
Abstract
The Frommelt Attitude Toward Care of the Dying Scale (FATCOD) is designed to assess the attitudes of professionals and trainees toward caring for the dying patient and their family members. In this study the main aim is to adapt the FATCOD to a Spanish context (FATCOD-S). In addition, the relations between FATCOD-S, sociodemographic variables, emotional intelligence, and death attitudes have been analyzed. A sample of 669 Spanish nursing students from four Universities responded to a questionnaire. The exploratory factor analysis (EFA) concludes a structure composed of two significant factors. A confirmatory factor analysis (CFA) was carried out. The CFA supported a two-factor model. Students with past experience of death and those who had received training in palliative care scored significantly higher on both factors of the FATCOD-S (p < 0.01). The FATCOD-S is an effective and valid tool for measuring the attitudes of Spanish nursing students toward caring for patients at the end of life.
Keywords
Introduction
The professional role of nurses often brings them into close contact with patients and families facing an end-of-life (EOL) situation, and they must therefore be able to manage and respond adequately to the suffering this entails (Ferrell & Coyle, 2008). However, the encounter with death and suffering is one of the experiences that nurses report finding most stressful (Costello, 2006; Peterson et al., 2010). Thus, there is evidence that continuous contact with the suffering of others can exert an emotional toll that requires considerable effort to manage (Wright, 2004), thus heightening the risk of compassion fatigue (Showalter, 2010; Slocum-Gori, Hemsworth, Chan, Carson, & Kazanjian, 2013). Consequently, there is a need for professionals with specific training in EOL nursing who are able to provide the high-quality care that these vulnerable patients and families require (Cummings & Bennett, 2012), while simultaneously maintaining their own emotional equilibrium. In this context, a number of studies (Barrere, Durkin, & LaCoursiere, 2008; Mallory, 2003; Wessell & Garon, 2005) have shown that attitudes and coping strategies regarding EOL care can be modulated and enhanced through education, and that such training reinforces more positive attitudes toward death and dying.
One of the most widely used instruments for assessing attitudes towards caring for the dying patient and their family is the Frommelt Attitude Toward Care of the Dying Scale (FATCOD; Frommelt, 1991), broadly used in nursing context.
Use of the FATCOD in the Nursing Context
The FATCOD scale has been used in numerous studies in the nursing context (Braun, Gordon, & Uziely, 2010; Dunn, Otten, & Stephens, 2005; Iranmanesh, Dargahi, & Abbaszadeh, 2008a; Lange, Thom, & Kline, 2008; Mallory, 2003; Matsui & Braun, 2010). Mallory (2003) applied the FATCOD to a sample of 104 North American nursing undergraduates in order to assess changes in their attitude toward care of the dying following a specific training program. The results indicated that training in EOL care and early practical experience of palliative care could lead to more positive attitudes toward caring for these patients. In another study conducted in the United States, Dunn et al. (2005) examined attitudes among 58 nurses working in oncology or medical/surgical units. They found that attitudes toward caring for dying patients and their families became more positive with greater professional experience. Based on their results, they suggest that undergraduate nurse training should include the teaching of strategies for coping with death and dying. Other studies have obtained similar results (Abudari, Zahreddine, Hazeim, Assi, & Emara, 2014; Braun et al., 2010; Lange et al., 2008), although it has also been highlighted that culture and religiosity can influence attitudes toward care of the dying. For instance, Matsui and Braun (2010), in their Japanese study involving 190 nurses and 177 caregivers, obtained mean FATCOD scores that were considerably lower than those reported by Dunn et al. (2005) in the United States and by Braun et al. (2010) with nurses in Israel, thus suggesting that Japanese nurses had less favorable attitudes toward care of the dying. Similarly, the mean FATCOD scores obtained by Iranmanesh et al. (2008a) in their study of Iranian nursing students were also lower than those reported in other cultural contexts.
Numerous studies, which have used FATCOD, have found that training in EOL care leads to more positive attitudes when working with the dying patient and his or her family members (Iranmanesh, Savenstedt, & Abbaszadeh, 2008b; Kassa, Murugan, Zewdu, Hailu, & Woldeyohannes, 2014; Matsui & Braun, 2010; Miyashita et al., 2007). Therefore, to assess the students’ attitudes toward caring for terminally ill persons and members of their families, before and after receiving specific training, it would be useful to detect training needs in this area. In a mixed-methods study of 21 North American nursing students who attended an educational workshop addressing critical moments in EOL care, Bailey and Hewison (2014) observed a significant improvement in attitudes toward caring for the dying. The qualitative data revealed that nurses felt the workshop to have been a valuable learning opportunity that had enabled them to share experiences with peers, as well as being a good way of linking theory and practice. Another factor that has been shown by research to favor more positive attitudes toward EOL care is previous contact with death and dying (Hagelin et al., 2016; Leombruni et al., 2014) whereas according to Iranmanesh et al. (2008a), the fear of death can lead to less positive attitudes toward the dying patient.
