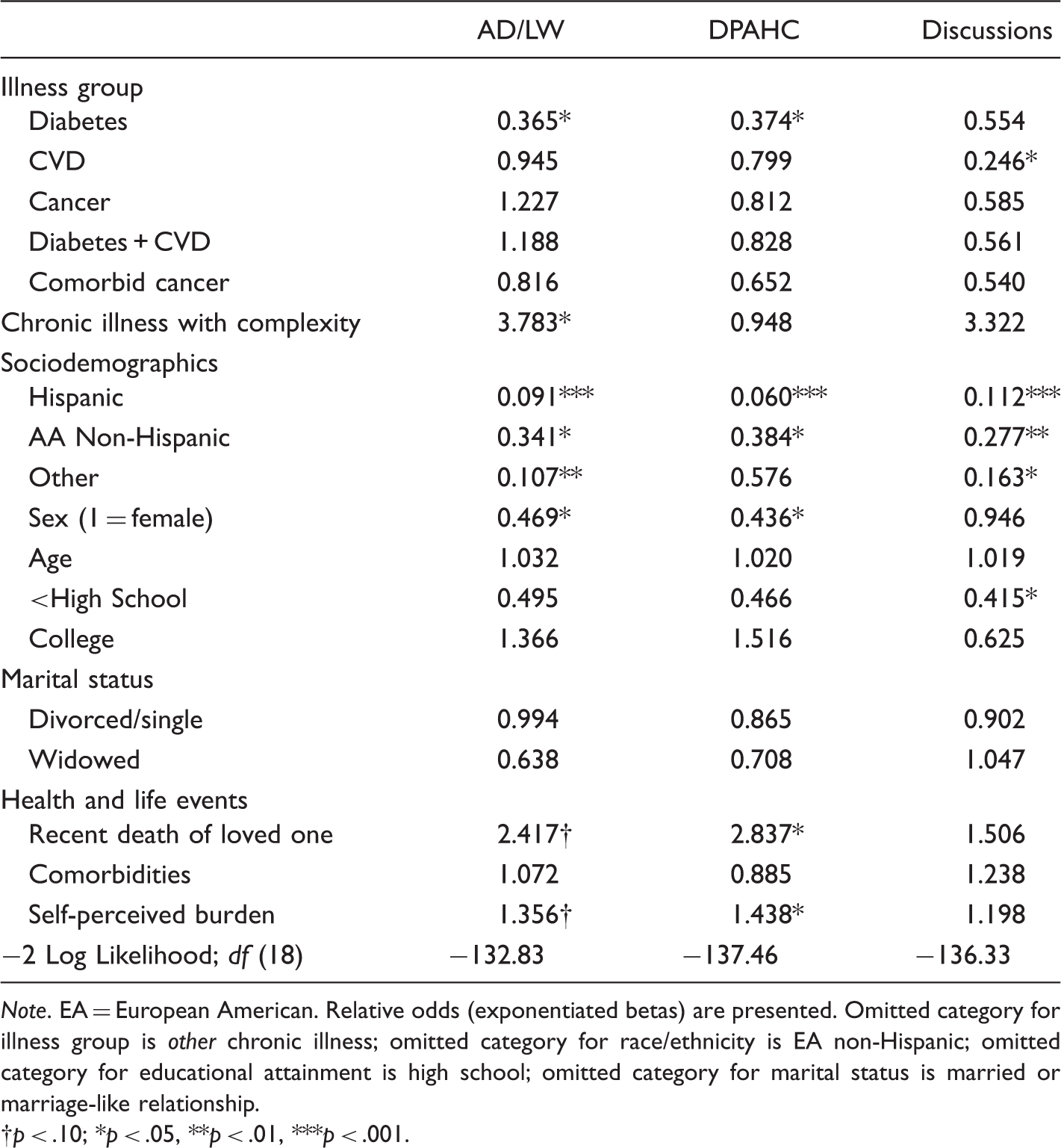
Note. EA = European American. Relative odds (exponentiated betas) are presented. Omitted category for illness group is other chronic illness; omitted category for race/ethnicity is EA non-Hispanic; omitted category for educational attainment is high school; omitted category for marital status is married or marriage-like relationship.
p < .10; *p < .05, **p < .01, ***p < .001.
