
Abstract
Clergy have a key role in suicide prevention but report being undertrained, perhaps because a model that captures the competencies needed to engage suicide in faith communities and how these skills develop has not previously been available. Using grounded theory, this study addressed this gap by generating a developmental rubric based on interviews with 19 Protestant clergy, which were analyzed using a constant comparative method and were checked by interviewees operating at the highest level of development. The final 10 dimensions described over four developmental stages are (a) knowing role as clergy, (b) listening, (c) confidence, (d) risk assessment, (e) referral, (f) self-care, (g) community building, (h) postvention: ministering to survivors, (i) conducting memorial services or memorial ceremonies, and (j) clergy guilt. Results are based on clergy’s intuitive categories and provide a usable rubric for developing suicide prevention training for clergy.
Background
Suicide is a public health problem, the 10th leading cause of death in the United States (Centers for Disease Control [CDC], 2013). In 2013, in the United States, more people died of suicide (41,149 people) than of homicide (16,121 people; Centers for Disease Control and Prevention [CDC], 2015). Suicide affects all ages, and in 2013, suicide was the third leading cause of death in the 10- to 14-year-old age range, the second leading cause of death in the 15- to 34-year-old age range, the fourth leading cause of death in the 35- to 44-year-old age range, and the 5th leading cause of death in the 45- to 54-year-old age range (Centers for Disease Control and Prevention [CDC], 2015). A national strategy has been developed to guide suicide prevention, and faith-based organizations are recognized as having an important role to play (U.S. Department of Health and Human Services, 2012) for several reasons. People see clergy as “first-line helpers” for most mental health problems including risk of self-harm (Ellison, Vaaler, Flannelly, & Weaver, 2006, p. 197) and indeed suicidal people seek help from clergy (Leane & Shute, 1998; Wang, Bergland, & Kessler, 2003). In addition, religiosity not only protects against suicide (Larson & Larson, 2003) but is also used to cope with suicidal thoughts (Alexander, Haugland, Ashenden, Knight, & Brown, 2009; Weaver, Flannelly, Flannelly, & Oppenheimer, 2003), and people prefer for their treatment to integrate a spiritual component (Pargament, Murray-Swank, & Tarakeshwar, 2005). It is also the case that clergy perform memorial services following suicide deaths (Mason, Geist, Kuo, Day, & Wines, 2015; Mason et al., 2011).
However, a clergy workgroup reported that their training “did not prepare them adequately” to engage suicide in their faith communities (Marshall, 2005, p. 15), which may affect their ability to fulfill a preventative role (Leane & Shute, 1998). The Association of Theological Schools (ATS, 2010) does not require training in suicide prevention but requires that students in accredited institutions acquire “the abilities requisite to the exercise of ministry in that community (p. 5).” While suicide prevention skills might be developed through continuing professional education such as Continuing Pastoral Education or training through the Association for Death Education and Counseling, it seems that some clergy do not avail themselves of these opportunities. One reason may be that while some critical elements needed for competency-based suicide prevention training for clergy have been identified (Marshall, 2005), the stages over which these skills develop have not been identified. Clergy report needing suicide prevention training to develop critical competencies, but the stages over which these needed competencies develop is not known. To address this gap, the research question that guided this study was: What competencies do clergy say they need to engage suicide in faith communities and how do they say these skills develop over time? It is expected that findings will be used to develop training for clergy to prepare them to fulfill a key preventative role.
Method
Design
Grounded theory was used to inductively generate a theory (Charmaz, 2006; Creswell, 2007; Glaser & Strauss, 1967) of the clergy competencies, or dimensions, used and the developmental stages of those skills for engagement with suicide in faith communities. The theory is presented in the form of a developmental rubric. Developmental rubrics are based on standardized developmental ratings (SDRs), which were developed between 1970 and 1980 by David Dirlam (1972, 1980, 2014a) as a way to capture developmental stages of human activities (Dirlam & Byrne, 1978). Unlike judgmental rubrics that assign labels such as poor, average, good, and excellent to behaviors, developmental rubrics define strategies people use during four distinct stages. The stages used in this study were labeled beginning, fundamental, practical, and inspiring. The beginning stage describes strategies clergy use when they first engage with suicide in their faith communities. These first encounters could mean a request to minister to a suicidal person or a request to conduct a suicide funeral. The fundamental stage describes strategies clergy use after the first encounters are behind them. These fundamental strategies work temporarily but do not work long term. The practical stage occurs after many encounters with suicide-related requests. Clergy usually do not use these practical strategies until they have been in ministry for several years. Some clergy continue to use these strategies and do not progress to the final set of strategies which are called inspiring strategies. In this last stage, which is “creative, inspiring, and contagious” (Dirlam, 2014b), clergy’s influence is beyond their local faith community. Clergy in this stage have a lifetime of experience in the ministry and are able to help inspire change regarding the issue of suicide.