In addition to the need for adequate training in EOL care, other authors (Aradilla-Herrero, Tomás-Sábado, & Gómez-Benito, 2012–2013; Edo-Gual, Tomás-Sábado, Bardallo-Porras, & Monforte-Royo, 2014; Jack & Wibberley, 2013) stress the importance of including complementary training in social and emotional skills as part of undergraduate nurse education. The idea here is that such training can help student nurses not only to develop more positive attitudes toward care of the dying patient, but also to cope more effectively with suffering and loss, at less emotional cost to themselves and with less anxiety about death.
Characteristics of the FATCOD.
Frommelt (1991) developed the FATCOD (Form A) to assess nurses’ attitudes toward caring for terminally ill persons and members of their families. The instrument consists of 30 Likert-type items that are scored on a 5-point scale (see Appendix A). Items 1, 2, 4, 10, 12, 16, 18, 20, 21, 22, 23, 24, 25, 27, and 30 are all positively worded, while the remainder are framed negatively. Possible scores range from 30 to 150, and higher scores reflect more positive attitudes. Two-thirds of the items relate directly to a person’s attitudes toward the patient, while the remaining one-third relates directly to attitudes toward family members of the terminally ill person. Although the original tool was designed to assess nurses’ attitudes, Frommelt (2003) subsequently made some slight modifications and developed the FATCOD Form B to be used by persons from any discipline. The scale has been adapted and validated in several different languages, including Japanese (Nakai et al., 2006), Swedish (Henoch et al., 2014), and Italian (Leombruni et al., 2014).
Nakai et al. (2006) translated the FATCOD into Japanese (FATCOD-Form B-J) and, using principal component analysis (PCA), found evidence of two scale domains. The first factor, which they labeled FATCOD I (positive attitudes toward caring for dying patients), had an internal consistency (Cronbach’s α) of .73, while the second factor, FATCOD II (perceptions of patient and family-centered care), had an α value of .65. Internal consistency for the total FATCOD-Form B-J was .85.
Henoch et al. (2014) recently translated and adapted the FATCOD (Form A) into Swedish. To compare their results with those of studies carried out using the Japanese FATCOD (Matsui & Braun, 2010; Miyashita et al., 2007; Nakai et al., 2006), they applied PCA to examine a two-component solution. The two-factor solution obtained in the Swedish sample was similar to that reported for the Japanese version. The only item that loaded on a different factor was item 24. Internal consistency for the Swedish adaptation was .70 for FATCOD I, .57 for FATCOD II, and .60 for the total scale. As Cronbach’s α coefficients were fairly low for the total FATCOD and the two subscales, Henoch et al. recommend that the Swedish version of the scale should be used with caution, and highlight that its psychometric properties need to be examined further.
The factor structure of the Italian version of the FATCOD was examined using PCA in a study by Leombruni et al. (2014). Four factors accounting for 37.2% of the total variance were extracted: emotional engagement, beliefs about EOL care, beliefs about professional boundaries, and beliefs and feelings about dying. The authors state that the results cannot be generalized because the internal consistency of the Italian version of the FATCOD (Form B) was questionable. Specifically, α coefficients for the dimensions ranged between .72 and .11, with a value of .68 for the total FATCOD. Although several studies have used this scale in the nursing context (Braun et al., 2010; Dunn et al., 2005; Henoch et al., 2014), it has not, to the best of our knowledge, been adapted for use in the Spanish-speaking population. The translation and adaptation of the FATCOD scale to Spanish will provide a useful instrument to assess students’ and professionals’ attitudes toward caring for dying patients and their families.
Aims
The specific aims of the study were to adapt the FATCOD to a Spanish context (FATCOD-S), to test the dimensionality of the scale by means of CFA, and to estimate the reliability of the resulting scale dimensions. A further aim was to examine the relationship between FATCOD-S scores and a series of sociodemographic and training-related variables, as well as with respect to emotional intelligence and death attitudes.
Methods
Study Design and Participants
This was a cross-sectional study carried out among Spanish nursing students. A convenience sample of 685 nursing undergraduates was recruited from four universities. Of these, 669 students completed the questionnaire correctly.
Data Collection and Ethical Considerations
All the nursing students were informed about the study objectives and procedures prior to administration of the questionnaire. The questionnaire was administered to students during their regular class timetable between March and December 2013. All students were informed of the voluntary nature of the study, and it was made clear that all data would remain anonymous and confidential. The study was approved by the research ethics committee.
Instruments
The students completed a self-administered questionnaire that gathered the following sociodemographic data: gender, age, academic year, past experience of death and dying (experiencing the death of a close friend or relative, coming into contact with death during their clinical placements, and having seen someone die) and previous training in palliative care. In addition to the FATCOD-S, the questionnaire also included the following validated scales.