Discussion
This study has demonstrated that the type of chronic illness an individual has impacts their choices about advance care plans at the EOL. Individuals with a diagnosis of diabetes or CVD are less likely to make ACP. Also, as hypothesized, different chronic illnesses associate with different types of EOL planning. While diabetes is associated with decreased likelihood of engaging in both forms of formal planning, individuals with CVD are less likely to engage in informal discussions with loved ones. These findings are consistent with the CSM, in which both are relatively asymptomatic conditions, thus being less likely to activate representations that would guide action. Consistent with prior studies (De Gendt, Bilsen, Stichele, & Deliens, 2013; Lau et al., 2010; Meeussen et al., 2011), those diagnosed with cancer are more likely to engage in ACP, although we found this to be a residual of other sociodemographic factors. In prior studies, cancer was compared with all noncancer diagnoses (Lau et al., 2010; Meeussen et al., 2011) and the outcome derived from health-care practitioner reports of documented ACP, not on patient reports; thus, the important aspect of discussions was not included in prior studies. This study provides a more nuanced description of how illness diagnosis can influence both components of formal planning and informal planning.
Perhaps the most unexpected finding is the discovery that comorbid mental illness associated with increased planning—a finding contradictory to the literature (e.g., Foti, Bartels, Merriman, Fletcher, & Van Citters, 2005). However, most of the literature examining mental health and ACP focuses on serious mental illnesses, such as dementia or psychosis (Dickinson et al., 2013; Foti et al., 2005), and their association with psychiatric ADs (Srebnik et al., 2005; Swanson et al., 2006). It is possible that people with less severe mental disorders maintain the cognitive resources and motivation to plan for the EOL. Moreover, those with cancer had higher rates of CIC, and Gonen et al. (2012) found that death anxiety was highest in cancer patients with comorbid psychiatric illness. It may be that CIC in cancer patients preferentially activates death anxiety, which associates with greater likelihood of formal planning but further research is needed to confirm this mechanism. Chronic illness diagnosis and CIC have an impact on ACP above and beyond race, sex, education, family relationships, and other health factors.
Contrary to our expectations, SPB did not act as a mediator between illness diagnosis and ACP. However, SPB did exert its own independent effect, increasing the odds of appointing a DPAHC. The nature of the sample once again may be the reason for this lack of SPB mediating the association between diagnosis and ACP behavior. We can theorize that these are people already at the EOL, dealing with (likely) lengthy chronic illness and death is a reality. Given the fact that over two thirds had discussions with loved ones, it seems reasonable that they expect their loved ones to know their wishes and thus feel comfortable appointing a DPAHC.
Limitations and Future Directions
The relatively small sample size precluded the ability to construct a more detailed look at within-diagnosis factors that may contribute to differences in ACP. Unfortunately, the sample size was also too small to examine how comorbid mental illness plays out within the context of each chronic illness group. Being able to further define what aspects of chronic physical and mental illness contribute to increased or decreased EOL planning behavior may enable more targeted interventions for increasing rates of ACP and thus ensuring a higher quality EOL. Diagnostic history should be an easily accessible piece of information that medical practitioners can readily use to identify patients most in need of EOL discussions. However, this highlights the need for an integrated system, in which information from specialists is shared across medical disciplines and available to all members of a patient’s care team. One avenue of future study could investigate whether patients with an integrated electronic medical record system have higher rates of ACP and whether the same findings for diagnostic groups remain in such a setting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Joanne Hash was supported by a National Institute of Mental Health training grant (AG023958), awarded to the Institute for Health, Health Care Policy & Aging Research.