Through professional and personal networks, we identified a purposive sample of 19 U.S. Protestant clergy who had engaged suicide in their faith community. This initial study did not include other religious traditions although equally important. For grounded theory, Creswell (2007) suggests a sample of 20 to 30 interviewees to saturate the categories or dimensions. We continued interviewing clergy until saturation, until no new dimensions emerged in interviews. In one-on-one semi-structured interviews (see Appendix A for sample interview questions) conducted by the three authors, clergy were asked to describe competencies they had developed to engage suicide in their faith communities and the stages of growth they personally had experienced. The interviews were conducted during 2013 and 2014 and ranged from 45 min to 2 h each. Dimensions and stages generated by each interview were noted and then analyzed using the constant comparative method (Glaser & Strauss, 1967) in monthly meetings where the three researchers worked to consensus. During each meeting, dimensions and stages were added to the rubric or revised. Member checking (Merriam, 2009) was conducted via online focus groups with 10 participants who were deemed experts and working at the inspiring developmental stage. To avoid burdening all 10 clergy, the authors grouped them based on the areas where they were deemed to be working at the inspiring stage. Three clergy reviewed the following dimensions: knowing role as clergy, referral, and self-care. Four others reviewed these dimensions: risk assessment, listening, confidence, and community building. Two clergy reviewed these dimensions: postvention: ministering to survivors, conducting memorial services or memorial ceremonies, clergy guilt, and self-care. One clergy reviewed all dimensions and stages. The dimensions and stages were e-mailed to participants who replied to all participants to produce an online group discussion. During the focus groups, participants reviewed the developmental rubric, discussed the content and wording, and gave suggestions for language and clarification. The institutional review board at Gordon–Conwell Theological Seminary approved the study on May 30, 2013.
The participants were 19 Protestant clergy both active and retired (eight parish priests or pastors, nine chaplains, and two who were both pastors and chaplains) who had experience engaging with suicide in their faith communities, nine of them in military settings. The 5 female and 14 male participants ranged from 31 to 71 years old and their years of experience as clergy ranged from 5 to 44 years. The participants reported a range of 4 to 600 when asked for the number of suicidal persons who requested their help. They reported a range from 0 to 100 in terms of the number of suicide deaths that had occurred with individuals in their faith communities and a range of 0 to 20 for the number of suicide funerals they had conducted. Participants from different backgrounds and experiences were interviewed; 15 of the participants were White, 2 were Hispanic, 1 was Black, and 1 was Native American. They came from a variety of Protestant denominations, a variety of states and rural, suburban, and urban areas.