Collett–Lester Fear of Death Scale
The Collett–Lester Fear of Death Scale (CLFDS; Lester & Abdel-Khalek, 2003; Spanish adaptation by Tomás-Sábado, Limonero, & Abdel-Khalek, 2007) is a self-report instrument with 28 items that assess four dimensions of the fear of death: fear of death of self, fear of dying of self, fear of death of others, and fear of dying of others. Each subscale contains seven items that are rated on a 5-point Likert scale. Higher scores indicate a greater fear of death. Reported indices of internal consistency (Cronbach’s α) for each of the four subscales are .83 for death of self, .89 for dying of self, .79 for death of others, and .86 for dying of others (Lester & Abdel-Khalek, 2003). The corresponding α values in the present study were .79, .82, .80, and .80, respectively.
Death anxiety inventory-revised
The Death Anxiety Inventory-Revised (DAI-R; Tomás-Sábado, Gómez-Benito, & Limonero, 2005) is a 17-item scale for measuring death anxiety. Items are rated on a 5-point Likert scale from 1 (totally disagree) to 5 (totally agree). Possible scores range from 17 to 85, with higher scores corresponding to a greater degree of death anxiety. The Cronbach’s α coefficient in the original validation study was .89, compared with .88 in the present sample.
Trait meta-mood scale
The Trait Meta-Mood Scale (TMMS-24) was devised by Salovey, Goldman, Turvey, and Palfai (1995), and subsequently modified and adapted to Spanish by Fernández-Berrocal, Extremera, and Ramos (2004). The TMMS-24 is a 24-item scale that uses a 5-point Likert format (anchored by 1 = strongly disagree and 5 = strongly agree). The scale assesses people’s beliefs or perceptions about their emotional skills, and its subscales (eight items each) address three dimensions of emotional intelligence: attention to feelings, clarity of feelings, and mood repair. In the Spanish version of the scale validated in the nursing context (Aradilla-Herrero, Tomás-Sábado, & Gómez-Benito, 2014), the internal consistency of the subscales was .87 for attention, .87 for clarity, and .84 for repair. In the present sample, we obtained Cronbach’s α values for each of the TMMS dimensions of .81 for attention, .88 for clarity, and 0.83 for repair.
Translation Procedure
The Spanish version of the FATCOD (FATCOD-S) was created following a forward–backward translation design based on international guidelines (International Test Commission [ITC], 2005). We began by obtaining permission from Frommelt, the author of the original version, for the translation and validation of the instrument. The FATCOD was then independently translated from English into Spanish by four bilingual researchers who were specialized in EOL education; one of them was also an expert in the field of psychometrics. The translation of each item was then compared and discussed until consensus was achieved among all the researchers. Finally, the preliminary version was sent to a bilingual professional for back translation. The back translation was then compared with the original English version and discussed by the initial group of researchers in order to ensure that the translation was comprehensible. The final Spanish version of the FATCOD was then tested in a small sample of Spanish students to ensure that all its items were clear and easy to understand. Appendix B shows the Spanish version of the FATCOD.
Data Analysis
With the exception of the CFA, all data were analyzed using SPSS for Windows v21.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were obtained for age, gender, and other sociodemographic variables, while Pearson’s correlation coefficients were calculated between FATCOD-S scores and other measures (DAI-R, CLFDS, and TMMS-24). An analysis of variance (ANOVA) was performed across academic years.
The dimensional structure of the FATCOD-S was tested by CFA using the LISREL 8.8 program (Jöreskog & Sörbom, 2006a). Due to the ordinal nature of the data, the maximum likelihood robust method was used for estimation, with the polychoric correlations and their corresponding asymptotic covariance matrices being previously generated by means of the Prelis 2.8 program (Jöreskog & Sörbom, 2006b. Model fit was evaluated with the following indices: the Satorra–Bentler scaled chi-square (S–Bχ2), the root mean square error of approximation (RMSEA) and its relative confidence interval, the non-normed fit index (NNFI), the comparative fit index (CFI), and the Akaike information criterion (AIC). Following Kaplan (2000), indicators of a good fit are that S–B χ2 is not significant, that NNFI and CFI have values above .90 (acceptable) or .95 (good), and that the RMSEA has a value between .05 and .08 (acceptable) or below .05 (good). The AIC index has a comparative purpose and the model with the lower value shows the best fit.
Cronbach’s α coefficients were calculated to examine the internal consistency of the total scale and of the dimensions resulting from the CFA.
Results
Sample Characteristics
Of the 669 students who completed the questionnaire correctly, 539 (80.5%) were women and 130 (19.4%) men. They ranged in age from 17 to 49 years (M = 22.57; SD = 5.32), and were drawn from across four academic years (323 students from Year 1, 212 from Year 2, 90 from Year 3, and 44 from Year 4).
Reliability and Exploratory Factor Analysis
Reliability on all FATCOD items, measured by Cronbach’s α, was .76. After measuring sample adequacy by means of the Kaiser–Meyer–Olkin test (KMO = .89) and Batlett’s test of esphericity (p < .01), responses to the 30 FATCOD items were analyzed by principal components analysis followed by ortogonal varimax rotation. The sequence of eigenvalues and explained variance suggests that the most consistent factor solution is formed by two factors which together accounted for 26, that is, 16% of the total variance.
The first factor, labeled care attitudes, accounted for14.11% of the variance and presents the highest factor loadings on items 13, 3, 26, 14, 5, 15, 6, 9, 11, 8, 7, 19, and 28.
The second factor accounts for 9.05% of the variance and was labelled perception of the family. It presents the highest factor loadings on items 21, 22, 16, 18, 4, 17, 27, 20, 24, 23, 30, 12, and 1. Four of the items (2, 29, 10, and 25) do no present significant loads in either factors.
Confirmatory Factor Analysis
To test the dimensional structure of the FATCOD-S, four competing models were compared.
The model proposed by Frommelt (1991), which formulates the FATCOD-Form A as a unidimensional scale. The model of Nakai et al. (2006), which found evidence for two factors (Factor 1: positive attitudes toward caring for dying patients, which includes items 1, 2, 3, 5, 6, 7, 8, 9, 11, 13, 14, 15, 17, 26, 29, and 30; and Factor 2: perceptions of patient and family-centered care, which includes items 4, 12, 16, 18, 19, 20, 21, 22, 23, 24, 25, 27, and 28). Item 10 was eliminated. The model described by Henoch et al. (2014), which proposes a two-factor scale that is consistent with the Japanese version (Nakai et al., 2006), except for Item 24 loading on Factor 1. Item 10 was eliminated. the model of Leombruni et al. (2014) based on four factors: Factor 1: emotional engagement (Items 3, 5, 7, 11, 13,14,15, 17, and 21), Factor 2: beliefs about EOL care (Items 4, 6, 16, 18, 19, 22, and 28), Factor 3: beliefs about professional boundaries (Items 10, 18, 20, and 24), and Factor 4: beliefs and feelings about dying (Items 1, 2, 8, 25, 26, and 29). Items 9, 12, 23, and 30 were eliminated.
CFA Goodness-of-Fit Statistics.
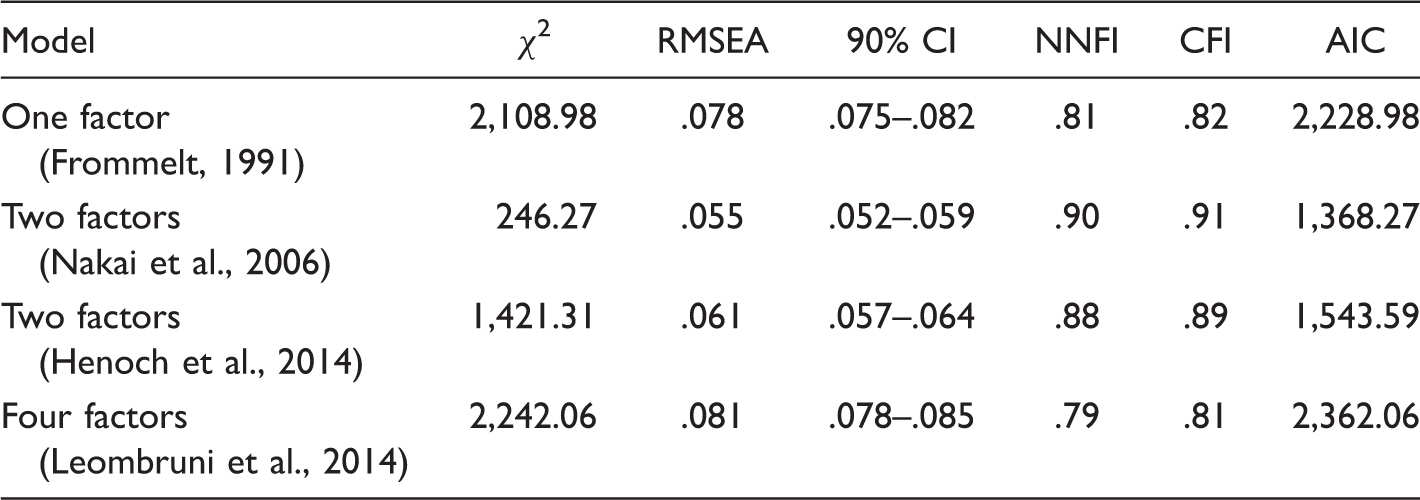
AIC = Akaike information criterion; CFI = comparative fit index; CI = confidence interval; NNFI = non-normed fit index; RMSEA = root mean square error of approximation.