Results
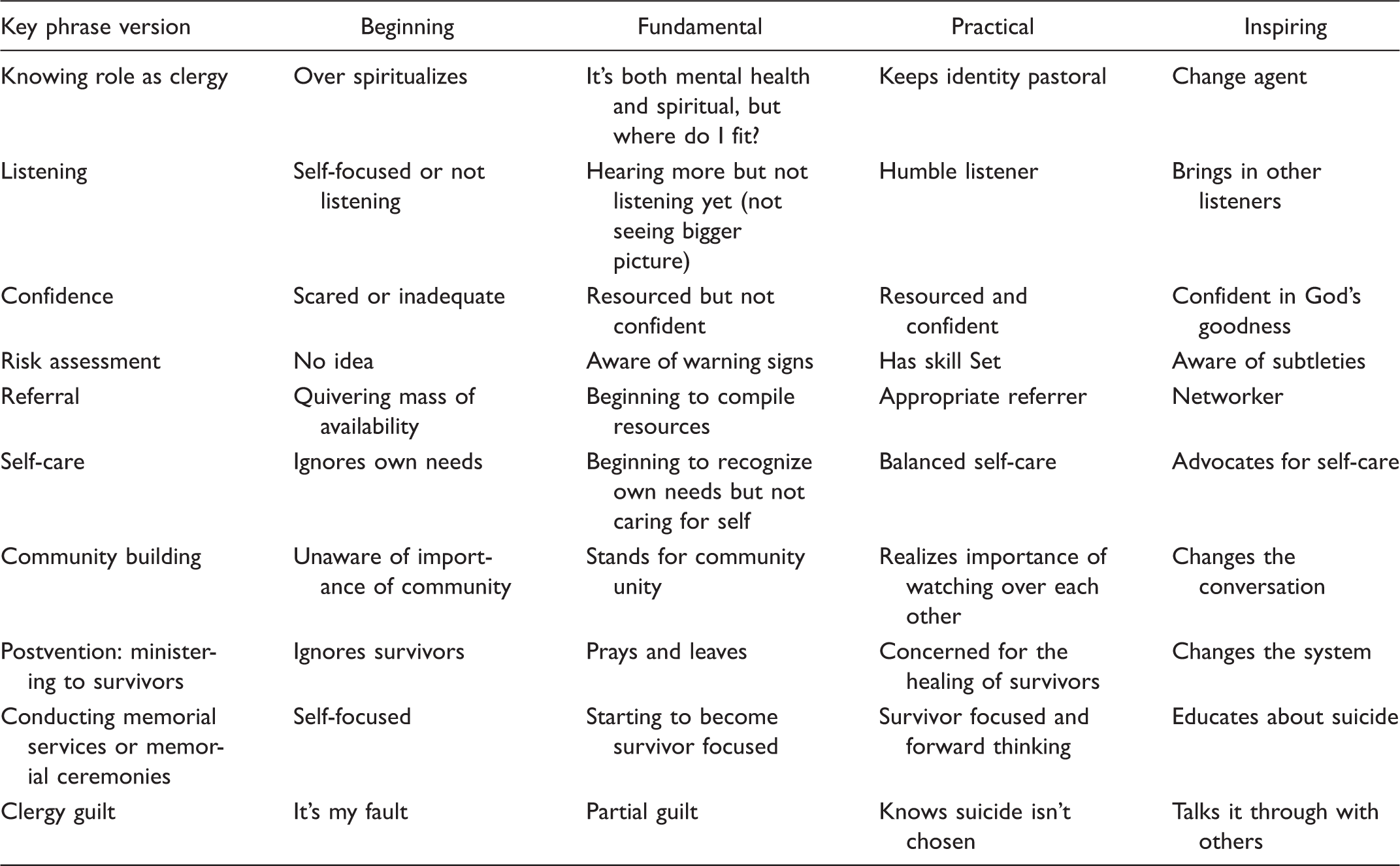
The developmental rubric contains 10 dimensions that clergy reported across four developmental stages of beginning, fundamental, practical, and inspiring. The 10 dimensions that were identified include (a) knowing role as clergy, (b) listening, (c) confidence, (d) risk assessment, (e) referral, (f) self-care, (g) community building, (h) postvention: ministering to survivors, (i) conducting memorial services or memorial ceremonies, and (j) clergy guilt. We found that not all clergy progressed through the four stages.
Suicide Engagement Dimensions Identified by Clergy Participants.