FATCOD-S Scores in Relation to Sociodemographic and Training-Related Variables
Comparisons of FATCOD-S Scores According to Gender, Past Experience of Death and Dying, and Previous Training in Palliative Care by Mean of the t test.
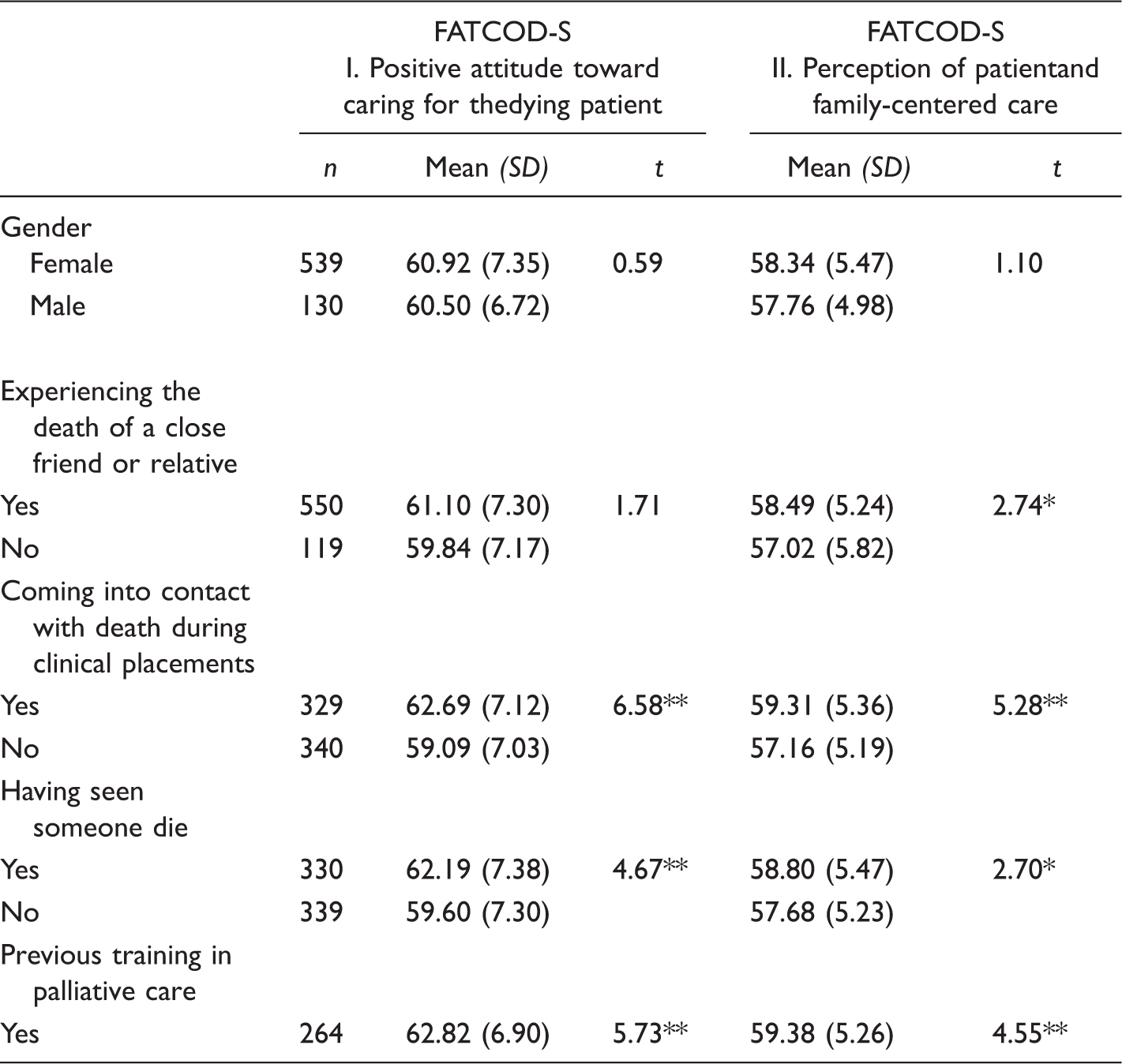
FATCOD-S = Spanish version of the Frommelt Attitude Toward Care of the Dying Scale; SD = standard deviation.
p < .05. **p < .01.
Students who had come into contact with death and dying during their clinical placements, those who had seen someone die, and those who had received training in palliative care scored significantly higher on both FATCOD-S factors than did their peers without these experiences (p < .01).
Comparisons of FATCOD-S Scores According to Academic Year and Results of the ANOVA (F).
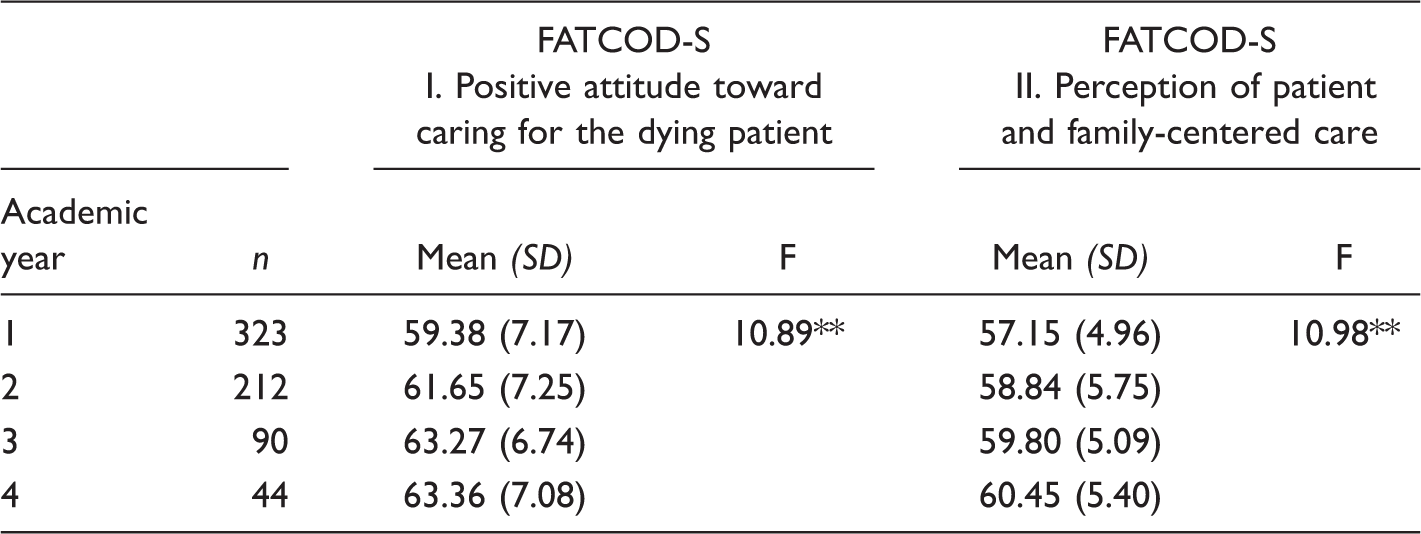
ANOVA = analysis of variance; FATCOD-S = Spanish version of the Frommelt Attitude Toward Care of the Dying Scale; SD = standard deviation.
p < .05. **p < .01.
Correlation with Other Variables
Pearson’s Correlation Coefficients Between the two FATCOD-S Dimensions and Scores On Death Anxiety (DAI-R), the Four Dimensions of fear of Death (CLFDS) and the three Dimensions of Emotional Intelligence (TMMS-24).

CLFDS = Collett–Lester Fear of Death Scale; DAI-R = Death Anxiety Inventory-Revised; FATCOD-S = Spanish version of the Frommelt Attitude Toward Care of the Dying Scale; TMMS-24 = Trait Meta-Mood Scale.
p < .05. **p < .01.
Regarding the relationship between the FATCOD-S and the three dimensions of emotional intelligence, the results showed that clarity and repair were positively and significantly (p < .01) associated with both scale factors.
Discussion
No previous study of the FATCOD in the nursing context has conducted a psychometric analysis that includes CFA of the scale’s dimensions. In developing the Spanish version of the FATCOD, we tested the four models proposed in the literature: a unidimensional structure based on the construct attitudes toward care of the dying, as formulated by the author of the original scale (Frommelt, 1991, 2003); the two-factor models proposed by Nakai et al. (2006) and Henoch et al. (2014) following exploratory factor analysis; and the four-factor model proposed by Leombruni et al. (2014). The two-factor model described by Nakai et al. showed the best fit to the data obtained in the Spanish validation, and it should be noted that this model is also one of the most widely used in research with the FATCOD (Mahiro, Takash, & Satoko, 2014; Matsui, Kanai, Kitagawa, & Hattori, 2013; Yoshioka, Moriyama, & Ohno, 2013). The fit indices obtained indicate that the two two-factor models are more appropriate than the unidimensional or the four-factor model, and of the two, the model of Nakai et al. shows the best fit to the data obtained in the Spanish context.
As already noted, the scale comprises two factors, one referring to attitudes toward care of the dying patient, and the other to perceptions of patient and family-centered care. In terms of the content of the two factors, we consider that the nomenclature used by Nakai et al. (2006) to label the dimensions is appropriate for the Spanish version of the FATCOD.
Our results regarding age are similar to those reported by other authors (Dunn et al., 2005; Lange et al., 2008), as younger nurses had less positive attitudes toward EOL care. This is probably due to their more limited experience of loss or death, and to the fact that they are likely to have not yet developed effective strategies for coping with such situations. As Kastenbaum (2000) notes, however, these findings should be interpreted with caution as age per se is not a predictor of attitudes toward death.