Knowing Role as Clergy
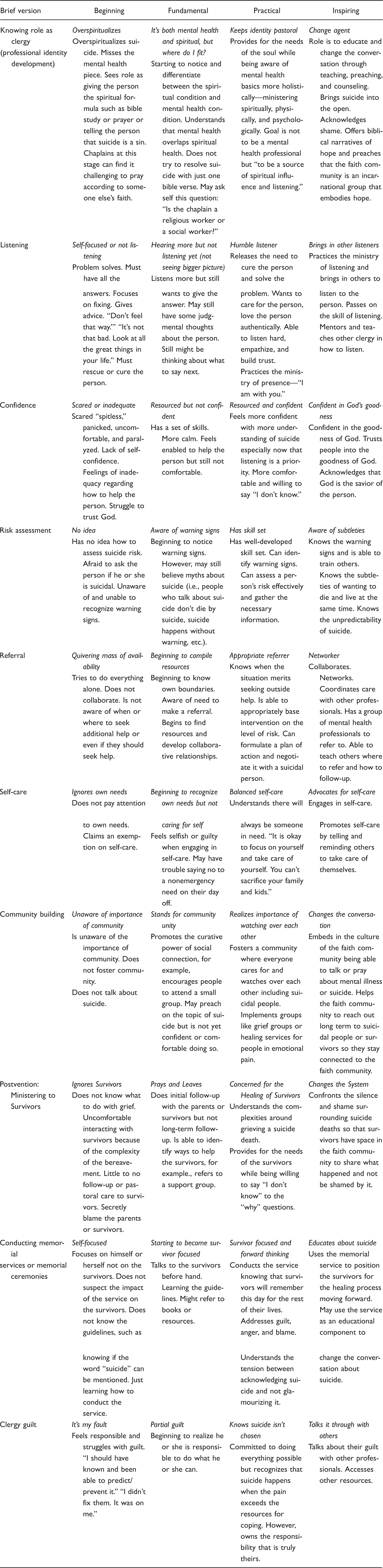
Participants said that in the beginning of the development of their professional identity, they would over spiritualize suicide and miss the mental health issue. One participant said, “I would tell people ‘Don’t do that because that would be a sin’ which would close down the conversation or [I would advise] bible study, prayer ‘Let’s pray that God would take those thoughts away.’” Middevelopment they began to differentiate between the spiritual and mental health conditions. One participant said, “Don’t attribute mental illnesses to a spiritual issue. It can be a mixture of both.” However, participants said they didn’t understand their role until the practical stage. As one clergy said, “Now I am clear about my role. I am a spiritual leader in the situation not the mental health professional” though clergy also said they needed to have a working knowledge of mental health basics. At the inspiring stage, clergy seek to be involved in “changing the conversation” about suicide through teaching and preaching.
Listening
Participants said they were so self-focused initially that they could not listen to suicidal people. They were especially focused on their perceived need to have a solution. One said, “I was rushing to find a solution, rushing to fix a problem before even getting a complete picture of what was going on in the person’s life.” They said that middevelopment they heard more of what the suicidal person said because they would “get off the pedestal” of needing to have all the answers. One clergy member reported, “The pastor needs to gain permission to be less than omniscient.” In the practical stage, clergy became humble listeners. I am not trying to fix anything for anyone. Rather I am looking forward to getting a deeper understanding of what this person is trying to communicate … so the person feels validated, so the person feels heard, the person feels I care.
Confidence
Participants said they were initially scared “spitless” to minister to a suicidal person because “I thought I had to be knowledgeable.” Another said, “I didn’t want others to know I didn’t know.” Another believed, “It was lack of confidence ….” Middevelopment, they began to develop skills, but it was not until the practical stage that they developed more confidence in their ministry to suicidal people. One clergy member said, “I don’t have all the answers but I am here with you, to walk with you.” At the inspiring stage, clergy trust God. “I don’t have a savior syndrome.” One said he knows now that “all healing comes from above.”
Risk Assessment
Participants said that in the beginning, they did not have any idea how to assess the risk level of a suicidal person and they were afraid to ask the suicidal person if he or she was suicidal. Middevelopment, they began to notice warning signs of suicidality but continued believing myths such as asking about suicide directly would put the idea in a person’s mind. Respondents at the practical stage had the skills to intervene with the suicidal person, often as a result of training and experience. At the inspiring stage, they train others and know the subtleties of ministering to a suicidal person like knowing about ambivalence or suicide’s unpredictability.
Referral
Respondents said that initially they did not refer a suicidal person. “In the beginning I was a ‘quivering mass of availability.’ 1 I wouldn’t refer. I overextended myself in terms of doing more than my role and exceeding my competencies.” Middevelopment, they began to develop resources such as collaborative relationships, and at the practical stage, they continued to play a role in providing spiritual care even after a referral. At the inspiring stage, clergy coordinate with other providers, see themselves as part of a team, may advocate for mental health system changes facilitating referral, and train others.
Self-Care
Participants said that in the beginning, they would ignore their own needs. Middevelopment, they began to recognize they had needs but felt guilty or selfish when caring for them and said they might take a call on their day off. At the practical stage, they sought balance in caring for others, self, and family. In the inspiring stage, clergy advocate for self-care for others.