With respect to academic year, the results show that attitudes toward care of the dying patient become more positive as nursing students progress through their training. This finding is consistent with previous reports (Aradilla-Herrero et al., 2012–2013; Edo-Gual, Tomás-Sábado, & Aradilla-Herrero, 2011). When students begin their training, they will have yet to experience the reality of the health-care setting, one in which they are likely to encounter terminally ill patients and where they will come into contact with the pain and suffering of others. This contact, together with their inexperience and lack of control, can become a source of stress for nursing students and lead them to have more negative attitudes toward caring for such patients. The fact that their attitudes subsequently become more positive suggests that their increasing experience and training in this context helps to minimize the impact of these stressful situations.
Regarding past experience of death, our results show that attitudes were more positive among those students who have previously come into contact with death. In a study of oncology nurses, Lange et al. (2008) likewise found that those with previous experience of caring for terminally ill patients reported more positive attitudes towards this role, a finding that led them to suggest that more training in EOL care could improve attitudes toward the care of these patients. Other authors (Dunn et al., 2005; Henoch et al., 2014) have similarly concluded that professional experience of palliative care is associated with more positive attitudes toward work of this kind. However, it should be noted that Barrere et al. (2008), in a study of North American nurses, found that previous experience of death was a predictive factor in the negative sense, as more positive attitudes were reported by nurses without such experience. These results suggest that a lack of contact with the reality of death and dying may mean that nurses have unrealistic attitudes towards EOL care, and that they underestimate the impact it can have. Given these discrepant findings, further research is needed on this topic.
With respect to previous training in palliative care, our analysis showed that this modulated attitudes toward care of the dying patient and his or her family, as attitudes were more positive among those nursing students who had received such training. This is consistent with the findings of Mallory (2003), who, in a study that included both an experimental and a control group of students nurses, found that those who underwent specific EOL training had more positive attitudes toward the care of these patients. Other studies in different cultural contexts (Hirakawa, Kimata, & Uemura, 2013; Nagamatsu, Natori, Yanai, & Horiuchi, 2014; Yoshioka et al., 2013) have similarly found that training in EOL care is a key factor in terms of improving attitudes toward working with dying patients and their families, and that it improves the quality of the care offered.
Regarding fear of death and death anxiety, our results show that the nursing students with more positive attitudes toward care of the dying patient were those who reported less fear of death on all four of the dimensions measured: fear of death of self, fear of dying of self, fear of death of others, and fear of dying of others. Positive attitudes toward care of the dying patient were also negatively correlated with death anxiety. These results are consistent with previous studies (Braun et al., 2010; Lange et al., 2008) showing that nurses who report a greater fear of death have less favorable attitudes toward care of the dying patient and his or her family.
A further objective of our study was to analyze the relationship between attitudes toward care of the dying patient and the three dimensions of emotional intelligence. The results show that students who scored higher on emotional clarity (i.e., the ability to understand the feelings aroused by coming into contact with death and suffering) and repair (i.e., the ability to manage their emotional states) held more favorable attitudes toward caring for the dying patient and his or her family. These findings are consistent with previous studies (Aradilla-Herrero et al., 2012-13; Aradilla-Herrero et al., 2014; Edo-Gual, Monforte-Royo, Aradilla-Herrero & Tomás-Sábado, 2015) showing that qualified and student nurses with higher levels of emotional intelligence report less death anxiety and fear of death. In this regard, Bailey and Hewison (2014) argue that the development of emotional intelligence should be one of the objectives of nurse training in relation to EOL care, and also that it should be based on experiential learning. This is because emotional work is a key component of the nursing role in this context, and adequate training can help to reduce the risk of occupational stress and burnout. Other authors (Aradilla-Herrero et al., 2014; Edo-Gual et al., 2014; Huang, Chang, Sun, & Ma, 2010; Strang et al., 2014) have similarly highlighted the importance of providing nurses with training in social and emotional skills, as caring for the dying patient is a complex task that requires an adequate emotional response in order to ensure high-quality care and to avoid an excessive emotional toll on the professional involved.
Limitations
This study has two main limitations. First, the use of a sample comprised solely of nursing undergraduates limits the extent to which the findings are generalizable. It is therefore important to conduct further studies of this kind in samples of qualified nurses in order to confirm the validity of the FATCOD-S. Second, the cross-sectional design prevents any causal relationships from being inferred among the study variables. Thus, future research should explore the temporal stability of the instrument. Finally, further research should aim to gather longitudinal data from different cohorts of students or qualified professionals, as this would enable more robust conclusions to be drawn regarding the possible causal relationship between the different variables studied here.
Conclusions
The results of this study indicate that the FATCOD-S is a valid instrument for assessing attitudes toward EOL care in the Spanish context. Fear of death and death anxiety can make it difficult for nurses to work with dying patients, and this may affect the quality of the care they provide. By contrast, emotional intelligence can help nurses to manage the feelings evoked through their close contact with patients and families in the EOL setting.
The use of the FATCOD-S with nursing students could provide important information about how these future professionals relate to dying patients and their family members. In this context, the training they receive should include strategies for developing their own social and emotional skills, thereby equipping them with the resources they need to care effectively not only for others but also for themselves.
Footnotes
Appendix A
Spanish Version of the FATCOD Scale (FATCOD-S). Copyright by Escuela Universitaria d’Infermeria Gimbernat: Adapted with permission of Katherine H Murray Frommelt, PhD., RN, PDE, CGC, FT.
Escala de Frommelt sobre Actitudes ante los cuidados del paciente moribundo
Totalmente en desacuerdo
En desacuerdo
Neutro
De acuerdo
Totalmente de acuerdo
1. Proporcionar cuidados de enfermería a una persona que se está muriendo es una experiencia muy valiosa
1
2
3
4
5
2. La muerte no es lo peor que le puede suceder a una persona
1
2
3
4
5
3. Me resultaría incómodo hablar con una persona que se está muriendo de su propia muerte
1
2
3
4
5
4. Los cuidados de enfermería a la familia deben continuar durante todo el proceso de duelo
1
2
3
4
5
5. No me gustaría tener que cuidar a una persona que se esté muriendo
1
2
3
4
5
6. La enfermera no es la persona adecuada para hablar de la muerte con una persona que se esté muriendo
1
2
3
4
5
7. Me provoca frustración el tiempo que requiere proporcionar cuidados de enfermería a una persona que se esté muriendo.
1
2
3
4
5
8. Me molestaría que una persona moribunda a la que estuviera cuidando perdiera la esperanza de mejorar
1
2
3
4
5
9. Es difícil establecer una relación estrecha con la familia de una persona que se está muriendo
1
2
3
4
5
10. A veces la muerte es aceptada por la persona que se está muriendo
1
2
3
4
5
11. Cuando un paciente pregunta a la enfermera, “¿me estoy muriendo?”, pienso que es mejor cambiar de tema
1
2
3
4
5
12. La familia debería implicarse en los cuidados físicos de la persona que se está muriendo
1
2
3
4
5
13. Preferiría que la persona a la que estoy cuidando muriese cuando yo no esté
1
2
3
4
5
14. Me da miedo establecer amistad con una persona que se está muriendo
1
2
3
4
5
15. Cuando una persona se muere, me dan ganas de salir corriendo
1
2
3
4
5
16. La familia necesita soporte emocional para aceptar los cambios en la conducta de la persona que se está muriendo
1
2
3
4
5
17. Cuando un paciente está cercano a la muerte, la enfermera debería dejar de implicarse en su cuidado
1
2
3
4
5
18. La familia debe preocuparse de que el enfermo viva lo mejor posible lo que le queda de vida
1
2
3
4
5
19. La persona que se está muriendo no debería tomar decisiones sobre sus cuidados físicos
1
2
3
4
5
20. La familia debería mantener un entorno tan normal como sea posible por el bien del enfermo
1
2
3
4
5
21. Es bueno que la persona que se está muriendo verbalice sus sentimientos
1
2
3
4
5
22. Los cuidados de enfermería deben hacerse extensivos a la familia de la persona que se está muriendo
1
2
3
4
5
23. Las enfermeras deben permitir un horario flexible de visitas para las personas que se están muriendo
1
2
3
4
5
24. La persona que se está muriendo y su familia deberían ser los responsables de la toma de decisiones
1
2
3
4
5
25. La adicción a los analgésicos no debería ser una preocupación para las enfermeras de un paciente moribundo
1
2
3
4
5
26. Me sentiría incómodo/a si al entrar en la habitación de un paciente con una enfermedad terminal, me lo encontrase llorando
1
2
3
4
5
27. Las personas moribundas deberían recibir respuestas honestas sobre su estado
1
2
3
4
5
28. Educar a las familias sobre la muerte y el proceso de morir no es una responsabilidad de enfermería
1
2
3
4
5
29. Los familiares que permanecen junto al paciente moribundo, a menudo interfieren en el trabajo del profesional con el paciente
1
2
3
4
5
30. Las enfermeras pueden ayudar a los pacientes a prepararse para la muerte
1
2
3
4
5
Acknowledgments
We are grateful to the participating nursing students and to the four nursing schools for their help with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the WeCare Chair: End-of-life Care of the Universitat Internacional de Catalunya, ALTIMA, and the Agency for the Management of University and Research Grants of the Government of Catalonia (grant numbers 2014SGR1139 and 2014SGR805). The sponsor had no role in the design or carrying out of the study, in the collection, management, analysis or interpretation of data, or in the preparation, review or approval of the manuscript.