Community Building
Respondents initially were unaware of the importance of community and did not foster it around the issue of suicide. Middevelopment, they began to see that social connection is curative for suicidal people and suicide survivors (those who have lost a loved one to suicide), but they did not encourage community-level interventions. At the practical stage, they intentionally fostered communities where everyone watches over each other. One chaplain said, “Everyone is a suicide watch stander.” Another reported, “We are a community that takes care of each other.” At the inspiring stage, clergy engage in changing the conversation at the faith community level, so that the community will reach out long term to suicidal people or suicide survivors. “An important aspect in ministering to survivors is to make sure that the community reaches out.” Another emphasized the importance of “fixing the condemning theology.”
Postvention: Ministering to Survivors
Clergy reported that in the beginning, they ignored survivors because they did not know how to respond to their grief because they were uncomfortable or because they did not understand their needs. One clergy member explained, “I would have treated [suicide] like any other death. No follow up. No pastoral care to survivors.” Middevelopment, they did initial follow-up but not long term. At the practical stage, they understood the complexities of grieving a suicide death and provided long-term pastoral care to the survivors, being willing to say, “I don’t know” to questions like “How could this happen?” or “Why did God allow this?” At the inspiring stage, clergy work to change the system, “to create a space where [survivors] can share … not be shamed by [suicide].” In addition, clergy realize they themselves are survivors following a suicide death.
Conducting Memorial Services or Memorial Ceremonies
Respondents said that in the beginning, they were focused on themselves during services not on the survivors because they didn’t know what they could say or not say. Middevelopment, clergy began to become survivor focused. Later, in the practical stage, clergy understood the importance of addressing suicide if the family allowed. They also were aware of how important the service is for the survivors’ healing. In the inspiring stage, clergy use memorial services to educate about suicide and to position the survivors for the healing process.
Clergy Guilt
Participants said that following a suicide, they initially felt guilty: “I should have known and been able to predict or prevent it.” Middevelopment, clergy realized that they did not bear the responsibility. In the practical stage, clergy were aware that suicide is not chosen by the suicidal persons but occurs because of their pain. Clergy own the responsibility to do all they can. In the inspiring stage, clergy talk through guilt with others.
Catalysts
Although this study was intended to identify stages of development, several clergy talked about events or experiences, catalysts, which helped them move from one stage to the next. Catalysts mentioned included self-reflection (e.g., dealing with one’s own death issues), education or training (e.g., clinical pastoral education, suicide-specific training), having a mentor or model, getting more life experience (e.g., working with suicidal people, doing death notifications or funerals), or responding to system change (e.g., the military changes their procedures).
Discussion
Clergy poignantly described their preventative role in ministering to suicidal people and survivors. They also clearly described competencies needed and how these develop, informing a path for undertrained clergy to improve their skills. Interviews with 19 Protestant clergy yielded 10 dimensions across four developmental stages. These findings provide (a) an accessible and substantive list of critical competencies for suicide prevention, based on clergy’s intuitive categories, (b) qualitative reflections on the process of career development of the competencies over time without judgment attached to any particular stage (e.g., without using labels of poor, average, good, or excellent), and (c) a usable rubric for developing training for clergy. It is important to note that though these competencies are discrete, they are also related and overlap. For example, referral is related to self-care because referral reduces clergy burden (McMinn et al., 2005; Weaver, Flannelly, Larson, Stapleton, & Koenig, 2002). It is also important to note that a number of these competencies are used broadly in pastoral counseling, such as knowing the clergy role, listening, developing confidence, referral and self-care. However, interviewees described how these basic competencies are used when engaging the issue of suicide.
While a previous clergy workgroup sponsored by The Link and the Suicide Prevention Resource Center (SPRC; Marshall, 2005) yielded similar competencies, a developmental model informing skill and curriculum development was not previously available. A strength of the current findings is that while this study’s findings corroborate previous findings, this study systematizes previous findings based on clergy intuitive categories into a more usable model. For example, a clergy workgroup (Marshall, 2005) said that two critical elements for a competency-based curriculum for clergy are “Information about the relationship between suicide and mental illness” and “How to approach the issue of suicide and related mental illnesses as more than just a ‘spiritual problem’” (Marshall, 2005, p. 6). The current rubric situates these competencies in one dimension, “knowing role as clergy.” As another example, the current rubric combines the following three critical elements into one dimension “referral”: “Information about handling suicide-related emergencies in terms of directing individuals to appropriate treatment,” “Information about the process of mental health services and referrals,” and “Information about how to build collaborative networks with mental health providers” (Marshall, 2005, p. 6).
The Link and SPRC workgroup (Marshall, 2005) mentioned a competency that was only indirectly mentioned by this study’s clergy, “exploring one’s own attitudes toward suicide” (p. 7). Only one of this study’s military chaplains described attitudes toward suicide of the “old school military folks” when he said, “The old school military folks aren’t comfortable. Why are we honoring someone with military ceremony same as a war hero?” Another respondent talked about “fixing the condemning theology [of suicide].” It would seem that this study’s respondents were focused on the attitude of stigma in their communities, presumably because they had already explored their own attitudes toward suicide. In this study’s findings, the exploration of attitudes is subsumed under the dimensions of community building and conducting memorial services or memorial ceremonies. The Link and SPRC workgroup generated a competency not mentioned in these interviews, “being knowledgeable of cultural issues that may affect suicide” (Marshall, 2005, p. 11). Although this sample was culturally diverse, they did not mention the cultural issues. This is surprising because different factors are related to suicide in different cultures (Chu, Chi, Chen, & Leino, 2014; Perez-Rodriguez et al., 2014). However, it may be that when faced with a suicidal person, the participants’ focus may have been on safety issues not on cultural risk and protective factors.
Neither group mentioned the skills of managing suicide contagion and clusters and developing a theology of suicide. These omissions are surprising for several reasons. How suicide is talked about in a memorial service or ceremony could affect imitation of suicide (Suicide Prevention Resource Center, 2004). Neither the workgroup nor this study’s interviewees directly mentioned concern over managing suicide contagion or clusters. In addition, a respondent in another study talked about the need for theological reflection about suicide: Formal theological training addressing these issues that did more than battle over whether or not suicide is a sin (how helpful is that going to be in that moment??) would have been of great value the first time someone walked into my office and asked if their mom was in hell because of her suicide. (Mason et al., in press) It is precisely this complexity [of suicide], and the resulting confusion, uncertainty, and discouragement, along with a lack of understanding of what the Bible says and does not say, that have kept most religious communities from addressing suicide with the urgency and careful attention it deserves in the midst of today’s crisis (p. 97).
This qualitative study of 19 diverse Protestant clergy produced rich descriptions of their suicide prevention competency development. A study limitation is the inclusion of only Protestant clergy. Further research is needed to validate these findings in larger and diverse samples, while including several other competencies such as the understanding of the contribution of culture, managing imitation of suicide, and theological reflection. Another limitation may be that the participants may have differed in their levels of training. Educational experiences or trainings were mentioned as contributing to development. The authors did not ask for educational and training information because this study was focused on competencies and stages, not on the catalysts, those experiences that catalyzed development from an earlier stage to a later one. Future research might focus on understanding the relationship between training and functioning at the inspiring stage of development as well as on other potential catalysts that may contribute to operating at the inspiring stage.
Conclusions and Clinical Implications
From these interviews, it is clear that clergy engage the issue of suicide broadly not just intervening with suicidal people but also helping grieving families and community members following a suicide. Clergy need a breadth of competencies to fulfill a suicide prevention role in faith communities. Clergy interviewees identified 10 discrete and interrelated dimensions. The rubric developed through this study clarifies the stages of development, which can inform clergy on how to improve their suicide prevention skills. The rubric can be used to develop suicide prevention training curriculum for clergy. However, given a lack of standards for clergy suicide prevention training to occur, it may also be important to raise awareness among clergy for the need for ongoing education beyond initial academic programs.
Appendix A
Sample of Semi-Structured Interview Questions
Clergy engage the issue of suicide both in helping suicidal people and in helping family members and faith communities following a suicide. In this interview, “engaging suicide” means helping suicidal people and helping family members and faith communities following a suicide.
What are some different components of becoming effective with engaging suicide? What skills do (pastors or chaplains) need to engage the issue of suicide in faith communities in order to work with suicidal people or to work with families or communities following a suicide? What does it look like when a clergy member member first learns to (listen)? How would I see a clergy member (listening)? What are things that a new clergy will do when engaging suicide? What are things that a more seasoned clergy member will stop doing when engaging suicide and start doing? What did you do in the past that no longer works? Is there a way where you use this skill differently at the beginning or middle or at the end of your career? What are things that a master clergy member will do when engaging suicide? As a more mature practitioner now, how do you (listen) differently?
Appendix B
Brief Version of Rubric
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.